

In the past decades, multiple studies testing interventions for adolescent substance use problems have shown that youth in treatment for substance use problems have better outcomes than those not in treatment, and there are multiple interventions that have been identified as “well-established” or “probably efficacious”.1 Contingency management (CM) is one such intervention. The CM approach grew out of the disciplines of behavioral pharmacology and behavior analysis that demonstrated substance use can be conceptualized as a learned behavior that is maintained, in part, by pharmacological actions (reinforcing effects) of the substance in conjunction with social and other non-pharmacological reinforcement that occur in the context of substance use. As such, CM capitalizes on knowledge that drug-seeking and drug-use can be reduced by arranging relevant environmental contingencies such that incompatible or competing prosocial reinforcing activities are made more available, and drug abstinence is directly reinforced while drug use is punished. Typically, CM interventions are used as part of a comprehensive substance use treatment program including some form of individual or family-based intervention.
CM programs (a) identify and specifically define target therapeutic behaviors such as drug abstinence; (b) carefully monitor the target behavior(s) objectively on a pre-specified schedule; and (c) deliver reinforcing or punishing events (e.g., tangible rewards or incentives, loss of privileges) when the target behavior is or is not achieved. Often CM programs are managed and delivered directly by program staff. In addition, CM interventions for youth often guide parents in developing and implementing a CM program at home. The goal of CM interventions is to systematically weaken the influence of reinforcement derived from substance use, and to increase the frequency and magnitude of reinforcement derived from healthier alternative activities, especially those that are incompatible with continued substance use.
Principles of Contingency Management
CM interventions are defined by the following metrics: the target behavior, the method of monitoring of the target behavior, the schedule used to deliver positive or negative consequences, the type of consequence, and the magnitude of the consequence. The most commonly selected target behavior used in CM programs has been drug abstinence. CM programs, however, have also targeted medication compliance, counseling attendance, and completion of prosocial activities or lifestyle changes. When choosing targets, one should be aware that successful change in one behavior may not result in change in another. For example, treatment attendance may improve by providing incentives for coming to sessions, but drug use might not be affected.2 Thus, it is recommended that, if possible, abstinence should always be a target behavior, although other supplemental behaviors may be targeted as well provided they can be objectively defined and monitored, as described next.
Effective monitoring of the targeted behavior is essential to a CM program, because consequences (reinforcement or punishment) must be applied systematically in order to be effective. When abstinence is the target behavior, this typically involves some form of biochemical verification, usually via urinalysis testing. Such testing requires careful planning so that the schedule of testing (frequency) allows optimal detection of substance use and abstinence. For example, detection windows range from hours (for alcohol use) to many days (cannabis), and depend on the type of testing employed (e.g., breath, urine, saliva). The importance of having a method for objectively and reliably verifying whether a target behavior occurred pertains as well to other target behaviors (e.g., attending self-help meeting, going to the gym, attending an after school program, completing therapeutic practice assignments). Reliance on self-reports of drug use or completion of other therapeutic tasks is not adequate for effective delivery of a CM program.
The schedule of reinforcement or punishment refers to the temporal relation between the target behavior and the delivery of the consequence. Generally, efficacy is likely to improve as the temporal delay between the occurrence of the target behavior and delivery of the consequence decreases. For example, all else being equal, providing positive reinforcement for drug abstinence on the same day on which a youth submits a negative urine specimen would likely be more effective than waiting a week before reinforcement is delivered. For this reason, the use of rapid drug tests in the clinic setting is much preferred over laboratory tests that do not provide immediate results as they permit more immediate reinforcement of abstinence. In working with clinicians and researchers in diverse settings who are interested in using CM with their clients or patients, questions often arise about the need for and implementation of urine drug testing. Although it can be challenging to address positive urine drug test results in real time, it may help to think of such information as similar to many other health status indicators collected during a health visit that can guide the clinical interaction (e.g., weight, blood pressure, HbA1c, etc.). Objective information about substance use is not only the most important target for CM, but also a vital marker of problem severity and response to intervention.
