

Abstract
Background.
Reducing maternal mortality is a priority in the U.S. and worldwide. Drug-related deaths and suicide may account for a substantial and growing portion of maternal deaths, yet information on the incidence of and sociodemographic variation in these deaths is scarce.
Objective.
We sought to examine incidence of drug-related and suicide deaths in the 12 months after delivery, including heterogeneity by sociodemographic factors. We also explored maternal decedents’ healthcare utilization prior to death.
Study design.
This retrospective, population-based cohort study followed 1,059,713 women who delivered a live-born infant in California hospitals during 2010-2012 to ascertain maternal death. Analyses were conducted using statewide, all-payer, longitudinally-linked hospital and death data.
Results.
A total of 300 women died during follow-up, a rate of 28.33 deaths per 100,000 person-years (p-y). The leading cause of death was obstetric-related problems (6.52 per 100,000 p-y). Drug-related deaths were the second leading cause of death (3.68 per 100,000 p-y), and suicide was the 7th leading cause (1.42 per 100,000 p-y); together, these deaths comprised 18% of all maternal deaths. Non-Hispanic White women, Medicaid-insured women, and women residing in micropolitan areas were especially likely to die from drugs/suicide. Two-thirds of women who died, including 74% of those who died by drugs/suicide, made ≥1 emergency department or hospital visit between their delivery and death.
Conclusion.
Deaths due to drugs and suicide are a major contributor to mortality in the post-partum period and warrant increased clinical attention, including recognition by physicians and Maternal Mortality Review Committees as a medical cause of death. Importantly, ED and inpatient hospital visits may serve as a point of identification of – and eventually, prevention for – women at risk for these deaths.
Keywords: Maternal mortality, poisoning, maternal morbidity, depression, accidental death, opioid overdose
Condensation:
Drug-related and suicide deaths comprised 54 of 300 (18%) post-partum deaths during 2010-2012 in California women, with mortality risk concentrated among socioeconomically disadvantaged and non-Hispanic White women.
Introduction
Reducing maternal mortality is a public health and clinical priority in the United States (US) and worldwide.1,2 However, maternal mortality increased by 26.6% from 2000 to 2014 in 48 U.S. states and Washington, DC.1 These concerning trends have resulted in the development of targeted action plans and safety bundles for clinical care that focus on common causes of pregnancy-related mortality, namely obstetric hemorrhage, severe hypertension in pregnancy, and peripartum venous thromboembolism.3 Moreover, in December 2018, the US Congress passed the Preventing Maternal Deaths Act (https://www.congress.gov/bill/115th-congress/house-bill/1318/text), standardizing definitions of maternal mortality and providing funding for state review committees to track and review maternal deaths.
On the other hand, despite growing evidence that maternal deaths due to drug-related causes (e.g., overdose) and suicide may be nearly as common as these pregnancy-related causes, published estimates of maternal mortality typically exclude these types of “accidental” deaths.1,4,5 Opioid use during pregnancy increased 4- to 8-fold from 2004-2013,6 and opioid overdose deaths among women 25-44 increased by 6.7% between 2014 and 2015 alone.7 Suicide rates, including suicide via drug poisoning, also increased substantially between 2003 and 2015, with some of the largest rate increases among women.8
Only a few publications report incidence of maternal deaths due to drug use or suicide, with most studies limited to a single state.5,9–13 A recent review, published in this Journal, highlighted the critical need for more epidemiological evidence on incidence of maternal drug-related and suicide deaths,4 particularly in light of the current opioid epidemic, rising rates of suicide among women, and the devastating consequences of these deaths for infants, children, and families.
To expand this limited evidence base, we utilized a unique statewide, all-payer, longitudinally-linked hospital and death database from California. Our first objective was to examine incidence of drug-related deaths and suicide in the 12 months after delivery among women with an index delivery in 2010-2012 and to describe heterogeneity in death rates by key sociodemographic factors. Our second objective was to examine incidence of emergency department (ED) visits and hospitalization between delivery and post-partum death to examine whether these health care encounters may serve as opportunities to identify women at risk of drug-related death or suicide.
