

Abstract
This retrospective study investigated the effectiveness and safety of acupuncture as an adjunctive therapy to topical ibuprofen (TIP) for patients with chronic knee pain (CKP) due to osteoarthritis.
This retrospective study analyzed medical records of 84 patients with CKP due to osteoarthritis. These patients were divided into a treatment group (n = 42) and a control group (n = 42). The patients in the treatment group were treated with acupuncture plus TIP, while the subjects in the control group received TIP monotherapy. The primary effectiveness endpoint was assessed by Western Ontario and McMaster Universities osteoarthritis index (WOMAC). The secondary effectiveness endpoints were evaluated by the numeric rating scale (NRS), 12-item Short FormHealth Survey (SF-12, mainly including mental component summary [MCS], and physical component summary [PCS]), and adverse events. All patients received an 8-week treatment. All endpoints were measured pre-treatment and posttreatment.
The patients who received acupuncture plus TIP showed better effectiveness in both primary endpoint of WOMAC scale (pain, P < .01; function, P < .01; and stiffness, P < .01) and secondary endpoints of NRS (P < .01), and SF-12 (MCS, P < .01; and PCS, P < .01), than patients who received TIP monotherapy. In addition, both groups had similar safety profile.
The results of this study showed that the effectiveness of acupuncture plus TIP may be better than TIP monotherapy for patients with CKP due to osteoarthritis.
Keywords: acupuncture, chronic knee pain, effectiveness, safety, topical ibuprofen
1. Introduction
Osteoarthritis is a chronic and progressive joint disorder, which often affects people over than 60 years old.[1–3] Previous study has reported that it affects 9.6% of men and 18% of women who are more than 60 years old worldwide.[4] This disorder can cause chronic knee pain (CKP), swelling, stiffness, restriction of movement of attacked joints, and eventually result in disability for patients with such condition.[5–7] Many factors can account for this condition, such as aging, genetic factors, obesity, occupation, injury, and so on.[2,7–8] Of them, obesity and age are the most common causes that can result in CKP.[9–11]
Effective clinical treatment, including pharmacological and nonpharmacological interventions, aims to relieve CKP, and to enhance the function and stiffness status for attacked knee joints.[12–15] Of them, oral ibuprofen is often recommended as an effective pain killer for CKP. However, patients often experience lots of severe adverse events if they took it for long term.[16–19] Thus, topical ibuprofen (TIP) is a promising alternative form for patients.[20–22] Unfortunately, its efficacy is also limited for some patients. Therefore, an add-on intervention is still needed for treatment of CKP with TIP.
Acupuncture is one of the most popular alternative therapies for a variety of pain conditions.[23–25] Lots of clinical trials have reported that acupuncture has very satisfied effectiveness for treating pain disorders, especially for CKP due to osteoarthritis.[26–28] However, no study has reported acupuncture as an add-on therapy to TIP for the treatment of patients with CKP due to osteoarthritis. Thus, in this retrospective study, we first investigated the effectiveness and safety of acupuncture plus TIP for the treatment of CKP due to osteoarthritis.
2. Methods
2.1. Ethics approval
This study was approved by the Medical Ethical Committee of First Affiliated Hospital of Jiamusi University and Second Affiliated Hospital of Jiamusi University.
2.2. Sample size calculation
Sample size was calculated based on the change of mean difference of Western Ontario and McMaster Universities arthritis index (WOMAC) score of −14.0 (after 8 weeks treatment), standard deviation of 20.5, with assuming 20% drop-out rate. Thus, we estimated that a total of 84 subjects would be needed for 2 groups, 42 patients in each group with α = 0.5, and β = 0.8, which would show a statistically significant enhancement in total WOMAC score between 2 groups after 8 weeks treatment.
2.3. Study design
A total of medical records of 84 patients were analyzed in this retrospective study. Those patients were allocated into 2 groups: a treatment group (n = 42, received acupuncture plus TIP) and a control group (n = 42, received TIP monotherapy). All medical records were collected from the Orthopedics department of First Affiliated Hospital of Jiamusi University, and Second Affiliated Hospital of Jiamusi University between August 2017 and November 2018. All patients were treated for a total of 8 weeks. After the treatment, all primary and secondary effectiveness endpoints were evaluated.