Schedules with frequent opportunities for reinforcement (e.g., at least weekly) are more likely to engender and strengthen abstinence. Once a behavior is established, less frequent schedules are typically considered for maintenance of behavior change. One schedule that has demonstrated efficacy across multiple substance abuse treatment studies is a fixed schedule with escalating rewards and a reset contingency (typically referred to as abstinence-based vouchers or incentives3). This schedule provides monetary rewards for each negative sample that can be “held” in a clinic account or loaded onto a reloadable credit card, with a small (usually financial) reward for the first negative sample, and rewards increase in value with each subsequent negative sample. Positive samples reset the reward value to the starting point, but a period of abstinence can reset the value back to the prior maximum. In addition, rewards can be provided according to an intermittent schedule using the fishbowl method,4 in which negative samples earn the opportunity to complete “draws” that have a possibility of winning a reward, with rewards of varying values available.
The magnitude of reinforcement is also an important factor that can greatly affect the efficacy of CM interventions. For example, if the goal is drug abstinence, a $10 incentive for each negative drug test is likely to be more effective in increasing abstinence than one worth $2.00. Multiple studies have demonstrated that greater magnitude schedules of reinforcement have resulted in better abstinence outcomes than lower magnitude.5
The type of reinforcers or punishers used in a CM program can also be critical to its success. Individuals vary greatly in terms of the types of goods and services that they value, and hence that will serve as effective reinforcers/incentives. For example, a specific reinforcer (e.g., pizza or movie theatre passes) that serves as an effective incentive for one youth may not be reinforcing for another. Use of a range of incentives or allowing youth to choose their incentive can increase the probability that the incentive will be effective and facilitate the desired target behavior. Gift cards or reloadable credit cards are often used as they serve as a flexible reward, allowing the youth to select personalized rewards that vary over time.
There are some excellent resources available to assist clinicians and researchers in developing CM interventions. Examples include a NIDA and SAMHSA Blending Initiative, Promoting Awareness of Motivational Incentives6, online information and training (https://arenaebp.com/), as well as published manuals.7,8
Research on CM with Youth
In two prior articles we reviewed research on CM for substance use among youth prior to 20109 and from 2010 to 201610. Since that latter article, we are aware of 2 additional studies using CM with adolescents.11,12 Most of these studies have involved youth whose primary or most frequent substance used is cannabis, and have demonstrated efficacy of CM across highly diverse settings (school, clinic, juvenile justice, continuing care), platform interventions using fixed (i.e., vouchers) and intermittent (i.e., fishbowl) incentive schedules, and incentive magnitude (~$25 to $725 total/~$6 to $50 per week).
These studies fall into several distinct categories. First, there is a group of studies that used CM to target tobacco use among high school students.13–16 Most of these studies were conducted in the school setting, but some have also been implemented remotely.15,16 Across studies, 4-week abstinence rates were generally >50%. One study also used a similar CM model to target substance use (primarily cannabis use) in the school setting, comparing brief motivational interviewing + CM to brief motivational interviewing alone.17 Results indicated greater reductions in cannabis use days per month among CM than MI only youth, with significant differences between conditions at the end of the 8-week intervention period, but not at the 16-week follow up assessment.
A series of studies have tested integration of family-based CM with juvenile drug court.18 Incentives for abstinence were provided both by the clinic and parents, who received instruction in setting up a home based CM program as well. Youth receiving CM had decreased odds of a cannabis positive urine test throughout the 9-month intervention (i.e., documenting cannabis use) relative to control group youth who received drug court as usual. At the 9-month assessment, 20% of the youth in the CM condition versus 34% of the control youth tested positive for cannabis. This program has an excellent manual available,8 and is being widely disseminated.19
CM has also been tested for adolescents stepping down from residential substance use treatment.20 Youth receiving CM had more days of abstinence from cannabis through the 9-month post treatment follow up compared to usual continuing care.
