

Abstract
Background:
Parafalcine subdural empyema (SDE) is a rare entity consisting of pus accumulating below the longitudinal sinus, between the falx cerebri and the arachnoid layer covering the medial surface of the cerebral hemisphere. Its treatment strategy is controversial, but most clinicians have the general belief that appropriate treatment consists of prompt surgery combined with long-term antibiotic therapy. Nevertheless, six reports published in the 1980s provided evidence that antibiotic therapy alone is a safe and suitable option. The treatment strategies and outcomes of the 31 well-described cases previously published, in addition to our own, are discussed.
Case Description:
We report a 21-year-old female with a right-side parafalcine SDE who presented with fever, headache, generalized tonic-clonic seizures, and contralateral hemiparesis 3 weeks after undergoing sinonasal surgery. Despite clinical symptoms almost entirely abating after starting treatment with broad-spectrum antibiotics, magnetic resonance imaging performed during the 2nd and 3rd weeks showed progressive enlargement of the interhemispheric collection (from 4 cm3 to 30 cm3). We reflect on the treatment strategy chosen for this patient, who experienced a total recovery.
Conclusion:
A nonsurgical strategy for parafalcine SDE might be contemplated for patients with a good clinical condition and no major midline shift on neuroradiological studies, given their usual indolent course and the relative difficulty in reaching the interhemispheric fissure. Conversely, surgery should be contemplated when the collection significantly enlarges despite antibiotic therapy. When surgical drainage is added to antibiotics, broad- range 16S ribosomal DNA polymerase chain reaction of the empyema is recommended to identify the causative organism as pus cultures are usually sterile.
Keywords: 16S ribosomal DNA polymerase chain reaction, Antibiotic therapy, Interhemispheric empyema, Parafalcine subdural empyema, Surgery

INTRODUCTION
Subdural empyema (SDE) is a rare but potentially life-threatening disease consisting of a pyogenic infection in the pre-formed space between the inner surface of the dura mater and the outer surface of the arachnoid layer. Purulent collections generally accumulate on top of brain convexity,[1,7] but their location between the falx cerebri and the medial surface of the cerebral hemisphere is quite a rare phenomenon.[4,14,30] Contrary to the typical convexity SDEs, the tendency of pus to extend along the length of the falx below the longitudinal sinus and bridging veins makes parafalcine, or interhemispheric, SDEs relatively difficult-to-reach collections.
The surgical challenge posed by parafalcine SDEs, along with the controversy regarding their treatment strategy,[32] piqued our interest in gathering the current knowledge on this topic after managing a patient with such a rare illness. A thorough review of the literature yielded 31 well-detailed case reports of parafalcine SDEs [Table 1].[1-3,5,6,8-11,13-17,19,23-27,29,31,35] Treatment strategies and outcomes of these cases and our own are discussed.
Table 1:
Parafalcine subdural empyemas from the CT era to the present*.

CASE DESCRIPTION
A 21-year-old female came to the emergency room with fever, headache, generalized tonic-clonic seizures, and left-side hemiparesis. Her Glasgow Coma Scale score on admission was 15 and she had no signs of meningeal irritation. Three weeks earlier she had undergone endoscopic sinonasal surgery, and the day before hospital admission, her ear-nose- throat surgeon prescribed oral antibiotics for acute sinusitis. No cerebrospinal fluid (CSF) fistula was noticed. On admission, her body temperature was 39°C, and serological examination revealed an increased white blood cell (WBC) count (13.510/mm3) with neutrophilia (12.680/mm3) and elevated C-reactive protein (194.80 mg/L). Non-enhanced cranial computed tomography (CT) scan was considered normal by emergency physicians [Figure 1a], so they decided to do a lumbar puncture. CSF count, protein, and sugar levels were 210 WBC/mm3 (polymorphonuclear cells: 75%), 101.2 mg/dl, and 54 mg/dl (53%), respectively. Despite no organisms being identified with CSF Gram stain, meningoencephalitis was suspected, and ceftriaxone and vancomycin were started. The following day, a retrospective assessment of the admission CT scan disclosed a laminar extracerebral collection adjacent to the falx [Figure 1a]. A definitive diagnosis of interhemispheric SDE was established using magnetic resonance imaging (MRI) [Figure 1b]. The small subdural collection (4 cm3) along the right side of the falx was found to be hyperintense on diffusion-weighted imaging (DWI) and with low signal intensity on apparent diffusion coefficient (ADC) [Figure 1b3-b4]. Moreover, hydro-aerial levels in the maxillary and fontal sinuses confirmed acute sinusitis. No signs of venous sinus thrombosis were observed.
