

Abstract
Introduction
Above half of mothers in Ethiopia give birth at home. Home based care within the first week after birth as a complementary strategy to facility-based postnatal care service is critical to increase the survival of both mothers and newborns. However, evidence on utilization of postnatal care and location of service among mothers who delivered at home in Ethiopia is insufficiently documented. Therefore, this study assessed the magnitude and determinants for place of postnatal care service utilization among mothers who delivered at home in Ethiopia.
Methods
We used the 2016 Ethiopian Demographic and Health Survey, and extracted data from 4491 mothers who delivered at home during 5 years preceding the survey. A multinomial logistic regression model was applied to examine the determinants of both facility and home -based postnatal care service utilization. Likelihood ratio test was used to see the model fitness and p-value of < 0.05 was used to determine statistical significance at 95% confidence interval.
Results
From the total 4491 mothers who delivered at home, only 130(2.9%) and 236(5.3%) of them utilized postnatal service at home and at a health facility respectively. Being from an urban region (AOR = 0.378, 95%CI: 0.193–0.740), ever using the calendar method to delay pregnancy (AOR = 0.528, 95%CI: 0.337–0.826), receiving four and above antenatal care visits (AOR = 0.245, 95%CI: 0.145–0.413) and having a bank account (AOR = 0.479, 95%CI: 0.243–0.943) were the factors associated with utilizing home- based postnatal care. Similarly being a follower of the orthodox religion (AOR = 1.698, 95%CI: 1.137–2.536), being in the rich wealth index (AOR = 0.608, 95%CI: 0.424–0.873), ever using the calendar method to delay pregnancy (AOR = 0.694, 95%CI: 0.499–0.966), wantedness of the pregnancy (AOR = 0.264, 95%CI: 0.352–0.953), receiving four and above antenatal care visits (AOR = 0.264, 95%CI: 0.184–0.380) and listening to radio at least once a week (AOR = 0.652, 95%CI: 0.432–0.984) were the determinants of facility-based postnatal care utilization.
Conclusion
The coverage of postnatal care service utilization among mothers who delivered at home was very low. Living in urban region, following the Orthodox religion, having higher wealth index, having a bank account, ever using calendar method to delay pregnancy, wantedness of the pregnancy, receiving four and above antenatal care visit and listening to radio at least weakly were associated with postnatal care service utilization. Therefore, targeted measures to improve socio-economic status, strengthen the continuum of care, and increase health literacy communication are critically important to increase postnatal care service utilization among women who deliver at home in Ethiopia.
Keywords: Postnatal care, Home delivery, Maternal service utilization, Place for PNC, Ethiopia
Plain English summary
Postnatal care is the care given to the mother and her newborn baby immediately after the birth and for the first 6 weeks postpartum irrespective of place of delivery. In Ethiopia evidence on utilization of postnatal care for mothers who delivered at home is insufficiently documented. Using national health survey data, this study sought to illuminate the magnitude, location and factors associated with postnatal care utilization among mothers who deliver at home in Ethiopia.
Data on mothers who delivered at home within the 5 years preceding the survey were taken from the nationally representative dataset. Accordingly 4491 mothers were included in the analysis.
The coverage of postnatal care service utilization among home delivered mothers was very low. In this study only 366(8.2%) of mothers who delivered at home received postnatal care. Living in an urban region, following the Orthodox religion, being in a high wealth index, having a bank account, ever used calendar to delay pregnancy, wantedness of the pregnancy, receiving four or more antenatal care visits and listening to radio at least weakly were associated with postnatal care utilization.
Targeted measures to improve socio-economic status, and strengthen awareness of postnatal care service and health literacy communications about postnatal care are critically important to increase postnatal care service utilization among women delivering at home.
Introduction
The early postnatal period, particularly the first hours of life, extending into the first 2–3 days of life is a period of high risk for both mothers and newborns [1–3]. The risk is more severe in communities where the overwhelming majority of births occur at home [4, 5]. In such communities unless safe household practices are followed and care is provided by health workers, undoubtedly catastrophic adverse outcomes will persist [1, 6]. Based on evidence, the World Health Organization (WHO) recommends home-based postnatal care (PNC) care for mothers and newborns in the first week of life as a complementary strategy to facility-based PNC in order to improve mothers and newborns survival [1, 7, 8].
Studies had shown that home-based newborn care interventions can prevent 30–61% of newborn deaths in high mortality settings and can lower the odds of maternal postpartum distress [9].
A home-based care strategy to promote an integrated package of preventive and curative newborn care is effective in reducing neonatal mortality in communities, even within a weak health system, especially if it is given by trained health professionals such as midwives [6, 9]. However, providing this service and ensuring optimal practices is not straightforward for many reasons such as staff shortages, and inconvenient transportation, which results in low to moderate home visitation coverage for PNC even with intensive support [1, 7]. Though they do not replace antenatal care (ANC), home visits by the community health workers during pregnancy were higher than the visits after birth [1, 10–12].
For institutional births, opportunities already exist to provide PNC to mothers and newborns before discharge [1]. However, even at health facility level, in Sub-Saharan Africa women are often discharged before 24 hrs, which limits them from receiving the WHO’s recommended services. Additionally visits at 72 hrs and seventh day are rare [13]. For home births, some mothers and babies access early postnatal care through a visit to a health facility. However, many cannot or do not receive facility-based PNC following home deliveries, leaving home visitation as a potentially attractive way to make such care available [1].
In Ethiopia, the maternal mortality ratio is still high; 412 maternal deaths out of 100,000 live births. Maternal mortality ratio has been reduced over the past two decades though still it remains high, with most maternal deaths happening during the postpartum period [14, 15]. The country has a significant proportion (above half, 52%) of home deliveries, and has been implementing PNC through home visitation as one of the interventions to reduce maternal and child morbidity and mortality [1, 16]. In Ethiopia, the Health Management Information System (HMIS) has indicators used to monitor the implementation of PNC for mothers and babies, which includes both health facility and home visits [7]. However, PNC coverage is very low with 42–48% of mothers delivering in a health facility receiving PNC, and only 1–2% of women delivering at home receiving PNC in the first 2 days of postpartum period [1, 14].
The main reasons listed for low PNC utilization in studies of different countries range from low awareness about the need to fear of health facilities [17, 18]. Furthermore mothers who deliver at home may experience discrimination in receiving PNC due to some locally practiced measures like financial penalties for home births [18, 19]. Moreover; the perspective of women, their families and community on the quality of service could influence their decision whether or not to seek care [20, 21].
