

Abstract
Objectives:
To describe the outcomes of a collaborative response of federal, state, county, and local agencies in conducting syndromic surveillance and delivering medical care to persons affected by the storm through the use of mobile medical units.
Methods:
Nine mobile medical vans were staffed with medical personnel to deliver care in communities affected by the storm. Individual patient encounter information was collected.
Results:
A total of 14 033 housing units were approached and checked for occupants. Of residents with whom contact was made, approximately 10 percent required medical assessment in their homes; 3 218 clients were medically evaluated on the mobile medical vans. Sixty-two percent of clients were female. The most common presenting complaints included normal health maintenance (59%), upper respiratory tract illness (10%), and other illness (10%). Injuries occurred in 9 percent. A total of 1 531 doses of medications were dispensed from the mobile medical units during the response.
Conclusion:
Mobile medical units provided an efficient means to conduct syndromic surveillance and to reach populations in need of medical care who were unable to access fixed local medical facilities.
Keywords: disaster relief, hurricane, mobile medical units, syndromic surveillance
Hurricane Wilma, the 21st named storm of the 2005 Atlantic hurricane season, struck the southwest coast of Florida on Monday, October 24, as a category 3 storm. Hurricane force winds more than 110 miles per hour and rain caused widespread damage to homes and power lines, and temporarily displaced thousands of residents. Initial estimates indicated that the most severe damage occurred along the southeastern coast of Florida.1 In Broward County, the hurricane caused widespread extended power outages affecting approximately 900 000 homes and businesses and lasting over 3 weeks in some neighborhoods.2,3 This effectively shut down routine services and impeded daily operation of health and social services for the approximately 1.7 million residents. Hurricane Wilma resulted in an estimated 41 deaths (9 in Broward County)4 and was determined to be the third costliest storm in US history, with damages estimated at $14.4 billion.5
On October 28,2005, United States Public Health Service (USPHS) officers were deployed at the request of state and local health authorities to the Broward County Health Department (BCHD) to staff mobile medical clinics in order to augment local relief efforts and to deliver medical services to the areas most heavily affected by Hurricane Wilma. Nine mobile medical vans were staffed with USPHS, local health department, and Department of Veterans’ Affairs (DVA) personnel, as well as Centers for Disease Control and Prevention (CDC) Public Health Advisors (PHAs) stationed within the state of Florida. These mobile teams were dispatched to multistory retirement communities, mobile home parks, low-income housing facilities, and other areas that experienced significant structural damage and/or that requested medical assistance due to the inability of residents to leave their premises and access local medical facilities. Because of the widespread power outages lasting up to 3 weeks in Broward County, many residents with limited mobility living above the ground level were trapped in their homes with limited supplies due to inoperable elevators. This was compounded by the disruption of telephone communications necessitating door-to-door assessment of medical need. Many of these communities as well as other low-income communities heavily affected by the storm were identified as priority areas needing medical assistance. The outcomes of the collaborative efforts of the USPHS, the CDC, Florida Department of Health, the BCHD, and the DVA, in delivering medical relief services and conducting syndromic surveillance in response to Hurricane Wilma, are summarized here.
Methods
Areas of need were identified by preassessment teams comprising experienced outreach workers, health educators, and case managers employed by the BCHD. These teams conducted assessments of communities affected by the storm. Environmental health workers and community nurses reported additional areas of medical need to the BCHD. Priority for mobile van deployment was given to areas without electricity, areas with homes blocked by fallen debris, and communities where citizens with known medical needs resided such as developments housing elderly persons. In addition, teams consisting of staff from the CDC, the North Carolina Department of Health, and the Florida Department of Health conducted a rapid needs assessment that included 210 interviews within 42 individual county census blocks that represented the approximately 375 580 households in northeastern Broward County on the basis of 2000 US Census estimates. The assessments indicated that 5 percent to 15 percent of the households had members with one or more medical needs. From this information, public health department officials and the county Emergency Operations Center prioritized additional areas of potential medical need and identified locations for mobile medical van deployment. These locations consisted of retirement communities, mobile home parks, low-income housing facilities/apartments, churches, and other areas heavily affected by the storm. Advanced notice of mobile van deployment to local communities was performed by distribution of flyers in the communities, contact with community leaders or association presidents, and notification of local law enforcement officials 1 to 2 days prior to the planned arrival of the medical unit.