2.4. Participants
All patients aged 55 to 80 years old with clinically diagnosed of knee osteoarthritis were included. Additionally, all of them experienced knee pain intensity, as measured by numeric rating scale (NRS) ≥4 for more than 6 months. However, patients were excluded if they had received acupuncture, TIP, or medication injection into the attacked knees within 1 month before this study. Additionally, patients were also excluded if the patients were pregnant, breastfeeding, and had a history of knee surgery, tumor and trauma, as well as accepted any other treatments during the study period regardless the acupuncture and TIP.
2.5. Interventions
All patients received ibuprofen cream to the attacked area about 3.0 cm diameter circles, once daily for a total of 8 weeks. In addition, patients in the treatment group also received acupuncture at attacked side acupoints of Yanglinquan (GB34, on the lateral aspect of the lower leg, in the depression anterior and inferior to the head of the fibula), Yinlinquan (SP9, on the lower border of the medial condyle of the tibia on level with the tuberosity of the tibia), Zusanli (ST36, 4 finger widths down from the bottom of your knee cap, along the outer boundary of your shin bone), Dubi (ST35, with knee flexed, below the patella in a depression lateral to the patellar ligament), and extra point Xiyan (with knee flexed, in the depression of the lateral humerus and patellar tendon). The acupuncture treatment was applied 30 minutes each session, 3 sessions weekly for a total of 8 weeks. In each session, patients received 3 manipulations to make sure each manipulation achieved Deqi.
2.6. Effectiveness endpoints
Primary effectiveness endpoint was measured by the WOMAC.[29] This scale consists of 5 items for pain (score range 0–20), 2 for stiffness (score range 0–8), and 17 for functional limitation (score range 0–68).
Secondary effectiveness endpoints were assessed by NRS ranges from 0 to 10,[30] and 12-item Short Form Health Survey (SF-12).[31] It mainly includes mental component summary (MCS), and physical component summary (PCS).[31] Both MCS and PCS range from 0 to 100. In addition, adverse events were also assessed. All primary and secondary effectiveness endpoints were evaluated pretreatment and post the 8-week treatment.
2.7. Statistical analysis
All characteristic and effectiveness endpoints data were analyzed by a professional statistician using SAS package (Version 9.1; SAS Institute Inc, Cary, NC). Mann–Whitney rank sum test or t test was used to analyze the continuous data. Fisher exact test or χ2 test will be used to analyze the categorical data. P < .05 was set as having statistical significance (2-side).
3. Results
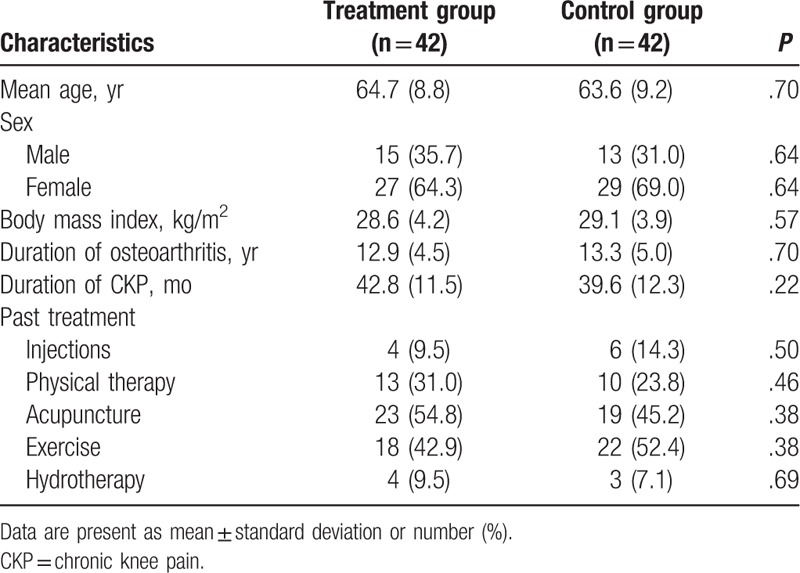
The characteristics of all included patients are summarized in Table 1. There were no significant differences regarding all characteristic values between 2 groups before the treatment.
