

Abstract
Tinnitus, also known as phantom auditory perception, is an annoying symptom and 13–17% of population reports bothersome tinnitus. Cochlear synaptic tinnitus is the most common type. Many treatments have been tried but none is yet considered to be well established. To evaluate effect of Inj.Caroverine and Ginkgo Biloba extract in cochlear synaptic tinnitus in terms of improving tinnitus grading, tinnitus matching and quality of life of patient. It is Randomised controlled study, conducted in department of ENT, on 86 patients, who met inclusion criteria, divided into 4 groups. Gr1—Inj Caroverin, Gr2—Inj Placebo, Gr3—Ginkgo Biloba extract, Gr4—Placebo as extract. A single dose infusion of caroverine immediately improves tinnitus grading and matching and provides immediate relief in reducing severity of tinnitus in 54.54% cases but improvement was not sustained in caroverine group at 3 month and 6 month follow-up after infusion. Ginkgo biloba also is effective in improving tinnitus grading and matching in 31.8% cases and improvement was sustained in ginkgo biloba group even after 3 month of cessation of treatment i.e. at 6 month follow-up. It is suggested that Inj.Caroverine as intravenous infusion should be given in severe cases of tinnitus to reduce its severity immediately and then patient should be put on Tab.Ginkgo biloba for a period of 3 months to provide sustained and long lasting relief. Thus combination therapy of Inj.Caroverin and Tab.Ginkgo Biloba, appropriately tailored to the need of patient will provide better results in greater majority of patients.
Keywords: Tinnitus, Injection caroverine, Ginkgo biloba extract, Cochlear, Cochlear synaptic tinnitus
Background
Although Cochlear synaptic tinnitus is the most common type of tinnitus, studies related to its treatment in Indian population are lacking.
Introduction
Tinnitus may be defined variously, as a sound perceived for more than 5 min at a time in absence of any external acoustical or electrical stimulation of the ear and not occurring immediately after exposure to loud noise, phantom auditory perception [1] or head noise [2].
The prevalence of tinnitus has been estimated to be as high as 32% in the adult population, with approximately 13–17% of population reporting bothersome tinnitus [3]. The severity of tinnitus can range from trivial to completely disabling [4]. Seventy percent of patients reported emotional difficulties due to tinnitus, including frustration, irritation, insecurity and a decreased ability to relax and concentrate [5] (Fig. 1).
| Systematic Tinnitus Classification |
|---|
| Objective tinnitus |
| Subjective tinnitus |
| Conductive tinnitus* |
| Sensorineural tinnitus* |
| Type I (motor tinnitus) |
| Type II (transduction tinnitus) |
| Type III (transformation tinnitus) |
| Type IV (extrasensory tinnitus) |
| Central tinnitus |
| Primary central tinnitus |
| Secondary central (centralized) tinnitus |
*Conductive tinnitus and sensorineural tinnitus form the peripheral tinnitus
Fig. 1.

Systematics of possible generation mechanisms of subjective tinnitus. Conductive tinnitus and sensorineural tinnitus form the peripheral tinnitus. (OHCs outer hair cells, IHCs inner hair cells and CNS central nervous system.)
According to function and anatomy, the following three divisions can be made: conductive tinnitus, sensorineural tinnitus and central tinnitus [6]. These three groups can be distinguished along the same lines as can hearing difficulties.
Cochlear Synaptic Tinnitus
Cochlear synaptic tinnitus is synonyms with signal transfer tinnitus, is a sensorineural tinnitus type III, is used to describe disorders arising during the signal transfer from the IHCs and along the afferent nerve fibres.
Reviews of the evidence for the effective treatment of tinnitus suggest that no treatment can yet be considered well established and no specific therapy is found to be satisfactory in all patients.
Recently, there has been an increased general interest in drug targeting glutamate receptors (caroverine) and studies on caroverine shows promising results in treatment of cochlear synaptic tinnitus. As cochlear synaptic tinnitus is the most common type of tinnitus and these type of studies are lacking in the Indian population so, we undertook the following study to evaluate the effectiveness of caroverine in cochlear synaptic tinnitus and compared it with other treatment modality i.e. ginkgo biloba.
Materials and Methods
The study was conducted on 86 patients who were diagnosed as having cochlear synaptic tinnitus. The cases were registered and given one number for each case. The age, sex, religion, socio-economic status, occupation and address of patients were recorded. The symptoms of the patients were recorded chronologically.