We have conducted a series of three randomized clinical trials (RCTs) testing the impact of CM when added to an evidence-based individual counseling platform.11,21,22 This 14-week CM intervention integrates clinic-delivered incentives (~$590 maximum for continuous abstinence) with home-based CM, in which parents receive instruction and weekly support in developing and implementing a substance monitoring contract (SMC) that specifies rewards for documented abstinence and consequences for substance use. Parents also earned incentives for session attendance, and compliance with the SMC (maximum earnings ~$270).
The home-based SMC specifies positive and negative consequences to be delivered by the parents in response to documented abstinence or use (based on clinic-based urine drug testing results) (see Figure 1). The consequences are determined via a collaborative process between therapist, parent and adolescent, and revaluated each week during weekly counseling sessions. This contract uses the same target (abstinence), schedule (at least weekly), and monitoring method (urine drug testing) as our clinic-based CM. Parents are also provided with disposable breathalyzers to test for alcohol use at home (see handout in Figure 2). Parents personalize the type of consequence (monetary, voucher type system, privileges) and the magnitude of the consequences, and these factors change throughout treatment in response to treatment success or failure. Examples of rewards have included earning a pre-specified amount of money for each negative sample, family activities like going out to dinner or choosing the menu for dinner at home, and access to the family car or gas money. Examples of consequences have included restrictions on media/internet/gaming/or phone use, grounding, or extra household chores. The procedures for working with parents to establish and implement their home contract were based on Adolescent Transitions,23 an evidence based parent training intervention. This model is now known as the Family Check Up (https://reachinstitute.asu.edu/family-check-up), and diverse training options for providers plus information for families are available.
Figure 1.
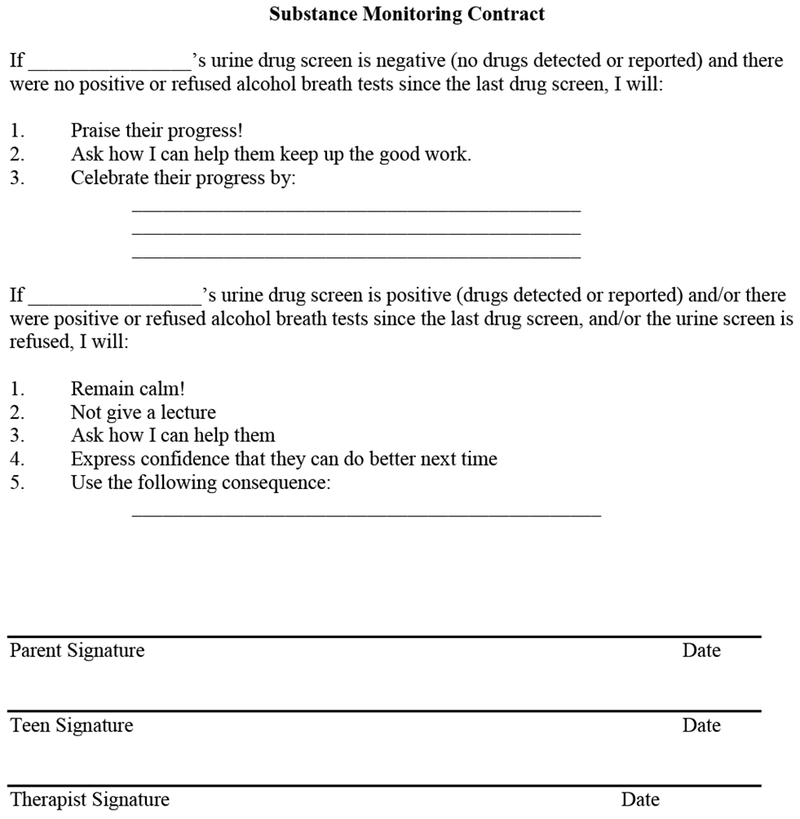
Substance monitoring contract for home-based CM
Figure 2.