Table 1.
Characteristics before the treatment.
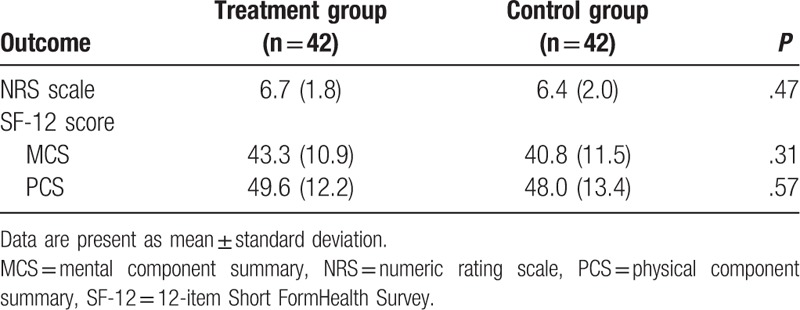
Before the treatment, there were no significant in WOMAC (total, P = .56; pain, P = .56; stiffness, P = .63; function, P = .45, Table 2), NRS (P = .47, Table 2), and SF-12 (MCS, P = .31; PCS, P = .57, Table 3) between the 2 groups.
Table 2.
Comparison of primary effectiveness endpoint pretreatment.
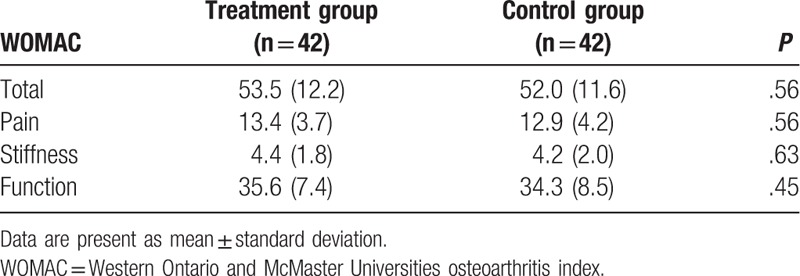
Table 3.
Comparison of secondary effectiveness endpoints pretreatment.
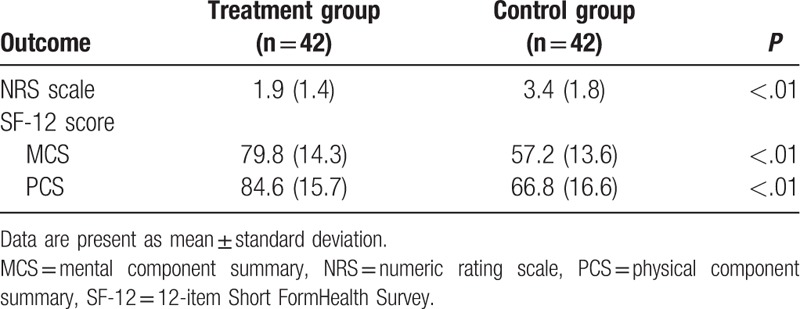
After 8-week treatment, patients in the treatment group had more promising effectiveness in WOMAC (pain, P < .01; stiffness, P < .01; function, P < .01, Table 4), NRS (P < .01, Table 5), and SF-12 (MCS, P < .01; PCS, P < .01, Table 5), than patients in the control group.
Table 4.
Comparison of primary effectiveness endpoint posttreatment.
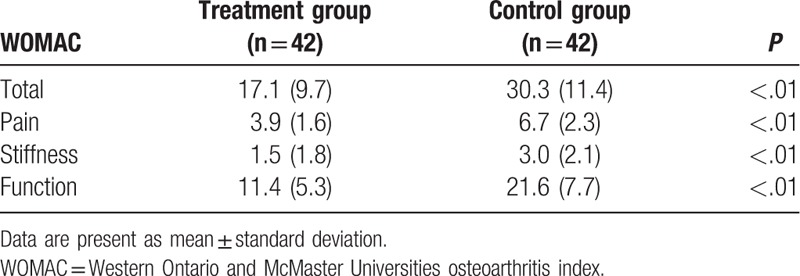
Table 5.
