

INTRODUCTION
The American Medical Association recently called for the elimination of solitary confinement for the mentally ill, citing its mental health harms.1 In solitary confinement, people are held in a prison cell roughly the size of a parking space for ~ 22–23 h per day with 1 or 2 h of exercise, also in isolation.2 Although the living conditions in these units (e.g., limited exercise, extreme loneliness) are known risk factors for adverse physical health outcomes including cardiovascular disease,2 the lifetime cardiovascular burden of solitary confinement is unknown.
METHODS
To estimate the lifetime cardiovascular disease burden and costs associated with solitary confinement, we used public data from a 2015 lawsuit3 describing the prevalence of hypertension diagnoses among two groups of incarcerated men ages 27–45: those housed in one prison’s solitary confinement “supermax” units and those in the prison’s less-isolating maximum security units (Table 1). Those in solitary confinement received no group recreation or contact visits and few (if any) phone calls; those in maximum security received 2 h of daily group recreation, contact visits, and more calls. Individuals in solitary confinement scored an average of 54.9 on the UCLA Loneliness Scale (scale ranges 20–80, 80 is most lonely); those in maximum security averaged 41.6.3
Table 1.
Calculation of the 31% Difference in Hypertension from the 2015 Hawkley Report. Values from the 2015 Hawkley Report3

*In the maximum security wing of the same prison
Using the Cardiovascular Disease Policy Model, a computer simulation of cardiovascular disease in US adults,4 we estimated the lifetime incremental burden of disease, loss of quality-adjusted life years (QALYs), and medical costs associated with new diagnoses of hypertension at age 35. We assumed average systolic blood pressure distributions and control rates among hypertensive 35-year-olds based on the 2011–2014 National Health and Nutrition Examination Survey. Quality-of-life weights were based on observational data from the Global Burden of Disease study. Medical costs were estimated using California’s Office of Statewide Health Planning and Development, deflated using cost-to-charge ratios and the ratio of the US national average costs to California’s, and then inflated to 2017 dollars using the Consumer Price Index.
RESULTS
Over a lifetime, 1000 men with newly diagnosed hypertension at age 35 are expected to experience 10 additional myocardial infarctions and 21 additional cardiovascular accidents, representing a loss of 732 QALYs and over $20 million in additional healthcare costs. Because individuals in solitary confinement experienced an absolute 31% higher hypertension prevalence than those in maximum security units (Table 1), nearly one-third may experience this higher burden of cardiovascular disease and cost.
Because we used previously collected data, this analysis assumed the following: (1) hypertension diagnoses persist over a lifetime; and (2) individuals in prison and the community experience the same control and cardiovascular effects of hypertension. These assumptions are reasonable based on the epidemiology of hypertension and likely conservative (we do not, for example, account for the larger effect sizes for hypertension on cardiovascular outcomes for African Americans, a population over-represented in prisons). We focused on hypertension-related cardiovascular disease and did not consider other possible conditions caused or worsened by solitary confinement, suggesting this analysis underestimates solitary confinement’s overall impact on health and related costs. While a wealth of research describes the impact of isolation on stress hormone dysfunction and adverse cardiovascular outcomes including hypertension and mortality,3 use of secondary data limited our ability to assess whether additional factors contributed to the increased hypertension prevalence among those housed in solitary confinement.
DISCUSSION
This study projects the lifetime cardiovascular disease and cost burden associated with the increased prevalence of hypertension diagnoses found in persons in solitary confinement compared with maximum security housing in the same prison. In 2017, over 60,000 US individuals were held in solitary confinement for 15 days or longer.5 Applying our findings to just the 25,000 individuals held in “supermax” solitary confinement units6 would alone result in $155 million in additional future healthcare costs and a loss of 5673 QALYs (Fig. 1)—likely significant underestimates given the widespread use of solitary confinement outside of “supermax” units. These findings, coupled with the growing consensus that solitary confinement is counter-productive as a public safety measure,5, 6 suggest an urgent need to dramatically reduce solitary confinement using alternative strategies that achieve safety without compromising health. This study also suggests cardiovascular disease organizations could join other associations in calling for solitary confinement reform and for the study of environmental health risks experienced by people in prison, including those in solitary confinement.
