

Abstract
Background:
Acupuncture is effective for reducing body weight; however, evidence in Asian populations is lacking. We performed a systematic review and meta-analysis to evaluate the efficacy of acupuncture for body weight reduction in Asians.
Methods:
The Medline, Embase, Cochrane library, and Chinese databases were searched for relevant studies through October 20, 2018. Publications describing randomized controlled trials (RCTs) comparing acupuncture with other treatments for the reduction of body weight were compiled. Reviewers assessed bias and collected data on trial characteristics and outcomes. The study was conducted based on the reporting items of the guidelines for systematic evaluation and meta-analysis (PRISMA). Review Manager 5.2 software was used to calculate weight mean difference (WMD) and 95% confidence intervals (CIs).
Results:
Twelve RCTs involving 1151 subjects were included. Compared with the control groups, the acupuncture groups exhibited significantly greater reductions of body mass index (BMI) (WMD −1.23 kg/m2; 95% CI −1.94, −0.51) and waist circumference (WMD −2.56 cm; 95% CI −4.43, −0.69). In the subgroup analyses, significant differences in the reduction of BMI and the reduction of waist circumference were observed between the acupuncture and sham acupuncture groups, the acupuncture plus diet and exercise, and the diet and exercise groups, and the acupuncture and no intervention groups, but not between the acupuncture plus exercise and exercise groups.
Conclusions:
Our study demonstrates that acupuncture is effective in the intervention of overweight/obesity in Asians; however, compared with exercise alone, acupuncture combined with exercise had no effect on the BMI or waist circumstance in the short term. Long-term studies are needed to evaluate the efficacy of acupuncture in weight reduction in Asians.
Keywords: acupuncture, Asians, meta-analysis, weight loss
1. Introduction
Obesity is gradually becoming a major public health challenge all over the world. According to World Health Organization (WHO) statistics, in 2016, more than 1.9 billion adults were overweight, and more than 650 million were obese. Between 1975 and 2016, the number of obese people has increased nearly 3 times.[1] The global average body mass index (BMI) of women increased from 22.1 kg/m2 in 1975 to 24. 4 kg/m2 in 2014, and that of men increased from 21.7 kg/m2 to 24.2 kg/m2 over the same period. If current trends continue, the global prevalence of obesity will reach 21% for women and 18% for men by 2025.[2] In China, among 46,239 adults surveyed in 2007 to 2008, the prevalence of overweight or obese was 36.67% and 29.77% in men and women, respectively, which doubled compared with the rate in 2002.[3] In 2014, the obese population of China was the largest in the world; for severe obesity, China is second.[2] Overweight or obesity leads to serious health issues: cardiovascular diseases, including coronary heart disease and stroke, which are the leading cause of death; diabetes mellitus, a global epidemic disease; hypertension; musculoskeletal disorders, especially osteoarthritis; cancers, such as carcinoma of the endometrium and colon cancer; and obstructive sleep apnea (OSA).[4,5] Weight reduction is associated with prolonged survival in type 2 diabetes and with reduced risks of morbidity and mortality,[6] and it can prevent the progression of OSA or even cure mild OSA in obese patients.[7]
The US Food and Drug Administration (FDA) has approved 6 medications, including orlistat, phentermine, lorcaserin, naltrexone/bupropion sustained-release, phentermine/topiramate extended-release, and liraglutide 3.0 mg, for the treatment of obesity[8]; however, their side effects and economic costs inhibit their usage. Acupuncture, as a complementary and alternative therapy, is widely used to reduce body weight. The efficacy and superiority of acupuncture for the treatment of obesity has been assessed and validated in meta-analyses.[9,10]
However, nearly all of these meta-analyses have included Asians and members of other populations. However, due to racial, lifestyle, and other differences, the threshold value of obesity varies among regions. Acupuncture seems to be effective for obesity, but whether it is specifically effective for obesity in Asians is unclear. Thus, we conducted a meta-analysis to evaluate the performance of acupuncture in weight loss in Asians.
2. Materials and methods
2.1. Outcomes measures of efficacy and safety
The primary endpoint of efficacy was the difference in BMI from baseline to the end of the study, and the secondary outcomes were the changes from baseline weight, percentage body fat, waist circumference, and serum lipid levels and the incidence of adverse events.
2.2. Eligibility criteria
Randomized clinical trials (RCTs) that compared acupuncture (electroacupuncture, body, or auricular acupuncture) with placebo, sham acupuncture, lifestyle intervention, or no treatment in the intervention of BMI from baseline to the endpoint were included. If the study was designed as crossover trial, only the first-phase results were analyzed to eliminate carryover effects. According to the WHO, the BMI cut-off of overweight and obesity in adult Asians was more than 23 and 25 kg/m2, respectively.[11] Trials were excluded if they met any the following: they compared different forms of acupuncture; they explored the clinical efficacy of acupoint catgut embedding, acupressure, moxibustion, laser acupuncture, or massage for treatment of overweight or obesity; they provided information on effective rate only between baseline and study end, presenting no BMI data. In addition, studies involving pregnant women or secondary obesity, such as Cushing syndrome-reduced obesity, were excluded.
2.3. Search strategy
The Medline, Embase, Cochrane library, the Chinese Biological Medicine Database (CBM), Wanfang Data, Chinese Technical Periodicals (VIP) and China National Knowledge Infrastructure (CNKI) databases to October 20, 2018 were searched. The search results were not restricted as to language and were limited to humans. The search terms used were acupuncture and overweight, obesity and randomized. The search strategy was adapted according to the demands of the different databases.
