

Background:
To use time-driven activity-based costing methodology to compare the costs of routine pediatric plastic surgical patient visits with and without a physician scribe.
Methods:
Pediatric plastic surgical clinic visits at a tertiary care facility with the following diagnoses were studied: skin lacerations, skin lesions, and plagiocephaly. Two plastic surgeons saw patients individually either with or without a scribe over a 10-month period. The time that the scribe and physician spent on the patient was recorded, including the duration of the clinic visit and time spent creating, dictating, reviewing, and signing the note. An average appointment activity time for each measurement component was produced, and a capacity cost rate was introduced to derive the cost per minute for a scribe and physician. Sensitivity analysis and paired t-test were conducted to analyze the results.
Results:
A total of 45 cases with a physician scribe were observed with an average appointment activity time of 12.83 minutes (4.97 min for the scribe, 0.92 min for the physician, and 6.95 min combined). A total of 72 cases without a physician scribe were observed with an average appointment activity time of 12.01 minutes. The total attributable cost saving per appointment was $13.82 when a physician scribe was utilized.
Conclusion:
Time-driven activity-based costing methodology showed that the use of a physician scribe reduced cost per office visit by substituting physician time for a less expensive resource.
INTRODUCTION
As more health care organizations emphasize the significance of value-based health care, time-driven activity-based costing (TDABC) methodology has been acknowledged as one of the most valuable applications to address costing challenges that institutions face.1 TDABC helps to efficiently capture the cost of different processes in care (especially personnel), and its ability to document the amount of time a patient spends with each resource is paramount to measuring the true cost of that resource.1–3 It continues to be the primary methodology to assess operational efficiency and reduction in cost.4 In modern competitive reimbursement environments, providers and facilities are looking for cost-accounting solutions capable of informing process improvement and meeting the expectations of cost control policies. TDABC has been described as a micro-costing approach well suited to accommodate the complexity of cost accounting in health care organizations.1,2 An accurate costing system accounts for the total costs of all the resources used by a patient through a full cycle of care, and the TDABC system allows users to assign costs accurately and relatively easily to each process step. This improved version of activity-based costing requires that providers estimate only 2 parameters at each process step: the cost of each of the resources used in the process and the quantity of time the patient spends with each resource.4
Among those resources, arguably the most valued (and expensive) is physician time. Increased expectations and pressure on physicians to complete time-consuming clerical responsibilities and still increase patient volume have led to conscious efforts to maximize physicians’ workdays.5,6 This is especially true in recent times as the introduction of electronic medical records (EMRs) has increased the time spent in documentation and other indirect patient care activities.6 A 2016 study found that physicians spent about 2 hours doing computer work for every hour spent face to face with a patient.9 In the examination room, physicians devoted half of their patient time facing the screen to do electronic tasks. The University of Wisconsin study found that the average workday for its family physicians had grown to 11 and a half hours.7 This dissociation from patient care has been cited as a possible contributor to epidemic levels of physician burnout.9 Forty percent of physicians screen positive for depression, and 7% report suicidal thinking—almost double the rate of the general working population.13–17
One solution to the electronic health record burden is physician scribe utilization.8–10 Over 2,600 health care facilities in 50 states have employed more than 15,000 scribes, and feedback has shown that physician scribes improve physician satisfaction, charting efficiency, wait times, and productivity levels.9–12 Scribes allow physicians to spend little to minimal time on dictation and note review and also improve patient communication and follow-up.18 A 2015 study of scribes for emergency physicians in an Atlanta hospital system found that the scribes produced a 36% reduction in the doctors’ computer documentation time and a similar increase in time spent directly interacting with patients.8
The purpose of this study was to determine the direct personnel cost effects of incorporating a physician scribe into an outpatient plastic surgery practice for documentation. We hypothesized that the utilization of a physician scribe would decrease costs per office visit for the practice and promote increased capacity. The specific aims were to measure the average appointment activity time (for each study personnel) associated with an outpatient visit with and without the use of a physician scribe and to calculate the cost difference for each scenario using a TDABC model.
