

Abstract
Osteoma of EAC is a rare tumour. Cholesteatoma of EAC associated with osteoma is consequence of osteoma of EAC. Its incidence is rare and very few cases have been reported in the literature. Its association with exuberant granulation tissue in the mastoid air cell system without extension of Cholesteatoma into middle ear cleft is even rare. This association has been reported for the first time as evident from review of literature.
Keywords: Osteoma, EACC—external auditory canal cholesteatoma, Granulation tissue, EAC—external auditory canal, PED—piezoelectric device
Introduction
Osteoma of EAC is slow growing benign tumour that can arise anywhere in the temporal bone. EAC is the most common site of temporal bone osteoma and can occur in all parts of temporal bone including EAC, mastoid, squamous portions, zygomatic process, glenoid fossa, middle ear, Eustachian tube, petrous apex, internal auditory meatus, styloid process [1, 2]. Its exact aetiology is not known. Probably they arise from preosseous connective tissue that localized at the suture line [3]. Because of its solitary, unilateral or slow growing nature, it usually is a symptomatic and discovered incidentally. It may rarely present with conductive hearing loss, recurrent otitis externa, headache or a mass in the EAC. EAC is the commonest site of involvement.
In the temporal bone with estimated incidence of 0.5% of total otalogical surgery [4]. EACC is similarly a rare entity seen in about 0.1–0.5% of new patient [5]. The assosication of osteoma with EAC Cholesteatoma is rare and only few cases have been reported in the literature.
Case report
A 52 years old male patient presented in ENT OPD with complaints of discharge from right ear since 1 year, decrease hearing right ear since 8 months. On examination there was hard bony mass in right EAC. Mass could be negotiated all around except anteriorly. It was hard in consistency.
Tympanic membrane couldn’t be visualized. Pure tone audiometry was suggestive of conductive hearing loss of about 30 db. CT scan of right temporal bone suggestive of bony mass in external auditory canal with soft tissue shadow medial to bony mass and in the middle ear cleft (Fig. 1). Patient was evaluated for fitness for general anesthesia and pathology was explored by post aural approach. Bony mass attached to anterior walls of external auditory canal excised (Fig. 2), EACC and granulation tissue from mastoid air cell system were removed (Fig. 3) and sent for histopathological examination separately. Histopathological report of the bone mass showed mature lamellar bone surrounded by fibro collagenous tissues, consistent with findings of osteoma. Tissue from EAC medial to osteoma was suggestive of Cholesteatoma. Tissue from mastoid air cell system was suggestive of granulation tissues. Since one year there is no evidence of recurrence of disease in this patient.
Fig. 1.

CT axial section of temporal bone showing well circumscribed mass in EAC
Fig. 2.