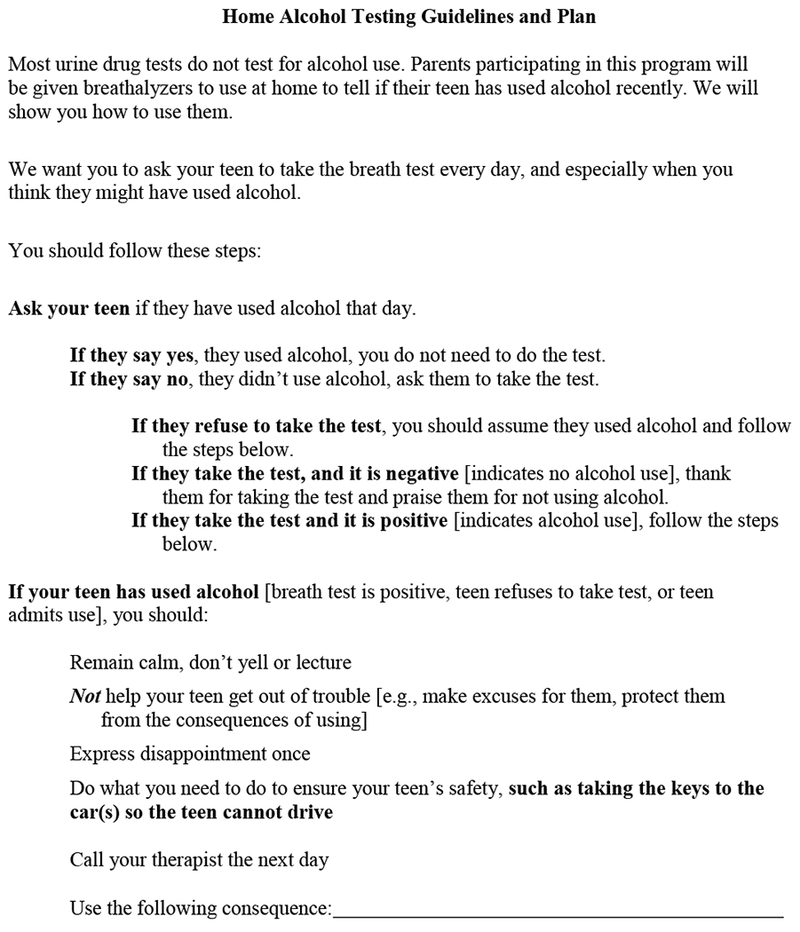
Alcohol testing guidelines and plan for home-based CM
Clinicians sometimes raise concerns about how parents might respond to test results indicating drug use. Working with parents to develop a home SMC can reduce conflict about test results, as parents and teens will have established a plan in advance for how to respond to the results – positive or negative. Moreover, reminders that the primary purpose of testing is to provide the teen with an opportunity to demonstrate that they are abstinent, and to earn rewards and privileges, can help maintain a positive attitude toward the SMC and testing in general. Persistent positive test results indicating persistent substance use suggest the need for a higher level of care. Figure 3 provides a sample handout we have used with teens and parents to provide the rationale for and information about the urine monitoring program. If clinic-based urine testing is not available, parents can consider implementing these procedures at home, although we strongly recommend clinician support in implementing such a procedure as it has many challenges.
Figure 3.