Materials and Methods
Data and study population
We obtained nonpublic emergency department and inpatient discharge data from the California Office of Statewide Health Planning and Development (OSHPD) on all patient visits to all California-licensed hospitals that included a unique identifier (encrypted SSN) and a California residential zip code.14 We then identified all women aged ≥10 who delivered a live infant in 2010-2012. OSHPD provided information on women in this cohort to the California Department of Public Health Vital Records, which assessed vital status in California death records and provided information on date, underlying cause, and manner of death for all matching decedents who died in the first 12 months after delivery. (Decedents who died out of state, <1% of the total, are excluded.) Hospital and death record datasets were deterministically linked using patient SSN and birthdate, with linkage rates of approximately 98%;15,16 all data obtained and used by the study team were de-identified. This study was approved by the Institutional Review Boards of the California Health and Human Services Agency and the University of California, Merced.
Delivery hospitalizations were identified using Diagnosis-Related Group (DRG) codes, a patient classification system that categorizes hospital admissions into groups based on ICD (International Classification of Diseases) diagnoses, procedures, patient characteristics, and presence of complications; these groups are clinically homogeneous in terms of resource use.17 Consistent with prior literature, delivery admissions were identified using DRG codes 767-768 and 774-775 (vaginal delivery) or 765-766 (Cesarean section).17 To simplify calculations, if a woman delivered more than once during the study period, only the first observed delivery – henceforth referred to as the index delivery – was retained for analysis.
Measures
Causes of death.
Primary outcomes of interest were drug-related deaths and suicide within the 12 months after an index delivery. We also assessed several other leading causes of death, using both the World Health Organization’s definition of maternal deaths18 and prior research19 as guides for classifying major causes of death. Underlying causes of death were ascertained using ICD-10 codes. Drug-related deaths comprised those with ICD-10 codes indicating unintentional drug overdose, drug overdose of undetermined intent, drug-induced diseases, drugs present in the blood, and mental/behavioral disorders due to drugs (see eTable 1).19 Suicide deaths comprised those with codes X60 to X84, Y87.0, or U03, including intentional self-poisoning.20 All other deaths were categorized into obstetric deaths (O00-O99, encompassing obstetric complications and pregnancy-related disease, as defined by the WHO18), circulatory system disease deaths (I00-I99), cancer (C00-C97), other unintentional injuries (V01-V99), homicide (X85-X90, X91, X93-X95, Y00-Y09, or Y87.1), and an “all other causes” category.
Follow-up began on each woman’s date of index delivery and ended at death or 365 days after delivery, whichever came first. The last possible follow-up date was Dec. 31, 2013. Women whose hospital record did not link to state mortality records were presumed alive.
Emergency department and inpatient hospital utilization.
We also examined ED and inpatient hospital utilization among women who died during follow-up. ED/inpatient utilization was defined as the woman’s total number of ED and/or inpatient visits made subsequent to the index delivery but prior to death.
Sociodemographic characteristics.
Sociodemographic factors of interest were measured at each woman’s index delivery and included age (<20 years, 20-35 years, ≥35 years), race/ethnicity (non-Hispanic (NH) White, NH Black, Hispanic, NH Asian/Pacific Islander, or NH other; American Indians were included in the “other” category due to small numbers), insurance status (private, Medicaid, self-pay, or other), and urbanicity of residential zip code.21 Urbanicity was categorized as metropolitan (≥10% of commuting flow was to an urbanized area of ≥50,000 residents), micropolitan (≥10% of commuting flow was to a large urban center of 10,000-49,999 residents), or small town/rural (≥10% of commuting flow was to a small urban center of 2,500-9,9999 residents or to areas outside urban centers).
Statistical analysis
We first examined the data descriptively using frequency statistics. For our first aim, we calculated person-years of follow-up (i.e., the total accumulated time at risk experienced by all individuals in the cohort), number of deaths from each cause of interest, and mortality rates per 100,000 person-years of follow-up (along with associated 95% confidence intervals [95% CIs]) for the cohort. This approach allowed us to accurately calculate death rates despite differing observation start and end times for each individual. We then calculated death rates for overall mortality, as well as for combined drug-related/suicide mortality, according to maternal age, race/ethnicity, insurance status, and urbanicity. Combining drug and suicide deaths accounted for these causes’ overlapping premorbid factors (e.g., psychiatric disorder and substance use) and difficulty in determining intent among overdose decedents;22 it also increased the precision of estimates for these subgroup analyses.
For our second aim, we calculated the percentage of decedents with any ED or hospital visit between index delivery and death, as well as descriptive statistics about the frequency of these visits. All statistical analyses were conducted using Stata 14.0 (StataCorp LP).