2.4. Data extraction
Two reviewers (M.N.X., Y.Z.S.) independently extracted data, which included data on baseline characteristics, interventions, efficacy, and safety outcomes according to the inclusion and exclusion criteria. Discrepancies between the 2 reviewers were resolved through re-review of the original data, consultation between the reviewers, or, when necessary, through consensus via consultation of a third reviewer (L.Z.). In the case of crossover designs, only the data before crossover were extracted.
2.5. Risk of bias
The Cochrane Collaboration's risk of bias tool, which addresses random sequence generation, allocation concealment, blinding of outcome assessors, incomplete data regarding outcome, selective outcome reporting, and other items, was used to assess the bias risk of the RCTs. The risk of bias of each trial was graded as high, low, or unclear. Two authors (L.Z. and Y.L.) assessed the risk of bias; in the event of disagreement, consensus was reached through consultation with a third reviewer (Z.Q.H).
2.6. Data synthesis and analysis
Continuous variables were analyzed using the weighted mean difference (WMD) and 95% confidence interval (CI) to express the size of the effect. If the change of mean and standard deviation (SD) from baseline to the endpoint of the trial were not reported, but the pre and postintervention values were reported, and the following formulas were used to calculate the mean and SD: x change = x post-treatment − x baseline.
 |
where r is the correlation coefficient and is assumed to be 0.4.[12] The statistical software Review Manager version 5.2 (Oxford, UK) was used to analyze the data. Statistical heterogeneity was examined with I 2 tests. A random-effect model was adopted for each outcome. Funnel plots were generated to visually assess publication bias.
2.7. Ethical Approval
Ethical approval was not necessary because the study was a systematic review and meta-analysis, and did not involve animals or humans.
3. Results
3.1. Search results and study characteristics
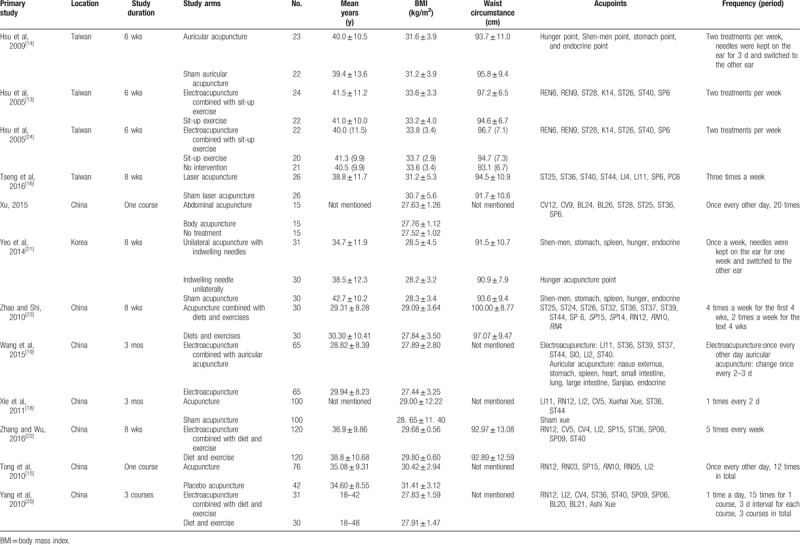
Figure 1 shows the selection flow diagram. According to the search strategies, a total of 1283 records were identified. After reviewing the titles, abstracts, and full texts, 12 articles[13,14,15,16,17,18,19,20,21,22,23,24] were included. The baseline characteristics are shown in Table 1. All of the included trials were performed at a single center. Four studies were from Taiwan,[13,14,16,24] 7 were from China's mainland,[15,17,18,19,20,22,23] and 1 was from Korea.[21] There were 608 subjects in the acupuncture groups, which received auricular acupuncture, electroacupuncture, laser acupuncture, body acupuncture, or abdominal acupuncture, and 543 in the control groups, in which sham auricular acupuncture, sham laser, sham acupuncture, placebo acupuncture, lifestyle intervention (diet, exercise), or no treatment were used. There were 4 trials[14,16,18,21] comparing acupuncture with sham acupuncture, 1 trial[15] comparing acupuncture with placebo acupuncture, 1 trial[17] comparing electro-acupuncture plus laser acupuncture with laser acupuncture, 3 trials[20,22,23] comparing acupuncture plus diet and exercise with diet and exercise, 2 trials comparing acupuncture plus exercise with exercise, and 2 trials[13,24] comparing acupuncture with no intervention. One trial[13] used a crossover design.
Figure 1.