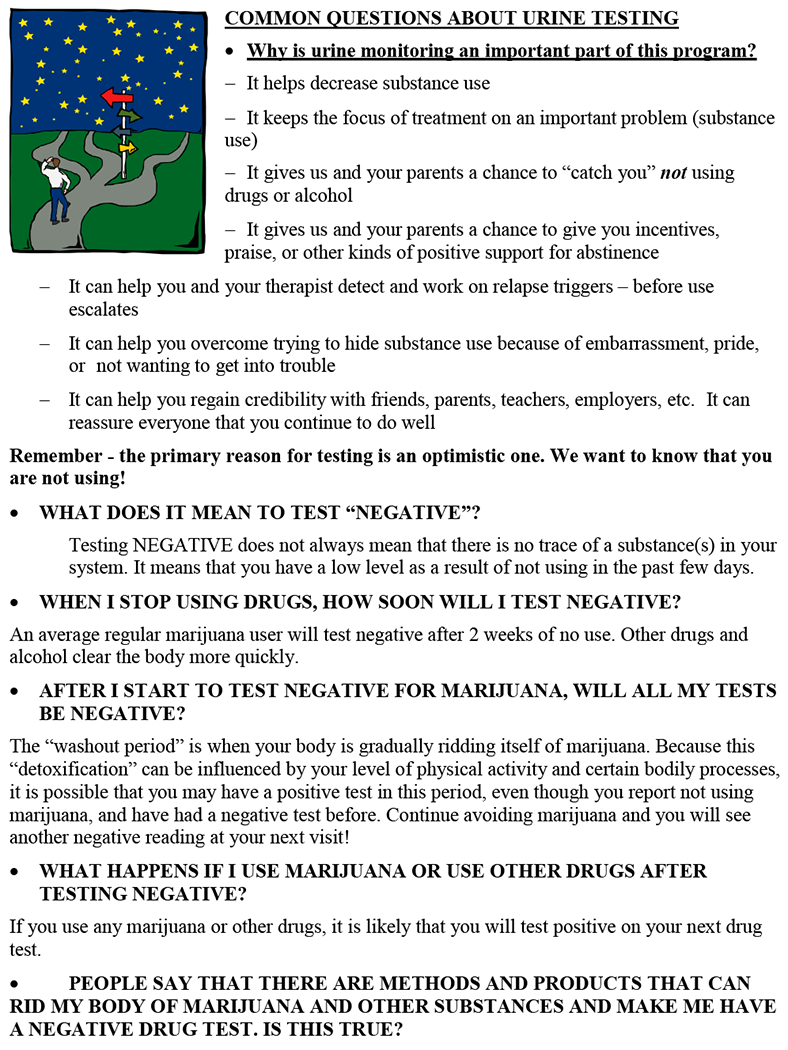
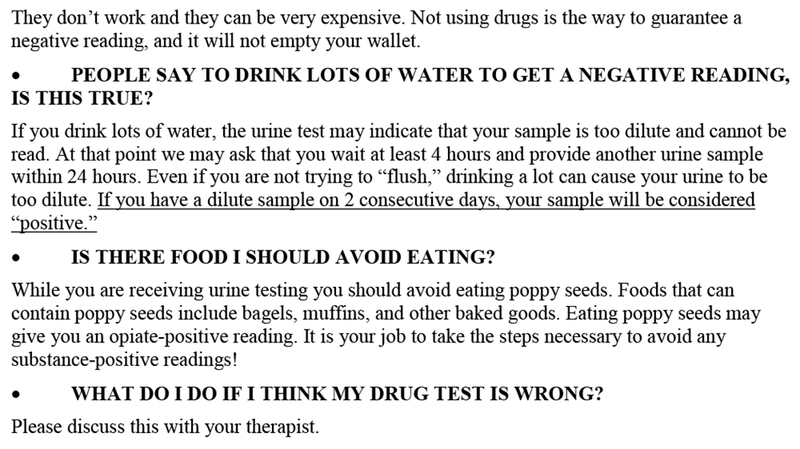
Handout addressing common questions about urine drug testing
Across the three RCTs, there were consistent positive effects of CM during treatment. For example, in the first study,22 CM enhanced continuous abstinence outcomes, engendering more weeks of continuous cannabis abstinence during treatment. Those receiving CM were also significantly more likely to achieve ≥8 weeks (53% vs. 30%) and ≥10 weeks of continuous abstinence (50% vs. 19%). However, there was no significant between-condition difference in abstinence 9 months post treatment. There was an increase in cannabis use from discharge to the 9-month follow up, that, while not returning to intake levels, was of significant concern. In the second study,21 youth receiving CM were more likely to achieve 4 weeks of continuous cannabis abstinence during treatment (48%) than were those not receiving CM (30%). In addition, among youth with at least one negative urine drug test during treatment, those who received CM had significantly more weeks of continuous abstinence from cannabis than those who did not receive CM. They were also significantly more likely to be abstinent at the end of treatment, but rates of abstinence were comparable between conditions at post treatment follow up assessments, and significant relapse was observed. Interestingly, self-reports of cannabis use frequency showed sustained decreases during and post treatment for all conditions. Thus, the effect of CM was greater on abstinence, as indicated by urine drug tests than via self-report. In our most recent CM study11 that focused on youth with alcohol use problems, with or without comorbid cannabis use, a similar percentage of youth maintained complete alcohol abstinence across the 36-week follow up in both conditions. However, among youth not entirely abstinent from alcohol, those receiving CM reported fewer alcohol use days during the 36 weeks after the end of treatment than those not receiving CM. Among youth who also used cannabis at baseline, results showed similar benefits of CM on cannabis use days.
Predictors of CM Efficacy
Of note, across all these studies with youth, no trial has tested the impact of CM magnitude (i.e., compared different magnitudes or schedules) for substance using youth. To date, no trial has systematically tested the independent or combined efficacy of clinic- vs. parent-based CM. The best outcomes across studies were reported for youth with the lowest rates of baseline substance use, that is, those in juvenile drug court or those entering continuing care after residential treatment.18,20 Intermediate, less enduring outcomes were reported for youth in outpatient and school-based settings.17,21 Finally, across studies, long-term reduction in use or abstinence among youth remains a serious challenge, even among those who show better post-treatment outcomes. The one study focused on continuing care suggests that including additional targets of CM such as engagement in specific types of prosocial activities together with targeting abstinence might better facilitate enduring change.20
