

Abstract
Rosai–Dorfman disease also known as sinus histiocytosis with massive lymphadenopathy is a rare benign disorder of unknown etiology. It is a benign condition which causes significant cervical lymphadenopathy in children and young adults. These cases are frequently misdiagnosed as lymphoma, and thus it is important to distinguish Rosai–Dorfman disease from other causes of neck swelling because of different treatment modalities. We report here a case of Rosai–Dorfman disease presenting with massive right cervical lymphadenopathy.
Keywords: Massive lymphadenopathy, Rosai–Dorfman disease, Sinus histiocytosis
Rosai–Dorfman disease also known as Sinus Histiocytosis with Massive Lymphadenopathy (SHML) is an uncommon benign systemic histio-proliferative disease which affects lymph nodes. Although cervical region is by far the most common and most prominent site of involvement but peripheral or central lymph nodes are also affected. In about 25–40% of cases, extra nodal sites are also affected [1–3]. Majority of patients are children or young adults [4]. Males are more commonly affected [5]. Etiology is not exactly known however like any other histiocytic disorder responds well to systemic steroids. Though it is considered as a benign disorder, can sometimes behave in an aggressive manner leading to significant morbidity and mortality [1]. We report a case of Rosai–Dorfman disease in a young male patient.
Case Report
A fifteen year old boy was presented to our hospital with chief complaints of painless progressive swelling in the right side of neck in last 6 months. Patient was having no history of fever, pain in throat, difficulty in deglutition, difficulty in respiration, chronic cough, loss of appetite or loss of weight. On examination there was non-tender, non-fluctuant soft to firm swelling involving anterior and posterior triangle of neck about 10 × 6.5 cm in dimension on right side. It was mobile and not adherent to underlying skin (Figs. 1, 2). There was also swelling involving bilateral supraclavicular region. There was no any swelling in axillary or inguinal region. On nasal endoscopy no abnormality was detected. Routine haematological examination showed Haemoglobin 12.2 g%, Total leukocyte count 6.3 × 109/litre, Erythrocyte sedimentation rate 15 mm 1st hour while differential leukocyte count was with in normal limits. Mantoux test was negative. High resolution Ultrasonography suggested multiple discrete, homogenous lymph node in right carotid space. There was no cystic necrotization, calcification or loss of fibrofatty plane are seen (Fig. 3). Contrast enhanced computed tomogram neck with thorax suggested a large lobulated soft tissue lesion about 10 × 6.5 × 5.5 cm in dimension (Fig. 4). No intratumoral necrosis was seen. Patchy heterogeneous enhancement was seen in post contrast images. Mass was mildly compressing trachea and right thyroid gland to the left (Figs. 5, 6). Bilateral supraclavicular lymph node was seen along with non-necrotic lymph node in superior mediastinum. Fine needle aspiration cytology from cervical lymph node was highly suggestive of Rosai–Dorfman disease, however biopsy was advised for confirmation. Biopsy was done under local anaesthesia from the posterior triangle of neck just behind the mid part of sternocleidomastoid muscle. Histopathology showed diffuse effacement of lymph node architecture and dilated sinuses distended with benign histiocytes (Figs. 7, 8); the diagnosis was given as sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease). This patient was put on oral prednisolone 10 mg three times a day in tapering doses for 21 days initially and then on low dose of steroids for next 4 months. The patient showed marked clinical improvement.
Fig. 1.

Patient with right sided lymphadenopathy
Fig. 2.

Patient with right sided lymphadenopathy
Fig. 3.
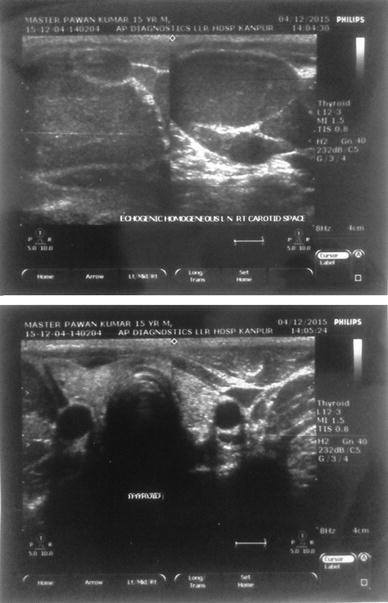
High resolution ultrasonography of neck
Fig. 4.
