

Abstract
Background:
Air pollutants and their pathogenic effects differ among regions and seasons. We aimed to explore the relationship between fine particulate matter (PM2.5), sulfur dioxide (SO2), and ozone-8 hours (O3-8h) concentrations in heating and non-heating seasons and the associated death risk due to cardiovascular diseases (CDs), respiratory diseases (RDs), and malignant tumors.
Methods:
Data were collected in Shenyang, China, from April 2013 to March 2016. We analyzed the correlation or lagged effect of atmospheric pollutant concentration, meteorological conditions, and death risk due to disorders of the circulatory system, respiratory system, and malignant tumor in heating and non-heating seasons. We also used multivariate models to analyze the association of air pollutants during holidays with the death risk due to the evaluated diseases while considering the presence or absence of meteorological factors.
Results:
An increase in the daily average SO2 concentration by 10 μg/m3 increased the death risk by CDs, which reached a maximum of 2.0% (95% confidence interval [CI]: 1.3%–2.7%) on lagging day 4 during the non-heating season and 0.2% (95% CI: 0.1%–0.4%) on lagging day 3 during the heating season. The risk of death caused by RDs peaked on lagging day 1 by 0.8% (95% CI: 0.4%–1.2%) during the heating season. An increase in O3-8h concentration by 10 μg/m3 increased the risk of RD-related death on lagging day 2 by 1.0% (95% CI: 0.4%–1.7%) during the non-heating season, which was significantly higher than the 0.1% (95% CI: 0–0.9%) increase during the heating season. Further, an increase in the daily average PM2.5 concentration by 10 μg/m3 increased the risk of death caused by RDs by 0.3% and 0.8% during heating and non-heating seasons, respectively, which peaked on lagging day 0. However, air pollution was not significantly associated with the risk of death caused by malignant tumors.
Conclusion:
Short-term exposure to PM2.5, SO2, and O3 during the non-heating season resulted in higher risks of CD-related death, followed by RD-related death.
Keywords: Air pollutants, Cardiovascular diseases, Respiratory diseases, Risk of death
Introduction
Many epidemiological studies have demonstrated that short-term exposure[1] or long-term exposure[2] to atmospheric pollutants may negatively affect human health. Reduction in life expectancy and premature death are the most direct and serious health consequences. The remarkable impacts of air pollutants on the cardiovascular system include increased risk of hypertension, arrhythmia, heart failure, and ischemic heart disease.[3–6] In addition, air pollutants have also been reported to increase the risk of respiratory diseases, such as asthma and chronic obstructive pulmonary disease, which considerably influence human health.[7–11] Recent studies have also found that the presence of fine particulate matter (PM2.5) is associated with the development of malignant tumors, such as lung cancer,[12,13] breast cancer,[14] pancreatic cancer,[15] and bladder cancer.[16] The concentrations of pollutants considerably differ among regions and seasons.[17,18] Owing to its geographic location in the south of northeast China, Shenyang has a temperate and semi-humid continental climate, with an annual temperature ranging from −35°C to 36°C and an average temperature of 8.3°C. Shenyang is the largest transport hub in northeast China, and it harbors both basic and processing industries. Thus, most air pollutants in this region originate from coal combustion and vehicle emissions, whereas a small proportion originates from photochemical reactions. In the current study, the pollution indices in Shenyang were evaluated during heating and non-heating seasons. To determine the relationship between air pollutants and human health, we analyzed the impact of the concentrations of PM2.5, sulfur dioxide (SO2), and ozone-8 hours (O3-8h) on cardiovascular and respiratory diseases and malignant tumors from April 1, 2013 to March 30, 2016 in Shenyang.
Methods
Ethical approval
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local ethics committee of Central Hospital affiliated to Shenyang Medical College (No. 2018[0026]).
Data source
Daily death data of residents from five districts in Shenyang City (China) were collected from the Center for Disease Control of the city between April 2013 and March 2016. The specific information collected included the following: sex, date of birth, date of death, regional code of permanent address, and code of the underlying cause of death. The causes of death were screened according to the regional code of patient's permanent address. The data on deaths caused by cardiovascular diseases (I00-I97), respiratory diseases (J00-J98), and tumors (C00-D48) were analyzed according to the code of the underlying cause of death (10th revision of the International Classification of Diseases).