For the most part, studies have shown that although many baseline characteristics are associated with poorer treatment outcomes (e.g., age, gender, ethnicity, presence of comorbid mental health problems), there are not differential effects of CM across such groups.18,24 However, research is particularly limited on moderation of CM efficacy by cognitive characteristics, such as delay discounting or other constructs related to executive function, including self-regulation or emotion-regulation. We reported a post-hoc analysis showing that youth with disruptive behavior disorder diagnoses (DBD) in addition to cannabis use disorder had better outcomes when they received CM.25 Interestingly, DBD-negative adolescents who received abstinence-based CM did not have significantly better cannabis use outcomes compared to counseling only. This may have been due to a ceiling effect; that is, DBD-negative adolescents receiving evidence based individual counseling had good clinical outcomes, making it more difficult to demonstrate improved outcomes with abstinence-based CM. These findings highlight the importance of future research focused on testing CM and other treatment approaches tailored to pretreatment youth characteristics.
Conclusion and Future Directions
CM strategies can be effective for retaining youth in treatment, increasing treatment attendance, and promoting abstinence across multiple types of substance use problems. The growing acceptance of abstinence-based CM as one of the most efficacious interventions for youth SUD is evidenced by its recent use as a treatment platform in several clinical trials of new behavioral or pharmacological treatments that seek strategies to further enhance outcomes for adolescents.26,27 That said, it is critical to attend to the defining components that make up each unique CM intervention, including the target, the monitoring method, the schedule of reinforcement, and the magnitude and type of rewards used, as each can influence intervention efficacy. Fortunately, evidence-based training and manuals are now available to guide research and practice. Avenues for future research include testing the efficacy of a solely parent-administered CM intervention without clinic delivered CM incentives and developing CM models focused on maintaining treatment gains and preventing relapse. We also expect that the growing development and application of diverse technological devices and platforms to improve health behavior should provide a surplus of ideas and innovations for adapting and implementing CM-based programs to better address adolescent substance use problems.28
Synopsis.