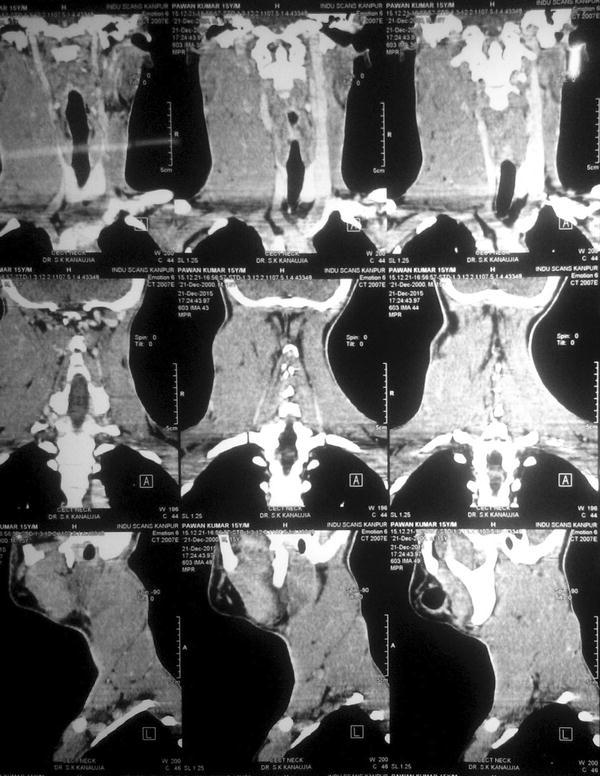
CT scan coronal view
Fig. 5.
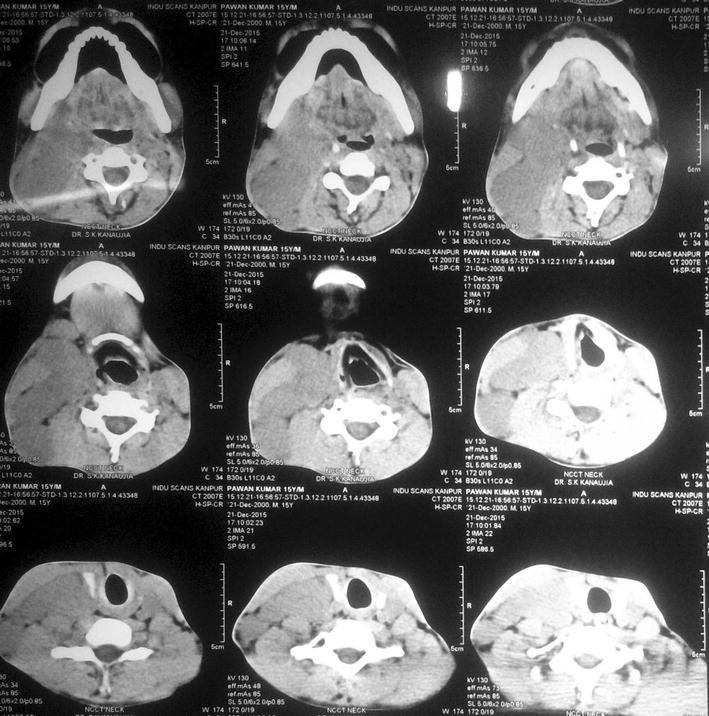
CT scan axial view 1
Fig. 6.