Environmental data
Data on atmospheric PM2.5, SO2, and O3-8h concentrations were obtained from eleven state-controlled environmental air quality automatic monitoring stations in Shenyang. PM2.5 concentrations were monitored using the β-ray absorption method (dynamic heating) and light scattering method (light turbidity); SO2 concentrations, using pulsed ultraviolet (UV) fluorescence method; and O3 concentrations, using UV photometry (TE 49I O3 Analyzer, American Thermoelectric Corporation, Waltham, MA, USA). During the monitoring process, the SO2 standard gas produced by the National Institute of Metrology was used for calibration, and the O3 analyzer was calibrated using the Thermo 49iPS UV photometer O3 calibrator (Thermo Fisher Scientific, Waltham, MA, USA). Each instrument was calibrated once every 7 days, and the sampling line was cleaned at least once a month to ensure the accuracy and validity of the monitored data. Relevant statistics and evaluations were based on the following: Environmental Air Quality Standards (GB3095-2012), AQI Technical Regulations (HJ 633-2012), and Technical Specifications for Environmental Air Quality Assessment (Trial) (HJ 663-2012). The eleven state-controlled environmental air quality automatic monitoring stations covered five districts in Shenyang: Heping District, Shenhe District, Huanggu District, Dadong District, and Tiexi District. Contaminant data were also collected from all environmental monitoring stations. Daily average temperature, average relative humidity, mean pressure, and other meteorological data were acquired from the Shenyang Meteorological Bureau.
Statistical analysis
The statistical software Stata 12.0 (StataCorp, TX, USA) was used for statistical analysis. For the general population, daily deaths caused by cardiovascular and respiratory diseases and tumors (time-series data) were considered as small-probability events; their distribution was similar to the Poisson distribution. Thus, the Poisson regression generalized linear model (GLM)[19] was used for analysis:
 |
where Yi is the observation day; E(Yi), death on the specific day i; α, predicted value of deaths on the observation day i; X, intercept; β, indicator variable that has a linear influence on the corresponding variable; Z, indicator variable coefficient estimated by the regression model; and Σ, variable that has a non-linear influence on the corresponding variable.
The effect of single atmospheric pollutant on the deaths caused by cardiovascular and respiratory diseases and malignant tumors was analyzed by fitting the single-factor GLM and employing the deviation test. Relative risks (RR) were used to evaluate the magnitude of the hazard, α = 0.05. P < 0.05 was considered statistically significant.
Considering the possible lagged effects of pollutants on human body, 1 to 7 days of lagging (lagging days) were selected to analyze the changes caused by atmospheric pollutants on the studied death cases.
Spearman rank correlation was used to analyze the correlation between atmospheric pollutants and the risk of death. Differences in the atmospheric pollutant index and deaths caused by cardiovascular and respiratory diseases and tumors between the heating and non-heating seasons were evaluated using the rank-sum test.
Results
Concentration of atmospheric pollutants, meteorological conditions, and deaths caused by cardiovascular and respiratory diseases and malignant tumors
The concentrations of atmospheric pollutants, meteorological conditions, and evaluated deaths did not follow a normal distribution from April 2013 to March 2016. The median daily PM2.5 concentration was 79 μg/m3, with a minimum concentration of 12 μg/m3, recorded on September 5, 2015 (non-heating season), and a maximum concentration of 885 μg/m3, recorded on November 8, 2015 (heating season). The median concentration of SO2 was 75 μg/m3 and that of O3-8h was 74 μg/m3. The wind speed was 2.2 ± 0.9 m/s. The median temperature was 9.0°C. The humidity level was 60.5% ± 15.1%, and the atmospheric pressure was 1016.2 ± 9.9 Pa. During the heating season, the wind speed was 2.2 ± 0.9 m/s; median temperature, −3.9°C; and atmospheric pressure, 1024.8 ± 6.5 Pa. During the non-heating season, the wind speed was 2.2 ± 0.9 m/s; median temperature, 18.2°C; humidity level, 62.8% ± 15.3%; and atmospheric pressure, 1010.6 ± 7.5 Pa.
The number of residents included in the study was 3,751,698. The average number of deaths per day caused by cardiovascular diseases (eg, chronic rheumatic heart disease, hypertensive heart disease, acute myocardial infarction, and cor pulmonale) was 41. The average number of deaths caused by respiratory diseases (eg, pneumonia, chronic lower respiratory tract disease, and pneumoconiosis) was nine per day and that caused by malignant tumors (eg, nasopharyngeal carcinoma, esophageal cancer, stomach cancer, colon cancer, rectal cancer, anal cancer, liver cancer, breast cancer, lung cancer, cervical cancer, bladder cancer, and leukemia) was 22 per day on average.