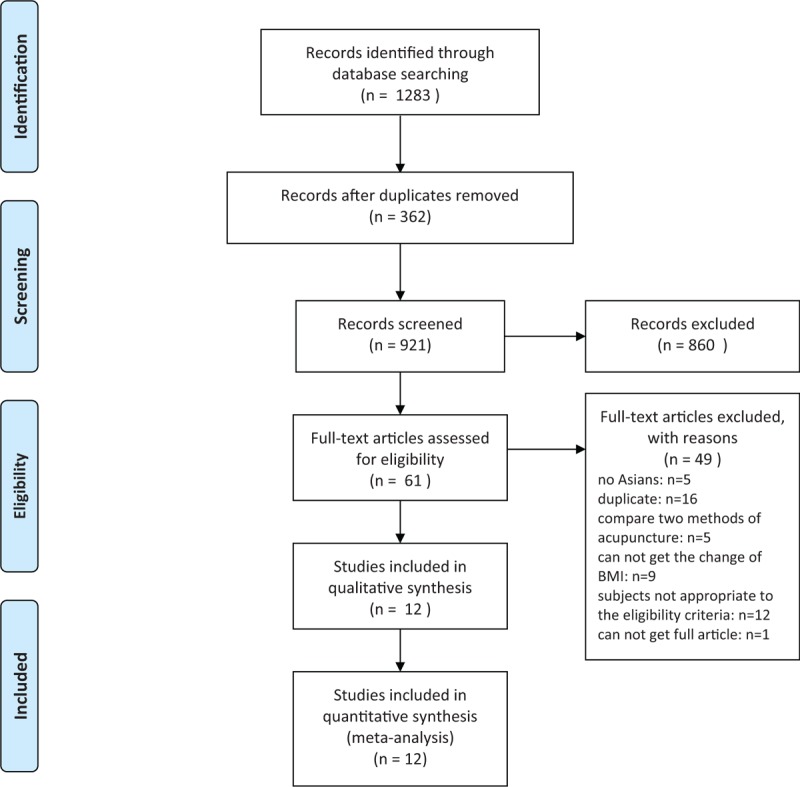
Flow diagram of study selection process.
Table 1.
Baseline characteristics in the meta-analysis.
3.2. Risk of bias assessment
Most of the included articles were evaluated as low quality due to the poor reporting of random sequence generation, allocation concealment, blinding of participants, and personnel or blinding of outcome assessment (Fig. 2).
Figure 2.
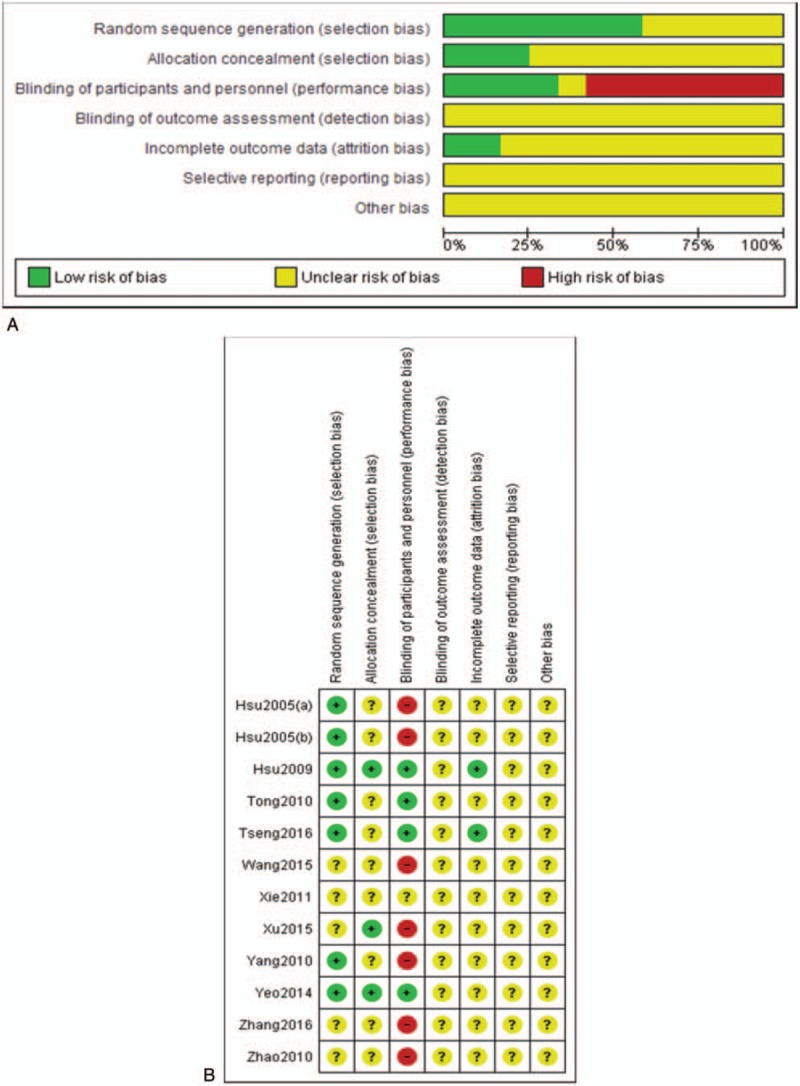
(A) Risk of bias graph; (B) risk of bias summary.
Visual inspection of funnel plots was used to evaluate publication bias (Fig. 3). In the funnel plot of BMI, there was a suggestion of missing studies in the left of the plot, which indicated plausible publication bias.
Figure 3.