Nine mobile medical vans provided by local hospital and clinic organizations and the DVA were staffed with USPHS officers, BCHD staff, CDC PHAs, and DVA personnel. Each mobile van unit was typically staffed with 9 to 10 personnel that included a team leader, one medical doctor, one mid-level provider (nurse practitioner or physician’s assistant), one pharmacist, two nurses and a medical assistant, one to two staff members from the Broward County Health Department, a CDC PHA, a county social worker, and one or two members of the Florida Department of Elder and Veterans Affairs. Broward County provided nurses that assisted in patient care needs and in the advance site inspections to identify high-need areas for the mobile units. Services provided on the mobile medical vans included health maintenance assessments, primary medical care, monitoring oxygen and respiratory tract therapy, dispensing medications, and arranging for continued services. The BCHD coordinated the procurement of the mobile medical vans, medical supplies, pharmaceuticals, staffing, and transportation logistics. Advance agreements for use of mobile medical units were not obtained prior to the storm.
Data collection and analyses
Individual patient encounter information including gender, age, race, ethnicity, zip code, and presenting medical complaint was collected using a standardized surveillance form developed by the Florida Department of Health for use in disaster response. A convenience sampling method was used. Persons who sought care on the mobile vans or were approached in their homes were included in the analysis of reasons for visit. Separate data analyses were not conducted on the basis of client self-presentation to the mobile vans versus door-to-door visits by mobile unit staff. Client identifiers were not collected. Data were compiled and entered daily into an Excel database. Data analyses were performed using Excel (Version 2000, Microsoft, Redmond, Washington).
Definitions of reason for visit to the mobile medical unit were defined on the standardized surveillance form and included 15 syndrome categories: animal bite, asthma, carbon monoxide poisoning, dermatologic disorder (rashes, sores insect bite, sunburn), febrile illness, gastrointestinal illness, heat-related injury, other injury, lower respiratory tract illness (cough, shortness of breath, pneumonia), mental health (stress, anxiety), musculoskeletal system trauma (fracture, sprain, dislocation), minor wound/injury (abrasion, laceration, puncture, foreign body removal), normal health maintenance (blood pressure and blood glucose monitoring, prescription refills), other (not fitting into other categories), poisoning (pesticides, gas fumes, ingestions), and upper respiratory tract illness (cold, sore throat). For analysis purposes, some definitions were combined into larger categories including respiratory complaints (asthma, upper and lower respiratory tract complaints), and injuries (animal bite, heat-related injury, musculoskeletal trauma, minor wound).
Diagnostic procedures such as sputum or nasopharyngeal bacterial and viral cultures were not performed on the mobile vans. Thus, tracking of diagnostic trends was not available for purposes of epidemic detection. Patients requiring more intensive care were transported by ambulance to functioning emergency care centers. Clinical criteria for emergency referral were clinician dependent and not defined by the mobile unit response.
Results
During the period, October 28 to November 9, 2005, mobile medical van units visited 51 housing developments. A total of 140 33 housing units were approached and checked for occupants. Of these, approximately 40 percent (n = 5 646) were occupied. Of residents with whom contact was made, an estimated 10 percent needed medical assessment in their homes. Most residents needing medical assessment in their homes were not able to ambulate to mobile medical units due to physical limitations. Health issues encountered among these clients were similar, per staff reports, to those of clients presenting as “walk-ins” to the mobile medical units.
A total of 3 218 clients self-presented for medical evaluation on the mobile medical vans or were medically evaluated in their homes. The majority of these clients (approximately 85%) presented as walk-ins to the mobile medical units. Sixty-two percent of clients were female (n = 2 009); 67 percent (n = 2 153) of clients were White and 19 percent were Black (n = 901). Twenty-one percent (n = 673) of clients reported being of Hispanic ethnicity (Table 1).
TABLE 1.
Demographics of clients presenting for medical care in mobile van units or in homes visited by United States Public Health Service personnel during the Hurricane Wilma response (N = 3 218)
| Variable | |
|---|---|
| Age | |
| 0–18 | 334 (10) |
| 19–30 | 201 (6) |
| 31–50 | 773 (24) |
| 51–65 | 766 (24) |
| >65 | 1 109 (35) |
| Unknown | 35 (1.1) |
| Gender | |
| Male | 1 204 (37) |
| Female | 2 009 (62) |
| Unknown | 5 (0.2) |
| Race | |
| White | 2 153 (67) |
| Black | 901 (28) |
| Other/unknown | 164 (5) |
| Ethnicity | |
| Hispanic | 673 (21) |
| Non-Hispanic | 2 446 (76) |
| History of chronic disease | |
| Hypertension | 836 (26) |
| Diabetes | 328 (10) |
| Chronic obstructive pulmonary disease | 92 (3) |
| Clinical syndrome category | |
| Animal bite | 4 (0.2) |
| Asthma | 76 (2) |
| Carbon monoxide poisoning | 0 (0) |
| Dermatologic disorder | 112 (3) |
| Febrile illness | 0 (0) |
| Gastrointestinal tract illness | 80 (2) |
| Heat related | 0 (0) |
| Injury, other | 95 (3) |
| Lower respiratory tract illness | 29 (9) |
| Mental health | 122 (4) |
| Musculoskeletal system trauma | 124 (4) |
| Minor wound injury | 62 (2) |
| Normal health maintenance | 1 898 (59) |
| Other | 310 (10) |
| Poisoning, other | 0 (0) |
| Upper respiratory tract illness | 319 (10) |
Values given are number (percentage).