Figure 1:

Preoperative neuroradiological studies. (a) Computed tomography scan performed the day of admission shows a hypodense laminar collection along the right side of the falx (arrow). (b) Magnetic resonance imaging (MRI) performed the following day. Axial (b1) and coronal (b2) T1 images confirm a frontoparietal interhemispheric collection without any mass effect. Collection shows high signal intensity on diffusion-weighted imaging (b = 1000 s/mm2, b3) and reduced water diffusion in apparent diffusion coefficient map (b4). (c) Study performed during the 2nd week of antibiotic therapy. T1-weighted, contrast-enhanced MRI (c1-c3) shows enlargement of the interhemispheric collection. c4: T2-weighted MRI demonstrates a hyperintense collection. (d) MRI performed during the 3rd week. d1-d3: Additional enlargement of the collection is demonstrated. d4: Fluid attenuated inversion recovery MRI demonstrates hyperintense areas in the brain adjacent to the collection (arrows).
Suspecting an interhemispheric SDE of nasosinusal origin, the patient was treated with broad-spectrum antibiotics including cefepime, metronidazole, and vancomycin. The last was later substituted for linezolid. She experienced progressive clinical improvement except for two episodes of the left leg focal seizures, which resolved after a second anti-epileptic drug was administered. Two weeks after admission, the patient’s fever, headache, and seizures had completely resolved, and the left hemiparesis had noticeably improved. Nevertheless, control MRI demonstrated a notable enlargement of the subdural collection [22 cm3, Figure 1c], and thus we were consulted about the possibility of surgical drainage. Given the good clinical situation of the patient, our recommendation was to continue with the pharmacological treatment alone. Cultures of CSF and blood were both negative, as well as serologic markers for hepatitis A, B, and C. Laboratory parameters continued to improve (normal WBC count and notable decrease of C-reactive protein to 15.9 mg/L) as did the clinical situation, except for the left foot paresis. Nevertheless, the MRI performed during the 3rd week showed an additional enlargement of the parafalcine collection [30 cm3, Figure 1d]. In addition, hyperintensity in the underlying brain on T2/fluid attenuated inversion recovery sequences pointing to a possible cerebritis was also observed [Figure 1d4]. At this point, we took the decision to operate on the patient despite having uncertainties given her good clinical condition.
A large right parasagittal frontoparietal craniotomy was performed [Figure 2]. After opening the dura mater, we found brain swelling, so the inter-hemispheric fissure could only be reached between two frontal bridging veins. We found easily-drainable white pus, a finding that contrasts with the general belief that pus tends to organize in the course of empyema, making delayed surgeries more difficult. The parafalcine compartment was repeatedly washed out with antibiotic solution (gentamicin and vancomycin). No drainage tubes were left in situ. Empyema material was processed for routine aerobic/anaerobic detection, revealing no growth. Nevertheless, amplification of bacterial 16S ribosomal DNA (rDNA) with polymerase chain reaction (PCR) demonstrated Prevotella oris, a Gram- negative, anaerobe commonly found in the oropharyngeal mucosa. Immediately following surgery, the patient developed a slight weakness in the left arm, which, as well as her preoperative lower limb paresis, completely resolved with rehabilitation therapy. Intravenous antibiotic therapy was extended for 4 weeks after surgery, but linezolid was suspended when the causative bacteria were identified. Based on her good clinical and radiological evolution, she was then treated with oral antibiotics (levofloxacin and metronidazole), which lasted 3 weeks until the follow-up MRIs demonstrated complete resolution of the subdural collection [Figure 3]. The patient was discharged completely asymptomatic from hospital 5 weeks after surgery.