Results
Sample characteristics
During the study period (2010-2012), 1,516,073 live births were recorded in California.23–25 Our study, which excluded births that were not the mother’s index delivery during the observation period (n=93,464) and hospital births that lacked a valid patient SSN (n=308,786), included a final population of 1,059,713 births (69.9% of all births), leaving 54,110 births (3.6% of all births) unaccounted for. These births likely occurred outside of state-licensed hospitals, e.g., at home, in a birth center, or in a federal hospital. Demographic characteristics of excluded deliveries are shown in eTable 2; in general, excluded deliveries were more likely than included deliveries to be for younger and Hispanic women and those covered by Medicaid.
Descriptive statistics of the study population are shown in Table 1. On average, mothers were in their late 20s at index delivery, and largely of NH White or Hispanic race/ethnicity. Nearly 60% of deliveries were covered by private insurance, with the majority of the rest covered by Medicaid. Most deliveries (94%) were to mothers living in a metropolitan zip code.
TABLE 1.
Sociodemographic characteristics of study population at index delivery hospitalization, among 1,059,714 women in California, 2010-2012.
| Characteristic | N (%) |
|---|---|
| Age in years | |
| <20 years | 82,986 (7.8%) |
| 20-35 years | 817,198 (77.1%) |
| >35 years | 159,529 (15.1%) |
| Race/ethnicity | |
| N-on Hispanic White | 390,901 (36.9%) |
| Non-Hispanic Black | 74,405 (7.0%) |
| Hispanic | 408,205 (38.5%) |
| Non-Hispanic Asian/Pacific Islander | 136,519 (12.9%) |
| Non-Hispanic other | 49,683 (4.7%) |
| Insurance/payer | |
| Private | 599,980 (56.6%) |
| Medicaid | 420,954 (39.7%) |
| Self-pay | 11,172 (1.1%) |
| Other | 27,607 (2.6%) |
| Urbanicity | |
| Metropolitan | 999,966 (94.4%) |
| Micropolitan | 42,5497 (4.0%) |
| Small town/rural | 17,248 (1.6%) |
Post-partum death rates
A total of 300 women died within one year of follow-up, for an overall mortality rate of 28.33 deaths per 100,000 person-years. Cause-specific deaths and corresponding incidence rates are shown in Table 2. The leading cause of post-partum death was obstetric-related disease, with a total of 69 women dying from direct or indirect obstetric causes (23% of all maternal deaths). Drug-related deaths (n=39) were the second leading cause of mortality. All but two of these deaths were coded as accidental drug overdoses, mostly to unspecified substances (n=20) but some to opioids or other narcotics (n=8) and some to sedatives/hypnotics (n=8). Additional details on the drugs involved were not available from the death records. Post-partum suicides were less common (n=15), but ranked as the seventh leading cause of death. Only one suicide death involved drug poisoning; the rest were included hanging/strangulation (n=9) or firearms (n=3). Together, drug-related and suicide deaths comprised 18% of all post-partum deaths. Two-thirds of these deaths occurred between 6 months and one year post-partum.
TABLE 2.
Causes and associated 12-month incidence rates of post-partum death, ranked in descending order, among women delivering in California, 2010-2012.
| Underlying cause | N deaths | Incidence rate (per 100,000 person-years) | 95% CI around incidence rate |
|---|---|---|---|
| Obstetric complications/disease | 69 | 6.52 | 5.15, 8.25 |
| Drug-related | 39 | 3.68 | 2.69, 5.04 |
| Circulatory system disease | 36 | 3.40 | 2.45, 4.71 |
| Cancer | 34 | 3.21 | 2.29, 4.49 |
| Other unintentional injuries | 33 | 3.12 | 2.22, 4.38 |
| Homicide | 17 | 1.61 | 1.00, 2.58 |
| Suicide | 15 | 1.42 | 0.85, 2.35 |
| All other causes | 57 | 5.38 | 4.15, 6.98 |
Heterogeneity by maternal sociodemographic factors
There was evidence of heterogeneity by maternal sociodemographic factors in the incidence of deaths overall and from drug-related/suicide causes, although precision of these estimates was low due to small numbers of cases in each subgroup (Table 3). Maternal older age, NH Black race, non-private insurance, and residence in a micropolitan zip code were all associated with substantially higher overall mortality risk.
TABLE 3.