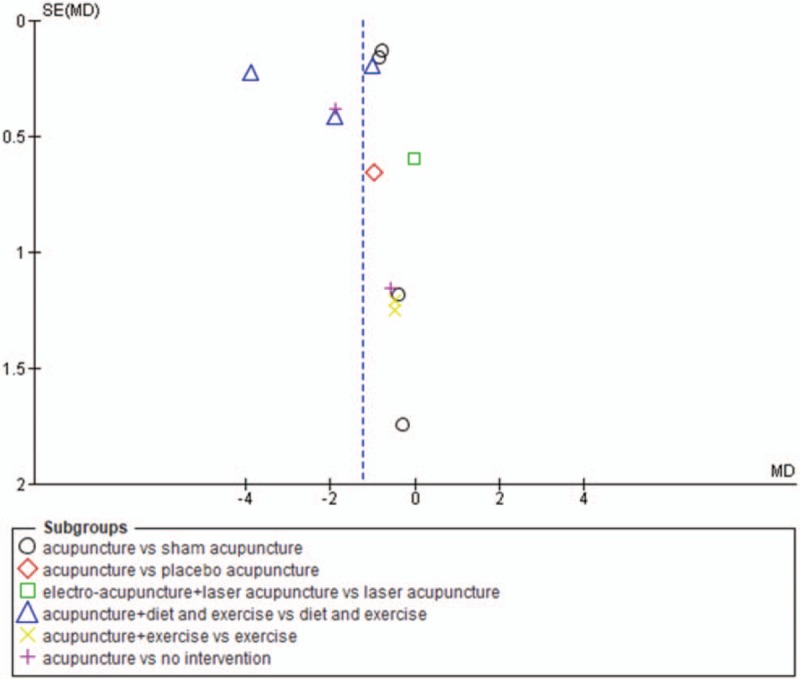
Funnel plot of body mass index (BMI).
3.3. Effect of acupuncture on BMI
The overall efficacy of acupuncture relative to control treatment was evident from a significant difference in the reduction of BMI (WMD −1.23 kg/m2; 95% CI −1.94, −0.51) (Fig. 4). In the subgroup analyses, significant differences in the reduction of BMI were noted between acupuncture and sham acupuncture (WMD −0.80 kg/m2; 95% CI −1.00, −0.60), acupuncture plus diet and exercise, and diet and exercise (WMD −2.27 kg/m2; 95% CI −4.26, −0.29), and acupuncture and no intervention (WMD −1.70 kg/m2; 95% CI −2.59, −0.81). No significant differences were observed in the comparisons of acupuncture with placebo acupuncture (WMD −0.98 kg/m2; 95% CI −2.26, 0.30), acupuncture plus laser acupuncture with laser acupuncture (WMD −0.04 kg/m2; 95% CI −1.21, 1.13), and acupuncture plus exercise with exercise (WMD −0.50 kg/m2; 95% CI −2.20, 1.20).
Figure 4.
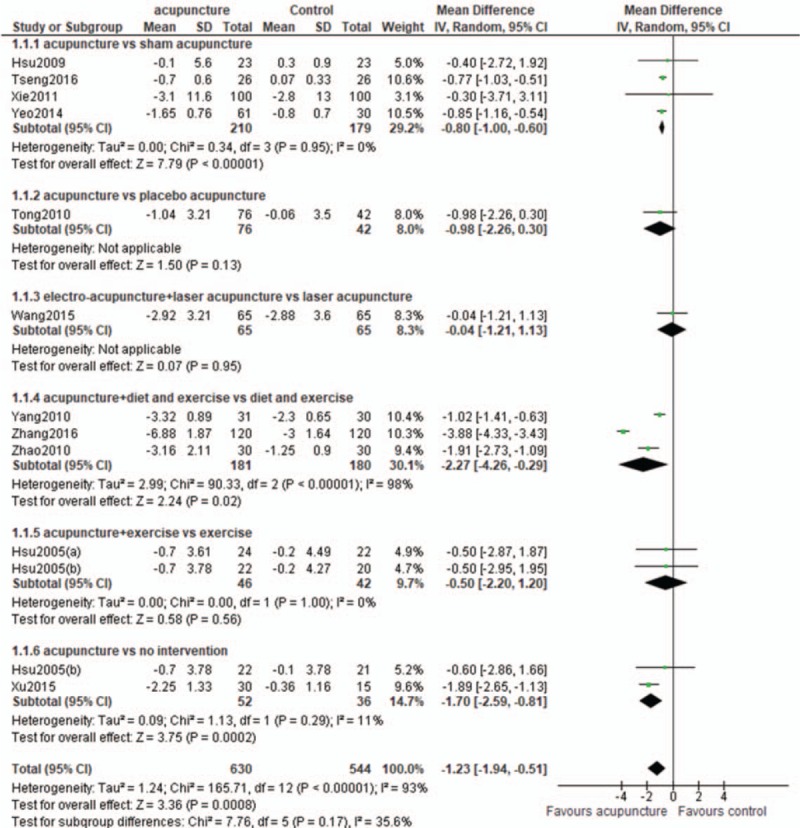
Body mass index (BMI): acupuncture vs control.
3.4. Effect of acupuncture on waist circumference
The overall efficacy of acupuncture relative to control treatment was evident from the significant difference in the reduction of waist circumference (WMD −2.56 cm; 95% CI −4.43, −0.69) (Fig. 5). In the subgroup analyses, there were significant differences in the reduction of waist circumference between acupuncture and sham acupuncture (WMD −3.69 cm; 95% CI −5.01, −2.37), acupuncture plus diet and exercise, and diet and exercise (WMD −4.35 cm; 95% CI −6.16, −2.54), and acupuncture and no intervention (WMD −0.29 cm; 95% CI −0.54, −0.05). There was no significant difference between acupuncture plus exercise and exercise (WMD −1.07 cm; 95% CI −4.29, 2.16).
Figure 5.