Differences in concentrations of atmospheric pollutants and deaths between heating and non-heating seasons
During the heating season, the average concentrations of PM2.5, SO2, and O3-8h were 93, 147, and 45 μg/m3, respectively; during the non-heating season, their concentrations were 55, 34, and 97 μg/m3, respectively. The concentrations of PM2.5 and SO2 during the heating season were significantly higher than those during the non-heating season (both P < 0.001). In contrast, the concentration of O3-8h during the non-heating season was significantly higher than that during the heating season (P < 0.001). Ozone, which is a secondary pollutant, is related to light, and usually reaches its maximum level in the afternoon.
The number of daily deaths caused by cardiovascular and respiratory diseases and malignant tumors was 44, 9, and 22, respectively, during the heating season (from November 1 to March 30 of the following year) and 39, 8, and 23, respectively, during the non-heating season (from April 1 to October 31). The number of daily deaths caused by cardiovascular diseases during the heating season was significantly higher than that during the non-heating season (P < 0.001). However, no significant difference was observed in the daily deaths caused by respiratory diseases and malignant tumors between the two seasons (P = 0.130).
Relationship between O3-8h and other pollutants during heating and non-heating seasons
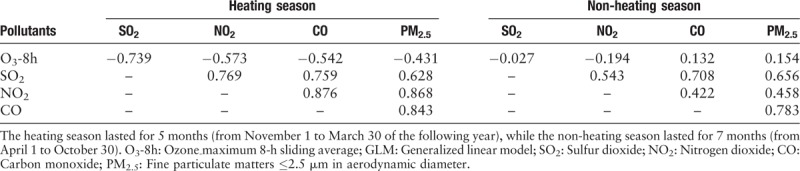
The correlation coefficient between O3-8h and SO2, NO2, CO, and PM2.5 during the heating season ranged from −0.739 to −0.431. The correlation coefficient between SO2 and NO2, CO, and PM2.5 ranged from 0.769 to 0.628, while that between O3-8h and SO2, NO2, CO, and PM2.5 during the non-heating season ranged from −0.027 to 0.154. The correlation coefficient between SO2 and NO2, CO, and PM2.5 ranged from 0.769 to 0.628 [Table 1].
Table 1.
The correlation coefficient between O3-8h and other pollutants by GLM.
Correlation analysis between concentrations of atmospheric pollutants and risk of death caused by cardiovascular and respiratory diseases and malignant tumors during the two seasons and the lagged effect
Single-factor GLM analysis of the concentrations of PM2.5, SO2, and O3-8h during the heating and non-heating seasons in relation to the analyzed deaths on different lagging days showed that when the daily average concentration of PM2.5 increased by 10 μg/m3 during both seasons, the risk of cardiovascular diseases peaked on lagging day 0. The RR increased by 0.3% (95% confidence interval [CI]: 0.1%–0.5%) and 0.8% (95% CI: 0.5%–1.1%) in the heating and non-heating seasons, respectively, whereas the lagged effects decreased with time. No significant influence was found on the risk of death caused by respiratory diseases and malignant tumors.
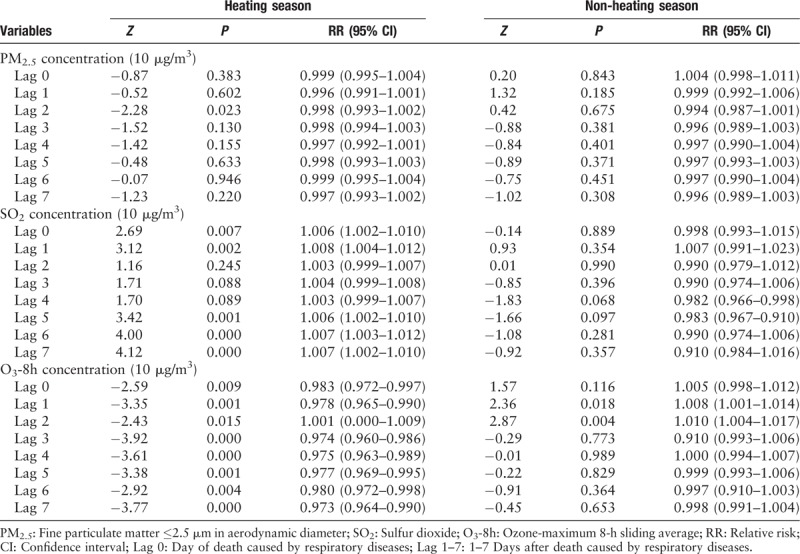
The increase in the daily average concentration of SO2 by 10 μg/m3 during the heating season increased the risk of cardiovascular diseases, which peaked on lagging day 3 by 0.2% (95% CI: 0.1%–0.4%). The risk of death caused by respiratory diseases peaked on lagging day 1 by 0.8% (95% CI: 0.4%–1.2%). During the non-heating season, the risk of cardiovascular diseases peaked on lagging day 4 by 2.0% (95% CI: 1.3%–2.7%). No significant influence was found on the risk of death caused by respiratory diseases and malignant tumors.