12-month incidence of post-partum death (overall and for drug-related/suicide deaths), according to maternal age, race/ethnicity, insurance status, and urbanicity at index delivery, among women delivering in California, 2010-2012.
| Sociodemographic characteristic | Total deaths (N) | Overall mortality rate (per 100,000 person-years) | Rate ratio (95% CI) | Drug-related/ suicide deaths (N) | Drug-related/ suicide mortality rate (per 100,000 person-years) | Rate ratio (95% CI) |
|---|---|---|---|---|---|---|
| Age in years | ||||||
| <20 years | 27 | 32.55 | 1.29 (.85, 1.96) | 5 | 6.03 | 1.23 (0.49, 3.11) |
| 20-35 years | 217 | 26.57 | 1.0 | 41 | 5.02 | 1.0 |
| ≥35 years | 56 | 35.13 | 1.40 (1.03, 1.90) | 8 | 5.02 | 1.03 (0.48, 2.19) |
| Race/ethnicity | ||||||
| Non-Hispanic White | 100 | 25.60 | 1.0 | 30 | 7.68 | 1.0 |
| Non-Hispanic Black | 46 | 61.87 | 2.37 (1.65, 3.42) | 5 | 6.73 | 0.70 (0.25, 1.99) |
| Hispanic | 108 | 26.47 | 0.97 (0.73, 1.29) | 11 | 2.70 | 0.35 (0.18, 0.70) |
| Non-Hispanic Asian/PI | 34 | 24.92 | 0.86 (0.57, 1.32) | 5 | 3.67 | 0.48 (0.19, 1.23) |
| Non-Hispanic other | 12 | 24.17 | 0.93 (0.50, 1.74) | 3 | 6.04 | 0.79 (0.24, 2.58) |
| Insurance/payer | ||||||
| Private | 105 | 17.51 | 1.0 | 14 | 2.34 | 1.0 |
| Medicaid | 162 | 38.51 | 2.20 (1.70, 2.85) | 34 | 8.08 | 3.36 (1.80, 6.28) |
| Self-pay | 10 | 89.60 | 4.57 (2.22, 9.41) | 1 | 8.96 | 3.84 (0.51, 29.19) |
| Other | 23 | 83.38 | 4.86 (3.03, 7.79) | 5 | 18.13 | 7.76 (2.80, 21.56) |
| Urbanicity | ||||||
| Metropolitan | 275 | 27.52 | 1.0 | 44 | 4.40 | 1.0 |
| Micropolitan | 19 | 44.74 | 1.63 (1.00, 2.67) | 8 | 18.83 | 3.74 (1.69, 8.31) |
| Small town/rural | 6 | 34.81 | 1.42 (0.63, 3.19) | 2 | 11.60 | 2.64 (0.64, 10.87) |
For drug/suicide deaths, maternal age and mortality risk were not associated. Compared to NH White women, Hispanic women had significantly lower risk of drug/suicide death (RR=0.35, 95% CI=0.18, 0.70), but associations with other race categories were not significant. Women who used Medicaid to pay for their index deliveries were approximately three times more likely to die by drugs/suicide than women who used private insurance (RR=3.36 [1.80, 6.28]), and women with other insurance had seven-fold increased risk (RR=7.76 [2.80, 21.56]), although this estimate was based on just five deaths. Residence in a micropolitan (vs. metropolitan) area was associated with three-fold higher risk of drug/suicide death (RR=3.74 [1.69, 8.31]).
Emergency department/inpatient utilization
Of all 300 women who died during follow-up, two-thirds (66%) had at least one ED or inpatient visit between their index delivery and death (Mean: 2.2, SD: 3.9). These metrics were higher among the 54 women who died of drug-related causes or suicide. As show in Figure 1, 74% made at least one ED or hospital visit , and 39% made ≥3 visits (Mean: 3.5, SD: 6.4).
Figure 1.
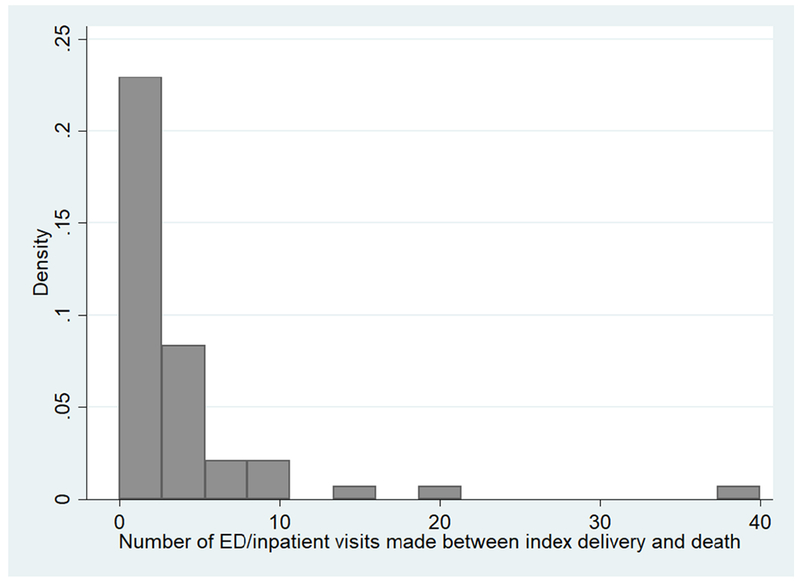
Number of emergency department or inpatient hospital visits made between index delivery and death among women who died post-partum from a drug-related cause or suicide, California, 2010-2012.