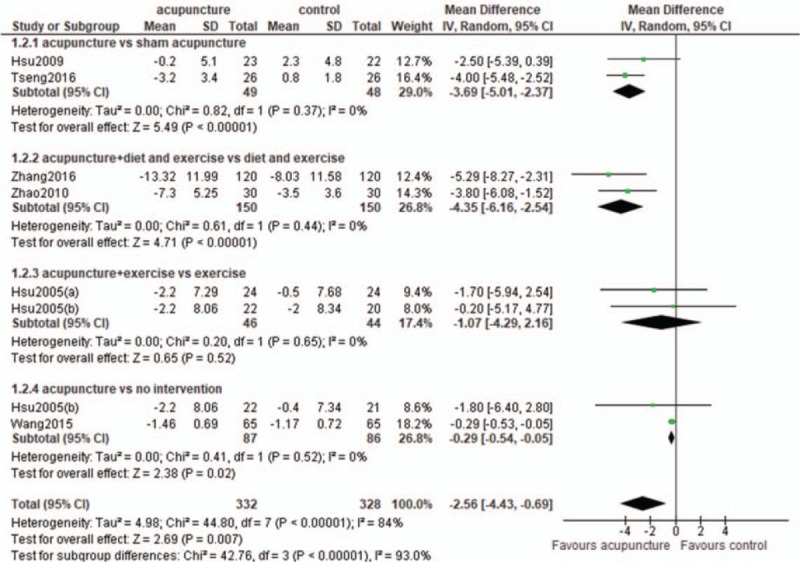
Waist circumference: acupuncture vs control.
3.5. Effects of acupuncture on cholesterol and triglyceride levels
There was no significant difference between the acupuncture and control groups in the reduction of cholesterol (WMD −0.08 mmol/L; 95% CI −0.36, 0.21) or triglyceride (WMD −0.03 mmol/L; 95% CI −0.14, 0.07). Similarly, no significant differences were observed in the subgroup analyses (Fig. 6).
Figure 6.
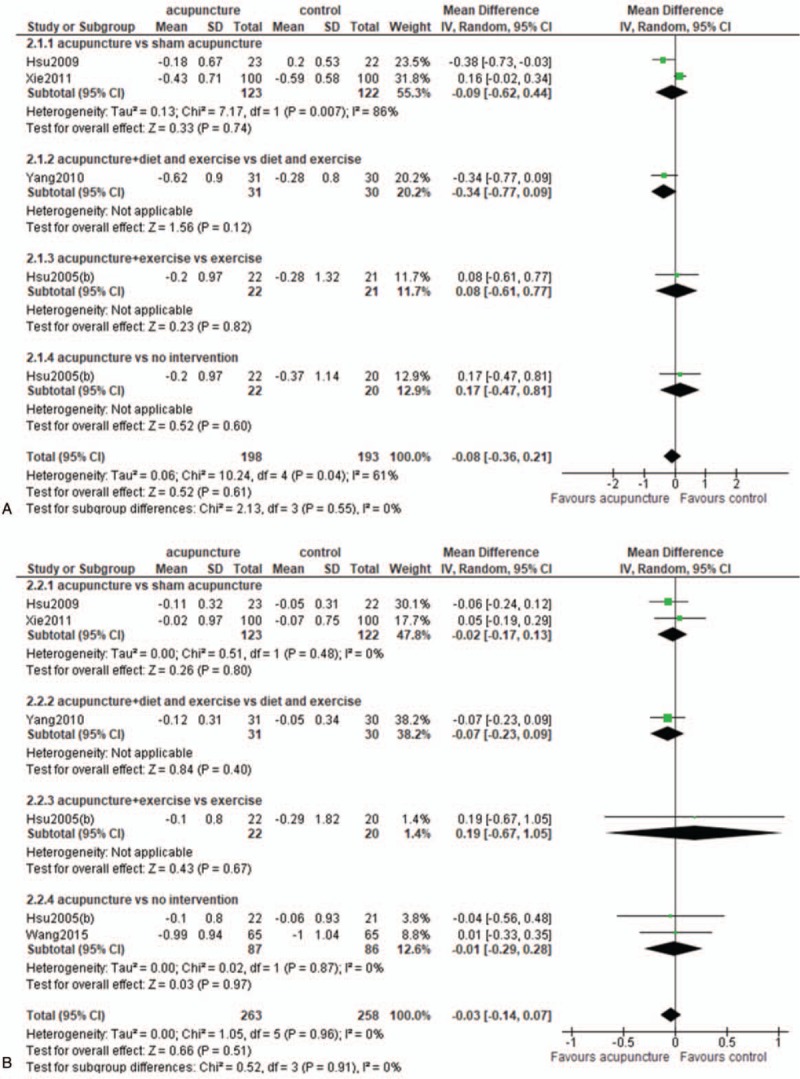
(A) Cholesterol: acupuncture vs control; (B) triglyceride: acupuncture vs control.