The most common presenting syndromes included normal health maintenance (59%, n = 1 898), upper respiratory tract illness (10%, n = 319), and other illness (10%, n = 310). The most frequent reasons for categorization as normal health maintenance (N = 1 898) included blood pressure check (64%, n = 1 215), medication refill (17%, n = 325), supportive reassurance (6%, n = 118), and glucose check (4%, n = 79). There were no presentations of suspected carbon monoxide poisoning (see Table 1). Current diagnosis of hypertension was reported by 26 percent (n = 836), diabetes by 10 percent (n = 328), and chronic obstructive pulmonary disease by 3 percent (n = 92) of clients. (see Table 1). The most frequently dispensed prescription and nonprescription medication types included pulmonary (15%, n = 231), pain relief (15%, n = 229), antibiotics (13%, n = 192), and hypertension (12%, n = 167). Forty-two tetanus vaccines were administered (Table 2).
TABLE 2.
Medication types dispensed from mobile medical units during the Hurricane Wilma response
| Medication type | |
|---|---|
| Diabetes | 74 (5) |
| Hypertension | 167 (11) |
| Cardiac | 97 (6) |
| Antibiotic | 192 (13) |
| Dermatologic | 63 (4) |
| Wound care | 108 (7) |
| Eye | 30 (2) |
| Pulmonary | 231 (15) |
| Pain | 229 (15) |
| Immunization | 42 (3) |
| Gastrointestinal | 110 (7) |
| Other | 188 (12) |
Values given are number (percentage).
Evaluation of the reason for visit to the mobile medical vans by date revealed an increasing proportion of acute care needs emerging during the period of the response (Figure 1). The proportion of visits for respiratory tract complaints, injuries, and mental health issues increased gradually, with peaks in these complaints 4 to 6 days after the initiation of the medical response. The most common reasons for emergency transport included severe hypertension and hyperglycemia. The estimated number of persons transported for emergency care for the above conditions during the response was 10.
FIGURE 1.
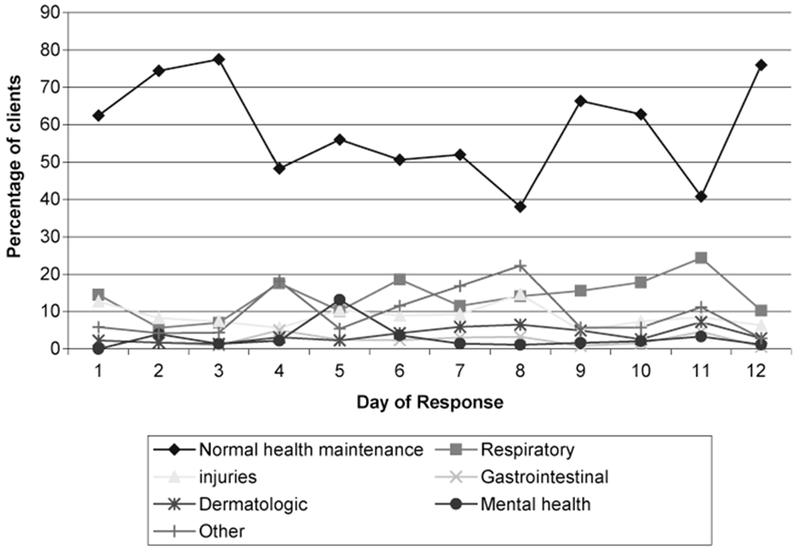
Reasons for Mobile Medical Unit Visit by Day of Response
Discussion
Hurricane Wilma followed hurricanes Katrina and Rita in the unforgettable storm season of 2005. Less attention was given to this storm despite it being one of the most costly storms in history. In part, this may be owing to the minimal mortality caused by the storm; only an estimated 41 fatalities were reported in comparison to the 1 200 plus deaths attributed to Hurricane Katrina.4 Rapid response by local and state governments to the needs of citizens affected by the storm is likely to have prevented some morbidity and psychological stress. Mobile medical units staffed by local health department personnel, DVA personnel, CDC PHAs, and USPHS officers played an integral role in finding and providing care to persons with medical conditions who were unable to access medical care locally caused by or exacerbated as a result of conditions produced by the storm. Intervention likely minimized the number of patients whose condition may have otherwise deteriorated to a life-threatening or fatal situation. Collaboration between federal, state, and local agencies facilitated the delivery of care to thousands of persons affected by Hurricane Wilma.