Comment
Principal findings of the study
Among more than 1 million women delivering a live infant in the state of California from 2010-2012, we found that drug-related deaths were the second leading cause of post-partum mortality, and that suicide was the seventh leading cause. Together, drug-related causes and suicide were responsible for more than one in six post-partum deaths.
NH White women, and women who were socioeconomically disadvantaged (i.e., had their deliveries covered by Medicaid or self-paid), appeared to be at especially elevated risk for dying from these causes within the year after delivery. We note, however, that NH Black women had the highest overall rates of post-partum mortality, a finding consistent with national data showing very high maternal mortality rates in this group, particularly from cardiovascular causes and homicide.26,27 In line with reports that drug and suicide rates are rising faster in non-metropolitan areas compared to metropolitan ones,28,29 we also found that women who lived in micropolitan areas had elevated risk of drug/suicide mortality risk compared to those in urban areas. Our results clearly indicate that drug-related and suicide deaths are a major contributor to post-partum maternal mortality and warrant increased attention. This work is especially urgent given increasing U.S. maternal mortality rates and related calls for action from the American College of Obstetricians and Gynecologists (ACOG) and the United States Congress.30,31
Comparison with existing literature
Our study is one of only a few to calculate incidence rates for drug-related and suicide deaths in the first year after delivery in a large, diverse state. Currently, data do not exist at the national level linking birth or delivery records with maternal deaths. Individual states often conduct maternal mortality reviews; however, these reviews do not always include deaths due to drugs and suicide.4,5 A handful of published studies using state-specific data have examined pregnancy-associated (i.e., during pregnancy or the first year post-partum) deaths due to drug-related causes and suicide. Estimates of the percentage of pregnancy-associated deaths due to drug-related causes range from 6.1% in Illinois (2002-2013)5 to 22% in Philadelphia (2010-2014);12 for suicide, estimates range from 4-5% in Philadelphia12 and Texas (2011-2012)10 to 13% in Colorado (2004-2012).9 Our findings that drug-related deaths and suicides comprised 13% and 5% of all post-partum deaths, respectively, are consistent with these ranges. Our estimated post-partum mortality rates of 3.7/100,000 for drug-related deaths and 1.4/100,000 for suicides are also consistent with national estimates.13,32
Clinical and research implications
Current research points to a critical need to identify women in the first year (or longer) after delivery who may be at risk of drug overdose or suicide. The overwhelming majority of women in our study who died from drug-related causes or suicide made at least one ED or hospital visit between their delivery and death dates. This observation suggests that ED and hospital visits may serve as a point of identification of—and eventually, intervention on—women at risk for post-partum death. Although examining details of these visits was beyond the scope of this study, this finding warrants further exploration in other samples, including examining the nature of these interactions to identify predictors of maternal death and/or points of intervention.
An obvious intervention point is screening for depression and anxiety among mothers at postpartum and well-baby visits or other health care encounters. The U.S. Preventive Services Task Force and ACOG recommend routine screening for depression and anxiety using validated instruments at postpartum visits,33,34 and some studies show that 80% or more of postpartum and well-child visits include a depression screen for the mother.35,36 However, mothers who die of drugs or suicide in the first year after delivery may not have attended a postpartum or well-baby visit, may not screen positive for depression or anxiety, or may not receive follow-up mental health services due to stigma, lack of access, or time constraints.37,38 Moreover, the stigma and potential repercussions (e.g., removal of the child) of acknowledging substance use during the postpartum period may prevent women from doing so and thus receiving services or treatment.39 Although pregnancy appears to be a motivation for many women to decrease substance use,40 recent research shows that, while perinatal nonfatal opioid overdose rates were lowest in the third trimester, this rate quadrupled by 7-12 months postpartum,41 suggesting that women may fall back into substance use after delivery and not continue to receive treatment.