3.6. Adverse events
Only 3 studies[13,14,24] reported adverse events. Hsu et al[14] reported that minor inflammation occurred in 1 subject in the acupuncture group, and that mild tenderness occurred in 7 subjects in the acupuncture group and 2 subjects in the sham acupuncture group. Hsu et al[13] reported that electroacupuncture treatment resulted in mild ecchymosis in 2 subjects and abdominal discomfort in 1 patient. Electroacupuncture treatment led to mild ecchymosis in 3 subjects and abdominal discomfort in 1 patient in 1 study.[24]
4. Discussion
To the best of our knowledge, this is the first meta-analysis and systematic review of acupuncture for the intervention of body weight in Asians. Our results demonstrated that relative to sham treatment, acupuncture was effective for the reduction of BMI and waist circumference. However, relative to diet and exercise intervention, acupuncture reduced weight only when it was provided in addition to diet and exercise treatment; no benefit of acupuncture monotherapy over exercise alone was observed. A previous meta-analysis found that acupuncture was effective in reducing BMI in obese subjects[10]; a review made similar conclusions.[25] Clinical studies[26,27] revealed that along with a reduction of BMI, eating desire, hunger feeling, and prospective food consumption were significantly decreased in the acupuncture groups relative to the control groups. The mechanism of the acupuncture-driven inhibition of food intake and body weight gain involves the stimulation of α-melanocyte-stimulating hormone expression and release in the arcuate nucleus of hypothalamus.[28] Our previous study showed that acupuncture led to weight loss through the demethylation of the hypothalamic Tsc1 promoter and through the inhibition of the activity of the mTORC1 signaling pathway.[29] However, Kim et al[9] reported that acupuncture treatment alone was similar to sham acupuncture alone in reducing weight body. Another study found that true acupuncture and sham acupuncture had significant and similar effects in weight loss.[30] The different results among studies may have several causes, such as study variation in intervention duration and the selection of acupoints. The intervention duration in our study was 6 weeks to 3 months; the duration in Kim et al's[9] report was 4 to 12 weeks. The best course of intervention is not yet clear. Furthermore, acupoint selection varied among the different studies, and different combinations of acupoints may produce different effects on weight loss. Presently, it is unclear what combination is optimal for weight loss. Moreover, the similarity of therapeutic effects between acupuncture groups and sham-acupuncture groups has raised the issue of acupoint specificity, which has been intensively discussed. Acupuncture showed its specificity effect in diseases and acupoint, such as Alzheimer disease and mild cognitive impairment patients,[31] regulation of hypothalamic- pituitary-adrenal cortex axis function,[32] and Rangu (KI 2) acupoint.[33] Many brain imaging and other studies have provided evidence of the acupoint specificity of acupuncture, but it is necessary to consider acupoint specificity-related issues, such as sham acupoints and the placebo phenomenon.[34] Whether there is acupoint specificity in the intervention of obesity by acupuncture, and, if so, what the mechanism is need study.
Although differences exist between Asian and Western populations, such as the consumption of more carbohydrate and less protein by Asian than Western populations, acupuncture treatment for weight loss has been found effective when Western and Asian subjects are considered together.[35] Lifestyle interventions for obesity include diet and exercise interventions, which play important roles in the prevention and treatment of obesity.[36,37] However, some studies have found that exercise alone did not lead to reduced weight. A meta-analysis showed that when lifestyle modification was treated as the reference treatment, acupuncture exhibited superior performance compared with no treatment or placebo treatment.[38]
Our results demonstrated that compared with diet and exercise, acupuncture plus diet and exercise can bring greater reductions in weight and waist circumstance; however, relative to exercise alone, acupuncture plus exercise had no effect on the change of BMI or waist circumstance. A previous study reported that diet was superior to total body weight loss, and exercise was beneficial for reducing visceral adiposity.[39] Do these findings indicate that diet and exercise play different roles in the management of overweight/obesity? We speculate that there may be several reasons for the findings of this meta-analysis. First, the frequency of acupuncture in the 2 trials was 2 treatments per week,[13,24] which may be insufficient to detect an effect. In the included trials, auricular needles were maintained on the ear for 3 days[14] or 1 week,[21] and then switched to the other ear; all of the remaining trials except 2 used at least acupuncture 3 times.[13,24] Second, the small sample size might have influenced the results. In the subgroup analysis of acupuncture plus exercise versus exercise alone, 46 subjects were in the treatment group and 44 were in the control group. A small sample size can lead to the inconsistent results and can make it difficult to detect true experimental differences. Furthermore, the risk of error is high, and it is easy to obtain “false-negative” results. Studies with larger sample sizes are needed.
Our results showed that acupuncture had no effects on cholesterol and triglyceride levels in either the main comparison or the subgroup analyses. However, some animal and clinical studies have found that acupuncture can decrease cholesterol and triglyceride levels significantly.[40,41] Cabioğlu and Ergene[42] reported that electroacupuncture intervention lead to decreases in serum total cholesterol and triglyceride levels in obese women, possibly by increasing serum beta-endorphin level. It is not clear whether there are differences between populations from the East and the West. Additional studies should be conducted to evaluate the effects of acupuncture on cholesterol and triglyceride levels.
Regarding the risk of bias, most of the included articles were evaluated as low quality, and plausible publication bias was found, indicating that the methodological quality of the included studies was not satisfactory. More rigorous trials need to be conducted to confirm the effect of acupuncture on weight loss in the future. Only 3 studies reported on adverse effects. Although acupuncture is considered generally safe, studies should report safety-related outcomes.
There are a few limitations with the present meta-analysis. First, the quality of most of the included trials was low, which limits the robustness of the results. Moreover, the duration of treatment was too short to evaluate the long-term efficacy of acupuncture, and most of the studies did not mention long-term follow-up. Weight regain is a common occurrence in any weight loss attempt. It is important to evaluate the long-term efficacy of acupuncture in the treatment of obesity. Clinical randomized controlled studies with long follow-up periods are needed to obtain reliable results. In addition, the frequency, duration, and type of acupuncture treatment were highly variable across studies. Furthermore, adverse effects were reported in only a few studies, preventing a comprehensive evaluation. In addition, the visual inspection of funnel plots indicated that publication bias may exist. Finally, the countries and regions represented in our study were Mainland China, Taiwan region, and Korea; these regions are not fully representative of Asia, and selection bias may have been present, possibly affecting our conclusions. However, we did not identify other studies that met the eligibility criteria except for those from the 3 countries and region. We will pay close attention to research on acupuncture treatment for obesity published in Asian countries. Finally, our meta-analysis did not compare the different styles of acupuncture with control treatment due to the small number of included studies.