MATERIALS AND METHODS
Study Design and Patients
A prospective cohort study of patients from a health care institution in an urban area who were seen for skin lesions, skin lacerations, and plagiocephaly was undertaken from November 2017 to September 2018. These diagnoses were chosen because they are common, relatively simple, and the care processes of these patients are streamlined (rarely need laboratories, radiological studies, or other consultations). The study followed 2 pediatric plastic surgeons (heretofore referred to as “physicians”) at a single institution with and without a physician scribe through clinic visits. This project was exempt from institutional review board approval because data were collected as part of a quality improvement initiative. A paired t-test was conducted to analyze the significance of the means of both appointment activity times.
Selection and Time Process
A day before each clinic, a randomized set of appointments for that day was sent to the physician and the scribe. This appointment schedule indicated which patients were to be timed by the physician alone and which by the physician and the scribe. The randomized assignment was generated solely by a research assistant who knew nothing about the patients other than the presenting diagnosis. The physician and scribe were blinded to the initial selection process. The scribe and physician used their smart phones to measure and record the time spent for each patient visit task. Tasks included preparation time (scribe only), visit length (scribe and physician), transcription time (scribe only), dictation time (physician only), note review, and signing time (physician only) (Table 1).
Table 1.
Tasks for Physicians and Scribes
| Scribe Preparation Time | Visit Length | Scribe Note Transcription | Dictation Time | Physician Note Review and Signing | |
|---|---|---|---|---|---|
| Visit with a scribe | ✔ | ✔ | ✔ | N/A | ✔ |
| Visit with a physician only | N/A | ✔ | N/A | ✔ | ✔ |
The scribe performed documentation before, during, and after the clinic visit. However, it was difficult to separate the time that the scribe spent observing and listening from the time spent documenting during the actual clinic visit. Thus, a separate “transcription time” measure (see above) was delineated to indicate additional time that the scribe needed to complete the visit document after the clinic visit. Note that this time does not reflect the entire time that the scribe spent on the document.
For consistency purposes, only tasks that involved documentation for the visit were included. Other tasks in which the scribe is not involved, such as placing orders, scheduling, other communications, follow-up review of studies or patient phone calls, were not included in this analysis. There was no plastic surgeon preparation time with or without a scribe. The plastic surgery diagnoses chosen for observation were simple and mitigated the need for any such preparation. Average appointment activity times were calculated for visits with and without a scribe, including a breakdown of the average time spent by the physician and scribe for the documentation of each visit.
Cost and Sensitivity Analysis
A TDABC analysis was performed to measure the costs for each activity. The times were aggregated to produce an average appointment activity time for each measurement component, and a capacity cost rate (the total cost of an employee divided into the employee’s work capacity over 1 year, in minutes) was introduced to derive the cost per minute for a scribe and physician. Supporting costs for personnel included salary and fringe benefits.19–22 A range for plastic surgeon salary was derived from multiple sources, which indicated that a plastic surgeon’s salary falls within a range of $353,303 to $547,753.23–26 The midpoint of this range ($450,000) was used for the calculations. However, salary alone does not account for total cost, and associated costs such as health insurance and other fringe benefits need also be considered. According to the Bureau of Labor Statistics US Department of Labor, fringe benefits for employee compensation were estimated to be 30% of salary and wages,19,27 which totaled $135,000 (30% of 450,000). This produces a total annual cost of $585,000. Plastic surgeon capacity assumed 9.98 hours/d (2,524 mean annual hours for family practice − 29 hours for plastic surgery = 2,495 mean annual hours for plastic surgery; 2,495 hours/y/50 wks/y = 49.9 hours/wk = 9.98 hours/d).28 Given our assumption of 9.98 work hours/d, the calculated cost capacity rate expressed as dollars per minute for a pediatric plastic surgeon was $4.28 per minute (Table 2). The cost capacity rate of a physician scribe was measured by the rate that the practice pays directly for that resource. In most cases, the scribe is hired through an agency (as was in this case) so the practice pays a per-hour rate as a direct cost. Based on multiple sources, this hourly rate is estimated to be $20.00 or $0.33 per minute (Table 2).30,31 Activity costs were attained by multiplying the observed average total times for each activity by the cost rate for each staff member involved in the activity. These costs were totaled to derive the total cost of an appointment for each type of visit. Average times and costs were reported. All costs were calculated from a provider’s perspective.