The active illness and injury surveillance implemented on the mobile medical units was similar to that used in responses to hurricanes Katrina and Rita.6 These surveillance activities served multiple functions during this response that included prompt evaluation of trends in diagnoses, assessing unmet needs related to medication refills, and informing mobile van deployment or redeployment. It has been demonstrated that less than 10 percent of persons arriving at a housing shelter following a disaster are in need of medical care.7 This was also true for our convenience sample; most of the health issues encountered were not related to Wilma and although acute care needs were addressed in some patients, far more presented for normal health maintenance needs (blood pressure checks, glucose checks, medication refills) that might have been prepared for prehurricane relief. A large percentage of patients had chronic diseases. Following disasters, it is these groups of persons that become unable to manage their chronic conditions due to disruptions in the medical care system.8 For example, many health-related facilities such as clinics and pharmacies remained closed for 1 to 2 weeks after Hurricane Wilma, and home healthcare services were also disrupted. Indeed, several cases of severe hypertension and hyperglycemia were identified on the mobile units following Wilma. Telephone service was also interrupted for extended periods, which made it difficult or impossible for many individuals to request needed medical or social assistance. Social services personnel working with the medical units were able to link persons to temporary housing, elderly care services, and mental health services. Mobile unit staff participating in the Hurricane Wilma response were able to reach a large number of persons with acute and chronic medical, mental health, and social services needs as they arose in the days after the event. Without these interventions, it is likely that many of the chronic medical conditions would have progressed to more severe conditions requiring emergency department visits or even hospitalization, resulting in further stress on limited medical resources already overwhelmed by the disaster.
Priority was given to developments housing elderly persons owing to the concern regarding limited mobility due to the loss of electricity resulting in inoperable elevators, limited lighting, and the inability to recharge power-assisted wheelchairs and other devices. Door-to-door visits conducted by mobile van staff concurrent with the provision of medical care on the mobile vans identified persons in medical need who were not otherwise able to present for care. Other health needs such as the need for food, water, medication refills, and assistance with ambulating were identified and fulfilled through these visits as well. The needs of the elderly during this and another disasters differ from those of younger populations and require specialized attention and response that may include door-to-door visits.
This is one of few reports to describe the use of mobile medical units to provide medical care and to gather medical surveillance information during hurricane relief efforts in the United States. Provision of medical care and medical surveillance using a mobile medical response effort should be considered for natural or manmade disasters where there is limited ability of individuals to access centralized facilities due to physical disabilities, fuel shortages, limitations in public transportation, or medical quarantine. These results are based on a convenience sample of persons who presented to or were contacted by the staff of the mobile medical units, and thus the findings may not represent other populations affected by this hurricane. Despite the sampling method used, the race/ethnicity distribution of this sample mirrors that of the US Census Bureau 2004 Community Survey for Broward County.8 This disaster response relied upon the functioning infrastructure of the local health department and emergency medical services. These activities may be difficult to coordinate in situations where a breakdown in the public health infrastructure occurs, such as was demonstrated after Hurricane Katrina.8,10
The Hurricane Wilma response demonstrated the critical role of the state and local health departments in organizing the disaster response effort. Equipped with knowledge of health, socioeconomic, and social demographics of their communities, the BCHD was able to coordinate with the county Emergency Operations Center to identify the highest priority areas for mobile medical unit deployments. The BCHD expended considerable effort in trying to locate, in this emergency situation, the proper persons to arrange formal agreements for use of the mobile medical units. Ideally, advance agreements should be made with organizations that operate and maintain mobile medical units for their use during disaster response. This type of coordination will prove critical in future disaster events that may threaten the health of communities such as pandemic influenza, bioterrorist events, or additional natural disasters. The use of properly staffed mobile medical van units may facilitate dispensing methods, such mass vaccination, and antibiotic stockpile distribution. Local, state, and federal public health agencies should consider the use of mobile medical clinics in their disaster preparedness planning and emergency response.