5. Conclusions
Our meta-analysis demonstrated that acupuncture was effective as an intervention for overweight/obesity in Asians; however, relative to exercise alone, acupuncture plus exercise had no effect on the change of BMI or waist circumstance. The evidence is weak due to the low quality of the included studies. Long-term, high-quality studies are needed to evaluate the efficacy of acupuncture for weight loss.
Author contributions
Project administration: Lin Zhang.
Resources: Zhiqiong He, Mingmin Xu, Yunzhou Shi.
Supervision: Lin Zhang, Ying Li.
Writing – original draft: Junpeng Yao, Ying Chen.
Lin zhang orcid: 0000-0002-3923-3974.
Footnotes
Abbreviations: BMI = body mass index, CI = confidence interval, OSA = obstructive sleep apnea, RCT = randomized controlled trials, US FDA = US Food and Drug Administration, WHO = World Health Organization, WMD = weighted mean difference.
JY, ZH, and YC contributed equally to this manuscript.
Funding: This work was supported by the National Natural Science Foundation of China [Grant No. 81673803]. Chengdu University of Traditional Chinese Medicine Xinglin scholars program [No. QNXZ2018033].
The authors have no conflicts of interest to disclose.
References
- [1]. World Health Organization. Obesity and overweight: fact sheet. Available at: http://www.who.int/features/factfiles/obesity/en Accessed July 10 2018. [Google Scholar]
- [2]. Collaboration NCDRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016;387:1377–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3]. Yang ZJ, Liu J, Ge JP, et al. Prevalence of cardiovascular disease risk factor in the Chinese population: the 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur Heart J 2012;33:213–20. [DOI] [PubMed] [Google Scholar]
- [4]. Field AE, Coakley EH, Must A, et al. Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Arch Intern Med 2001;161:1581–6. [DOI] [PubMed] [Google Scholar]
- [5]. Fruhbeck G, Toplak H, Woodward E, et al. Obesity: the gateway to ill health: an EASO position statement on a rising public health, clinical and scientific challenge in Europe. Obes Facts 2013;6:117–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6]. Poobalan AS, Aucott LS, Smith WC, et al. Long-term weight loss effects on all cause mortality in overweight/obese populations. Obes Rev 2007;8:503–13. [DOI] [PubMed] [Google Scholar]
- [7]. Tuomilehto H, Seppa J, Uusitupa M, et al. The impact of weight reduction in the prevention of the progression of obstructive sleep apnea: an explanatory analysis of a 5-year observational follow-up trial. Sleep Med 2014;15:329–35. [DOI] [PubMed] [Google Scholar]
- [8]. Srivastava G, Apovian C. Future pharmacotherapy for obesity: new anti-obesity drugs on the horizon. Curr Obes Rep 2018;7:147–61. [DOI] [PubMed] [Google Scholar]
- [9]. Kim SY, Shin IS, Park YJ. Effect of acupuncture and intervention types on weight loss: a systematic review and meta-analysis. Obes Rev 2018;19:1585–96. [DOI] [PubMed] [Google Scholar]
- [10]. Zhang RQ, Tan J, Li FY, et al. Acupuncture for the treatment of obesity in adults: a systematic review and meta-analysis. Postgrad Med J 2017;93:743–51. [DOI] [PubMed] [Google Scholar]
- [11]. World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and its Treatment. Geneva: World Health Organization; 2000. [Google Scholar]
- [12]. Follmann D, Elliott P, Suh I, et al. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol 1992;45:769–73. [DOI] [PubMed] [Google Scholar]
- [13]. Hsu CH, Hwang KC, Chao CL, et al. Effects of electroacupuncture in reducing weight and waist circumference in obese women: a randomized crossover trial. Int J Obes (Lond) 2005;29:1379–84. [DOI] [PubMed] [Google Scholar]
- [14]. Hsu CH, Wang CJ, Hwang KC, et al. The effect of auricular acupuncture in obese women: a randomized controlled trial. J Womens Health (Larchmt) 2009;18:813–8. [DOI] [PubMed] [Google Scholar]
- [15]. Tong JC, Zhang ZQ, Pan Y, et al. Therapeutic effect of acupuncture therapy for simple obesity (Chinese). J Guangzhou Univ Tradit Chin Med 2010;27:579–82. [Google Scholar]
- [16]. Tseng CC, Tseng A, Tseng J, et al. Effect of laser acupuncture on anthropometric measurements and appetite sensations in obese subjects. Evid Based Complement Alternat Med 2016;2016:9365326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17]. Wang KY, Liu ZC, Xu B. Clinical observation on electro-acupuncture combined with ear-acupuncture in treating patients with obesity of stomach-intestine excessive heat type complicated with hyperlipidemia (Chinese). Chin J Tradit Chin Med 2015;30:4513–6. [Google Scholar]
- [18]. Xie CF, Fu WS, Sun J, et al. Standardized plan for acupuncture treatment of simple obesity (Chinese). Chin J Gerontol 2011;31:4751–3. [Google Scholar]
- [19]. Xu Z, Li R, Zhu C, et al. Effect of acupuncture treatment for weight loss on gut flora in patients with simple obesity. Acupunct Med 2013;31:116–7. [DOI] [PubMed] [Google Scholar]