Strengths and limitations
We could not examine all mothers in California during the study period, as some deliveries occur outside state-licensed hospitals, and not all delivery hospitalizations could be linked to the death record data. This would have primarily affected calculation of mortality rates among low-income Hispanic women, as most delivery hospitalizations missing a unique identifier were to Hispanic women covered by Medicaid (some of whom may have been undocumented immigrants). Whether this would have resulted in under- or overestimating drug-related and suicide mortality in this subgroup is unclear, as mortality from these causes in our analytic sample was lower for Hispanic women but higher for Medicaid-insured women. Relatedly, mortality data for cohort women who died outside of California were not available for this study; we expect this biases our absolute mortality rate calculations downward slightly. We also could not ascertain maternal deaths that occurred during pregnancy, because pregnant women who died without first delivering their infants in a hospital would not be observed in the study dataset. Second, correctly classifying drug-related deaths as intentional or otherwise is challenging, for reasons related to stigma avoidance, legal and religious pressure, and under-resourcing of death investigation systems; the result of such misclassification is usually to undercount suicides.22,42 We view this as an additional rationale for examining drug-related and suicide deaths together as a cause of maternal mortality.
Finally, data from California are not necessarily generalizable to the rest of the U.S., although California generates one-sixth of all live births in the U.S. and is one of the most diverse states in terms of racial/ethnic makeup. However, California is the only state that has experienced a drop in maternal mortality from 2003-2014,1 suggesting that our estimates might provide a lower bound on estimates for the rest of the U.S. On the other hand, this decrease in California’s maternal mortality rate likely resulted primarily from efforts to reduce deaths due to obstetric hemorrhage and preeclampsia, and may not have translated to declines in drug-related and suicide deaths.1
Our study also had important advantages, including its focus on drug and suicide deaths, the use of statewide data from California – a highly diverse, and the most populous, US state – and our analysis of maternal decedents’ ED/hospital utilization prior to death.
Conclusions
In summary, our findings clearly indicate a need for increased research as well as public health and clinical attention to maternal deaths due to drugs and suicide. An important first step would be further documentation of this problem across the U.S., which will require that all state Maternal Mortality Review Committees (MMRCs) categorize deaths due to drugs, suicide, and other non-obstetric causes as medical deaths that fall within the scope of their review, particularly in wake of Congressional legislation providing funding for all states to form MMRCs. Postpartum morbidity from drug abuse, psychological disorder, and suicidal behavior also warrants greater attention, as the deaths observed in the current study likely reflect only the tip of the iceberg of the growing health challenges facing women and their families.
Supplementary Material
AJOG at a Glance:
A. Why was this study conducted?
To describe the incidence of and sociodemographic heterogeneity in post-partum drug-related and suicide deaths.
B. What are the key findings?
Among >1 million women who delivered a live-born infant in California 2010-2012, drug-related deaths were the second leading cause of death (incidence rate of 3.68 per 100,000) over 12 months of follow-up, and suicide was the seventh leading cause.
Medicaid-insured women, those of non-Hispanic White race, and those residing in micropolitan areas were especially likely to die from drug/suicide causes.
C. What does this study add to what is already known?
Our study is one of only a few to calculate incidence rates for drug-related and suicide deaths in the first year after delivery in a large, diverse state.
This investigation also sheds light on sociodemographic variation in post-partum drug-related and suicide death rates and potential opportunities for prevention.
Acknowledgments
Funding:
This project was funded, in part, through National Institutes of Health grant R15 MH113108-01 to S.G.M., as well as through National Institutes of Health grant K01-HL128843 to C.M. Neither sponsor had any role in the study design; collection, analysis, or interpretation of data; writing of the report, or decision to submit the article for publication. No financial disclosures were reported by the authors of this paper.
Abbreviations:
- ED
Emergency department
- ICD-10
International Classification of Diseases, Tenth Revision
- OSHPD
California Office of Statewide Health Planning and Development
- DRG
Diagnostic-Related Groupings
- ACOG
American College of Obstetricians and Gynecologists
- SSN
Social security number
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of interest: The authors report no potential conflicts of interest.