Multiple interventions for treating adolescents with substance use disorders have demonstrated efficacy, but most teens do not show an enduring positive response to these treatments. Contingency-management (CM) based strategies provide a promising alternative, and clinical research focused on the development and testing of innovative CM models continues to grow. This article provides information on the principles that underlie CM interventions, key metrics that define their development and implementation, a brief review of studies that have tested these approaches, and some clinical CM tools. CM interventions can play a key role in motivating abstinence among youth with substance use problems. As with other interventions to help youth with substance use problems, there is still much to learn about CM approaches especially ways to tailor interventions to youth with different clinical needs, and ways to improve long-term efficacy.
Key Points.
Contingency management (CM) interventions can increase abstinence among youth with substance use problems.
In developing CM interventions, it is important to consider target outcomes, objective monitoring, and the timing, magnitude, and type of rewards and consequences.
Parents can successfully implement CM at home with training and support.
Acknowledgments
This work was supported by NIH Grants DA15186 and P30DA029926. None of the authors have any conflict of interest or other disclosures.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Hogue A, Henderson CE, Becker SJ, Knight DK. Evidence Base on Outpatient Behavioral Treatments for Adolescent Substance Use, 2014-2017: Outcomes, Treatment Delivery, and Promising Horizons. J Clin Child Adolesc Psychol. 2018;47(4):499–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Iguchi MY, Lamb RJ, Belding MA, Platt JJ, Husband SD, Morral AR. Contingent reinforcement of group participation versus abstinence in a methadone maintenance program. Exp Clin Psychopharmacol. 1996;4:315–321. [Google Scholar]
- 3.Higgins ST, Heil SH, Lussier JP. Clinical implications of reinforcement as a determinant of substance use disorders. Annu Rev Psychol. 2004;55:431–461. [DOI] [PubMed] [Google Scholar]
- 4.Petry NM, Peirce JM, Stitzer ML, et al. Effect of prize-based incentives on outcomes in stimulant abusers in outpatient psychosocial treatment programs: A national drug abuse treatment clinical trials network study. Arch Gen Psychiatry. 2005;62:1148–1156. [DOI] [PubMed] [Google Scholar]
- 5.Lussier JP, Heil SH, Mongeon JA, Badger GJ, Higgins ST. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction. 2006;101(2):192–203. [DOI] [PubMed] [Google Scholar]
- 6.Hamilton J, Kellogg S, Killeen T, et al. Promoting Awareness of Motivational Incentives (PAMI). http://pami.nattc.org/explore/priorityareas/science/blendinginitiative/pami/. Published 2009. Accessed September 29, 2009.
- 7.Petry N Contingency management for substance abuse treatment: A guide to implementing this evidence-based practice. Routledge; 2011. [Google Scholar]
- 8.Henggeler SW, Cunningham PB, Rowland MD, et al. Contingency management for adolescent substance abuse: A practitioner’s guide. New York, NY, US: Guilford Press; 2012. [Google Scholar]
- 9.Stanger C, Budney AJ. Contingency management approaches for adolescent substance use disorders. Child and Adolescent Psychiatric Clinics of North America.2010;19(3):547–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stanger C, Lansing AH, Budney AJ. Advances in research on contingency management for adolescent substance use. Child and Adolescent Psychiatric Clinics of North America. 2016;25(4):645–659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stanger C, Scherer EA, Babbin SF, Ryan SR, Budney AJ. Abstinence based incentives plus parent training for adolescent alcohol and other substance misuse. Psychology of Addictive Behaviors. 2017;31(4):385–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Letourneau EJ, McCart MR, Sheidow AJ, Mauro PM. First Evaluation of a Contingency Management Intervention Addressing Adolescent Substance Use and Sexual Risk Behaviors: Risk Reduction Therapy for Adolescents. J Subst Abuse Treat. 