Table 2.
Estimated Cost Capacity Rate of Plastic Surgeon and Physician Scribe Based on National Averages2,3-27, 30,31
| Physician Scribe | Plastic Surgeon | |
|---|---|---|
| Mean salary, $ | – | $450,000 |
| Fringe benefits, $ | – | $135,000 |
| Total cost, $ | $20.00/h | $585,000/y |
| Cost rate per minute, $/min | $0.33 | $4.28 |
RESULTS
A total of 117 cases with the aforementioned diagnoses were measured, recorded, and analyzed. As shown in Table 6, there were 45 observations utilizing a physician scribe and 72 observations without a scribe.
Table 6.
Sensitivity Analysis of Variable Cost Capacity Rates and Savings per Appointment
| Pediatric Plastic Surgeon | ||||||
|---|---|---|---|---|---|---|
| Physician scribe | Cost Rate | $3.33/min | $3.81/min | $4.28/min | $4.76/min | $5.24/min |
| $0.33/min | $9.88 | $11.88 | $13.82 | $15.82 | $17.81 | |
| $0.38/min | $9.29 | $11.28 | $13.23 | $15.22 | $17.21 | |
| $0.42/min | $8.81 | $10.80 | $12.75 | $14.75 | $16.74 | |
Time Analysis
The average appointment activity time was 12.83 ± 6.71 (±SD) minutes with a physician scribe and 12.01 ± 5.01 (±SD) minutes without a scribe. In the physician scribe group, scribe preparation time was an average of 2.42 ± 1.12 (±SD) minutes, visit length was 6.95 ± 5.01 (±SD) minutes, note review for the scribe was an average of 2.55 ± 2.32 (±SD) minutes, and physician note review was an average of 0.92 ± 0.69 (±SD) minutes (Fig. 1). In the physician-only group, visit length was 8.53 ± 3.72 (±SD) minutes, dictation was an average of 2.79 ± 1.24 (±SD) minutes, and physician note review was an average of 0.69 ± 0.40 (±SD) minutes. The average appointment activity times for each cohort and the average times for each activity, for both cohorts and by visit type (ie, new or return), are shown in Table 3.
Fig 1.
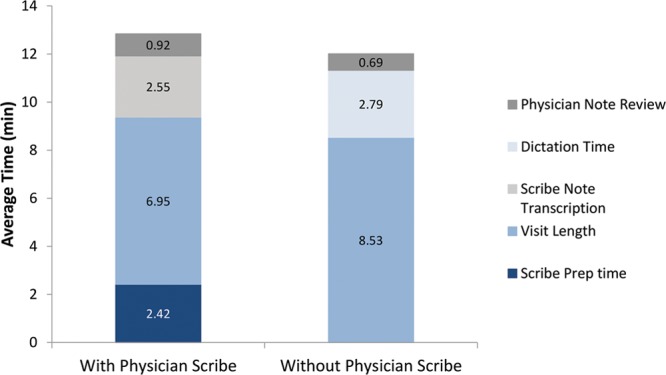
Total average appointment activity time.
Table 3.
