

Abstract
Osteomas of temporal bone are rare, slow growing benign tumours and they are reported in all parts of temporal bone. This study is a retrospective study of the clinical presentation, management and complications of temporal bone osteoma done from January 1999 through January 2017. The study population is thirteen patients, all who has been radiologically and histopathologically proven to be a case of osteoma. Total number of patients were 13 of which 7 were females and rest 6 were male. Presenting complaints included swelling behind the ear (6 cases), reduced hearing in 4 cases, 2 cases had ear discharge, 3 of them were asymptomatic in whom it was diagnosed accidently. The duration of symptoms ranged from 1 month to 10 years. Of total 13 patients 7 had external auditory canal involvement and 4 cases had mastoid region. Two patients were managed conservatively, one refused surgery and rest ten cases underwent excision. The specimen was sent for histopathological examination and diagnosis of osteoma was confirmed. The decision regarding whether to operate or not depends on each case depending on its size, symptoms and more importantly the complications. Excision of osteoma remains the treatment of choice.
Keywords: Osteoma, Temporal bone
Introduction
Osteomas are rare benign lesions which are slow growing and are made up of mature bone [1]. Though rare, they can be seen in many parts of temporal bone like external auditory canal, mastoid and squamous portion, middle ear, Eustachian tube, petrous apex, internal auditory canal, zygomatic process, glenoid fossa and styloid process [2–4]. External auditory canal is commonest site of involvement with an estimated incidence of 0.5% of the total ear surgeries [5]. These are usually asymptomatic apart from those in whom cosmetic deformities are seen. These can be associated with external auditory canal cholesteatoma and its complications [4, 6]. In this article we present a retrospective review of 13 cases of temporal bone osteoma.
Methodology
The study was conducted in a tertiary care hospital on patients who came to otolaryngology department. It is a retrospective study done from January 1999 through September 2017. Demographic details, detail history, general examination and otorhinolaryngology examination findings, radiological data, site of involvement and treatment given for each patient was noted down.
Results
Total number of patients were 13 of which 7 were females and rest 6 were male (Fig. 1). Mean age of involvement was found to be 16.6 years (Fig. 2). Majority of cases (6 cases) had swelling behind the ear as their presenting complaints (Fig. 3), 4 cases had reduced hearing, 2 cases had ear discharge, 3 of them were asymptomatic in whom it was diagnosed accidently and one case gave history of injury to canal with match stick prior to presentation. The duration of symptoms ranged from 1 month to 10 years. Of total 13 patients 7 had external auditory canal (Fig. 4) involvement and 4 cases had mastoid region. Symptoms of each patients, their site of involvement and treatment given is tabulated in Table 1.
Fig. 1.
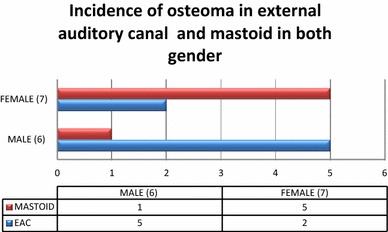
Showing gender distribution
Fig. 2.
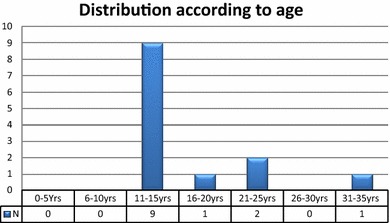
Showing age distribution
Fig. 3.

A photograph showing swelling behind left ear as initial presentation
Fig. 4.

Photograph showing mass in external auditory canal
Table 1.