Figure 2:
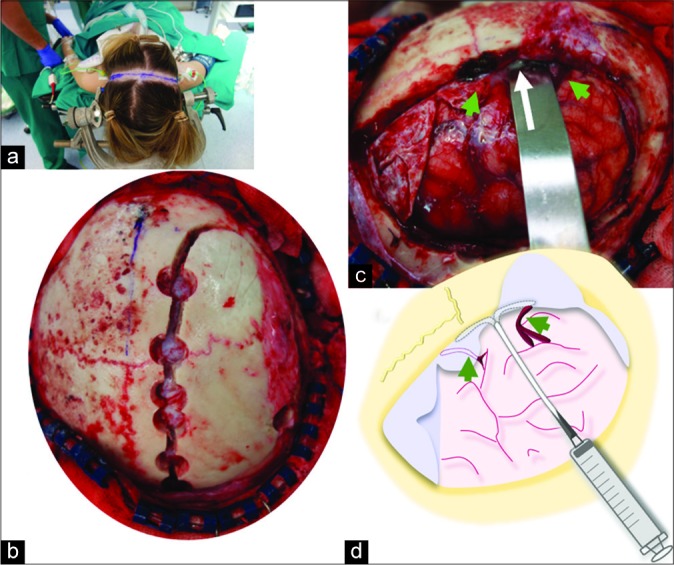
Operative photographs. (a) The patient is placed in the supine position. A bicoronal skin incision was performed. (b) A large right parasagittal frontoparietal craniotomy was performed. (c) Following dura opening, a swollen brain was found. White liquid pus (arrow) was drained between two bridging veins (green arrowheads). (d) The subdural compartment was washed out, anteriorly and posteriorly, between the two bridging veins (green arrowheads) with saline and antibiotics using a soft rubber catheter.
Figure 3:

Postoperative neuroradiological studies. (a) Computed tomography scan performed the day after surgery shows a notable reduction of the interhemispheric collection. (b-d) Follow-up magnetic resonance imaging (MRIs) demonstrate progressive reduction of the collection (asterisk) along the right falx, which completely disappeared in the 7th week after surgery (d). Hyperintense areas of the adjacent brain on T2-weighted MRI (b3, arrows) also resolved in the last MRI study (d3).
DISCUSSION
Nowadays, most clinicians have the general belief that most appropriate treatment of SDE is prompt surgery combined with long-term antibiotics.[1,32] This idea is probably rooted in the pre-antibiotic era, when surgery was the only possible therapy. Nevertheless, it was the introduction of penicillin in 1944 that significantly reduced mortality from almost 100% to 35%.[12] The second decisive factor that additionally improved outcome was the introduction of CT in the 1970s, which allowed an earlier and more accurate diagnosis.[16,18] From that time onward, the mortality rate has progressively decreased to about 5–10% in recent studies,[6,25] thanks to the higher resolution of MRI and to the better diffusion into the central nervous system and effectiveness of new antimicrobial treatments against anaerobic organisms.[10,34] Bright signal of the collection on DWI in addition to low signal on ADC images and elevated lactate on 1H spectroscopy studies strongly suggest the diagnosis of SDE.[1]
The absolute necessity of surgical drainage is uncertain.[15,30] Surgical treatment cannot be justified by possible doubts regarding antibiotic penetration, as angiographic studies have demonstrated an unusual development of meningeal arteries that may bring large quantities of antibiotics to the SDE.[16] The fact that antibiotics do penetrate the SDE is also supported by the high rate of sterile pus cultures.[6,16] Our review of the 32 parafalcine SDEs in the literature [Table 1] shows that pus culture was reported to be positive in only 9 out of the 24 operated cases (37%), a rate similar to that reported in recent series of SDEs.[25,33] Accordingly, nor is surgical indication justified to identify the causative organism and its antibiotic sensitivity unless new methods of microbiological diagnosis are employed, such as broad-range 16S rDNA PCR.[21] To the best of our knowledge, our case is the first SDE in which this novel technique detecting both viable and nonviable bacteria was used.