- [20]. Yang J, Xing HJ, Wang SJ, et al. Effect of acupuncture combined with diet and aerobic exercise on BMI and blood lipid levels in patients with simple obesity(Chinese). Li Shen Zhen Med Mater Med Res 2010;21:2367–9. [Google Scholar]
- [21]. Yeo S, Kim KS, Lim S. Randomised clinical trial of five ear acupuncture points for the treatment of overweight people. Acupunct Med 2014;32:132–8. [DOI] [PubMed] [Google Scholar]
- [22]. Zhang SQ, Wu JD. Acupuncture treatment of 120 cases of spleen deficiency and dampness simple obesity (Chinese). Chin Med Herald 2016;22:101–2. 106. [Google Scholar]
- [23]. Zhao LQ, Shi Y. Electroacupuncture combined with diets and exercises in treatment of simple obesity compl icated with excess heat syndrome of stomach and intestine (Chinese). J Anhui Coll Tradit Chin Med 2010;29:33–7. [Google Scholar]
- [24]. Hsu CH, Hwang KC, Chao CL, et al. Electroacupuncture in obese women: a randomized, controlled pilot study. J Womens Health (Larchmt) 2005;14:434–40. [DOI] [PubMed] [Google Scholar]
- [25]. Cho SH, Lee JS, Thabane L, et al. Acupuncture for obesity: a systematic review and meta-analysis. Int J Obes (Lond) 2009;33:183–96. [DOI] [PubMed] [Google Scholar]
- [26]. Pan YTJ, Chen JX, Zhang ZQ, et al. Clinical study on regulation of acupuncture therapy for appetite in obesity patients(Chinese). J Tradit Chin Med Univ Hunan 2010;30:65–7. [Google Scholar]
- [27]. Yao H, Chen JX, Zhang ZQ, et al. Effect of acupuncture therapy on appetite of obesity patients (Chinese). Zhen Ci Yan Jiu 2012;37:497–501. [PubMed] [Google Scholar]
- [28]. Fei W, Tian DR, Tso P, et al. Arcuate nucleus of hypothalamus is involved in mediating the satiety effect of electroacupuncture in obese rats. Peptides 2011;32:2394–9. [DOI] [PubMed] [Google Scholar]
- [29]. Leng J, Xiong F, Yao J, et al. Electroacupuncture reduces weight in diet-induced obese rats via hypothalamic tsc1 promoter demethylation and inhibition of the activity of mTORC1 signaling pathway. Evid Based Complement Alternat Med 2018;2018:3039783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30]. Moffet HH. Sham acupuncture may be as efficacious as true acupuncture: a systematic review of clinical trials. J Altern Complement Med 2009;15:213–6. [DOI] [PubMed] [Google Scholar]
- [31]. Shan Y, Wang JJ, Wang ZQ, et al. Neuronal specificity of acupuncture in Alzheimer's disease and mild cognitive impairment patients: a functional MRI study. Evid Based Complement Alternat Med 2018;2018:7619197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32]. Wang SJ, Zhang JJ, Yang HY, et al. Acupoint specificity on acupuncture regulation of hypothalamic- pituitary-adrenal cortex axis function. BMC Complement Altern Med 2015;15:87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33]. Li A, Li XL, Zhang F, et al. A functional magnetic resonance imaging study of the neuronal specificity of an acupoint: acupuncture at Rangu (KI 2) and its sham point. Intern Med J 2016;46:973–7. [DOI] [PubMed] [Google Scholar]
- [34]. Xing JJ, Zeng BY, Li J, et al. Acupuncture point specificity (Chinese). Int Rev Neurobiol 2013;111:49–65. [DOI] [PubMed] [Google Scholar]
- [35]. Sui Y, Zhao HL, Wong VC, et al. A systematic review on use of Chinese medicine and acupuncture for treatment of obesity. Obes Rev 2012;13:409–30. [DOI] [PubMed] [Google Scholar]
- [36]. Cheng CC, Hsu CY, Liu JF. Effects of dietary and exercise intervention on weight loss and body composition in obese postmenopausal women: a systematic review and meta-analysis. Menopause 2018;25:772–82. [DOI] [PubMed] [Google Scholar]
- [37]. Laskowski ER. The role of exercise in the treatment of obesity. PM R 2012;4:840–4. [DOI] [PubMed] [Google Scholar]
- [38]. Fang S, Wang M, Zheng Y, et al. Acupuncture and lifestyle modification treatment for obesity: a meta-analysis. Am J Chin Med 2017;45:239–54. [DOI] [PubMed] [Google Scholar]
- [39]. Verheggen RJ, Maessen MF, Green DJ, et al. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: distinct effects on body weight and visceral adipose tissue. Obes Rev 2016;17:664–90. [DOI] [PubMed] [Google Scholar]
- [40]. Han M, Sun Y, Su W, et al. The efficacy of acupuncture on anthropometric measures and the biochemical markers for metabolic syndrome: a randomized controlled pilot study. Evid Based Complement Alternat Med 2017;2017:8598210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41]. Shen W, Wang Y, Lu SF, et al. Acupuncture promotes white adipose tissue browning by inducing UCP1 expression on DIO mice. BMC Complement Altern Med 2014;14:501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42]. Cabioğlu MT, Ergene N. Electroacupuncture therapy for weight loss reduces serum total cholesterol, triglycerides, and LDL cholesterol levels in obese women. Am J Chin Med 2005;33:525–33. [DOI] [PubMed] [Google Scholar]