Showing patients signs and symptoms
| No. | Age (years) | Sex | Complaints | Site | Duration of symptoms | Treatment |
|---|---|---|---|---|---|---|
| 1 | 14 | F | Swelling in the left temporal region | Squamous portion of the temporal bone | 1 year | None; patient refused surgery |
| 2 | 15 | F | None (found in the mastoid antrum during cortcial mastoidectomy) | Mastoid antrum | N/a | Excision |
| 3 | 12 | F | Swelling in the mastoid region | Mastoid portion of the temporal bone | 9 months | Excision |
| 4 | 15 | F | Swelling in the mastoid region | Mastoid portion of the temporal bone | 1 year | Excision |
| 5 | 14 | M | Swelling in the mastoid region | Mastoid portion of the temporal bone | 2 years | Excision |
| 6 | 12 | F | Swelling in the EAC | EAC | 4 years | Excision with radical mastoidectomy |
| 7 | 15 | M | Decreased hearing | EAC | 5 months | Excision |
| 8 | 12 | M | None (found during removal of impacted wax) | EAC | N/a | Observation |
| 9 | 14 | M | None (found during routine examination) | EAC | N/a | Observation |
| 10 | 18 | F | Swelling in the mastoid region | Mastoid portion of the temporal bone | 3 years | Excision |
| 11 | 21 | M | Decreased hearing | EAC | 3 months | Excision with canaloplasty |
| 12 | 34 | M | Swelling in the mastoid region, decreased hearing, ear discharge | EAC | 10 years | Excision with tympanoplasty |
| 13 | 21 | F | Decreased hearing, injury by matchstick, ear discharge | EAC | 1 month | Excision |
CT was done for all cases and it showed a bony, dense mass in each (Figs. 5, 6). Ten patients underwent excision. The specimen was sent for histopathological examination and diagnosis of osteoma was confirmed (Fig. 7).
Fig. 5.

CT scan showing dense mass over the left mastoid region (arrow)
Fig. 6.
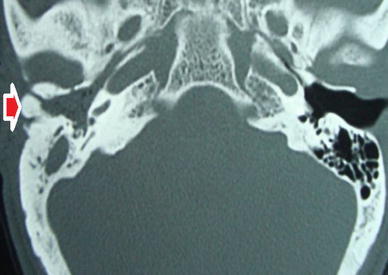
CT scan showing dense mass in the right ear canal (arrow)
Fig. 7.
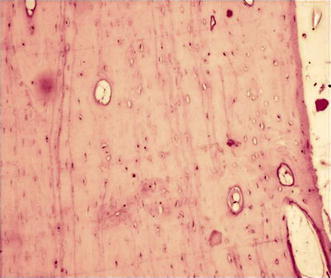
Microphotograph showing mature lamellar bone and fibro vascular tissues
Discussion
Osteoma in head and neck region is a very rare entity. According to Dominiguez perez et al., only 150 cases have been reported in literature in 2010 [7].They can be seen in all the parts of temporal bone like external auditory canal, mastoid and squamous portion, middle ear, eustachian tube, petrous apex, internal auditory canal, zygomatic process, glenoid fossa and styloid process [2–4]; external auditory canal being the most common site followed by mastoid region [2].
The eatiopathogenesis of osteoma is controversial subject. Several factors have been proposed including chronic infection, trauma, hereditary, surgery, radiotherapy and glandular dysfunction (pituitary gland). Varboncoeur et al. [8] mentioned that osteomas origin from embryologic cartilaginous rest or persistent embryologic periosteum. Yamasoba et al. [9] proposed in their case report that osteoma might be congenital. Kaplan et al. [10] propsed that the development of osteoma might be due to trauma and muscle traction.
In the current study one patient had history of trauma but duration of 15 days makes it insignificant. Four cases had an associated ear infection, one of them had osteoma in the mastoid antrum and 2 of them had an additional external auditory canal cholesteatoma along with the osteoma.
Osteoma of the temporal bone seems to arise from preosseous connective tissue from suture line, which relatively has thick subcutaneous layer with rich blood supply [6, 11]. As the osteomas are slow growing, they remain asymptomatic and stable for many years. They present as smooth surface with characteristic hard, bony consistence on palpation [2]. Osteomas in the mastoid region are solitary and grow out from surface producing external swelling [12].