Controversy over the treatment strategy of SDEs is even higher for the rare cases located in the parafalcine compartment given the difficulty in reaching the interhemispheric fissure with brain swelling. Even gentle manipulation may aggravate contralateral hemiparesis, as is illustrated by our case. The specific location of these collections below the sagittal sinus and bridging veins implies that less aggressive surgical procedures such as burr holes are not safe unless neuronavigation is used.[31] Craniotomy was the method chosen for all but three parafalcine SDEs [Table 1], in agreement with the general thought that craniotomy allows both, more complete evacuation of pus and brain decompression.[20] Stereotactic-guided drainage has been recently proposed as a surgical option given the relatively difficult-to-reach SDEs.[1] On the other hand, contrary to what can normally be achieved in the typical convexity SDEs, usual extension of pus from the frontal lobe to the occipital area prevents complete surgical drainage. In this series of parafalcine SDEs, postoperative recurrence requiring reoperation was as high as 17%. Another notable difference between parafalcine SDEs and purulent collections on top of the brain convexity is that the clinical presentation of the former seems to be more indolent, possibly due to its limitation by arachnoid adhesions between the junction of the falx and the convexity dura. Retrospective review of 699 patients with SDEs found that those localized in the parafalcine compartment associated the best outcomes.[20] In the present series of 32 parafalcine SDEs, only 2 cases experienced rapid neurological deterioration (cases 29 and 31).[2,29]
Total recovery with empirical antibiotic therapy alone, without specific knowledge of the causal organisms, was reported in 7 parafalcine SDEs. Six of these cases were published from the late 1970s to the late 1980s, coinciding with the development of better antibiotics.[14,15,17,24] Nonetheless, since then, this accepted conservative strategy seems to have been almost forgotten. Of particular significance is that half of these cases had altered levels of patient consciousness, despite this being the major predictor of a poor outcome.[6,28] Total recovery even occurred in one patient reported by Leys et al. who was in a coma [case 7, Table 1].[15] In addition, the case reported by Mauser et al. not only had consciousness impairment but also had experienced a slight growth of the collection (transverse diameter grew from 0.4 cm to 0.6 cm), shown in the CT scan performed in the 3rd week of pharmacological treatment (case 9).[17] This specific finding makes us question whether our patient would also have had a total recovery if we had chosen to continue with the nonsurgical strategy, as enlargement of the collections on MRIs was the major factor that led us to indicate surgery. Nevertheless, our patient experienced a seven-fold volume increase in her collection in 3 weeks. Likewise, a notable size increase despite antibiotic therapy was also the reason to indicate surgery in the cases reported by Kakawa (collection grew from 1 cm, in axial sections, to 2.5 in 5 weeks), Kawano (from 0.5 cm to 2 cm in 2 weeks), and Akhaddar (from 0.5 cm to 2 cm in 1 week).[1,9,10]
Regarding the theoretical longer course of antibiotics and the necessity of strict radiological monitoring that some authors use to reason against conservative treatment, this seems quite a weak argument. Regardless of the treatment strategy, antibiotic therapy lasted around 4–6 weeks in this series of parafalcine SDEs. In our case, a relatively long duration of antibiotics was indicated because neuroradiological alterations were not completely resolved until 7 weeks after the operation. Therefore, the experience accumulated with parafalcine SDEs seems to call into question the absolute need for surgical treatment, particularly in those patients with early improvement with antimicrobial therapy who present a good clinical condition and no major midline shift on neuroradiological studies. Further studies are needed to define a decision tree which would help clinicians decide on the best treatment option for such a rare intracranial infectious disease.
CONCLUSION
The mainstay of treatment for parafalcine SDE is early and long-term antibiotic therapy. The absolute necessity to operate this rare entity was challenged by six reports published in the 1980s. A nonsurgical strategy might be contemplated for patients with a good clinical condition and no major midline shift on neuroradiological studies. On the contrary, surgery should be considered for those cases with a notable volume increase despite antibiotic therapy. When the decision is to associate surgical drainage, broad-range 16S rDNA PCR of the empyema is strongly recommended to identify the causative organism as pus cultures are usually sterile.
Acknowledgments
We are indebted to Crystal Smith and Liliya Gusakova, reference librarians of the National Library of Medicine, National Institutes of Health (Bethesda, MD) for their generous assistance during the process of retrieving some of the original articles used in this study. We are also grateful to George Hamilton for his critical review of the language and style of the manuscript.
Footnotes
How to cite this article: Prieto R, Ortega C. Parafalcine subdural empyema: The unresolved controversy over the need for surgical treatment. Surg Neurol Int 2019;10:203.
Contributor Information
Ruth Prieto, Email: rprieto29@hotmail.com.