Average Observed Times for Each Activity in Each Cohort
| With Scribe | Skin Laceration | Skin Lesion | Plagiocephaly* | Total Average Appointment Activity Time | |||
|---|---|---|---|---|---|---|---|
| New | Return | New | Return | New | Return | ||
| No. observations | 5 | 4 | 21 | 8 | 4 | 3 | – |
| Scribe preparation time | 2.68 | 2.60 | 2.77 | 3.40 | 1.25 | 1.83 | 2.42 |
| Visit length | 6.12 | 7.53 | 9.39 | 4.70 | 5.96 | 7.99 | 6.95 |
| Scribe note transcription | 2.18 | 4.11 | 4.38 | 2.31 | 1.23 | 1.07 | 2.55 |
| Physician note review | 1.01 | 0.62 | 1.53 | 0.50 | – | – | 0.92 |
| Total average time | 11.99 | 14.86 | 18.07 | 10.91 | 8.44 | 10.89 | 12.83 |
| Without Scribe | Skin Laceration | Skin Lesion | Plagiocephaly* | Total Average Appointment Activity Time | |||
| New | Return | New | Return | New | Return | ||
| No. observations | 4 | 7 | 24 | 16 | 16 | 5 | – |
| Visit length | 9.10 | 7.54 | 10.82 | 6.1 | 8.98 | 8.66 | 8.53 |
| Dictation time | 2.83 | 2.26 | 3.45 | 1.51 | 3.22 | 3.48 | 2.79 |
| Physician note review | 1.1 | 0.47 | 0.83 | 0.35 | – | – | 0.69 |
| Total average time | 13.03 | 10.27 | 15.1 | 7.96 | 12.20 | 12.14 | 12.01 |
Statistical Analysis
A paired t-test was conducted to analyze the significance of the difference in appointment times. This test was utilized because the study compared the means of 2 groups after a variable (physician scribe) was introduced. The paired t-test produced a P-value of 0.776, illustrating that there was no significant difference in appointment times between the 2 groups (with and without physician scribe).
Cost and Sensitivity Analysis
Since the cost capacity rates depend on the range of salaries for a plastic surgeon and physician scribe, a sensitivity analysis was used to assess the range of potential cost-saving outcomes (Tables 4 and 5).25,26,30,31 Higher hourly rates selected for a physician scribe in the sensitivity analysis led to a conservative measurement of cost savings. If a facility is able to obtain a physician scribe for less than $20 per hour, then there would be even more savings. Table 6 illustrates a minimum cost savings of $8.81 per appointment and a maximum of $17.81 per appointment.
Table 4.
Potential Range of Physician Costs
| Pediatric Plastic Surgeon | |||||
|---|---|---|---|---|---|
| Base salary | $350,000 | $400,000 | $450,000 | $500,000 | $550,000 |
| Fringe benefits | $105,000 | $120,000 | $135,000 | $150,000 | $165,000 |
| total compensation | $455,000 | $520,000 | $585,000 | $650,000 | $715,000 |
| cost per minute | $3.33/min | $3.81/min | $4.28/min | $4.76/min | $5.24/min |
Table 5.
Potential Range of Scribe Costs
| Physician Scribe Capacity Cost Rate | |||
|---|---|---|---|
| Hourly rate | $20/h | $22.5/h | $25/h |
| Cost per minute | $.33/min | $.38/min | $.42/min |
According to the data in Table 6 (in bold), choosing a median level of plastic surgeon salary and a commonly quoted cost rate for a physician scribe leads to an estimated $13.82 savings per appointment when a physician scribe was utilized. When projecting these savings across all department-wide cases related to skin lesions, skin laceration, and plagiocephaly, total costs would be reduced to upwards of $138,200 in a fiscal year.
CONCLUSIONS
The purpose of this study was to determine the direct personnel cost of incorporating a physician scribe into an outpatient pediatric plastic surgery practice for documentation. We hypothesized that the utilization of a physician scribe would decrease costs per office visit.
In our cohort, analysis illustrated a range of cost-saving outcomes, dependent on a variable cost capacity rate. The cost savings per appointment was $13.82 when a physician scribe was used, with a 0.82-minute extension in total appointment activity time. The cost savings stem from shifting dictating responsibilities onto the scribe and reducing the time a physician spent on dictation and the note review process. The duration of the actual visit was observed to be shorter when a scribe was present, by an average of 1.58 minutes. Although this finding can be attributable to bias (patients were randomized but physician and scribe could not be blinded), a more likely explanation is that the presence of a scribe actually facilitated the clinic visit. The scribe allows the physician to minimize taking notes and interacting with the EMR.18,32–35 This, in turn, translates to more time interacting directly with the patient without interruption.32–35 Our initial hypothesis was that clinic times would be influenced with the scribe present, and hence we chose to measure this time as well as direct documentation time.