Osteomas have been classified in many ways, by their pattern of growth into outgrowing or ingrowing, unilateral or bilateral and on histopathological examination into 4 histopathological types [13], they are made up of discrete fibrovascular channels surrounded by lamellar bone.
Osteoma compactum—it is common type, is hard and attached to cortex of mastoid process. Histologically, it is composed of dense lamellated bone tissue and is traversed by few vessels.
Osteoma cancellare—consists of fibrous cellular tissue and cancellous bone.
Osteoma cartilagineum—it is rare; consisting of bone and cartilage.
Osteoma mixtum—consists of mixture of types of bone found in osteoma compactum and osteoma cancellare.
Osteomas of temporal bone are predominantly asymptomatic which are incidentally found on examination [12] and in our study 3/13 were asymptomatic. Symptoms like reduced hearing or fullness in ear may be seen in case of external auditory canal osteoma either due to tumour itself or due to cerumen [14].
Extracanalicular osteomas of the temporal bone are primarily composed of mature bone and they have predominance in young females. Osteomas of middle ear are extremely rare and when they do, they arise from promontory and results in progressive conductive hearing loss usually due to involvement of ossicular chain. Other sites involves pyramidal eminence, hypotympanum and lateral semicircular canal [15].
Osteomas of internal auditory canal exhibit as a wide variety of symptoms including asymmetrical sensorineural hearing loss, vertigo, tinnitus, facial nerve palsy and vestibular dysfunction. It is rare and so far only 12 cases have been reported in the world literature [16].
There was one case in our study were osteoma extended from external auditory canal to middle ear but none with origin from middle ear.
Osteoma of external auditory canal has an estimated incidence of 0.5% of the total ear surgeries [5] and they manifest as solitary, unilateral, pedunculated bony mass of unknown origin [17]. External ear cholesteotoma is the main complication of ear canal osteoma [18] and in our study 2 such patients were noted.
Treatment of choice is surgical excision. In case of extracanalicular osteoma, surgery is indicated if it is causing cosmetic disfigurement, reduced hearing, if the tumour is having accelerated growth and for histopathological diagnosis [19]. The surgical excision involves removal of the tumour at the base where it attached to cortical bone. Surgery has been the treatment of choice for external auditory canal osteoma if it obstructs the canal or associated with external auditory canal cholesteatoma, for middle ear osteoma if it is causing hearing loss and for symptomatic internal auditory canal osteoma [1].
In our study 10/13 underwent surgical excision of the tumour. The decision regarding whether to operate or not depends on each case depending on its size, symptoms and more importantly the complications [20].
Conclusions
Osteoma is a slow growing asymptomatic benign tumour. Complication external auditory canal is canal cholesteatoma and early surgical intervention is advised to prevent complications.
References
- 1.Viswanatha B. Extracanalicular osteoma of the temporal bone. Ear Nose Throat J. 2008;87(7):381–383. doi: 10.1177/014556130808700709. [DOI] [PubMed] [Google Scholar]
- 2.Denia A, Perez F, Canalis RR, Graham MD. Extracanalicular osteomas of the temporal bone. Arch Otolaryngol. 1979;105(12):706–709. doi: 10.1001/archotol.1979.00790240020005. [DOI] [PubMed] [Google Scholar]