Maternal, newborn and child health issues are national priorities of many countries. However, specific policies for postpartum care are weak, and there is a very little evidence of effective PNC implementation [7, 13]. The ideal way to provide maternal and child health services such as PNC is through health services delivered by skilled personnel in health facilities. However, in developing countries like Ethiopia, a more realistic model requires working hard to strengthen the health system and improve access to facility-based care, while also enabling access to PNC at the community level through home visit [13, 22].
Comprehensive studies on utilization of PNC through facility-based and home-based care are rare. However, having such inclusive evidence is critically important to develop appropriate strategies to help improve the low service utilization and reduce the maternal and newborn morbidity and mortality, especially if the evidence is derived from country specific data like the Demographic Health Surveys. Therefore, this study aimed to assess the utilization of PNC and its determinants among mothers who delivered at home in Ethiopia.
Methods
Data source and study design
This was a cross-sectional secondary analysis of data collected in the 2016 Ethiopian Demographic Health Survey (EDHS). It is the fourth EDHS conducted by the Central Statistical Agency as part of the International Demographic and Health Survey program. The data for mothers who delivered at home were extracted from the pregnancy and PNC dataset of the EDHS 2016 and included. We only included the most recent child of the women so as to avoid mix-ups in the recall and reporting of mothers experiences, especially for mothers who had more than one birth in the previous 5 year period. Additionally, mothers who did not remember the PNC they received for either the mother herself or her newborn were excluded from analysis. Therefore, a total of 4491 mothers (between 15 and 49 years) were included in this study.
Outcome variable
To develop the outcome variable from the dataset the question “where did you give birth?” was used as a starting point for this study. According to this question the dataset is categorized in to two subgroups i.e. “1=health facility delivery” and “2 = home delivery”. Accordingly, from the total (N = 7188) mothers, 37.5% (n = 2697) delivered at a health facility and 62.5% (n = 4491) of them gave birth at home. The latter subgroup was used as our study participants in this study. Using the responses to the questions “Did anyone check on your health after you gave birth?” and “In the two months after delivery, did anyone check the health of your child?” we determined how many mothers and newborns received postnatal care services. According to the WHO, PNC service is defined as service given for both the mother and her newborn within 42 days of delivery [2]. However, the EDHS 2016 dataset contained data for care provided to newborns extending up-to 2 months. This does not contradict to the WHO’s definition rather it is better to give comprehensive understanding on the community based newborn care (CBNC) program which is being implemented as an intervention to decrease the high ratio of newborn deaths in the country [23].
For mothers who indicated that they had been “Checked by anyone”, we used the questions “Where did your first health check take place?” and “Where did your child’s first health check take place?” Responses categorized “at health facility” included those who were checked at governmental, private and NGO health facilities and “at home” was used to define those receiving PNC at home. Since PNC includes services for both the newborn and the mother, we consider checked at home and health facility for either of the two (mother or her newborn) or both for those who were checked by Doctor, Nurse, Midwife, Health Officer or Health Extension Worker using the data on the questions “who checked your health at that time?” and “who checked your child’s at that time?”. Respondents who were checked by traditional birth attendants and other family members were considered as not receiving PNC.
The outcome variable was “place of PNC utilization” which was categorized in to three levels: 1) At home when either the mother or newborn or both were checked at home by a health personnel after giving birth at home, 2) At health facility when either of mother or newborn or both were checked at health facility after giving birth at home and 3) Not utilized at all when neither the mother nor newborn were checked by a trained personnel either at home or at a health facility a giving birth at home.
Independent variables
The independent variables included socio-demographic factors (age, marital status, educational status, place of residence, region type, religion, number of family members and sex of family head), socio-economic factors (wealth status, respondent’s and husband’s occupation, having a bank account and autonomy for health service utilization) and maternal health service, and health literacy communication related factors (wantedness of the last child, ever using anything to delay pregnancy, ANC utilization and frequency, awareness on fistula, owning a mobile phone and frequency of listening to radio).
Data analysis
Frequencies and proportions were used to describe categorical variables using cross tabulation. Multi-collinearity was checked using Variance Inflation Factor (VIF) test and variables with value of > 5 were excluded from the model. Multinomial logistic regression model was applied to identify determinants of place of postnatal care service utilization. Likelihood ratio test was used to see the model fitness and the value was 0.000 which showed the model was well-fitted. The adjusted odds ratio (AOR) was reported with their 95% confidence interval, and a p-value of < 0.05 was considered to declare statistical significance. The overall correct predicted classification of the model in this analysis was 91.9%.
Results
Socio-demographic characteristics
Among young mothers (15–24 years of age) who delivered at home, only 4.5% (n = 48) utilized PNC at a health facility and more than 90% (n = 980, 92.9%) did not utilize PNC at all. Among urban and rural residents, 14% (n = 36) and 7.8% (n = 330) utilized PNC service at a health facility or home respectively. A slightly higher percentage of mothers with 1–4 family members utilized PNC either at home or at a health facility (8.4%) compared to mothers with > 8 number of family members (6.7%) (Table 1).
Table 1.