Picture showing excised osteoma from EAC
Fig. 3.
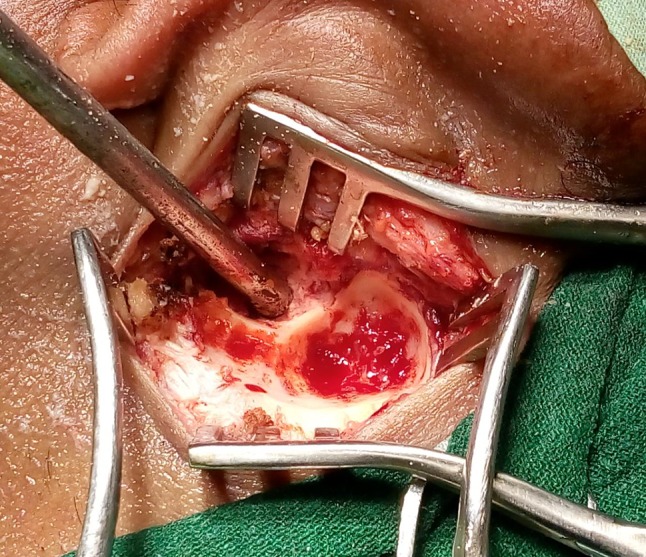
Granulation tissue in the mastoid air cell system without cholesteatoma
Discussion
Osteoma of EAC associated with EACC is rare entity osteoma have been classified in many ways such as unilateral or bilateral, By their pattern of growth into ingrowing or outgrowing and according to histopathological classification into spongeous, compact or mixed [6].
Exact aetiology of osteoma of temporal bone is not known probably they arise from pre-osseous connective tissue most often Localized at suture line [3]. Various aetiological factors have been reported which include trauma, surgery, radiotherapy, chronic infections, hereditary, glandular conditions s.a. pituitary dysfunction [1]. A variety of theories inciting their growth have been suggested from time to time.
Freidberg et al.—Suggested trauma with subsequent ossifying petrositis [7].
Varboncoeur et al.—Suggested that osteoma arise either from an embryological cartilaginous rest or from a persistence embryologic periosteum [8].
Yamasoba et al.—Suggested that osteoma may be congenital in nature based on their reported case of an osteoma that was seen in conjunction with congenital Cholesteatoma [3].
Kaplan et al.—Theoried that a combination of trauma and muscle traction may play a role in the development of osteoma [9].
On CT scan osteoma typically appears as well circumscribed mass without bony destruction. Histologically osteomas are made up of discrete fibrovascular channels surrounded by lamellar bone. Various complications due to osteoma of EAC associated with EACC have been reported in the literature such as neck abscess, cerebellar abscess, FN palsy, meningitis [1].
In our case patient has osteoma which was attached to anterior wall of EAC while in literature almost all patients have osteoma having origin form posterior wall of EAC. In addition to this there was EACC extending medial to osteoma without extension to middle ear cleft but there was exuberant granulation tissue in the mastoid air cell system. The decision regarding treatment will depend upon site, size and symptoms of osteoma and more importantly complications. The symptoms developed mainly due to collection of squamous epithelium in EAC medial to osteoma and its potential to develop into Cholesteatoma and to create complications. Hence surgical removal is treatment of choice.
Piezoelectric device
Osteoma can be removed using this technique. PED is a new bony scalpel using micro vibrations at ultrasonic frequency so that soft tissue will not be damaged even on accidental contact with cutting cup [10].
Conclusion
Osteoma of EAC is benign slow growing tumour and it can be associated with Cholesteatoma of EAC as its secondary effects which may lead to different complications. Hence early surgical intervention is indicated in these patients.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Ethical approval was approved by institutional authority, C.S. Amravati.
Human and animal rights
This article does contain any studies with human or animals.
Informed consent
Informed consent was taken from patient before sending this article to the journal.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vishwanath B. A case of osteoma with cholesteatoma of EAC and cerebellar abscess. Int J Pediatr Otolaryngol. 2007;2(1):34–39. [Google Scholar]
- 2.Fisher EW, Mamanus TC. Surgery for EAC exostoses and osteoma. J Laryngeal Otol. 1994;108:106–110. doi: 10.1017/S0022215100126027. [DOI] [PubMed] [Google Scholar]
- 3.Yamasoba T, Harda T, Okuno T, Nomura Y. Osteoma of ME. Arch Otolaryngol Head Neck Surg. 1990;116(10):1214–1216. doi: 10.1001/archotol.1990.01870100108025. [DOI] [PubMed] [Google Scholar]
- 4.Sheehy JL. Diffuse exostoses and osteoma of EAC, a report of hundred operations. Otolaryngol Head Neck Surg. 1982;90:337–342. [PubMed] [Google Scholar]
- 5.Malcom PN, Francis IS, Weareing MJ, Cox TCS. CT appearances of EAC cholestestoma. Br J Radiol. 1997;70:959–960. doi: 10.1259/bjr.70.837.9486076. [DOI] [PubMed] [Google Scholar]
- 6.Sente M. External auditory canal osteoma. Srp Arch Celok Lek. 2009;137:73–76. doi: 10.2298/SARH0902073S. [DOI] [PubMed] [Google Scholar]
- 7.Freidberg SA. Osteoma of mastoid process. Arch Otolaryngol. 1938;28:20–26. doi: 10.1001/archotol.1938.00650040027003. [DOI] [Google Scholar]
- 8.Varboncoeur AP, Vanbelois HJ, Bowen LL. Osteoma of maxillary sinus. J Oral Maxillofac Surg. 1990;48(8):882–883. doi: 10.1016/0278-2391(90)90351-2. [DOI] [PubMed] [Google Scholar]
- 9.Kaplan I, Colderon S, Buchner A. Peripheral osteoma of mandible: a study of ten new cases and analyses of literature. J Oral Maxillofac Surg. 1994;52(5):467–470. doi: 10.1016/0278-2391(94)90342-5. [DOI] [PubMed] [Google Scholar]
- 10.Salami AD, Mora R, Dellepiane M, Vercellotti T. Piezoelectric bone surgery in otologic surgery. Otolaryngol Head Neck Surg. 2007;136:484–485. doi: 10.1016/j.otohns.2006.10.045. [DOI] [PubMed] [Google Scholar]