An increase in the daily average concentration of O3-8h by 10 μg/m3 during the heating and non-heating seasons increased the risk of death caused by respiratory diseases, which peaked on lagging day 2, with increases of 0.1% (95% CI: 0%–0.9%) and 1.0% (95% CI: 0.4%–1.7%), respectively. Minimal influence was found on the risk of death caused by cardiovascular diseases. No influence was found on the risk of death caused by malignant tumors [Tables 2–4].
Table 2.
Relationship between cardiovascular diseases and PM2.5, SO2, and O3-8h concentrations during the two seasons in the single-pollutant model in Shenyang from April 2013 to March 2016.
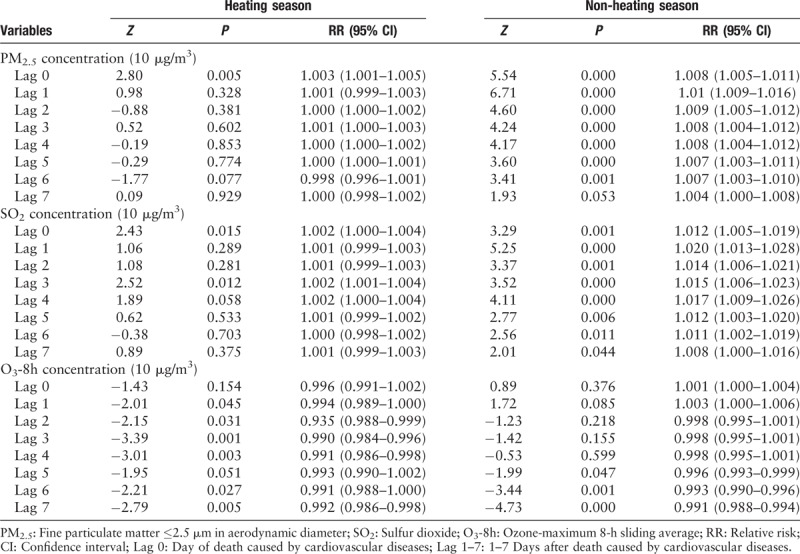
Table 4.
Relationship between malignant tumors and PM2.5, SO2, and O3-8h concentrations during the two seasons in the single-pollutant model in Shenyang from April 2013 to March 2016.
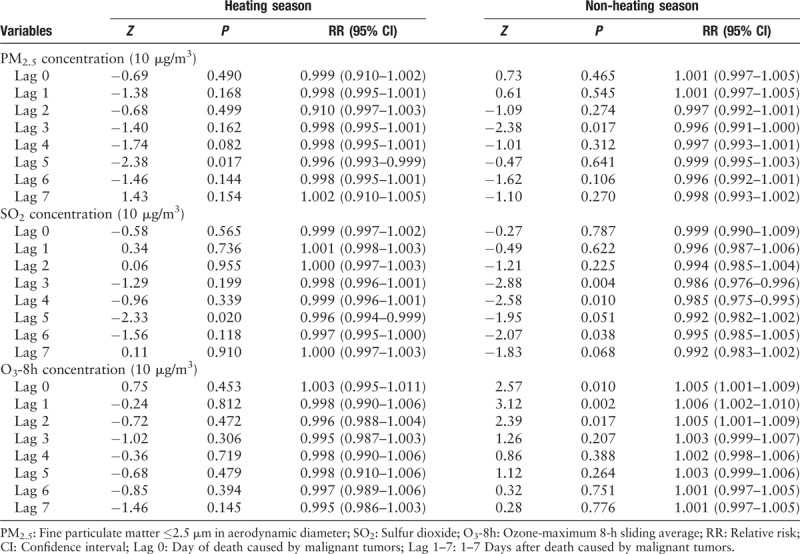
Table 3.
Relationship between respiratory diseases and PM2.5, SO2, and O3-8h concentrations during the two seasons in the single-pollutant model in Shenyang from April 2013 to March 2016.