Socio-demographic characteristics of study women by place of postnatal care service utilization in Ethiopia, analysis from EDHS 2016
| Variable | Place of PNC Utilization | |||
|---|---|---|---|---|
| At Home n (%) |
At Health Facility n (%) |
Not utilized at all n (%) | Total N (%) |
|
| Age group | ||||
| 15–24 years | 27 (2.6) | 48 (4.5) | 980 (92.9) | 1055 (100) |
| 25–34 years | 70 (3.2) | 120 (5.5) | 2001 (91.3) | 2191 (100) |
| 35–49 years | 33 (2.7) | 68 (5.5) | 1144 (91.8) | 1245 (100) |
| Marital status | ||||
| Married/lived w p. | 123 (2.9) | 216 (5.1) | 3872 (91.6) | 4211 (100) |
| Others | 7 (2.5) | 20 (7.1) | 253 (90.4) | 280 (100) |
| Educational status | ||||
| Not Educated | 91 (2.7) | 149 (4.4) | 3152 (92.9) | 3392 (100) |
| Primary and above | 39 (3.5) | 87 (7.9) | 973 (88.5) | 1099 (100) |
| Religion | ||||
| Orthodox Christian | 40 (3.5) | 103 (9.1) | 991 (87.4) | 1134 (100) |
| Muslim | 61 (2.6) | 86 (3.7) | 2166 (93.6) | 2313 (100) |
| Others | 29 (2.8) | 47 (4.5) | 968 (92.7) | 1044 (100) |
| Place of residence | ||||
| Urban | 8 (3.1) | 28 (10.9) | 220 (85.9) | 256 (100) |
| Rural | 122 (2.9) | 208 (4.9) | 3905 (92.2) | 4235 (100) |
| Region | ||||
| Agrarian | 62 (2.8) | 149 (6.7) | 2019 (90.5) | 2230 (100) |
| Pastoralists | 52 (2.7) | 65 (3.3) | 1824 (94) | 1941 (100) |
| Urban administration | 16 (5.0) | 22 (6.9) | 282 (88.1) | 230 (100) |
| No family members | ||||
| 1–4 | 33 (2.7) | 68 (5.7) | 1101 (91.6) | 1202 (100) |
| 5–7 | 65 (2.9) | 128 (5.8) | 2023 (91.3) | 2216 (100) |
| > = 8 | 32 (3.0) | 40 (3.7) | 1001 (93.3) | 1073 (100) |
| Sex of household head | ||||
| Male | 106 (3.0) | 192 (5.4) | 3266 (91.6) | 3564 (100) |
| Female | 24 (2.6) | 44 (4.7) | 859 (92.7) | 927 (100) |
| Partner’s Educational level | ||||
| No education | 56 (2.2) | 109 (4.3) | 2360 (93.5) | 2525 (100) |
| Primary | 53 (4.0) | 86 (6.5) | 1180 (89.5) | 1319 (100) |
| Secondary and above | 14 (3.8) | 21 (5.7) | 332 (90.5) | 367 (100) |
p partner, Educ Educational
Socio-economic characteristics
A higher proportion of mothers in the highest wealth index utilized PNC either at home or health facility than participants in the lowest wealth index (14.4 and 5.5% respectively). Furthermore, mothers with a bank account were more likely to utilize PNC either at health facility or home compared to participants without bank account (20.8% (n = 38) and 7.6% (n = 328) respectively) (Table 2).
Table 2.
Socio-economic characteristics of study women by place of postnatal care service utilization in Ethiopia, analysis from EDHS 2016
| Variable | Place of PNC Utilization | |||
|---|---|---|---|---|
| At Home n (%) |
At Health Facility n (%) |
Not utilized at all n (%) | Total N (%) |
|
| Wealth Index | ||||
| Poorer | 62 (2.1) | 100 (3.4) | 2746 (94.4) | 2908 (100) |
| Middle | 31 (4.4) | 46 (6.6) | 625 (89.0) | 702 (100) |
| Richer | 37 (4.2) | 90 (10.2) | 754 (85.6) | 8891 (100) |
| Husband’s occupation | ||||
| Agricultural work | 85 (3.1) | 131 (4.9) | 2483 (92.0) | 2699 (100) |
| Others | 38 (2.5) | 85 (5.6) | 1389 (91.9) | 1512 (100) |
| Participant’s occupation | ||||
| No work | 65 (2.4) | 102 (3.8) | 2534 (93.8) | 2701 (100) |
| Agricultural work | 35 (3.3) | 73 (6.9) | 943 (89.7) | 1051 (100) |
| Others | 30 (4.1) | 61 (8.3) | 648 (87.7) | 739 (100) |
| Autonomy to utilize PNC | ||||
| Self | 23 (3.5) | 41 (6.2) | 602 (90.4) | 666 (100) |
| Self and partner | 70 (2.7) | 134 (5.2) | 2380 (92.1) | 2584 (100) |
| Partner alone | 29 (3.0) | 41 (4.3) | 882 (92.6) | 952 (100) |
| Others | 8 (2.8) | 20 (6.9) | 261 (90.3) | 289 (100) |
| Has bank account | ||||
| No | 117 (2.7) | 211 (4.9) | 3981 (92.4) | 4309 (100) |
| Yes | 13 (7.1) | 25 (13.7) | 144 (79.1) | 182 (100) |
Health service and health literacy communication related characteristics
About 12% (n = 105) of mothers who had received 4+ ANC visits utilized PNC at health facility, while only 2.4% (n = 55) of mothers who did not receive ANC utilized PNC at health facility. Furthermore 19% (n = 148) of mothers who were told about pregnancy danger signs during their ANC visit utilized PNC at home or a health facility, compared to only 10% (n = 139) of mothers who were not counseled on danger signs during ANC. A higher proportion of mothers who were aware of fistula utilized PNC at home or health facility compared to those who were not aware of fistula (12.1 and 6.7% respectively) (Table 3).
Table 3.