Contributor Information
Melanie M. Taylor, Medical Epidemiologist, United States Public Health Services Commissioned Corps, Rockville, Maryland, and Division of STD Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention, Atlanta, Georgia
William S. Stokes, Deputy Team Commander, Assistant Surgeon General, United States Public Health Services Commissioned Corps, and Director, National Toxicology Program Interagency for the Evaluation of Alternative Toxicological Methods, National Institute of Environmental Health Sciences, National Institutes of Health, Research Triangle Park, North Carolina
Ronald Bajuscak, Response Team Commander, National Consultant for Oral Medicine/Pathology, United States Public Health Services Commissioned Corps, Rockville, Maryland.
Mary Serdula, Medical Epidemiologist, United States Public Health Services Commissioned Corps, Nutrition Branch, Division of Nutrition, Physical Activity and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Division of Nutrition and Physical Activity, Centers for Disease Control and Prevention, Atlanta, Georgia.
Karen L. Siegel, Team Leader, United States Public Health Services Commissioned Corps, and Senior Staff Specialist, National Institutes of Health, Physical Disabilities Branch (a collaboration between the National Institute of Child Health and Human Development and the NIH Clinical Center), Bethesda, Maryland
Brian Griffin, Ready Responder, United States Public Health Services Commissioned Corps, National Health Service Corps, Health Resources and Services Administration, Philadelphia, Pennsylvania.
Jeffrey Keiser, Deputy Administrator, Broward County Health Department, Florida Department of Health, Ft Lauderdale, Florida.
Lisa Agate, HIV/AIDS Program Director, Broward County Health Department, Florida Department of Health, Ft Lauderdale.
Aaron Kite-Powell, Surveillance Epidemiologist, Bureau of Epidemiology, Florida, Department of Health, Tallahassee.
David Roach, Administrator, Broward County Health Department, Florida Department of Health, Ft Lauderdale.
Nancy Humbert, Deputy Secretary for Health, Florida Department of Health, Tallahassee.
Kristin Brusuelas, Senior Management Official, Office of the Director, Centers for Disease Control and Prevention, Atlanta, Georgia.
Sam S. Shekar, Assistant Surgeon General, United States Public Health Services Commissioned Corps, and Director of Clinical Research Grants, Office of Extramural Research, National Institutes of Health, Bethesda, Maryland
REFERENCES
- 1.National Oceanic and Atmospheric Administration’s National Weather Service. http://www.srh.noaa.gov/mfl/events/?id=Wilma Published December 1, 2005. Accessed February 28, 2006.
- 2.Broward County Board of County Commissioners. Community update, November 2005. Broward County continues to recover from Hurricane Wilma. http://www.broward.org/enews/communityupdate/november05.htm Published November 2005. Accessed March 15, 2006.
- 3.Office of Electricity Delivery and Energy Reliability (OE). U.S. Department of Energy. Gulf Coast Hurricanes Situation Report #34, November 2, 2005. http://www.oe.netl.doe.gov/docs/gulf_coast/gulf_110205-1500.pdf Published November 2, 2005. Accessed March 15, 2006.
- 4.Ragan P, Schulte J, Nelson S. 2004-2005 Florida hurricane mortality [abstract]. Presented at: Council of State and Territorial Epidemiologists 2006 Annual Conference; June 4–8, 2006; Anaheim, California. [Google Scholar]
- 5.National Oceanic and Atmospheric Administration’s National Weather Service. http://www.srh.noaa.gov/data/NHC/TWSAT Published October 30,2005. Accessed February 28, 2006.
- 6.Centers for Disease Control and Prevention. Injury and illness surveillance in hospitals and acute-care facilities after hurricanes Katrina and Rita—New Orleans area, Louisiana, September 25-October 15,2005. MMWR. 2006;55:35–38. [PubMed] [Google Scholar]
- 7.Mattox K Hurricanes Katrina and Rita: role of individuals and collaborative networks in mobilizing/coordinating societal and professional resources for major disasters. Crit Care. 2006;10:205–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Greenough PG, Kirsch TD. Public health response-assessing needs. N Engl J Med. 2005;353:1544–1546. [DOI] [PubMed] [Google Scholar]
- 9.United States Census Bureau. American Community Survey. Broward County, Florida. http://factfinder.census.gov Published 2005. Accessed May 19,2006.
- 10.Centers for Disease Control and Prevention. Surveillance for Illness and Injury After Hurricane Katrina—New Orleans, Louisiana, MMWR. September 8–25, 2005. 2005;54:1018–1021. [PubMed] [Google Scholar]