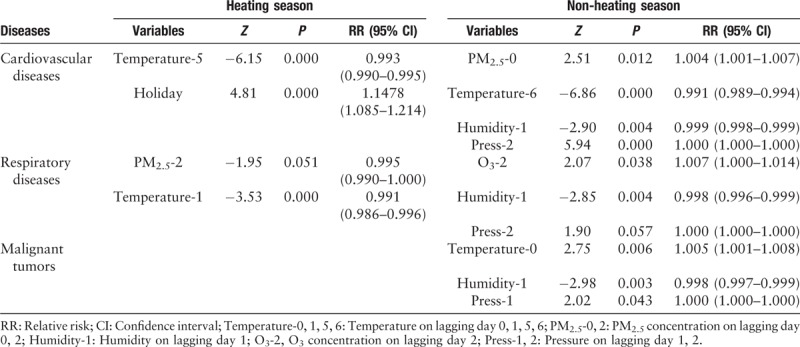
Analysis of death risk caused by cardiovascular and respiratory diseases and malignant tumors based on meteorological factors, holidays, and multivariate models of air pollutants in different seasons
During the heating season, the holidays and the temperature on lagging day 5 were significantly correlated with the risk of death in the circulatory system, indicating that the temperature during the heating season and the activities of the holidays increased the death of the circulatory system. Considering that PM2.5 may be highly correlated with temperature, only one of PM2.5 and temperature could be significantly correlated with the risk of death from the circulatory system.
The PM2.5 concentrations on the lagging day 0 of the non-heating season, temperature on lagging day 6, humidity level on lagging day 1, and pressure on lagging day 2 were significant, indicating that the PM2.5 concentrations during the non-heating season and death caused by cardiovascular diseases are related to temperature, air pressure, and humidity level.
The temperature on lagging day 1 during the heating season was significant, indicating that a low temperature during the heating season may increase the risk of death caused by respiratory diseases. The O3-8h concentration on lagging day 2 during the non-heating season, humidity level on lagging day 1, and pressure on lagging day 2 were also significant, indicating that O3-8h pollution, low humidity level, and high air pressure during the non-heating season increase the risk of death caused by respiratory diseases.
There were no significant variables during the heating season. The temperature on lagging day 0 in the non-heating season, humidity level on lagging day 1, and pressure on lagging day 1 were significant, indicating that a high temperature, low humidity level, and high air pressure during the non-heating season may increase the risk of death caused by malignant tumors [Table 5].
Table 5.
Analysis of the correlation of cardiovascular and respiratory diseases and malignant tumors with meteorological factors, holidays, and multivariable models of air pollutants during the two seasons.
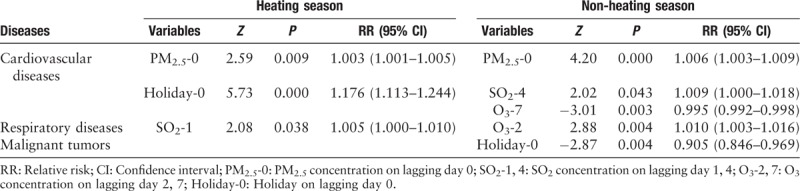
Correlation between air pollutant concentrations in multivariate model analysis during holiday season and other seasons, and the risk of death caused by cardiovascular and respiratory diseases and malignant tumors, regardless of meteorological factors
The PM2.5 on lagging day 5 and holidays are significant, indicating that higher PM2.5 during heating and holiday activities can increase the death of the circulatory system.
During non-heating season, PM2.5 on lagging day 0, SO2 concentration on lagging day 4, and O3 concentration on lagging day 7 were significant, indicating that PM2.5 and SO2 concentrations and a lower O3 concentration (to be studied) in a longer non-heating season can increase the risk of death caused by cardiovascular diseases.
The SO2 concentration, which increased on lagging day 1 in the heating season, was significant, indicating that a higher SO2 concentration during the heating season can increase the risk of death caused by respiratory diseases.
The O3 concentration, which increased on lagging day 2 in the non-heating season, remained significant, indicating that it can increase the risk of death caused by respiratory diseases.
Considering the risk of malignant tumors, the heating season showed no significant difference. The concentration of the air pollutants during the non-heating season was also not significant. However, holidays during the non-heating season were related to a reduced risk of death caused by malignant tumors, in consideration of staying indoors in the presence of smog [Table 6].
Table 6.
Correlation between the air pollutants in the multivariate model analysis and cardiovascular and respiratory diseases and malignant tumors during holidays and other seasons, regardless of meteorological factors.