Maternal health service and health literacy communication related characteristics of study women by place of postnatal care service utilization in Ethiopia, analysis from EDHS 2016
| Variable | Place of PNC Utilization | |||
|---|---|---|---|---|
| At Home n (%) |
At Health Facility n (%) |
Not utilized at all n (%) | Total N (%) |
|
| Number of ever born children | ||||
| 1–2 children | 32 (2.6) | 64 (5.3) | 1112 (92.1) | 1208 (100) |
| 3–4 children | 37 (3.0) | 72 (5.8) | 1143 (91.3) | 1252 (100) |
| > = 5 children | 61 (3.0) | 100 (4.9) | 1870 (92.1) | 2031 (100) |
| Number of living children | ||||
| 4 and bellow | 77 (2.8) | 158 (5.7) | 2536 (91.5) | 2771 (100) |
| 5 and above | 53 (3.1) | 78 (4.5) | 1589 (92.4) | 1720 (100) |
| Ever used anything to delay pregnancy | ||||
| No | 53 (1.9) | 88 (3.1) | 2683 (95.0) | 2824 (100) |
| Used outside calendar | 8 (6.2) | 13 (10.1) | 108 (83.7) | 129 (100) |
| Used in calendar | 69 (4.5) | 135 (8.8) | 1334 (86.7) | 1538 (100) |
| Wanted pregnancy when become pregnant | ||||
| Then | 96 (2.7) | 159 (4.4) | 3350 (92.9) | 36.5 (100) |
| Later | 28 (4.9) | 53 (9.2) | 495 (85.9) | 576 (100) |
| No more | 6 (1.9) | 24 (7.7) | 280 (90.3) | 310 (100) |
| Number of ANC Visits | ||||
| No ANC visit | 25 (1.1) | 55 (2.4) | 2229 (96.5) | 2309 (100) |
| 1–3 visits | 58 (4.6) | 76 (6.0) | 1137 (89.5) | 1137 (89.5) |
| > =4 visits | 47 (5.2) | 105 (11.5) | 759 (83.3) | 911 (100) |
| Told about pregnancy danger signs | ||||
| Have no ANC visit | 24 (1.0) | 55 (2.4) | 2219 (96.6) | 2298 (100) |
| Not told | 50 (3.6) | 89 (6.3) | 1264 (90.1) | 1403 (100) |
| Told | 56 (7.1) | 92 (11.6) | 642 (81.3) | 790 (100) |
| Told about birth preparedness plan | ||||
| No ANC visit (N/A) | 24 (1.0) | 55 (2.4) | 2219 (96.6) | 2298 (100) |
| No | 41 (3.4) | 66 (5.5) | 1102 (91.1) | 1209 (100) |
| Yes | 65 (6.6) | 115 (11.7) | 804 (81.7) | 984 (100) |
| Size of newborn at birth | ||||
| Larger than average | 35 (2.8) | 61 (4.9) | 1144 (92.3) | 1240 (100) |
| Average | 59 (3.1) | 105 (5.6) | 1720 (91.3) | 1184 (100) |
| Small than average | 36 (2.6) | 70 (5.1) | 1261 (92.2) | 1367 (100) |
| Ever heard of fistula | ||||
| No | 77 (2.3) | 143 (4.4) | 3062 (93.3) | 3282 (100) |
| Yes | 53 (4.4) | 93 (7.7) | 1063 (87.9) | 1209 (100) |
| Owns mobile telephone | ||||
| No | 113 (2.9) | 190 (4.8) | 3644 (92.3) | 3947 (100) |
| Yes | 17 (3.1) | 46 (8.5) | 481 (88.4) | 544 (100) |
| Frequency of listing to radio | ||||
| Not at all | 94 (2.5) | 165 (4.5) | 3448 (93.0) | 3707 (100) |
| Less than once a week | 19 (4.6) | 34 (8.2) | 361 (87.2) | 414 (100) |
| At least once a week | 17 (4.6) | 37 (10.0) | 316 (85.4) | 370 (100) |
N/A Not Applicable
Magnitude of PNC utilization
From the total 4491 mothers who delivered at home included in the study, 130 (2.9%) utilized postnatal service at home, while 236 (5.3%) of them utilized PNC at a health facility (Fig. 1).
Fig. 1.
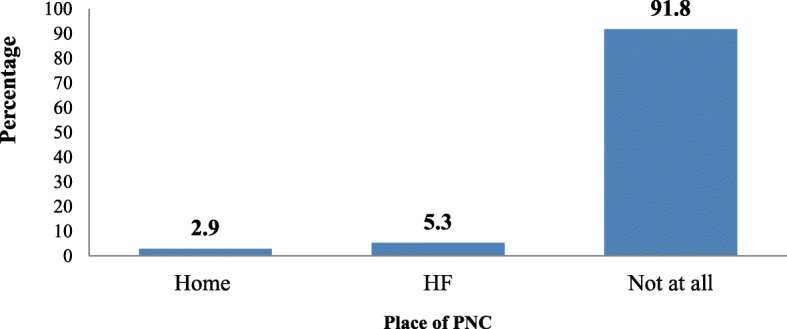
Place of postnatal care utilization among home delivered
mothers in Ethiopia, analysis of EDHS 2016
Factors affecting postnatal care utilization
Type of region (agrarian, pastoralist or urban) where mothers live, ever using anything to delay pregnancy, receiving ANC and having a bank account were all significant factors affecting home-based postnatal care utilization. Participants from agrarian regions were 62.2% less likely to receive PNC at home than not utilizing at all when compared to participants from urban areas (AOR = 0.378, 95%CI 0.193–0.740). Participants who had not ever used anything to delay pregnancy were 47.2% less likely (AOR = 0.528, 95%CI 0.337–0.826) to receive PNC at home than not utilizing at all when compared to those used calendar as method of delay to pregnancy. Furthermore participants with > 4 ANC visits were 4 times (AOR = 4.1, 95%CI 2.42–6.88) more likely to receive PNC at home than not utilizing at all when compared to those who have no ANC visit. Participants without a bank account were approximately half as less likely (AOR = 0.479, 95%CI 0.243–0.943) to receive PNC at home when compared to participants with a bank account (Table 4).
Table 4.
Coefficients of multinomial logistic regression on place of PNC utilization in Ethiopia, analysis from EDHS 2016
| Predictor variables | Multinomial Logit Model | |||||||
|---|---|---|---|---|---|---|---|---|
| Utilizes PNC at home versus not utilized at all | Utilizes PNC at HF versus not utilized at all | |||||||
| 95%CI | 95%CI | |||||||
| P-value | AOR | Lower bound | Upper bound | P-Value | AOR | Lower bound | Upper bound | |
| Age group | ||||||||
| 15–24 years | 0.571 | 1.241 | 0.588 | 2.618 | 0.306 | 0.745 | 0.423 | 1.310 |
| 25–34 years | 0.366 | 1.250 | 0.770 | 2.030 | 0.458 | 0.868 | 0.596 | 1.262 |
| 35–49 years RC | ||||||||
| Region | ||||||||
| Agrariana | 0.005 | 0.378 | 0.193 | 0.740 | 0914 | 0.969 | 0.551 | 1.704 |
| Pastoralistsb | 0.466 | 0.788 | 0.415 | 1.496 | 0.800 | 0.929 | 0.526 | 1.640 |
| Urban adminc RC | ||||||||
| Place of residence | ||||||||
| Urban | 0.105 | 0.498 | 0.215 | 1.158 | 0.840 | 1.057 | 0.615 | 1.816 |
| Rural RC | ||||||||
| Educational status | ||||||||
| Not Educated | 0.740 | 1.080 | 0.685 | 1.705 | 0.139 | 0.778 | 0.558 | 1.085 |
| Primary and above RC | ||||||||
| Religion | ||||||||
| Orthodox Christian | 0.798 | 1.073 | 0.624 | 1.847 | 0.010 | 1.698 | 1.137 | 2.536 |
| Muslim | 0.889 | 0.964 | 0.572 | 1.623 | 0.423 | 1.181 | 0.786 | 1.777 |
| Othersd RC | ||||||||
| Number of family members | ||||||||