The scribe involved with this study had a minimum experience of 3 months working with each physician before undertaking this study. It is possible that a more experienced scribe could translate to even shorter observed times across the board. Nevertheless, it is clear from our analysis that at worst, the scribe does not slow down the clinic visit; and at best, the presence of a scribe improves visit times.
Utilizing a physician scribe allows the physician to use time (that otherwise would have been spent dictating) more efficiently. The cost savings, when extrapolated across all department-wide cases related to skin lesions, skin lacerations, and plagiocephaly, would reduce total costs upwards of $138,200 in a fiscal year. It is likely that these savings can be easily generalized to other common diagnoses and would thus offer even greater cost savings. Our sensitivity analysis indicated that savings can be realized even with conservative estimates of physician and scribe costs. Nevertheless, this costing calculation potentially underestimates the true savings afforded by a scribe, as the reduction in time enhances the availability of the physician to see other patients or tend to other duties that further increase efficiency and revenue for the facility.
Utilizing physician scribes also benefits physician morale. The increased pressures and expectations of physicians to complete administrative and clerical tasks have resulted in physicians being pulled further away from actual patient care, leading to physician burnout and fatigue.14–17,36 Burnout and fatigue is only being accelerated by the adoption and implementation of legacy EMRs that are poorly designed from a user standpoint, and which are fundamentally designed for patient billing and not for efficient patient management.37,38,40 The impact is evident in a recent report in which the fourth cause of burnout after bureaucratic tasks (eg, charting, paperwork), hours and lack of respect from administrators/employers, was “computerization of practice (EMR).”39 By introducing scribes, 3 of the top 4 causes can be directly alleviated and the negative impact of burnout that results in higher medical error rates, lower patient satisfaction and higher physician turnover can potentially be prevented. Lastly, there is a societal and educational benefit of teaching a scribe, many of whom are medical school candidates who use this experience to enrich their medical knowledge and clinical communication in an early stage of their career. Not all of these aforementioned benefits can be captured in simple dollar terms and thus bear consideration in the overall calculus of introducing scribes in the clinical realm.
Our practice is managed within an academic medical center, and cost savings seen herein may not be directly generalizable to private or adult plastic surgical practices. Nevertheless, the authors believe that any busy plastic surgical practice that sees specific diagnoses frequently is likely to gain value from a physician scribe. Seeing specific diagnoses consistently allows the scribe to be trained and develop an efficient workflow to minimize overall activity time. This intervention improves cost savings and value, especially if the practice is capacity constrained (meaning there is adequate demand but less capacity to service that demand). In cases where the practice is demand constrained (meaning there is ample capacity to service demand), additional physician availability time afforded by the scribe will not directly translate to seeing more patients. In these types of practices, a physician scribe is less likely to be of direct, measurable financial value.
There are some limitations to this study. Although the subjects were randomized, the physician and scribe could not be blinded completely and this may have introduced some bias. Furthermore, the numbers of observations in each diagnosis group (eg, skin lesions, skin lacerations, and plagiocephaly) were not uniform because of time limitations, patient cancellations, seasonal variation, or other practice-related issues. Finally, there may be minor measurement errors in the data collection due to the self-reporting nature of the observations for each of the activities.
In conclusion, this study shows that the use of physician scribes in outpatient plastic surgery visits decreases costs and improves efficiency. The analysis of practice efficiency is important to comprehensively appraise the quality and effectiveness of care, both for the patient and for the provider.41 Gathering such outcomes from employing a physician scribe that can be integrated within the clinical workflow provides both practicality and accessibility. Healthcare needs systems that make the right care simpler for both patients and professionals, not more complicated. In addition, they must do so in ways that strengthen human connections, instead of weakening them.9 Through TDABC methodology, we were able to contextualize the direct financial value of a physician scribe. To this extent, TDABC better positions health care organizations to identify and control cost information in the effort to create true value in health care. We hope that the experiences described herein may assist other teams that wish to implement physician scribes at their own institutions.