Discussion
Shenyang city is located in the south of northeast China. Emissions of atmospheric pollutants in this region mainly originate from coal combustion, construction site dust emission, urban vehicle exhaust, industrial production emissions, and dust from other places. During the heating season, the percentages of air pollutants originating from different sources were as follows: coal combustion, approximately 45.5%; dust emission (construction site and other places), 8.9%; exhaust from urban vehicles, 18.6%; industrial production emission, 11.7%; and other sources, 17.3%. During the non-heating season, the percentages were as follows: coal combustion, approximately 28.0%; dust emission (construction site and other places), 16.1%; urban vehicle exhaust, 20.0%; industrial production emission, 22.8%; and other sources, 13.1%. The percentage of pollutants originating from coal combustion was higher than that from vehicle exhaust, regardless of the season. Thus, coal combustion is the primary source of PM2.5 pollution. PM2.5 in developed countries mainly originates from vehicle exhaust,[20] and the relationship between PM2.5 exposure and human health is stronger than that between PM10 (aerodynamic diameter: ≤10 μm) exposure and human health; thus, PM2.5 has greater influence on human death than does PM10.[21] The atmospheric pollution in the Pearl River Delta in China has largely been attributed to vehicle exhaust emissions and annual photochemical reactions caused by high insulation, which affect human death rates because these sources are related to environmental oxidants (O3).[22] Therefore, the sources of atmospheric pollutants vary among regions. Consequently, these pollutants also yield diverse negative health effects.
The results of our study showed that the concentrations of PM2.5 and SO2 consistently change. The concentrations of these two pollutants during the heating season were significantly higher than those during the non-heating season. In contrast, the concentration of O3-8h during the non-heating season was significantly higher than that during the heating season. The number of daily deaths caused by cardiovascular and respiratory diseases was higher during the heating season than during the non-heating season. However, the number of deaths caused by malignant tumors was not related to the type of season. Changes in the concentrations of PM2.5, SO2, and O3-8h and number of human deaths differed between the heating and non-heating seasons. The average daily concentration of PM2.5 during the heating season exceeded the grade II Ambient Air Quality Standard of China; and that during the non-heating season did not exceed this standard. However, the concentrations of SO2 and O3-8h did not exceed the standard in any of the two seasons. The average daily concentrations of SO2 during the heating season and O3-8h during the non-heating season were higher than those in the Pearl River Delta of China[18] and foreign countries.[23] The concentrations of the atmospheric pollutants and the number of deaths caused by cardiovascular and respiratory diseases during the heating season differed from those during the non-heating season. The concentration of atmospheric pollutants was directly related to an increase in pollutant emissions; however, no safety threshold is available in relation to the risk of death caused by the evaluated diseases.
Short-term exposure to atmospheric fine particles may increase the risk of death caused by cardiovascular and respiratory diseases. However, the effects of particulate matter on the estimated rates of death and lagged effects differed among studies.[24,25] Short-term or acute exposure to atmospheric pollutants during the non-heating season in northeast China caused a higher risk of death due to cardiovascular diseases, followed by respiratory diseases. In contrast, low concentrations of SO2 and O3-8h during the non-heating season yielded higher risks of deaths due to cardiovascular and respiratory diseases than did the high concentrations during the heating season. Moreover, the risks posed by SO2 and O3-8h exhibited different degrees of lagged effects on human deaths caused by cardiovascular and respiratory diseases. These results may be associated with increased tolerance to contaminants and decreased susceptibility in populations greatly exposed to pollutants.
Choi et al[26] showed that the influence of meteorological factors should be considered when the relationship between atmospheric pollutants and cardiovascular diseases is examined. Atmospheric pollutants that influence blood pressure have been reported to vary in different seasons; PM10 and NO2 yielded effects mainly during summer, whereas SO2 and O3 showed effects mainly during winter. Scarborough et al[27] studied deaths caused by coronary heart disease in England from 1999 to 2004 and found that the number of deaths increased as the temperature and duration of sunshine decreased. In the current study, data from the heating and non-heating seasons were classified, and the analysis showed that SO2 during the heating season played a decisive role in increasing the number of deaths caused by cardiovascular and respiratory diseases, which is consistent with the findings of previous statistics.
We also explored the correlation between meteorological factors, holiday seasons, and air pollutant multivariate models in different seasons and the risk of death caused by cardiovascular and respiratory diseases and malignant tumors. We found that multivariate model analysis correlates with the risk of death from circulatory, respiratory, and malignant disease. There was no significant variable in relation to the risk of death during the heating season. The temperature on lagging day 0 in the non-heating season, the humidity level after day 1, and the pressure on day 1 were significant, indicating that a high temperature, low humidity level, and high pressure during the non-heating season can increase the risk of death correlated to tumors. On considering the correlation between the multivariate model of air pollutants on holidays and in different seasons and the risk of death caused by cardiovascular and respiratory diseases and malignant tumors, regardless of meteorological factors, we found that holidays during the non-heating season were related to a reduced risk of death caused by tumors, given that the residents were in a good mood and did not leave their houses when high levels of smog were present.