| 1–4 | 0.845 | 0.939 | 0.479 | 1.839 | 0.130 | 1.498 | 0.888 | 2.527 |
| 5–7 | 0.590 | 0.875 | 0.538 | 1.422 | 0.121 | 1.380 | 0.918 | 2.074 |
| > = 8 RC | ||||||||
| Sex of household head | ||||||||
| Male | 0.592 | 0.868 | 0.518 | 1.456 | 0.754 | 0.937 | 0.622 | 1.411 |
| FemaleRC | ||||||||
| Wealth Index | ||||||||
| Poor | 0.154 | 0.696 | 0.423 | 1.146 | 0.007 | 0.608 | 0.424 | 0.873 |
| Middle | 0.466 | 1.216 | 0.718 | 2.061 | 0.257 | 0.791 | 0.527 | 1.187 |
| Rich RC | ||||||||
| Ever used anything to delay pregnancy | ||||||||
| No | 0.005 | 0.528 | 0.337 | 0.826 | 0.030 | 0.694 | 0.499 | 0.966 |
| Used outside calendar | 0.410 | 1.396 | 0.631 | 3.091 | 0.466 | 1.264 | 0.673 | 2.376 |
| Used in calendar RC | ||||||||
| Wanted Pregnancy when become pregnancy | ||||||||
| Then | 0.465 | 1.388 | 0.576 | 3.345 | 0.031 | 0.579 | 0.352 | 0.953 |
| Later | 0.051 | 2.544 | 0.998 | 6.486 | 0.894 | 1.038 | 0.597 | 1.805 |
| No more RC | ||||||||
| Number of ANC Visits | ||||||||
| Have no ANC visit | 0.000 | 0.245 | 0.145 | 0.413 | 0.000 | 0.264 | 0.184 | 0.380 |
| 1–3 visits | 0.826 | 0.955 | 0.634 | 1.439 | 0.001 | 0.568 | 0.412 | 0.784 |
| > =4 visits RC | ||||||||
| Marital status | ||||||||
| Married/lived with partner. | 0.745 | 1.156 | 0.483 | 2.770 | 0.876 | 0.955 | 0.535 | 1.705 |
| Otherse RC | ||||||||
| Participant’s occ. | ||||||||
| No work | 0.225 | 0.745 | 0.462 | 1.200 | 0.065 | 0.711 | 0.495 | 1.022 |
| Agricultural work | 0.446 | 0.812 | 0.475 | 1.387 | 0.999 | 1.000 | 0.672 | 1.489 |
| Others fRC | ||||||||
| Ever heard of fistula | ||||||||
| No | 0.064 | 0.697 | 0.476 | 1.021 | 0.264 | 0.844 | 0.627 | 1.136 |
| Yes RC | ||||||||
| Number of living children | ||||||||
| 4 and bellow | 0.3688 | 0.692 | 0.310 | 1.544 | 0.200 | 1.423 | 0.830 | 2.440 |
| 5 and above RC | ||||||||
| Frequency of listing radio | ||||||||
| Not at all | 0.196 | 0.691 | 0.394 | 1.210 | 0.041 | 0.652 | 0.432 | 0.984 |
| Less than once a week | 0.606 | 0.933 | 0.416 | 1.668 | 0.235 | 0.731 | 0.435 | 1.227 |
| At least once a week RC | ||||||||
| Owns mobile telephone | ||||||||
| No | 0.298 | 1.376 | 0.755 | 2.511 | 0.311 | 0.806 | 0.530 | 1.224 |
| Yes RC | ||||||||
| Has bank account | ||||||||
| No | 0.033 | 0.479 | 0.243 | 0.943 | 0.642 | 0.886 | 0.532 | 1.476 |
| Yes RC | ||||||||
| Ever born children | ||||||||
| 1–2 children | 0.789 | 0.876 | 0.333 | 2.305 | 0.152 | 0.622 | 0.325 | 1.192 |
| 3–4 children | 0.827 | 1.094 | .489 | 2.449 | 0.299 | 0.757 | 0.448 | 1.280 |
| > = 5 children RC | ||||||||
| Size of the newborn at birth | ||||||||
| Larger than average | 0.785 | 0.934 | 0.573 | 1.524 | 0.374 | 0.845 | 0.583 | 1.225 |
| Average | 0.676 | 1.097 | 0.711 | 1.693 | 0.908 | 0.981 | 0.708 | 1.358 |
| Smaller than average | ||||||||
a Tigray, Amhara, Oromo, and South nation nationality and peoples. bAfar, Gambella, Benishangule, and Somalia, cAddis-Ababa, Harrar and Drie-Dawa. dCatholic, Protestant and Others. e Single, divorced, widowed, separated. fDaily laborer, industrial work and others.
AOR Adjusted Odds Ratio. RC Reference Category
Boldfaces significant variables at p < 0.05
Similar to the findings on factors associated with receiving PNC at home, there were a number of factors associated with receiving PNC at a facility among women who delivered at home. Religion, wealth index, ever using anything to delay pregnancy, wantedness of the pregnancy, ANC visits and listening to radio were associated with facility-based PNC utilization. Women who follow the Orthodox religion were 69% more likely (AOR = 1.698, 95%CI 1.137–2.539) to utilize PNC at a health facility than not utilizing at all when compared to women whose religion was “others”(not orthodox or Muslim). Mothers in the low wealth index were 40% less likely (AOR = 0.608, 95%CI 0.424–0.873) to utilize PNC at a health facility than not utilizing at all when compared to women in the upper wealth index. Women who wanted their pregnancy were 42% less likely (AOR = 0.579, 95%CI 0.352–0.953) to utilize PNC at a health facility than not utilizing at all when compared with women who had not want to became pregnant. Lastly, listening to radio was associated with PNC utilization in a health facility; women who did not listen to radio at all were 34.8% less likely (AOR = 0.652, 95%CI 0.432–0.984) to utilize PNC at a health facility than not utilizing at all when compared with women who listened to radio at least once a week when other variables were held constant (Table 4).
Discussion
This study used data from the 2016 DHS assessment in Ethiopia-the fourth survey to capture detailed information on maternal and newborn health in general and PNC services in particular at national level. In this paper we have explored the coverage of home-based and facility-based PNC utilization among mothers who delivered at home, and factors associated with place of PNC service utilization in Ethiopia. Below we will discuss the implications of the study findings for program, policy and future research in Ethiopia.
This study shows that only 8.2% of mothers who delivered at home utilized PNC services (2.9% of mothers received at home and 5.3% a health facility). Analysis of the factors associated with place of PNC utilization in the study show that region type, religion, wealth index, having a bank account, ever using anything to delay pregnancy, wantedness of pregnancy, antenatal care visits, and radio listening appear to be important factors for PNC utilization either at home or facility in Ethiopia.