- 3.Estrem SA, Vessely MB, Oro JJ. Osteoma of the internal auditory canal. Otolaryngol Head Neck Surg. 1993;108(3):293–297. doi: 10.1177/019459989310800314. [DOI] [PubMed] [Google Scholar]
- 4.Viswanatha B. A case of osteoma with cholesteatoma of the external auditory canal and cerebellar abscess. Int J Pediatr Otorhinolaryngol Extra. 2007;2(1):34–39. doi: 10.1016/j.pedex.2006.12.001. [DOI] [Google Scholar]
- 5.Sheehy JL. Diffuse exostoses and osteoma of the external auditory canal: a report of 100 operations. Otolaryngol Head Neck Surg. 1982;90:337–342. [PubMed] [Google Scholar]
- 6.Lee D, Jun B, Park C, Cho K. A case of osteoma with cholesteatoma in the external auditory canal. Auris Nasus Larynx. 2005;32:281–284. doi: 10.1016/j.anl.2005.03.010. [DOI] [PubMed] [Google Scholar]
- 7.Pérez ADD, Romero RR, Durán DE, Montaño PR, Bernal RA, Rodríguez CM. El osteoma en la mastoides, ¿un hallazgo incidental? Acta Otorrinolaringol Esp. 2011;62:140–143. doi: 10.1016/j.otorri.2010.03.003. [DOI] [PubMed] [Google Scholar]
- 8.Varboncoeur AP, Vanbelois HJ, Bowen LL. Osteoma of the maxillary sinus. J Oral Maxillofac Surg. 1990;48(8):882–883. doi: 10.1016/0278-2391(90)90351-2. [DOI] [PubMed] [Google Scholar]
- 9.Yamasoba T, Harada T, OkunoT Nomura Y. Osteoma of the middle ear. Otolaryngol Head Neck Surg. 1990;116(10):1214–1216. doi: 10.1001/archotol.1990.01870100108025. [DOI] [PubMed] [Google Scholar]
- 10.Kaplan I, Calderón S, Buchner A. Peripheral osteoma of the mandible: a study of 10 new cases and analysis of the literature. J Oral Maxillofac Surg. 1994;52(5):467–470. doi: 10.1016/0278-2391(94)90342-5. [DOI] [PubMed] [Google Scholar]
- 11.Graham MD. Osteomas and exostoses of the external auditory canal. A clinical, histopathological and scanning electron microscopic study. Ann Otol Rhinol Laryngol. 1979;88(4 pt i):566–572. doi: 10.1177/000348947908800422. [DOI] [PubMed] [Google Scholar]
- 12.Freidberg SA. Osteoma of mastoid process. Arch Otolaryngol. 1938;28:20–26. doi: 10.1001/archotol.1938.00650040027003. [DOI] [Google Scholar]
- 13.Morocco WA. Multiple osteoma of mastoid cavity. Arch Otolaryngol. 1948;47:673–677. doi: 10.1001/archotol.1948.00690030699011. [DOI] [PubMed] [Google Scholar]
- 14.Fleming S. Osteoma of the mastoid. Can J Surg. 1966;9(4):402–405. [PubMed] [Google Scholar]
- 15.Viswanatha B. Characteristics of osteomas of the temporal bone in young adolescents. Ear Nose Throat J. 2011;90(2):72–79. doi: 10.1177/014556131109000207. [DOI] [PubMed] [Google Scholar]
- 16.Davis TC, Thedinger BA, Greene GM. Osteomas of the internal auditory canal: a report of two cases. Am J Otol. 2000;21(6):852–856. [PubMed] [Google Scholar]
- 17.Orita Y, Nishizaki K, Fukushima K, Akagi H, Ogawa T, Masuda Y, Fukazawa M, Mori Y. Osteoma with cholesteatoma in the external auditory canal. Int J Pediatr Otolaryngol. 1998;43:289–293. doi: 10.1016/S0165-5876(98)00022-6. [DOI] [PubMed] [Google Scholar]
- 18.Puttamadai GM, Viswanatha B, D’Souza GE. Osteoma mastoid with cholesteatoma of external auditory canal—a rare presentation. Res Otolaryngol. 2014;3(4):53–56. [Google Scholar]
- 19.Dalambiras S, Boutsioukis C, Tilaveridis I. Peripheral osteoma of the maxilla: report of an unusual case. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2005;100(1):e19–e24. doi: 10.1016/j.tripleo.2005.03.011. [DOI] [PubMed] [Google Scholar]
- 20.Prakash MD, Viswanatha B, Shreeharsha M, Patil S. External ear canal osteoma with canal cholesteatoma; a rare association. Res Otolaryngol. 2014;3(5):70–72. [Google Scholar]