Thus, short-term or acute exposure to PM2.5, SO2, and O3-8h during the non-heating season in Shenyang yielded a higher risk of death caused by cardiovascular diseases than by respiratory diseases. Low concentrations of SO2 and O3-8h during the non-heating season yielded higher risk of deaths caused by cardiovascular and respiratory diseases than did high concentrations during the heating season. However, the probable influence of the superposition and modification effects of PM2.5, SO2, and O3-8h on deaths caused by such diseases needs further study. Further, as the air pollution data, meteorological data, and patient sample collection in this study were only from Shenyang, there are certain limitations. Large prospective cohort studies are needed to explore the different components of atmospheric pollutants causing harm to the human body for relevant government departments to provide scientific theoretical bases for the prevention and control of atmospheric pollution.
Funding
This study was supported by grants from the Science and Technology Research Project of Department of Education of Liaoning Province (No. L2014419) and the Science and Technology Plan Project of Shenyang (No. F16-156-9-00).
Conflicts of interest
None.
Footnotes
How to cite this article: Xia SY, Huang DS, Jia H, Zhao Y, Li N, Mao MQ, Lin H, Li YX, He W, Zhao L. Relationship between atmospheric pollutants and risk of death caused by cardiovascular and respiratory diseases and malignant tumors in Shenyang, China, from 2013 to 2016: an ecological research. Chin Med J 2019;132:2269–2277. doi: 10.1097/CM9.0000000000000453
References
- 1.Shang Y, Sun Z, Cao J, Wang X, Zhong L, Bi X, et al. Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ Int 2013; 54:100–111. doi: 10.1016/j.envint.2013.01.010. [DOI] [PubMed] [Google Scholar]
- 2.Kim H, Kim J, Kim S, Kang SH, Kim HJ, Kim H, et al. Cardiovascular effects of long-term exposure to air pollution: a population-based study with 900 845 person-years of follow-up. J Am Heart Assoc 2017; 6:e007170.doi: 10.1161/JAHA.117.007170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cai Y, Zhang B, Ke W, Feng B, Lin H, Xiao J, et al. Associations of short-term and long-term exposure to ambient air pollutants with hypertension: a systematic review and meta-analysis. Hypertension 2016; 68:62–70. doi: 10.1161/HYPERTENSIONAHA.116.07218. [DOI] [PubMed] [Google Scholar]
- 4.Song X, Yu L, Hu Y, Zhao X, Tian J, Ding G, et al. Short-term exposure to air pollution and cardiac arrhythmia: a meta-analysis and systematic review. Int J Environ Res Public Health 2016; 13:642.doi: 10.3390/ijerph13070642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shah AS, Langrish JP, Nair H, McAllister DA, Hunter AL, Donaldson K, et al. Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet 2013; 382:1039–1048. doi: 10.1016/S0140-6736 (13)60898-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Xu M, Guo Y, Zhang Y, Westerdahl D, Mo Y, Liang F, et al. Spatiotemporal analysis of particulate air pollution and ischemic heart disease mortality in Beijing, China. Environ Health 2014; 13:109.doi: 10.1186/1476-069X-13-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.DeVries R, Kriebel D, Sama S. Low level air pollution and exacerbation of existing COPD: a case crossover analysis. Environ Health 2016; 15:98.doi: 10.1186/s12940-016-0179-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Taj T, Malmqvist E, Stroh E, Oudin Åström D, Jakobsson K, Oudin A. Short-term associations between air pollution concentrations and respiratory health-comparing primary health care visits, hospital admissions, and emergency department visits in a multi-municipality study. Int J Environ Res Public Health 2017; 14:587.doi: 10.3390/ijerph14060587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ghozikali MG, Mosaferi M, Safari GH, Jaafari J. Effect of exposure to O3, NO2, and SO2 on chronic obstructive pulmonary disease hospitalizations in Tabriz, Iran. Environ Sci Pollut Res Int 2015; 22:2817–2823. doi: 10.1007/s11356-014-3512-5. [DOI] [PubMed] [Google Scholar]
- 10.Ghanbari Ghozikali M, Heibati B, Naddafi K, Kloog I, Oliveri Conti G, Polosa R, et al. Evaluation of chronic obstructive pulmonary disease (COPD) attributed to atmospheric O3, NO2, and SO2 using air Q model (2011–2012 year). Environ Res 2016; 144:99–105. doi: 10.1016/j.envres.2015.10.030. [DOI] [PubMed] [Google Scholar]