In this study, the magnitude of PNC utilization either at home or at a health facility was similar with findings from some studies [1, 24–26] though lower than the findings from other studies [11, 13, 27–30]. This difference could be due to differences in the schedule of visits considered in the different studies, which could affect the comparability and results between the different studies [1]. Additionally, it could reflect differences in the socio-demographic and socio-economic characteristics of the study populations. Furthermore, these studies may have included PNC given at a health facility to women who delivered in health facilities, which would be expected to be higher compared to a study like ours’, which only considered mothers who delivered at home.
In our study, mothers from urban regions were more likely to utilize PNC at home compared to participants from agrarian regions while there was no statistically significant variation in PNC utilization in a facility by region type. Being from urban regions (Addis Ababa, Dire-Dawa, and Harrar) could expose women to improved awareness and good access to trained professionals [24, 31] even to mobile home-based care. Utilization of services that precede PNC, including ever using anything to delay pregnancy and receiving ANC were two other factors which were significantly associated with PNC service utilization, both at home and at a health facility. This is not surprising, as many other studies [28–30, 32–37] found similar findings. It is plausible that if mothers had previous contact with health professionals (especially for ANC), they would be more likely to seek PNC at a health facility or to have contact with a community health worker after giving birth to receive PNC at home [1, 32, 38].
Surprisingly, although the vast majority of women wanted the pregnancy at the time they became pregnant (80%, n = 3605), women who did not wish to become pregnant then were more likely to utilize PNC at health facilities compared to those who wanted the pregnancy when they become pregnant. This may be related a higher incidence of complications developing after birth among those with unwanted pregnancies. Additionally, findings from other studies have revealed that mothers may not seek care at health facilities if they did not develop complications [1, 18, 39, 40], and those who did not want the pregnancy may develop more complications than those who wanted it.
Media exposure was also associated with PNC service utilization, women who listened to radio at least once a weak were more likely to utilize PNC at a health facility compared to those who did not listen to radio at all. Media exposure could improve the awareness of women of the value of seeking care [41], including PNC, even among mothers who gave birth at home.
Furthermore, mothers with a bank account were more likely to utilize PNC at home than those without bank account, and mothers from the highest wealth index were more likely to receive PNC at a health facility compared to women in the lowest wealth index. These findings are similar with other findings [31, 42–44]. A possible pathway of the influence of these factors could be that mothers with the lowest income could face financial hardship, including in obtaining transport to a health facility, while those with the highest income may struggle less with transport coast. In this study, mothers who follow the Orthodox Christian religion were more likely to utilize PNC at a health facility when compared with women of other religions, excluding Muslim women. Though we could not find any reference to explain this finding, a possible reason could be that there may be differences in health facility access among the Orthodox Christian followers compared to other religious groups (excluding Muslim women). Furthermore, there could be differences in the involvement of religious leaders in advising followers to utilize modern health services. However, this needs further research to explore the differences in PNC utilization among followers of different religions.
Limitations and strengths of the study
This study made use of cross-sectional data from the 2016 Ethiopian Demographic and Health Survey. The data relies on women’s self-reported care utilization, and may be influenced by recall bias, given that the study events took place within the 5 years preceding the survey.
However, the study has a number of strengths. The data is national survey data, and the sample size is powered to be generalizable at national and regional level. This study was unique in that conducted advanced analysis of PNC coverage and location, and factors associated with place of PNC service utilization among mothers who delivered at home. These findings will provide useful information for practitioners and policy makers for increasing utilization of PNC among the substantial population of mothers who give birth at home. It also highlights research areas that need further studies in the future to better understand the barriers and facilitators of place of PNC.
Conclusion
The utilization of postnatal care service among mothers who delivered at home is low in Ethiopia. Living in urban regions, having a bank account, and ever using anything to delay pregnancy were associated with receiving PNC at home. Furthermore being in the upper wealth index, having unwanted pregnancy, receiving 4+ ANC visits and listening to radio weekly were associated with PNC utilization in health facilities among women who delivered at home. Therefore, targeted measures to improve socio-economic status, strengthen the continuum of care and improve health literacy communication are critically important to mitigate the gaps on postnatal care service utilization among women who deliver at home.
Acknowledgements
We would like to thank Central Statistical Agency (CSA) and MEASURE DHS project for providing free access to the data.
Abbreviations
- ANC
Antenatal Care
- AOR
Adjusted Odds Ratio
- EDHS
Ethiopian Demographic Health Survey
- PNC
Postnatal Care
- WHO
World Health Organization
Authors’ contributions
BGA: Carried out the conception and designing the study, performed statistical analysis and wrote the manuscript. MAW and HWG: Conducted the conception and designing the study. MAW, HWG, EGG, HG, TH, AAA, and AAM: critically evaluated and made progressive suggestions throughout the manuscript. All of the authors read and approved the final draft of the manuscript.
Authors’ information
BGA: MPH in General public Health, Tigray Health Research Institute, Tigray, Ethiopia.
MAW: MPH in Nutrition, Tigray Health Research Institute, Tigray, Ethiopia.
HWG: MSc in Maternal and Reproductive Health, Mekelle University, College of Health Sciences, Department of Midwifery.
EGG: MPH in field Epidemiology, Tigray Health Research Institute, Tigray, Ethiopia.
HG: MPH in General public Health, Tigray Health Research Institute, Tigray, Ethiopia.
TH: MPH in General public Health, Tigray Health Research Institute, Tigray, Ethiopia.
AAA: MPH in Nutrition, Tigray Health Research Institute, Tigray, Ethiopia.
AAM: PhD in General Public Health, Mekelle University, College of Health Sciences, School of Public Health.
Funding
‘Not applicable’.
Availability of data and materials
The dataset generated and/or analyzed for the current study is available from MEASURE DHS project but restrictions apply to the availability of the data, which were used under license for the current study, and so are not publicly available. However data is available from the MEASURE DHS project upon reasonable online request.
Ethics approval and consent to participate
Authorization to use the data was obtained from MEASURE DHS by providing a brief description of the study through their website (https://dhsprogram.com/data/). Approval for EDHS data utilization for this study was obtained from the data originator, ICF Macro International U.S.A before the data was extracted from their web platform.
Consent for publication
‘Not applicable for this’.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Brhane Gebrekidan Ayele, Email: brhane3127@gmail.com.