Celia Ortega, Email: celia.ortega92@gmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Akhaddar A, editor. Atlas of Infections in Neurosurgery and Spinal Surgery. 1st ed. Switzerland: Springer International Publishing; 2017. Cranial subdural empyemas; pp. 51–64. [Google Scholar]
- 2.Arifianto MR, Ma’ruf AZ, Ibrahim A, Bajamal AH. Interhemispheric and infratentorial subdural empyema with preseptal cellulitis as complications of sinusitis: A case report. Pediatr Neurosurg. 2018;53:128–33. doi: 10.1159/000481512. [DOI] [PubMed] [Google Scholar]
- 3.Baerlocher K, Arregger G, Benini A, Gaspar B, Valavanis A, Schubiger O, et al. Subdural interhemispheric empyema in a 7-year-old boy. Helv Paediatr Acta. 1979;34:583–8. [PubMed] [Google Scholar]
- 4.Bok AP, Peter JC. Subdural empyema: Burr holes or craniotomy? A retrospective computerized tomography-era analysis of treatment in 90 cases. J Neurosurg. 1993;78:574–8. doi: 10.3171/jns.1993.78.4.0574. [DOI] [PubMed] [Google Scholar]
- 5.Borovich B, Braun J, Honigman S, Joachims HZ, Peyser E. Supratentorial and parafalcial subdural empyema diagnosed by computerized tomography. Case report. J Neurosurg. 1981;54:105–7. doi: 10.3171/jns.1981.54.1.0105. [DOI] [PubMed] [Google Scholar]
- 6.Dill SR, Cobbs CG, McDonald CK. Subdural empyema: Analysis of 32 cases and review. Clin Infect Dis. 1995;20:372–86. doi: 10.1093/clinids/20.2.372. [DOI] [PubMed] [Google Scholar]
- 7.Hitchcock E, Andreadis A. Subdural empyema: A review of 29 cases. J Neurol Neurosurg Psychiatry. 1964;27:422–34. doi: 10.1136/jnnp.27.5.422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Inamasu J, Horiguchi T, Saito R, Nakamura Y, Ichikizaki K, Takahashi K, et al. Interhemispheric subdural empyema in a young man. Am J Emerg Med. 2001;19:602–3. doi: 10.1053/ajem.2001.28041. [DOI] [PubMed] [Google Scholar]
- 9.Kagawa R, Shima T, Matsumura S, Okada Y, Nishida M, Yamada T, et al. Primary interhemispheric subdural abscess: Report of a case. No Shinkei Geka. 1989;17:647–52. [PubMed] [Google Scholar]
- 10.Kawano H, Yonemura K, Misumi Y, Hashimoto Y, Hirano T, Uchino M, et al. A case of interhemispheric subdural empyema with sinusitis diagnosed by diffusion-weighted MRI. Rinsho Shinkeigaku. 2005;45:449–52. [PubMed] [Google Scholar]
- 11.Kazemi KA, Pishjoo M, Safdari Z. Interhemispheric subdural empyema in 16 years old boy, a case report. Int J Med Invest. 2015;4:407–9. [Google Scholar]
- 12.Keith WS. Subdural empyema. J Neurosurg. 1949;6:127–39. doi: 10.3171/jns.1949.6.2.0127. [DOI] [PubMed] [Google Scholar]
- 13.Klein O, Freppel S, Schuhmacher H, Pinelli C, Auque J, Marchal JC. Empyèmes sous-duraux de l’enfant: Stratégie thérapeutique. Neurochirurgie. 2006;52:111–8. doi: 10.1016/s0028-3770(06)71205-x. [DOI] [PubMed] [Google Scholar]
- 14.Lalkaka JA, Parikh JM, Nath AR, Meisheri YV, Vengsarkar US, Deshpande DV, et al. Interhemispheric empyema. An unusual form of subdural empyema. J Assoc Physicians India. 1989;37:394–6. [PubMed] [Google Scholar]
- 15.Leys D, Destee A, Petit H, Warot P. Management of subdural intracranial empyemas should not always require surgery. J Neurol Neurosurg Psychiatry. 1986;49:635–9. doi: 10.1136/jnnp.49.6.635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Luken MG, 3rd, Whelan MA. Recent diagnostic experience with subdural empyema. J Neurosurg. 1980;52:764–71. doi: 10.3171/jns.1980.52.6.0764. [DOI] [PubMed] [Google Scholar]
- 17.Mauser HW, Ravijst RA, Elderson A, van Gijn J, Tulleken CA. Nonsurgical treatment of subdural empyema. Case report. J Neurosurg. 1985;63:128–30. doi: 10.3171/jns.1985.63.1.0128. [DOI] [PubMed] [Google Scholar]