Comparison of secondary effectiveness endpoints posttreatment.
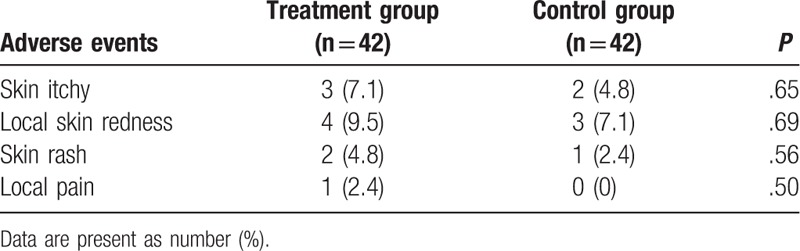
After 8-week treatment, no severe adverse events were recorded in either group (Table 6). No significant differences of all adverse events were found between 2 groups in this study.
Table 6.
Comparison of adverse events.
4. Discussion
The results of this study indicated that elderly patients with CKP demonstrated significant improvements after 8-week treatment. As CKP is the most prevalent symptom in patients with osteoarthritis, and also the leading cause of disability, the identification of adjunctive acupuncture therapy showed effectiveness in decreasing pain intensity of CKP, and also improving the function, and reducing stiffness in patients with osteoarthritis. This improvement was produced by an 8-week acupuncture treatment period of 3 times weekly sessions along with the current conventional modality regime.
To our best knowledge, no study has reported to utilize acupuncture as an adjunctive therapy to TIP for the treatment of CKP. Thus, the present study is the first study to assess the effectiveness and safety of acupuncture plus TIP for patients with CKP due to the osteoarthritis. The results of this study may provide helpful evidence for the clinical practice and further studies.
This study included 84 patients with CKP. Of them, 42 subjects received acupuncture plus TIP, and the other 42 participants received TIP monotherapy. Patients in both groups were treated for a total of 8 weeks. The results showed that patients who received acupuncture and TIP achieved much better effectiveness in all primary and secondary endpoints than patients who received TIP monotherapy. The findings of this study indicated that acupuncture plus TIP may benefit more for patients with CKP due to the osteoarthritis.
Several advantages and disadvantages existed in this study. As for advantage, this study firstly explored the effectiveness and safety of acupuncture plus TIP for the treatment of patients with CKP, which may provide helpful evidence for both clinicians and future studies. As for disadvantage, this study was impossible to apply procedures of randomization, and blinding to neither the patients nor the researchers, because all data were collected from completed medical records of eligible patients.
5. Conclusion
The findings of this study showed that acupuncture plus TIP may benefit more for patients with CKP than TIP monotherapy.
Author contributions
Conceptualization: Shi-Chen Liu, Xiao-Feng Qiao, Jian-Hua Yang, Tian-Qi Wang, Ya-Jie Xiao, Jian-Min Qiao.
Data curation: Shi-Chen Liu, Qing-Xi Tang, Xiao-Guang Li, Jian-Hua Yang, Ya-Jie Xiao, Jian-Min Qiao.
Formal analysis: Xiao-Feng Qiao.
Funding acquisition: Shi-Chen Liu.
Investigation: Tian-Qi Wang, Jian-Min Qiao.
Methodology: Xiao-Feng Qiao, Xiao-Guang Li.
Project administration: Shi-Chen Liu, Jian-Min Qiao.
Resources: Shi-Chen Liu, Qing-Xi Tang, Xiao-Guang Li, Ya-Jie Xiao.
Software: Xiao-Feng Qiao, Jian-Hua Yang.
Supervision: Jian-Min Qiao.
Validation: Qing-Xi Tang, Xiao-Guang Li, Jian-Min Qiao.
Visualization: Qing-Xi Tang, Xiao-Guang Li, Jian-Hua Yang, Tian-Qi Wang, Ya-Jie Xiao.
Writing – original draft: Shi-Chen Liu, Xiao-Feng Qiao, Qing-Xi Tang, Jian-Hua Yang, Tian-Qi Wang, Jian-Min Qiao.