Mulugeta Abrha Woldu, Email: mulugetawoldu425@gmail.com.
Haftom Weldearegay Gebrehiwot, Email: haftom1224@gmail.com.
Equbay Gebru Gebre-egziabher, Email: equblab2003@gmail.com.
Hailay Gebretnsae, Email: hailish14@gmail.com.
Tsegay Hadgu, Email: tsegayhadgu28@gmail.com.
Alemnesh Araya Abrha, Email: alemneshab2017@gmail.com.
Araya Abrha Medhanyie, Email: araya.medhanyie@gmail.com.
References
- 1.McPherson R, Hodgins S. Postnatal home visitation: lessons from country programs operating at scale. Journal of global health. 2018;8(1). [DOI] [PMC free article] [PubMed]
- 2.WHO . WHO recommendations on Postnatal care of the mother and newborn. 2013. [PubMed] [Google Scholar]
- 3.Tunçalp Ӧ, Were WM, MacLennan C, Oladapo OT, Gülmezoglu AM, Bahl R, Daelmans B, Mathai M, Say L, Kristensen F, Temmerman M. Quality of care for pregnant women and newborns—the WHO vision. BJOG: an international journal of obstetrics & gynaecology. 2015;122(8):1045-9. [DOI] [PMC free article] [PubMed]
- 4.Abebe Fantu, Berhane Yemane, Girma Belaineh. Factors associated with home delivery in Bahirdar, Ethiopia: A case control study. BMC Research Notes. 2012;5(1):653. doi: 10.1186/1756-0500-5-653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chungu C, Makasa M, Chola M, Jacobs CN. Place of delivery associated with postnatal care utilization among childbearing women in Zambia. Frontiers in public health. 2018;6:94. [DOI] [PMC free article] [PubMed]
- 6.Fenwick J, et al. Western Australian women’s perceptions of the style and quality of midwifery postnatal care in hospital and at home. Women Birth. 2010. [DOI] [PubMed]
- 7.WHO et al. Informal Meeting on provision of home based care to mother and child in the first week after birth: Follow-up to the Joint WHO/UNICEF Statement on home visits for the newborn child. 2012. [Google Scholar]
- 8.WHO, UNICEF, USAID, Save the Children. WHO-UNICEF Joint Statement on home visits for the newborn child: a strategy to improve survival. 2009. [PubMed]
- 9.Staehelin K, Kurth E, Schindler C, Schmid M, Zemp Stutz E. Predictors of early postpartum mental distress in mothers with midwifery home care: Results from a nested case-control study. Swiss medical weekly. 2013;143:w13862. [DOI] [PubMed]
- 10.Last 10 Kilometers(L10K) Trends in reproductive, maternal, newborn and child health care practices in 115 L10K woredas: Analyses of three rounds of survey data. 2015. [Google Scholar]
- 11.Namazzi Gertrude, Okuga Monica, Tetui Moses, Muhumuza Kananura Rornald, Kakaire Ayub, Namutamba Sarah, Mutebi Aloysius, Namusoke Kiwanuka Suzanne, Ekirapa-Kiracho Elizabeth, Waiswa Peter. Working with community health workers to improve maternal and newborn health outcomes: implementation and scale-up lessons from eastern Uganda. Global Health Action. 2017;10(sup4):1345495. doi: 10.1080/16549716.2017.1345495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chichiabellu TY, Mekonnen B, Astawesegn FH, Demissie BW, Anjulo AA. Essential newborn care practices and associated factors among home delivered mothers in Damot pulasa Woreda, southern Ethiopia. Reproductive health. 2018;15(1):162. [DOI] [PMC free article] [PubMed]
- 13.Duysburgh E, et al. Opportunities to improve postpartum care for mothers and infants: design of context-specific packages of postpartum interventions in rural districts in four sub-Saharan African countries. BMC Pregnancy Childbirth. 2015;15:131. doi: 10.1186/s12884-015-0562-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Central Statistical Agency (CSA) [Ethiopia] and ICF . Ethiopia Demographic and Health Survey 2016. Addis Ababa, and Rockville: CSA and ICF; 2016. [Google Scholar]
- 15.Tessema GA, Laurence CO, Melaku YA, Misganaw A, Woldie SA, Hiruye A, Amare AT, Lakew Y, Zeleke BM, Deribew A. Trends and causes of maternal mortality in Ethiopia during 1990–2013: findings from the Global Burden of Diseases study 2013. BMC public health. 2017;17(1):160. [DOI] [PMC free article] [PubMed]
- 16.Ethiopian Public Health Institute (EPHI) Ethiopia Mini Demographic and Health Survey 2019 Key Indicators. Rockville: ICF; 2019. [Google Scholar]
- 17.Devasenapathy Niveditha, George Mathew Sunil, Ghosh Jerath Suparna, Singh Archna, Negandhi Himanshu, Alagh Gursimran, Shankar Anuraj H, Zodpey Sanjay. Why women choose to give birth at home: a situational analysis from urban slums of Delhi. BMJ Open. 2014;4(5):e004401. doi: 10.1136/bmjopen-2013-004401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sacks E, et al. Postnatal Care Experiences and Barriers to Care Utilization for Home- and Facility-Delivered Newborns in Uganda and Zambia. New York: Springer Science+Business Media; 2016. [DOI] [PubMed] [Google Scholar]
- 19.Greeson Dana, Sacks Emma, Masvawure Tsitsi B, Austin-Evelyn Katherine, Kruk Margaret E, Macwan’gi Mubiana, Grépin Karen A. Local adaptations to a global health initiative: penalties for home births in Zambia. Health Policy and Planning. 2016;31(9):1262–1269. doi: 10.1093/heapol/czw060. [DOI] [PubMed] [Google Scholar]
- 20.Quality E. Dignity a network for improving Quality of Care for Maternal. Malawi: Newborn and Child Health; 2017. [Google Scholar]
- 21.Xiang Yuan-xi, Xiong Ju-yang, Tian Miao-miao, Yuan Fang, Feng Zhan-chun. Factors influencing the utilization of postpartum visits among rural women in China. Journal of Huazhong University of Science and Technology [Medical Sciences] 2014;34(6):869–874. doi: 10.1007/s11596-014-1366-1. [DOI] [PubMed] [Google Scholar]
- 22.Open UNiversity, Postnatal Care Module: 4. Preparation for Postnatal Care. https://www.open.edu/openlearncreate/mod/oucontent/view.php?id=338.