Figure 1.
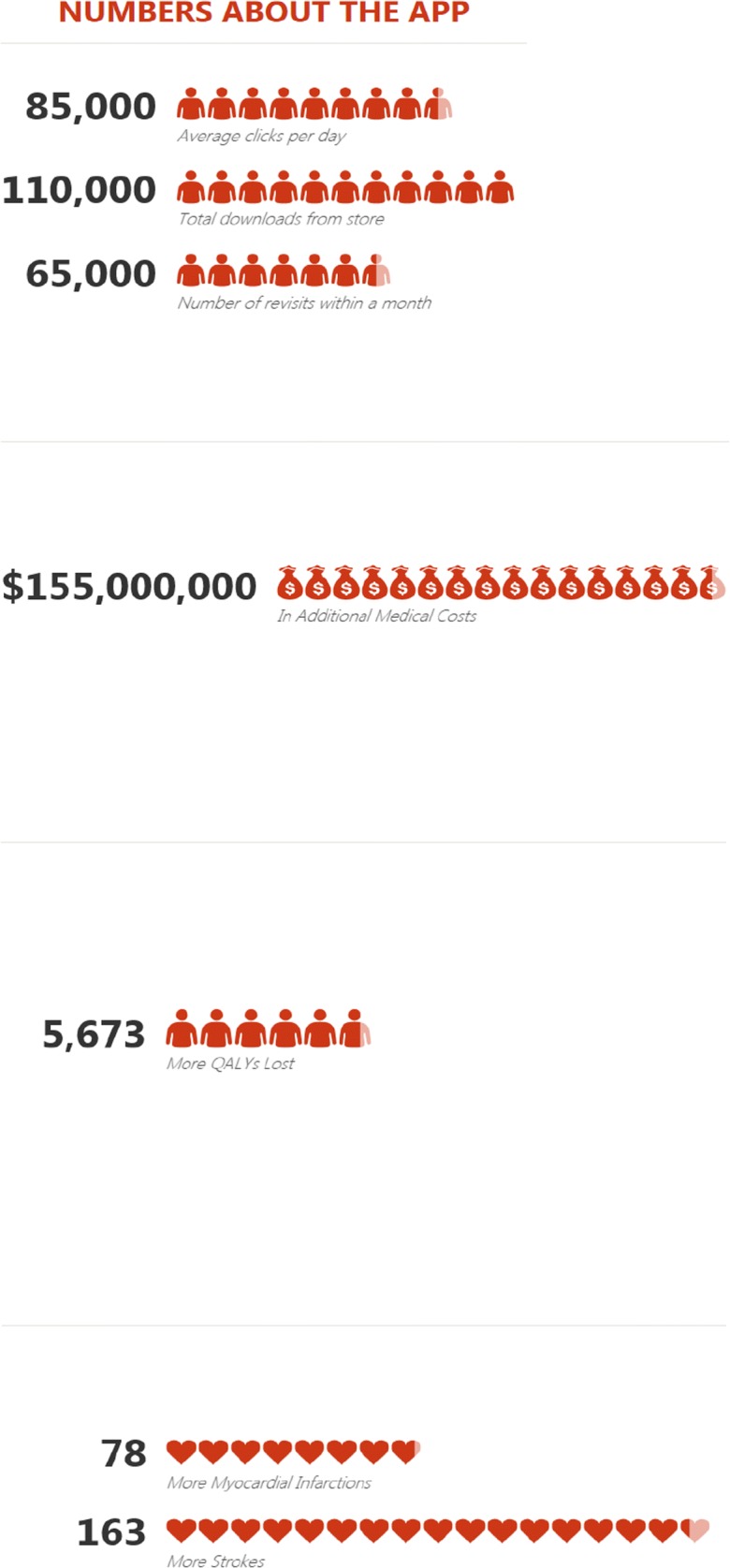
Increased adverse cardiovascular outcomes and high associated costs. For the 25,000 people currently in solitary confinement in US supermax prisons, a 31% increase in prevalence of hypertension will result in the following additional outcomes over the next 45 years (assuming an average life expectancy of 80 years old and the development of premature hypertension at age 35), compared with their counterparts in the maximum security wing of the same prison who experience less social isolation. Figure 1 contains poor-quality text inside the artwork. Please do not re-use the file that we have rejected or attempt to increase its resolution and re-save. It is originally poor; therefore, increasing the resolution will not solve the quality problem. We suggest that you provide us the original format. We prefer replacement figures containing vector/editable objects rather than embedded images. Preferred file formats are eps, ai, tiff, and pdf. Also, please confirm if it is captured correctly.We attach here the figure in its original format.