- 11.Bowatte G, Erbas B, Lodge CJ, Knibbs LD, Gurrin LC, Marks GB, et al. Traffic-related air pollution exposure over a 5-year period is associated with increased risk of asthma and poor lung function in middle age. Eur Respir J 2017; 50:1602357.doi: 10.1183/13993003.02357-2016. [DOI] [PubMed] [Google Scholar]
- 12.Cao Q, Rui G, Liang Y. Study on PM2.5 pollution and the mortality due to lung cancer in China based on geographic weighted regression model. BMC Public Health 2018; 18:925.doi: 10.1186/s12889-018-5844-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pun VC, Kazemiparkouhi F, Manjourides J, Suh HH. Long-term PM2.5 exposures and respiratory, cancer and cardiovascular mortality in older US adults. Am J Epidemiol 2017; 186:961–969. doi: 10.1093/aje/kwx166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Parikh PV, Wei Y. PAHs and PM2.5 emissions and female breast cancer incidence in metro Atlanta and rural Georgia. Int J Environ Health Res 2016; 26:458–466. doi: 10.1080/09603123.2016.1161178. [DOI] [PubMed] [Google Scholar]
- 15.Wang Y, Li M, Wan X, Sun Y, Cheng K, Zhao X, et al. Spatiotemporal analysis of PM2.5 and pancreatic cancer mortality in China. Environ Res 2018; 164:132–139. doi: 10.1016/j.envres.2018.02.026. [DOI] [PubMed] [Google Scholar]
- 16.Yeh HL, Hsu SW, Chang YC, Chan TC, Tsou HC, Chang YC, et al. Spatial analysis of ambient PM2.5 exposure and bladder cancer mortality in Taiwan. Int J Environ Res Public Health 2017; 14:508.doi: 10.3390/ijerph14050508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cichowicz R, Wielgosiński G, Fetter W. Dispersion of atmospheric air pollution in summer and winter season. Environ Monit Assess 2017; 189:605.doi: 10.1007/s10661-017-6319-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Schwela D. Air pollution and health in urban areas. Rev Environ Health 2000; 15:13–42. doi: 10.1515/REVEH.2000.15.1-2.13. [DOI] [PubMed] [Google Scholar]
- 19.Schwartz J, Doekery DW, Neas LM. Is daily mortality associated specifically with fine particles? J Air Waste Manag Assoc 1996; 46:927–939. doi: 10.1080/10473289.1996.10467528. [PubMed] [Google Scholar]
- 20.Laumbach RJ, Kipen HM. Respiratory health effects of air pollution: update on biomass smoke and traffic pollution. J Allergy Clin Immunol 2012; 129:3–13. doi: 10.1016/j.jaci.2011.11.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Granum B, Løvik M. The effect of particles on allergic immune responses. Toxicol Sci 2002; 65:7–17. doi: 10.1093/toxsci/65.1.7. [DOI] [PubMed] [Google Scholar]
- 22.Tao Y, Huang W, Huang X, Zhong L, Lu SE, Li Y, et al. Estimated acute effects of ambient ozone and nitrogen dioxide on mortality in the Pearl River Delta of southern China. Environ Health Perspect 2012; 120:393–398. doi: 10.1289/ehp.1103715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bell ML, Kim JY, Dominici F. Potential confounding of particulate matter on the short-term association between ozone and mortality in multisite time-series studies. Environ Health Perspect 2007; 115:1591–1595. doi: 10.1289/ehp.10108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lu F, Xu D, Cheng Y, Dong S, Guo C, Jiang X, et al. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ Res 2015; 136:196–204. doi: 10.1016/j.envres.2014.06.029. [DOI] [PubMed] [Google Scholar]
- 25.Zeka A, Zanobetti A, Schwartz J. Short term effects of particulate matter on cause specific mortality: effects of lags and modification by city characteristics. Occup Environ Med 2005; 62:718–725. doi: 10.1136/oem.2004.017012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Choi JH, Xu QS, Park SY, Kim JH, Hwang SS, Lee KH, et al. Seasonal variation of effect of air pollution on blood pressure. J Epidemiol Community Health 2007; 61:314–318. doi: 10.1136/jech.2006.049205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Scarborough P, Allender S, Rayner M, Goldacre M. Contribution of climate and air pollution to variation in coronary heart disease mortality rates in England. PLoS One 2012; 7:e32787.doi: 10.1371/journal.pone.0032787. [DOI] [PMC free article] [PubMed] [Google Scholar]