- 23.Mathewos Bereket, Owen Helen, Sitrin Deborah, Cousens Simon, Degefie Tedbabe, Wall Stephen, Bekele Abeba, Lawn Joy E, Daviaud Emmanuelle. Community-Based Interventions for Newborns in Ethiopia (COMBINE): Cost-effectiveness analysis. Health Policy and Planning. 2017;32(suppl_1):i21–i32. doi: 10.1093/heapol/czx054. [DOI] [PubMed] [Google Scholar]
- 24.Kanté AM, Chung CE, Larsen AM, Exavery A, Tani K, Phillips JF. Factors associated with compliance with the recommended frequency of postnatal care services in three rural districts of Tanzania. BMC pregnancy and childbirth. 2015;15(1):341. [DOI] [PMC free article] [PubMed]
- 25.Chen L, Qiong W, Van Velthoven MH, Yanfeng Z, Shuyi Z, Ye L, Wei W, Xiaozhen D, Ting Z. Coverage, quality of and barriers to postnatal care in rural Hebei, China: a mixed method study. BMC pregnancy and childbirth. 2014;14(1):31. [DOI] [PMC free article] [PubMed]
- 26.Takai IU, et al. Factors responsible for under-utilization of postnatal care services in Maiduguri, North-Eastern Nigeria. 2015. [Google Scholar]
- 27.Uppadhaya SK, Bhansali S, Sivodia SK, Agrawal N, Garg K, Singh M. Utilization of Postnatal Care Services in Rural Area of Western Rajasthan, India. Ntl J Community Med. 2016;7(7):569-572.
- 28.Facha Wolde. Couples’ Opinion and Women’s Utilization of Postnatal Care Service in Wolaita Zone, Southern Ethiopia: A Community Based Mixed Study. Science Journal of Public Health. 2017;5(4):288. doi: 10.11648/j.sjph.20170504.12. [DOI] [Google Scholar]
- 29.Khadka R, Hong SA, Thepthien BO. Postnatal care service utilization and its determinants in Ramechhap district, Nepal: A community-based cross-sectional study. Journal of Public Health and Development. 2017;15(3):1-6.
- 30.Abebo TA, Tesfaye DJ. Postnatal care utilization and associated factors among women of reproductive age Group in Halaba Kulito Town, Southern Ethiopia. Arch Public Health. 2018;76(1):9. doi: 10.1186/s13690-018-0256-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Khanal V, Adhikari M, Karkee R, Gavidia T. Factors associated with the utilisation of postnatal care services among the mothers of Nepal: analysis of Nepal demographic and health survey 2011. BMC women's health. 2014;14(1):19. [DOI] [PMC free article] [PubMed]
- 32.Sitrin Deborah, Guenther Tanya, Murray John, Pilgrim Nanlesta, Rubayet Sayed, Ligowe Reuben, Pun Bhim, Malla Honey, Moran Allisyn. Reaching Mothers and Babies with Early Postnatal Home Visits: The Implementation Realities of Achieving High Coverage in Large-Scale Programs. PLoS ONE. 2013;8(7):e68930. doi: 10.1371/journal.pone.0068930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tesfahun Fikirte, Worku Walelegn, Mazengiya Fekadu, Kifle Manay. Knowledge, Perception and Utilization of Postnatal Care of Mothers in Gondar Zuria District, Ethiopia: A Cross-Sectional Study. Maternal and Child Health Journal. 2014;18(10):2341–2351. doi: 10.1007/s10995-014-1474-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Belachew T, Taye A, Belachew T. Postnatal care service utilization and associated factors among mothers in Lemo Woreda, Ethiopia. J Women’s Health Care. 2016;5(10.4172):2167-0420.
- 35.Heyi WD, Deshi MM, Erana MG. Determinants of postnatal care service utilization in diga district, east wollega zone, wester Ethiopia: case-control study. Ethiopian Journal of Reproductive Health. 2018;10(4).
- 36.Jacobs C, Moshabela M, Maswenyeho S, Lambo N, Michelo C. Predictors of antenatal care, skilled Birth attendance, and Postnatal care Utilization among the remote and Poorest rural communities of Zambia: a Multilevel analysis. Frontiers in Public Health. 2017;5:11. [DOI] [PMC free article] [PubMed]
- 37.Dutamo Z, Assefa N, Egata G. Maternal health care use among married women in Hossaina, Ethiopia. BMC Health Serv Res. 2015;15(1):365. doi: 10.1186/s12913-015-1047-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Tesfaye S, Barry D, Gobezayehu AG, Frew AH, Stover KE, Tessema H, Alamineh L, Sibley LM. Improving coverage of postnatal care in rural Ethiopia using a community‐based, collaborative quality improvement approach. Journal of midwifery & women's health. 2014;59(s1):S55-64. [DOI] [PubMed]
- 39.Titaley CR, Hunter CL, Heywood P, Dibley MJ. Why don't some women attend antenatal and postnatal care services?: a qualitative study of community members' perspectives in Garut, Sukabumi and Ciamis districts of West Java Province, Indonesia. BMC pregnancy and childbirth. 2010;10(1):61. [DOI] [PMC free article] [PubMed]
- 40.Bedford Juliet, Gandhi Meena, Admassu Metasebia, Girma Anteneh. ‘A Normal Delivery Takes Place at Home’: A Qualitative Study of the Location of Childbirth in Rural Ethiopia. Maternal and Child Health Journal. 2012;17(2):230–239. doi: 10.1007/s10995-012-0965-3. [DOI] [PubMed] [Google Scholar]
- 41.Regassa N. Antenatal and postnatal care service utilization in southern Ethiopia: a population-based study. African health sciences. 2011;11(3). [PMC free article] [PubMed]
- 42.Mon AS, et al. Utilization of full postnatal care services among rural Myanmar women and its determinants: a cross-sectional study [version 1; referees: 3 approved]. F1000Research. 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Amin Ruhul, Shah Nirali M, Becker Stan. Socioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: A cross-sectional analysis. International Journal for Equity in Health. 2010;9(1):9. doi: 10.1186/1475-9276-9-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Titaley CR, Dibley MJ, Roberts CL. Factors associated with non-utilisation of postnatal care services in Indonesia. Journal of Epidemiology & Community Health. 2009;63(10):827-31. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset generated and/or analyzed for the current study is available from MEASURE DHS project but restrictions apply to the availability of the data, which were used under license for the current study, and so are not publicly available. However data is available from the MEASURE DHS project upon reasonable online request.