2017;72:56–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cavallo DA, Cooney JL, Duhig AM, et al. Combining cognitive behavioral therapy with contingency management for smoking cessation in adolescent smokers: A preliminary comparison of two different CBT formats. American Journal on Addictions.2007;16(6):468–474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Krishnan-Sarin S, Cavallo DA, Cooney JL, et al. An exploratory randomized controlled trial of a novel high-school-based smoking cessation intervention for adolescent smokers using abstinence-contingent incentives and cognitive behavioral therapy. Drug Alcohol Depend. 2013;132(1-2):346–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kong G, Goldberg AL, Dallery J, Krishnan-Sarin S. An open-label pilot study of an intervention using mobile phones to deliver contingency management of tobacco abstinence to high school students. Exp Clin Psychopharmacol. 2017;25(5):333–337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Reynolds B, Dallery J, Shroff P, Patak M, Leraas K. A web-based contingency management program with adolescent smokers. Journal of Applied Behavior Analysis. 2008;41(4):597–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stewart DG, Felleman BI, Arger CA. Effectiveness of Motivational Incentives for Adolescent Marijuana Users in a School-Based Intervention. J Subst Abuse Treat. 2015;58:43–50. [DOI] [PubMed] [Google Scholar]
- 18.Henggeler SW, McCart MR, Cunningham PB, Chapman JE. Enhancing the effectiveness of juvenile drug courts by integrating evidence-based principles. Journal of Consulting and Clinical Psychology. 2012;80(2):264–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cunningham PB, Henggeler SW. The Development and Transportability of Multisystemic Therapy-Substance Abuse: A Treatment for Adolescents with Substance Use Disorders AU - Randall, Jeff. Journal of Child & Adolescent Substance Abuse. 2018;27(2):59–66. [Google Scholar]
- 20.Godley MD, Godley SH, Dennis ML, Funk RR, Pasetti LL, Petry NM. A randomized trial of assertive continuing care and contingency management for adolescents with substance use disorders. Journal of Consulting and Clinical Psychology. 2014;82(1):40–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stanger C, Ryan SR, Scherer EA, Norton GE, Budney AJ. Clinic- and home-based contingency management plus parent training for adolescent cannabis use disorders. Journal of the American Academy of Child & Adolescent Psychiatry. 2015;54(6):445–453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stanger C, Budney AJ, Kamon JL, Thostensen J. A randomized trial of contingency management for adolescent marijuana abuse and dependence. Drug and Alcohol Dependence. 2009;105(3):240–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dishion TJ, Kavanagh K. Intervening in Adolescent Problem Behavior: A Family-Centered Approach. New York, NY: Guilford Press; 2003. [Google Scholar]
- 24.Kaminer Y, Burleson JA, Burke R, Litt MD. The efficacy of contingency management for adolescent cannabis use disorder: a controlled study. Subst Abus. 2014;35(4):391–398. [DOI] [PubMed] [Google Scholar]
- 25.Ryan SR, Stanger C, Thostenson J, Whitmore JJ, Budney AJ. The impact of disruptive behavior disorder on substance use treatment outcome in adolescents. Journal of Substance Abuse Treatment. 2013;44:506–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Letourneau EJ, McCart MR, Asuzu K, Mauro PM, Sheidow AJ. Caregiver Involvement in Sexual Risk Reduction with Substance Using Juvenile Delinquents: Overview and Preliminary Outcomes of a Randomized Trial. Adolesc Psychiatry (Hilversum). 2013;3(4):342–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McCart MR, Sheidow AJ, Letourneau EJ. Risk Reduction Therapy for Adolescents: Targeting Substance Use and HIV/STI-Risk Behaviors. Cognitive and Behavioral Practice. 2014;21(2):161–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Budney AJ, Marsch LA, Bickel WK. Computerized therapies in the treatment of substance use disorders In: el-Guebaly, ed. Textbook of Addiction Treatment: International Perspectives. Berlin: Springer-Verlag; 2014. [Google Scholar]