Footnotes
Published online 16 October 2019.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Kaplan RS, Anderson SR. Time-driven activity-based costing. Harv Bus Rev. 2004;82:131–138, 150. [PubMed] [Google Scholar]
- 2.Kaplan RS, Porter ME. How to solve the cost crisis in health care. Harv Bus Rev. 2011;89:46–52, 54, 5661. [PubMed] [Google Scholar]
- 3.McLaughlin N, Burke MA, Setlur NP, et al. Time-driven activity-based costing: a driver for provider engagement in costing activities and redesign initiatives. Neurosurg Focus. 2014;37:E3. [DOI] [PubMed] [Google Scholar]
- 4.Keel G, Savage C, Rafiq M, et al. Time-driven activity-based costing in health care: a systematic review of the literature. Health Policy. 2017;121:755–763. [DOI] [PubMed] [Google Scholar]
- 5.Bank AJ, Gage RM. Annual impact of scribes on physician productivity and revenue in a cardiology clinic. Clinicoecon Outcomes Res. 2015;7:489–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bank AJ, Obetz C, Konrardy A, et al. Impact of scribes on patient interaction, productivity, and revenue in a cardiology clinic: a prospective study. Clinicoecon Outcomes Res. 2013;5:399–406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gilchrist V, McCord G, Schrop SL, et al. Physician activities during time out of the examination room. Ann Fam Med. 2005;3:494–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hemant BK, Mishra A. Electronic medical records and physician productivity: evidence from panel data analysis. https://ssrn.com/abstract=1952287.
- 9.Gawande A. Why doctors hate their computers. The New Yorker. https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers.
- 10.Hess JJ, Wallenstein J, Ackerman JD, et al. Scribe impacts on provider experience, operations, and teaching in an academic emergency medicine practice. West J Emerg Med. 2015;16:602–610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Scribe America. Medical scribes. https://www.scribeamerica.com/why-scribe-america/. Accessed November 16, 2018.
- 12.Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172:1377–1385. [DOI] [PubMed] [Google Scholar]
- 13.Gellert GA, Ramirez R, Webster SL. The rise of the medical scribe industry: implications for the advancement of electronic health records. JAMA. 2015;313:1315–1316. [DOI] [PubMed] [Google Scholar]
- 14.Shanafelt TD, Balch CM, Bechamps GJ, et al. Burnout and career satisfaction among American surgeons. Ann Surg. 2009;250:463–471. [DOI] [PubMed] [Google Scholar]
- 15.Lee RT, Ashforth BE. A meta-analytic examination of the correlates of the three dimensions of job burnout. J Appl Psychol. 1996;81:123–133. [DOI] [PubMed] [Google Scholar]
- 16.Leiter MP, Durup J. The discriminant validity of burnout and depression: a confirmatory factor analytic study. Anxiety Stress Copin. 7:357–373. [Google Scholar]
- 17.Dyrbye LN, Shanafelt TD. Physician burnout: a potential threat to successful health care reform. JAMA. 2011;305:2009–2010. [DOI] [PubMed] [Google Scholar]
- 18.Shultz CG, Holmstrom HL. The use of medical scribes in health care settings: a systematic review and future directions. J Am Board Fam Med. 2015;28:371–381. [DOI] [PubMed] [Google Scholar]
- 19.Resnick CM, Daniels KM, Flath-Sporn SJ, et al. Physician assistants improve efficiency and decrease costs in outpatient oral and maxillofacial surgery. J Oral Maxillofac Surg. 2016;74:2128–2135. [DOI] [PubMed] [Google Scholar]
- 20.Inverso G, Lappi MD, Flath-Sporn SJ, et al. Increasing value in plagiocephaly care: a time-driven activity-based costing pilot study. Ann Plast Surg. 2015;74:672–676. [DOI] [PubMed] [Google Scholar]
- 21.Husted H, Kristensen BB, Andreasen SE, et al. Time-driven activity-based cost of outpatient total hip and knee arthroplasty in different set-ups. Acta Orthop. 2018;89:515–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McCreary DL, White M, Vang S, et al. Time-driven activity-based costing in fracture care: is this a more accurate way to prepare for alternative payment models? J Orthop Trauma. 2018;32:344–348. [DOI] [PubMed] [Google Scholar]
- 23.Levin LS. The business of academic plastic surgery. Plast Reconstr Surg. 2010;126:303–307. [DOI] [PubMed] [Google Scholar]
- 24.Salary.com. Salary range for Surgeon – pediatric in the United States. https://www1.salary.com/Surgeon-Pediatric-salary.html. Accessed March 25, 2019.