References
- 1.MacDorman MF, Declercq E, Cabral H, Morton C. Recent increases in the U.S. maternal mortality rate: Disentangling trends from measurement issues. Obstet Gynecol 2016;128(3):447–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Perlow JH, Lesmes H. Maternal mortality: time for national action. Obstet Gynecol 2014;123(2 Pt 1):362. [DOI] [PubMed] [Google Scholar]
- 3.D’Alton ME, Main EK, Menard MK, Levy BS. The National Partnership for Maternal Safety. Obstet Gynecol 2014;123(5):973–7. [DOI] [PubMed] [Google Scholar]
- 4.Mangla K, Hoffman MC, Trumpff C, O’Grady S, Monk C. Maternal self-harm deaths: An unrecognized and preventable outcome. Am J Obstet Gynecol 2019. [epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 5.Koch AR, Geller SE. Addressing maternal deaths due to violence: the Illinois experience. Am J Obstet Gynecol 2017;217(5):556–e1. [DOI] [PubMed] [Google Scholar]
- 6.Villapiano NL, Winkelman TN, Kozhimannil KB, Davis MM, Patrick SW. Rural and urban differences in neonatal abstinence syndrome and maternal opioid use, 2004 to 2013. JAMA Pediatr 2017;171(2):194–6. [DOI] [PubMed] [Google Scholar]
- 7.Rudd RA, Seth P, David F, Scholl L. Increases in drug and opioid-involved overdose deaths — United States , 2010 – 2015. MMWR Morb Mortal Wkly Rep 2016;65(50 & 51):1445–52. [DOI] [PubMed] [Google Scholar]
- 8.Hedegaard H, Curtin SC, Warner M. Suicide mortality in the United States, 1999 – 2017. NCHS Data Brief 2018;(330):1–8. [PubMed] [Google Scholar]
- 9.Metz TD, Rovner P, Hoffman MC, Allshouse AA, Beckwith KM, Binswanger IA. Maternal deaths from suicide and overdose in Colorado, 2004-2012. Obstet Gynecol 2016;128(6):1233–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baeva S, Archer NP, Ruggiero K, et al. Maternal mortality in Texas. Am J Perinatol 2017;34(06):614–20. [DOI] [PubMed] [Google Scholar]
- 11.Bronson J, Reviere R. Pregnancy-associated deaths in Virginia due to homicides, suicides, and accidental overdoses compared with natural causes. Violence Against Women 2017;23(13):1620–37. [DOI] [PubMed] [Google Scholar]
- 12.Mehta K, Kramer H, Durazo-Arvizu R, Cao G, Tong L, Rao M. Depression in the US population during the time periods surrounding the Great Recession. J Clin Psychiatry 2015;76(4):E499–504. [DOI] [PubMed] [Google Scholar]
- 13.Gemmill A, Kiang MV., Alexander MJ. Trends in pregnancy-associated mortality involving opioids in the United States, 2007–2016. Am J Obstet Gynecol 2018;220(1):115–6. [DOI] [PubMed] [Google Scholar]
- 14.Office of Statewide Healthcare Planning and Development. MIRCal edit flag description guide: Inpatient data. Sacramento, CA: 2017. [Google Scholar]
- 15.Office of Statewide Healthcare Planning and Development. Appendix C: Linkage counts by match criteria for the Patient Discharge Data. Sacramento, CA: 2010. [Google Scholar]
- 16.Zingmond D Linkage Documentation: Death Statistical Master File linkage to OSHPD databases (PDD, EDD, and ASD) with three year mortality outcomes for all eligible records; years 2005 to 2009. Los Angeles, CA: 2010. [Google Scholar]
- 17.Bardenheier BH, Imperatore G, Gilboa SM, et al. Trends in gestational diabetes among hospital deliveries in 19 U.S. States, 2000-2010. Am J Prev Med 2015;49(1):12–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.World Health Organization. The WHO application of ICD-10 to deaths during pregnancy, childbirth and the puerperium: ICD-MM. 2012.