The history of present episode or previous such episodes were recorded. The past history of systemic disorders, ototoxic drug use, was recorded. The familial and personal history including the occupational work conditions, drug abuse (including tobacco), headphone use and life style were also inquired. The thorough clinical examination was carried out which included complete general examination and complete otorhinolaryngological examination.
They were then given/explained a questionnaire adapted from appendix A of University of Denver Tinnitus Centre. The educated patients were given the same to answer whereas in case of the uneducated cases the question were asked and answers were marked accordingly.
After the completion of the questionnaire the patients were given appointment for pure tone audiometry. Then the PTA was done. During the examination the other audiological tests including ART, clinching reflex, Tympanometry, SISI, ABLB and TDT were performed. Tinnitus frequency and loudness match using narrow band sound in the contralateral ear was performed in the same sitting. The masking of tinnitus was done in the diseased ear using narrow band noise
Diagnosis of Cochlear Synaptic Tinnitus
Investigations to confirm cochlear synaptic tinnitus:
Audiometry (0–16,000 Hz)—high frequency loss and sensorineural hearing loss is consistent with the diagnosis of cochlear synaptic tinnitus.
Impedance Audiometry—should be within normal range to exclude middle ear pathologies.
Eustachian Tube function test—should be within normal range
Acoustic Reflex (Ipsi and Contra)—in cochlear synaptic tinnitus the acoustic reflexes will be present at comparatively lesser sound intensity levels due to loudness recruitment.
Clinching Reflex Test—In continuations of acoustic reflex, while testing for 500 and 1000 Hz, once normal reflex are recorded, repeat the recording with clinching of teeths. In case of myoclonus tinnitus there will be significant deepening of the reflexes will be found. In this situations it is in favour of middle ear tinnitus, unless proved otherwise.
Reflex Decay—to exclude retrocochlear pathology. Abnormal decay of acoustic reflex is indicative of retrocochlear pathology.
Tinnitus Matching—has prognostic value
Tinnitus Grading—has prognostic value
S.I.S.I.-scores of 80% to 100% only are typical of cochlear pathology.
BERA is dependable in assessing the nature of pathology, whether conductive or cochlear or retrocochlear.
Selection of Cases
Inclusion Criteria:
Age of patient between 18 and 60 years.
Diagnosis of tinnitus, unilateral or bilateral
Cochlear hearing defect
Reflex audiometry confirming cochlear-synaptic tinnitus and excluding middle ear tinnitus
Written consent after explanation by consultant incharge.
Exclusion Criteria:
Patients NOT willing to give written consent after receiving due instructions.
Reasonable doubts as to the patient’s cooperation
SEVERE SECONDARY DISORDERS (i.e. any acute/chronic illness)
Contra-indication for caroverine therapy (e.g. severe hypertension)
Concomitant symptoms
Pregnancy or plan for having children
Hydrops cochlea or Meniere’s disease
Retrocochlear hearing defect
Blast injury
Status post psychiatrist therapy
Status post operation of the middle ear
Pulse-synchronous tinnitus
Excessive consumption of alcohol, drug or nicotine
Known to intolerance to caroverine
Concomitant medication
Medicative tinnitus therapy within 1 week prior to enrollment
Masticatory movements influencing subjective tinnitus sensation
By using computer generated block randomization method participants were randomized into four groups
GROUP 1- CAROVERINE—patients were infused with a single dose of intravenously 160 mg/8 ml of caroverine in 100 ml of physiological saline at the rate of 2 ml/min.
GROUP 2- CAROVERINE PLACEBO—patients were infused with a single dose of intravenously 8 ml of caroverine placebo in 100 ml of physiological saline at the rate of 2 ml/min.
GROUP 3- GINKGO BILOBA—patients were treated with 60 mg of ginkgo biloba extract 12 hourly for a period of 3 months.
GROUP 4- GINKGO BILOBA PLACEBO—patients were treated with 60 mg of placebo 12 hourly for a period of 3 months.
They were treated accordingly, followed up and evaluated over a period of 6 months for improvement of clinical symptoms in term of tinnitus grading and quality of life.