- 25.Merritt Hawkins. 2018 Compilation of physician compensation surveys. https://www.merritthawkins.com/uploadedFiles/merritthawkins_2018_compensation_brochure.pdf. Accessed March 25, 2019.
- 26.American Medical Group Association. 2015 Medical group compensation and productivity survey. http://physiciancompensation.org/PDFs/2015RSPWB/2015Survey.pdf. Accessed March 25, 2019.
- 27.Bureau of Labor Statistics, US Department of Labor. Employer costs for employee compensation – December 2018. https://www.bls.gov/news.release/pdf/ecec.pdf. Accessed March 26, 2019.
- 28.Leigh JP, Tancredi D, Jerant A, et al. Annual work hours across physician specialties. Arch Intern Med. 2011;171:1211–1213. [DOI] [PubMed] [Google Scholar]
- 29.Scribe America. Medical scribe frequently asked questions. https://www.scribeamerica.com/faq/. Accessed March 27, 2019.
- 30.Hospital Careers. Medical scribe. https://www.hospitalcareers.com/career-profiles/medical-scribe/#salary. Accessed March 27, 2019.
- 31.Becker’s Hospital Review. Are medical scribes worth the investment? https://www.beckershospitalreview.com/patient-flow/are-medical-scribes-worth-the-investment.html. Accessed March 27, 2019.
- 32.Fleming NS, Becker ER, Culler SD, et al. The impact of electronic health records on workflow and financial measures in primary care practices. Health Serv Res. 2014;49:405–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.King J, Patel V, Jamoom EW, et al. Clinical benefits of electronic health record use: national findings. Health Serv Res. 2014;49:392–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Menachemi N, Collum TH. Benefits and drawbacks of electronic health record systems. Risk Manag Healthc Policy. 2011;4:47–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Montague E, Asan O. Dynamic modeling of patient and physician eye gaze to understand the effects of electronic health records on doctor-patient communication and attention. Int J Med Inform. 2014;83:225–234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dewa CS, Loong D, Bonato S, et al. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv Res. 2014;14:325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pozdnyakova A, Laiteerapong N, Volerman A, et al. Impact of medical scribes on physician and patient satisfaction in primary care. J Gen Intern Med. 2018;33:1109–1115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Campanella P, Lovato E, Marone C, et al. The impact of electronic health records on healthcare quality: a systematic review and meta-analysis. Eur J Public Health. 2016;26:60–64. [DOI] [PubMed] [Google Scholar]
- 39.The National Institute of Mental Health. Major depression among adults. https://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adults.shtml. Accessed November 16, 2017.
- 40.Friedberg MW, Chen PG, Van Busum KR, et al. Factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Rand Health Q. 2014;3:1. [PMC free article] [PubMed] [Google Scholar]
- 41.Woodcock DV, Pranaat R, McGrath K, et al. The evolving role of medical scribe: variation and implications for organizational effectiveness and safety. Stud Health Technol Inform. 2017;234:382–388. [PubMed] [Google Scholar]