Authors’ Contributions
All those listed as authors had an active role and significant impact on conceptualizing, performing, analyzing, and/or writing up this research. No others made meaningful contributions to this work.
Funding
Funding and support was provided by the Jacob & Valeria Langeloth Foundation and the Medical Student Training in Aging Research (MSTAR) Program (NIH T35 AG026736).
Compliance with Ethical Standards
Conflict of Interest
Dr. Williams has served as an expert witness and as a court consultant in legal cases related to prison conditions of confinement. These relationships have included the National American Civil Liberties Union; Squire Patton Boggs; the Center for Constitutional Rights; and others. Dr. Williams was an informal consultant on a different aspect of the case described in this study and did not testify about it in court. No organization played a role in the decision to write this manuscript or in the analysis described in this manuscript. No other authors have conflicts of interest to report.
Disclaimer
Sponsors played no role in the design and conduct of this study or in preparation, review, or approval of the manuscript.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.American Medical Association House of Delegates. Reducing the Use of Restrictive Housing in Prisoners with Mental Illness: Resolution 412. 2018, page 641. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/hod/a18-reference-committee-reports.pdf. Last accessed March 18, 2019.
- 2.Ahalt Cyrus, Haney Craig, Rios Sarah, Fox Matthew P., Farabee David, Williams Brie. Reducing the use and impact of solitary confinement in corrections. International Journal of Prisoner Health. 2017;13(1):41–48. doi: 10.1108/IJPH-08-2016-0040. [DOI] [PubMed] [Google Scholar]
- 3.Expert Report of Louise C. Hawkley, Judge: Honorable Claudia Wilken. United States District Court Northern District of California Oakland Division: Todd Ashker, et Al., Plaintiffs, v. Governor of the State of California, et Al., Defendants.; 2015. https://ccrjustice.org/sites/default/files/attach/2015/07/Hawkley Expert Report.pdf. Last accessed March 18, 2019.
- 4.Odden Michelle C., Pletcher Mark J., Coxson Pamela G., Thekkethala Divya, Guzman David, Heller David, Goldman Lee, Bibbins-Domingo Kirsten. Cost-Effectiveness and Population Impact of Statins for Primary Prevention in Adults Aged 75 Years or Older in the United States. Annals of Internal Medicine. 2015;162(8):533. doi: 10.7326/M14-1430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Resnik, Judith and VanCleave, Anna and Bell, Kristen and Harrington, Alexandra and Conyers, Gregory and McCarthy, Catherine and Tumas, Jenny and Wang, Annie, Reforming Restrictive Housing: The 2018 ASCA-Liman Nationwide Survey of Time-in-Cell (October 10, 2018). Yale Law School, Public Law Research Paper No. 656. Available at SSRN: https://ssrn.com/abstract=3264350or10.2139/ssrn.3264350. Last accessed March 18, 2019.
- 6.2014 ACLU Foundation. ACLU Briefing Paper: The Dangerous Overuse of Solitary Confinement in the United States. New York; 2014. https://www.aclu.org/report/dangerous-overuse-solitary-confinement-united-states. Last accessed March 18, 2019.