Result
Most of the patients suffering from cochlear synaptic tinnitus were in fifth decade followed by fourth decade. There was a male preponderance. Left ear tinnitus was most common. Immediate after caroverine infusion there was a significant fall in tinnitus grading and matching of caroverine group. There was a significant fall in tinnitus grading and matching of ginkgo biloba group at 1 month follow-up. At 3 month follow-up, tinnitus grading and matching of caroverine group rises. Whereas, there was a fall in tinnitus grading and matching category of ginkgo biloba group. There was a further rise in tinnitus grading and matching of caroverine group at 6 month follow-up. whereas, there was no change in tinnitus grading and matching of ginkgo biloba group (Table 1; Figs. 2, 3).
Table 1.
Number of responders (patients who show improvement in tinnitus matching and grading)
| Time interval | Group 1 (n = 22) | Group 2 (n = 21) | Group 3 (n = 22) | Group 4 (n = 21 | ||||
|---|---|---|---|---|---|---|---|---|
| No. | % age | No. | % age | No. | % age | No. | % age | |
| Immediate after infusion | 12 | 54.4 | 3 | 13.6 | NA | 0 | 0 | |
| At 1 month | 12 | 54.4 | 0 | 0 | 7 | 31.8 | 0 | 0 |
| At 3 month | 10 | 45.4 | 0 | 0 | 7 | 31.8 | 0 | 0 |
| At 6 month | 9 | 40.9 | 0 | 0 | 7 | 31.8 | 0 | 0 |
Fig. 2.
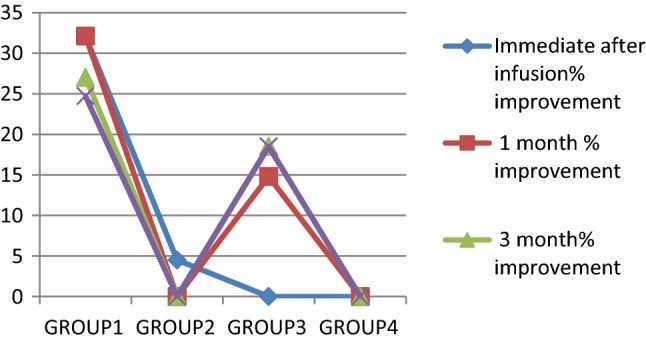
Percentage improvement in mean value of tinnitus grading of different groups with time
Fig. 3.
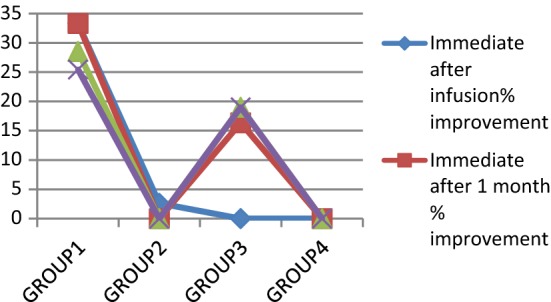
Percentage improvement in mean value of tinnitus matching of different groups with time
Discussion
Tinnitus, “ringing in the ears,” is one of the most common problems encountered in everyday otolaryngology practice. In spite of a long history of tinnitus research and a rapid increase in the understanding of the auditory system, tinnitus remains a mystery. A relatively recent shift towards recognizing that tinnitus is a phantom auditory perception and importance of various structures and systems in the brain have yielded substantial progress in the understanding and treatment of tinnitus. Many treatments have been proposed during last 30 years and the effectiveness of these treatments has increased considerably during this time. Benzodiazepines has been reported to be beneficial in tinnitus treatment [7]. Flunarazine has been demonstrated to reduce tinnitus in a subset of patients suffering from dizziness.
Two randomized controlled studies [8, 9] found carbamazepine effective in controlling the tinnitus ([10]—81%) and ([11]—67%). In Briner [12] attempted to control tinnitus with prostaglandin analogues and according to another double blind placebo controlled study using misoprostal [13] it may provide relief in some patients of tinnitus. In Barany [14] reported relief from tinnitus following lidocaine injection into nasal turbinate. Ehrenberg [15] has performed a study in 1997, to examine whether a single infusion of carovarine, can be used successfully in treatment of tinnitus. Many trials has been reported on effectiveness of Ginkgo biloba [16].
In our study, 86 patients suffering from cochlear synaptic tinnitus were registered. Most of the patients were in fifth decade of life (40.69%) followed by fourth decade of life (22.09%) and age range of patients was from 18 to 60 years. Our data correlated well with the study of Coles [4] who found that prevalence of tinnitus was a positive function of age: 38% of patients were less than 40 years of age and 62% of patients were more than 40 years of age.