Writing – review and editing: Shi-Chen Liu, Qing-Xi Tang, Xiao-Guang Li, Jian-Hua Yang, Tian-Qi Wang, Ya-Jie Xiao, Jian-Min Qiao.
Footnotes
Abbreviations: CKP = chronic knee pain, MCS = mental component summary, NRS = numeric rating scale, PCS = physical component summary, SF-12 = 12-item Short FormHealth Survey, TIP = topical ibuprofen, WOMAC = Western Ontario and McMaster Universities osteoarthritis index.
S-CL and X-FQ contributed equally to this study.
This study was supported by the Key Project of Jiamusi University Science and Technology (12Z1201507).
The authors have no conflicts of interest to disclose.
References
- [1].Zhang Q, Yue J, Golianu B, et al. Updated systematic review and meta-analysis of acupuncture for chronic knee pain. Acupunct Med 2017;35:392–403. [DOI] [PubMed] [Google Scholar]
- [2].O’Neill TW, McCabe PS, McBeth J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract Res Clin Rheumatol 2018;32:312–26. [DOI] [PubMed] [Google Scholar]
- [3].Agaliotis M, Mackey MG, Jan S, et al. Burden of reduced work productivity among people with chronic knee pain: a systematic review. Occup Environ Med 2014;71:651–9. [DOI] [PubMed] [Google Scholar]
- [4].Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81:646–56. [PMC free article] [PubMed] [Google Scholar]
- [5].Bhatia A, Peng P, Cohen SP. Radiofrequency procedures to relieve chronic knee pain: an evidence-based narrative review. Reg Anesth Pain Med 2016;41:501–10. [DOI] [PubMed] [Google Scholar]
- [6].O’Neill TW, Felson DT. Mechanisms of osteoarthritis (OA) pain. Curr Osteoporos Rep 2018;16:611–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Knapik JJ, Pope R, Orr R, et al. Osteoarthritis: pathophysiology, prevalence, risk factors, and exercise for reducing pain and disability. J Spec Oper Med 2018;18:94–102. [DOI] [PubMed] [Google Scholar]
- [8].Spahn G, Lipfert JU, Maurer C, et al. Risk factors for cartilage damage and osteoarthritis of the elbow joint: case-control study and systematic literature review. Arch Orthop Trauma Surg 2017;137:557–66. [DOI] [PubMed] [Google Scholar]
- [9].Chu IJH, Lim AYT, Ng CLW. Effects of meaningful weight loss beyond symptomatic relief in adults with knee osteoarthritis and obesity: a systematic review and meta-analysis. Obes Rev 2018;19:1597–607. [DOI] [PubMed] [Google Scholar]
- [10].Litwic A, Edwards MH, Dennison EM, et al. Epidemiology and burden of osteoarthritis. Br Med Bull 2013;105:185–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Messier SP. Osteoarthritis of the knee and associated factors of age and obesity: effects on gait. Med Sci Sports Exerc 1994;26:1446–52. [PubMed] [Google Scholar]
- [12].Gregori D, Giacovelli G, Minto C, et al. Association of pharmacological treatments with long-term pain control in patients with knee osteoarthritis: a systematic review and meta-analysis. JAMA 2018;320:2564–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Majeed MH, Sherazi SAA, Bacon D, et al. Pharmacological treatment of pain in osteoarthritis: a descriptive review. Curr Rheumatol Rep 2018;20:88. [DOI] [PubMed] [Google Scholar]
- [14].Kroon FPB, Carmona L, Schoones JW, et al. Efficacy and safety of non-pharmacological, pharmacological and surgical treatment for hand osteoarthritis: a systematic literature review informing the 2018 update of the EULAR recommendations for the management of hand osteoarthritis. RMD Open 2018;4:e000734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Cuperus N, Hoogeboom TJ, Kersten CC, et al. Randomized trial of the effectiveness of a non-pharmacological multidisciplinary face-to-face treatment program on daily function compared to a telephone-based treatment program in patients with generalized osteoarthritis. Osteoarthritis Cartilage 2015;23:1267–75. [DOI] [PubMed] [Google Scholar]