- 19.Monnat SM. Factors associated with county-level differences in U.S. drug-related mortality rates. Am J Prev Med 2018;54(5):611–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: Final data for 2013. Natl Vital Stat Reports 2016;64(2):1–119. [PubMed] [Google Scholar]
- 21.U.S. Department of Agriculture Economic Research Service. Rural-Urban Commuting Area Codes, version 3.10. Available from: https://ruralhealth.und.edu/ruca [Google Scholar]
- 22.Stone DM, Holland KM, Bartholow B, et al. Deciphering suicide and other manners of death associated with drug intoxication: A Centers for Disease Control and Prevention consultation meeting summary. Am J Public Health 2017;107(8): 1233–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Martin JA, Hamilton BE, Ventura SJ, et al. Births: final data for 2010. Natl Vital Stat Rep 2012;60(1). [PubMed] [Google Scholar]
- 24.Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Mathews TJ. Births: final data for 2011. Natl Vital Stat Rep 2013;62(1):1–69, 72. [PubMed] [Google Scholar]
- 25.Martin JA, Hamilton BE, Osterman MJ, Curtin SC, Matthews TJ. Births: final data for 2011. Natl Vital Stat Rep 2013;62(9):1–68. [PubMed] [Google Scholar]
- 26.Wallace ME, Hoyert D, Williams C, Mendola P. Pregnancy-associated homicide and suicide in 37 US states with enhanced pregnancy surveillance. Am J Obs Gynecol 2016;215(3):364.e1–364.e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. 2018. Available from: http://reviewtoaction.org/Report_from_Nine_MMRCs [Google Scholar]
- 28.Paulozzi LJ, Xi Y. Recent changes in drug poisoning mortality in the United States by urban-rural status and by drug type. Pharmacoeconomics 2008;17:997–1005. [DOI] [PubMed] [Google Scholar]
- 29.Ivey-Stephenson AZ, Crosby AE, Jack, Shane PD, Haileyesus T, Kresnow-Sedacca M. Suicide trends among and within urbanization levels by sex, race/ethnicity, age group, and mechanism of death - U.S., 2001-2015. Morb Mortal Wkly Rep 2017;66(18). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.American College of Obstetricians and Gynecologists. Reverse America’s Rising Rates of Maternal Mortality. 2018. Accessed on April 6, 2019, from: https://www.acog.org/-/media/Departments/Government-Relations-and-Outreach/2018CLCMMRCReversingRate.pdf?dmc=1&ts=20180419T2111374689
- 31.Murray and Senate Democrats call for examination of state efforts to address mounting maternal mortality crisis. 2018. Accessed February 23, 2019, from: https://www.help.senate.gov/ranking/newsroom/press/murray-and-senate-democrats-call-for-examination-of-state-efforts-to-address-mounting-maternal-mortality-crisis
- 32.Palladino CL, Singh V, Campbell J, Flynn H, Gold KJ. Homicide and suicide during the perinatal period: Findings from the national violent death reporting system. Obstet Gynecol 2011;118(5): 1056–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.ACOG Committee Opinion No. 757: Screening for Perinatal Depression. Obstet Gynecol 2018;132(5):e208–12. [DOI] [PubMed] [Google Scholar]
- 34.US Preventive Services Task Force. Interventions to Prevent Perinatal Depression: US Preventive Services Task Force Recommendation. JAMA 2019;321(6):580–7. [DOI] [PubMed] [Google Scholar]
- 35.Lind A, Richter S, Craft C, Shapiro AC. Implementation of routine postpartum depression screening and care initiation across a multispecialty health care organization: An 18-month retrospective analysis. Matern Child Heal J 2017;21(6):1234–9. [DOI] [PubMed] [Google Scholar]
- 36.Fedock GL, Alvarez C. Differences in Screening and Treatment for Antepartum Versus Postpartum Patients: Are Providers Implementing the Guidelines of Care for Perinatal Depression? J Womens Heal 2018;27(9):1104–13. [DOI] [PubMed] [Google Scholar]
- 37.Kallem S, Matone M, Boyd RC, Guevara JP. Mothers’ mental health care use after screening for postpartum depression at well-child visits. Acad Pediatr 2018. November 26 pii: S1876-2859(18)30761-7. doi: 10.1016/j.acap.2018.11.013 [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 38.Prevatt BS, Desmarais SL. Facilitators and barriers to disclosure of postpartum mood disorder symptoms to a healthcare provider. Matern Child Health J 2018;22(1): 120–9. [DOI] [PubMed] [Google Scholar]
- 39.Brogly SB, Link K, Newman A, Children for the KH of R for W and. Barriers to treatment for substance use disorders among women with children. Can J Addict 2018;9(3). [Google Scholar]
- 40.Kendler KS, Ohlsson H, Ph D, et al. The protective effect of pregnancy on risk for drug abuse: A population, co-relative, co-spouse, and within-individual analysis. Am J Psychiatry 2017;174:954–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Schiff DM, Nielsen T, Terplan M, et al. Fatal and nonfatal overdose among pregnant and postpartum women in Massachusetts. Obstet Gynecol 2018;132(2):466–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rockett IRH, Hobbs G, De Leo D, et al. Suicide and unintentional poisoning mortality trends in the United States, 1987-2006: two unrelated phenomena? BMC Public Health 2010;10(1):705. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.