- 18.Miller ES, Dias PS, Uttley D. Management of subdural empyema: A series of 24 cases. J Neurol Neurosurg Psychiatry. 1987;50:1415–8. doi: 10.1136/jnnp.50.11.1415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mitsuoka H, Tsunoda A, Mori K, Tajima A, Maeda M. Hypertrophic anterior falx artery associated with interhemispheric subdural empyema case report. Neurol Med Chir (Tokyo) 1995;35:830–2. doi: 10.2176/nmc.35.830. [DOI] [PubMed] [Google Scholar]
- 20.Nathoo N, Nadvi SS, Gouws E, van Dellen JR. Craniotomy improves outcomes for cranial subdural empyemas: Computed tomography-era experience with 699 patients. Neurosurgery. 2001;49:872–7. doi: 10.1097/00006123-200110000-00017. [DOI] [PubMed] [Google Scholar]
- 21.Patel A, Harris KA, Fitzgerald F. What is broad-range 16S rDNA PCR ? Arch Dis Child Educ Pract Ed. 2017;102:261–4. doi: 10.1136/archdischild-2016-312049. [DOI] [PubMed] [Google Scholar]
- 22.Pathak A, Sharma BS, Mathuriya SN, Khosla VK, Khandelwal N, Kak VK, et al. Controversies in the management of subdural empyema. A study of 41 cases with review of literature. Acta Neurochir (Wien) 1990;102:25–32. doi: 10.1007/BF01402182. [DOI] [PubMed] [Google Scholar]
- 23.Ratamess NA. Announcement: New JSCR article format. J Strength Cond Res. 2019;33:1179. doi: 10.1519/JSC.0000000000003174. [DOI] [PubMed] [Google Scholar]
- 24.Rosazza A, de Tribolet N, Deonna T. Nonsurgical treatment of interhemispheric subdural empyemas. Helv Paediatr Acta. 1979;34:577–81. [PubMed] [Google Scholar]
- 25.Salunke PS, Malik V, Kovai P, Mukherjee KK. Falcotentorial subdural empyema: Analysis of 10 cases. Acta Neurochir (Wien) 2011;153:164–9. doi: 10.1007/s00701-010-0695-5. [DOI] [PubMed] [Google Scholar]
- 26.Sammartino F, Feletti A, Fiorindi A, Mazzucco GM, Longatti P. Aspiration of parafalcine empyemas with flexible scope. Childs Nerv Syst. 2016;32:1123–9. doi: 10.1007/s00381-016-3082-6. [DOI] [PubMed] [Google Scholar]
- 27.Saravu K, Kadavigere R, Shastry AB, Pai R, Mukhopadhyay C. Neurologic melioidosis presented as encephalomyelitis and subdural collection in two male labourers in India. J Infect Dev Ctries. 2015;9:1289–93. doi: 10.3855/jidc.6586. [DOI] [PubMed] [Google Scholar]
- 28.Shearman CP, Lees PD, Taylor JC. Subdural empyema: A rational management plan. The case against craniotomy. Br J Neurosurg. 1987;1:179–83. doi: 10.3109/02688698709035302. [DOI] [PubMed] [Google Scholar]
- 29.Shen YY, Cheng ZJ, Chai JY, Dai TM, Luo Y, Guan YQ, et al. Interhemispheric subdural empyema secondary to sinusitis in an adolescent girl. Chin Med J (Engl) 2018;131:2989–90. doi: 10.4103/0366-6999.247213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sogoba Y, Kanikomo D, Coulibaly O, Singaré K, Maiga Y, Samaké D, et al. Nonsurgical treatment of infratentorial subdural empyema: A case report. Case Rep Clin Med. 2013;2:294–7. [Google Scholar]
- 31.Stephanov S, Sidani AH, Amacker JJ. Interhemispheric subdural empyema case report. Swiss Surg. 2001;7:229–32. doi: 10.1024/1023-9332.7.5.229. [DOI] [PubMed] [Google Scholar]
- 32.Stephanov S, Sidani AH. Intracranial subdural empyema and its management. A review of the literature with comment. Swiss Surg. 2002;8:159–63. doi: 10.1024/1023-9332.8.4.159. [DOI] [PubMed] [Google Scholar]
- 33.Venkatesh MS, Pandey P, Devi BI, Khanapure K, Satish S, Sampath S, et al. Pediatric infratentorial subdural empyema: Analysis of 14 cases. J Neurosurg. 2006;105:370–7. doi: 10.3171/ped.2006.105.5.370. [DOI] [PubMed] [Google Scholar]
- 34.Wong AM, Zimmerman RA, Simon EM, Pollock AN, Bilaniuk LT. Diffusion-weighted MR imaging of subdural empyemas in children. AJNR Am J Neuroradiol. 2004;25:1016–21. [PMC free article] [PubMed] [Google Scholar]
- 35.Yüksel MO, Gürbüz MS, Karaarslan N, Caliskan T. Rapidly progressing interhemispheric subdural empyema showing a three-fold increase in size within 12 hours: Case report. Surg Neurol Int. 2016;7:S872–5. doi: 10.4103/2152-7806.194495. [DOI] [PMC free article] [PubMed] [Google Scholar]