- [16].Karimifar M, Soltani R, Hajhashemi V, et al. Evaluation of the effect of Elaeagnus angustifolia alone and combined with Boswellia thurifera compared with ibuprofen in patients with knee osteoarthritis: a randomized double-blind controlled clinical trial. Clin Rheumatol 2017;36:1849–53. [DOI] [PubMed] [Google Scholar]
- [17].Gordo AC, Walker C, Armada B, et al. Efficacy of celecoxib versus ibuprofen for the treatment of patients with osteoarthritis of the knee: a randomized double-blind, non-inferiority trial. J Int Med Res 2017;45:59–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Zamani O, Böttcher E, Rieger JD, et al. Comparison of safety, efficacy and tolerability of dexibuprofen and ibuprofen in the treatment of osteoarthritis of the hip or knee. Wien Klin Wochenschr 2014;126:368–75. [DOI] [PubMed] [Google Scholar]
- [19].Kuptniratsaikul V, Dajpratham P, Taechaarpornkul W, et al. Efficacy and safety of Curcuma domestica extracts compared with ibuprofen in patients with knee osteoarthritis: a multicenter study. Clin Interv Aging 2014;9:451–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Trnavský K, Fischer M, Vögtle-Junkert U, et al. Efficacy and safety of 5% ibuprofen cream treatment in knee osteoarthritis. Results of a randomized, double-blind, placebo-controlled study. J Rheumatol 2004;31:565–72. [PubMed] [Google Scholar]
- [21].Rovenský J, Miceková D, Gubzová Z, et al. Treatment of knee osteoarthritis with a topical non-steroidal antiinflammatory drug. Results of a randomized, double-blind, placebo-controlled study on the efficacy and safety of a 5% ibuprofen cream. Drugs Exp Clin Res 2001;27:209–21. [PubMed] [Google Scholar]
- [22].Tiso RL, Tong-Ngork S, Fredlund KL. Oral versus topical Ibuprofen for chronic knee pain: a prospective randomized pilot study. Pain Physician 2010;13:457–67. [PubMed] [Google Scholar]
- [23].Yin C, Buchheit TE, Park JJ. Acupuncture for chronic pain: an update and critical overview. Curr Opin Anaesthesiol 2017;30:583–92. [DOI] [PubMed] [Google Scholar]
- [24].Ju ZY, Wang K, Cui HS, et al. Acupuncture for neuropathic pain in adults. Cochrane Database Syst Rev 2017;12:CD012057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].White A, Foster NE, Cummings M, et al. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford) 2007;46:384–90. [DOI] [PubMed] [Google Scholar]
- [26].Hinman RS, McCrory P, Pirotta M, et al. Efficacy of acupuncture for chronic knee pain: protocol for a randomised controlled trial using a Zelen design. BMC Complement Altern Med 2012;12:161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Helianthi DR, Simadibrata C, Srilestari A, et al. Pain reduction after laser acupuncture treatment in geriatric patients with knee osteoarthritis: a randomized controlled trial. Acta Med Indones 2016;48:114–21. [PubMed] [Google Scholar]
- [28].Li H, Zhang FH, Wang YC. Observation on the efficacy of acupuncture and fire needle therapy for hand osteoarthritis. Zhongguo Zhen Jiu 2013;33:885–8. [PubMed] [Google Scholar]
- [29].Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988;15:1833–40. [PubMed] [Google Scholar]
- [30].Bellamy N, Carette S, Ford PM, et al. Osteoarthritis antirheumatic drug trials: III, setting the delta for clinical trials: results of a consensus development (Delphi) exercise. J Rheumatol 1992;19:451–7. [PubMed] [Google Scholar]
- [31].Angst F, Aeschlimann A, Stucki G. Smallest detectable and minimal clinically important differences of rehabilitation intervention with their implications for required sample sizes using WOMAC and SF-36 quality of life measurement instruments in patients with osteoarthritis of the lower extremities. Arthritis Rheum 2001;45:384–91. [DOI] [PubMed] [Google Scholar]