In present study male to female ratio was 2.07:1 showing male preponderance. However, our data does not correlate with population statistics that suggest female (57.5%) are more effected than males (42.5%) [3].
In our study 54.4% (12 out of 22) patients responded immediately after infusion of caroverine and 13.6% (3 out of 21) patients responded in placebo group. However, all 3 responders of placebo group reverted back to their pre-treatment level at 1 month follow-up. All the patients who initially responded to caroverine infusion, remained responder at 1 month follow-up in the caroverine group. At 3 month follow-up, two patients who initially responded to caroverine reverted back to pre-treatment level. So the number of responder at 3 month follow-up were 10 (i.e. 45.4%). At 6 month follow-up, one more patient reverted back to pre-treatment level and so, number of responders drop down to 9 (40.9%). One of patient in our study complained of nausea following caroverine infusion which was amenable to intra venous ondansetron. However, none of the patient in caroverine study became symptom free completely.
From our study on caroverine we found that single dose infusion of caroverine is effective in reducing the severity of cochlear synaptic tinnitus but, it cannot abolish the tinnitus, and its effect weans off with time in 25% of responders.
Compared to Prof. Ehrenberg’s study we also found statistically significant improvement in subjective symptom (tinnitus grading) and psycho- acoustic measure (tinnitus matching) (p < 0.05) in the experimental group.
In our study 43 patients of cochlear synaptic tinnitus were randomized and treated either with 2 × 60 mg of oral ginkgo biloba or with placebo and patients were followed-up at 1 month, 3 month and 6 month time interval for observation of improvement in tinnitus matching and grading. In ginkgo biloba group 31.8% (7 out of 22) patients responded at 1 month follow-up, and none responded in control group. At subsequent follow-up responders showed further improvement in tinnitus matching and grading at 3 months. However, plateau occurred at subsequent follow-up at 6 month with no further improvement. No side effects were noted during the 6 months follow-up. Two of the patients in ginkgo biloba group were reported cured after 3 months of treatment. Compared to their study on Ginkgo biloba [16] we also found statistically significant improvement in subjective symptom (tinnitus grading) and psycho- acoustic measure (tinnitus matching) (p < 0.05) in the experimental group.
From our study on ginkgo biloba we found that ginkgo biloba is effective in treating cochlear synaptic tinnitus and response increases with continuation of therapy and its effectiveness persist even after the cessation of treatment.ginkgo biloba can also abolish the tinnitus.
Thus ginkgo biloba seems to be a better drug for control of cochlear synaptic tinnitus. However a further study is needed with a repeat dose of inj. Caroverine in non-responder.
It is finally suggested that inj. Caroverine 160 mg/8 ml in 100 ml of physiological saline as intravenous infusion should be given in severe cases of tinnitus to reduce its severity immediately and then patient should be put on tab. biloba 60 mg twice a day for a period of 3 months to sustained and long lasting relief.
Conclusion
A single dose infusion of caroverine immediately improves tinnitus grading and matching and provides immediate relief in reducing the severity of tinnitus in 54.54% of cases but improvement is not sustained in caroverine group at 3 month and 6 month follow-up after infusion. It reduces to 45.4% at 3 month follow-up and to 40.9% at 6 months follow-up. Ginkgo biloba is also effective in improving tinnitus grading and matching in 31.8% of cases. There is further improvement of tinnitus grading and matching on continuation of treatment but, plateau occurred after cessation of treatment. Improvement was sustained in ginkgo biloba group even after 3 month of cessation of treatment i.e. at 6 month follow-up. Ginkgo biloba takes longer time to improve tinnitus but it provides greater relief on long term follow-up. Due to its sustained effectiveness and no side effect Ginkgo biloba seems to be a better drug for control of cochlear synaptic tinnitus. It is suggested that inj. Caroverine 160 mg/8 ml in 100 ml of physiological saline as intravenous infusion should be given in severe cases of tinnitus to reduce its severity immediately and then patient should be put on tab.ginkgo biloba 60 mg twice a day for a period of 3 months to provide sustained and long lasting relief. Thus our study suggests that combination therapy of Caroverin and Ginkgo Biloba, appropriately tailored to the need of the patient will provide better results in greater majority of patients.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Rajeev Kumar Nishad, Email: drrajeevkumarnishad@gmail.com.
Anil Kumar Jain, Email: jaindranil@gmail.com.
Mangal Singh, Email: drmangalsingh@rediffmail.com.
Reetu Verma, Email: vermareetu001@gmail.com.
Sanyogita Jain, Email: drsajain@gmail.com.
References
- 1.Jastrboff PJ. Phantom auditory perception (tinnitus): mechanism of generation and perception. Neurosci Res. 1990;8:221–254. doi: 10.1016/0168-0102(90)90031-9. [DOI] [PubMed] [Google Scholar]
- 2.Fowler EP. Subjective head noises (tinnitus aurium): genesis and differential, diagnostic significance. A few facts and several speculations. Laryngoscope. 1965;75:1610–1618. doi: 10.1002/lary.5540751013. [DOI] [PubMed] [Google Scholar]
- 3.Cooper JC., Jr Tinnitus, subjective hearing loss and well being. Health and Nutrition Examination Survey of 1971–75: part II. J Am Acad Audiol. 1994;5:37–43. [PubMed] [Google Scholar]
- 4.Coles RRA. Epidemiology of tinnitus: (1) Prevalence and (2) Demographic and clinical features. J Laryngol Otol Suppl. 1984;9(7–15):195–202. doi: 10.1017/S1755146300090466. [DOI] [PubMed] [Google Scholar]
- 5.Tyler RS, Kesely D. Advantages and disadvantages reported by some of the better cochlear- implant patients. Am J Otol. 1990;11:282–289. [PubMed] [Google Scholar]
- 6.Shulman A, Goldstein B. A final common pathway for tinnitus. Implications for treatment. Int Tinnitus J. 1996;2:137–142. [PubMed] [Google Scholar]
- 7.Jhonson RM, Brummett R, Scluening A. Use of Alprazolam for relive of tinnitus. Double blind study. Arch Otolaryngol Head Neck Surg. 1993;119:842–845. doi: 10.1001/archotol.1993.01880200042006. [DOI] [PubMed] [Google Scholar]
- 8.Murai K, Tyler RS, Harker LA, Sttoufer JL. Review of pharmacological treatment of tinnitus. Am J Otol. 1992;13:454–464. [PubMed] [Google Scholar]
- 9.Dobie RA. A review of randomized clinical trial in tinnitus. Laryngoscope. 1999;109:1202–1211. doi: 10.1097/00005537-199908000-00004. [DOI] [PubMed] [Google Scholar]
- 10.Shea JJ, Harell M. Management of tinnitus aurium with lidocaine and carbamazepine. Laryngoscope. 1978;88:1477–1484. doi: 10.1002/lary.1978.88.9.1477. [DOI] [PubMed] [Google Scholar]
- 11.Melding PS, Goodey RJ. The treatment of tinnitus with oral anticonvulsants. J Laryngol Otol. 1973;93:111–122. doi: 10.1017/S0022215100086837. [DOI] [PubMed] [Google Scholar]
- 12.Briner W, House J, O’Leary M. Synthetic prostaglandin E1 misoprostal as a treatment of tinnitus. Arch Otolaryngol Head Neck Surg. 1993;119:652–654. doi: 10.1001/archotol.1993.01880180068013. [DOI] [PubMed] [Google Scholar]
- 13.Yilmaz I, Akkuzu B, Cakmak O, Ozuloglu LN. Misoprostal in treatment of tinnitus: a double blind study. Otolaryngol Head Neck Surg. 2004;130:604–610. doi: 10.1016/j.otohns.2003.08.027. [DOI] [PubMed] [Google Scholar]
- 14.Barany B. Die Beeinflussung des ohrensausens durch intravenous injizierte Lokalanaesthetica. Acta Otolaryngol. 1935;23:201–207. doi: 10.3109/00016483609123219. [DOI] [PubMed] [Google Scholar]
- 15.Ehrenberg K, Denk DM, Heinz H, Franz P. Carovarine in tinnitus treatment. A placebo controlled blind study. Acta Otolaryngol. 1997;117:825–830. doi: 10.3109/00016489709114208. [DOI] [PubMed] [Google Scholar]
- 16.Meyer B. Etude multicentrique randomise a double insuface au placebo du traitment des acouphenes par I’ extrait Ginkgo biloba. La Presse Med. 1986;15(1562):1564. [PubMed] [Google Scholar]