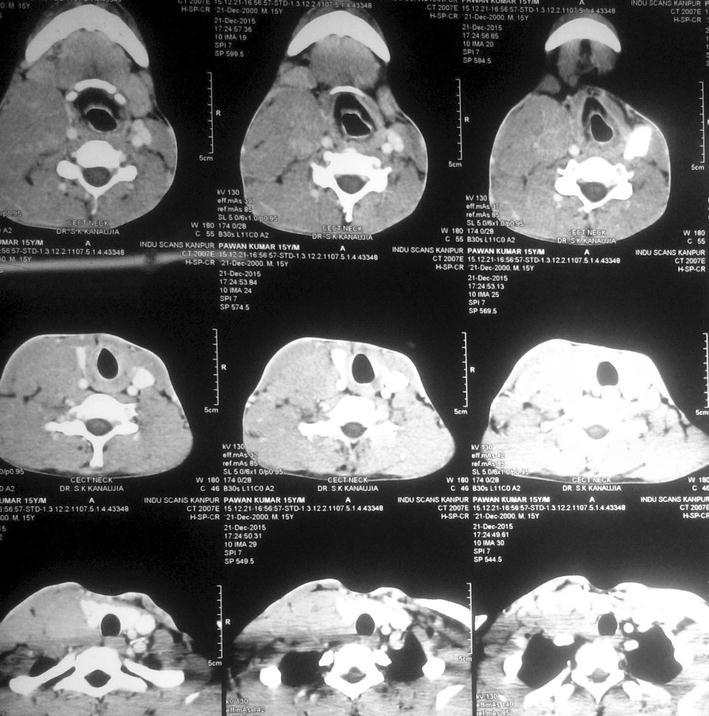
CT scan axial view 2
Fig. 7.
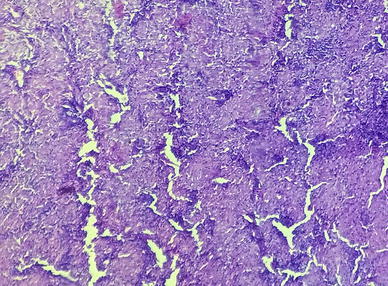
Low magnification histopathology showing dilated sinuses distended with benign histiocytes
Fig. 8.

High magnification histopathology showing dense lymphocytic infiltrate
Discussion
Rosai–Dorfman disease is a distinct benign histiocytic disorder, first described by Rosai and Dorfman in 1969. The disease also known as sinus histiocytosis with massive lymphadenopathy (SHML), is benign, self-limiting disorder that commonly involves the lymph nodes. The disease is worldwide in distribution and males are commonly affected with male to female ratio of approximately 2:1. Cervical lymph nodes are most commonly affected [6]; however, other lymphnodal groups, like axillary, inguinal and mediastinal may also be involved. Extranodal involvement is seen in 25–40% cases. Various extranodal sites have been reported including the upper respiratory tract, gastrointestinal tract, paranasal sinuses, orbit and even meninges. It can affect any age group but most commonly seen in second decade of life. The Etiology of the disease is still controversial but it is presumed to be due to an immune regulation disorder, as well as infections caused by agents like Herpes viruses, Epstein–barr virus, Cytomegalovirus, Brucella and Klebsiella [6, 7]. The disease is thought to be a disorder of immune regulation or response to a presumed infectious agents (HHV-6/EBV) with its major manifestation in lymph nodes with resultant proliferation of sinusoidal histiocytes. This theory is supported by the study done by Middel et al. [8], where they concluded that stimulation of monocytes/macrophages via macrophage colony stimulating factor (M-CSF) leading to immune suppressive macrophages represents a main mechanism for the pathogenesis of sinus histiocytosis with massive lymphadenopathy. The onset of sinus histiocytosis with massive lymphadenopathy is typically insidious; the active phase is prolonged, there may be spontaneous remissions and relapses. Deaths have been reported in very few cases [5, 9]. Diagnosis of Rosai–Dorfman disease is based on clinical suspicion and histopathological confirmation. Histologically, there is infiltration of the tissue by lymphocytes, histiocytes and plasma cells. Presence of emperipolesis, i.e. engulfment of lymphocytes and erythrocytes by histiocytes, is usually diagnostic of Rosai–Dorfman disease.
Immunohistochemistry is usually necessary for confirmation of diagnosis. Characteristically, S-100 is always positive. Also, some other markers, like CD68, CD163, alpha1 antichymotrypsin and alpha1 antitrypsin, may also be positive [4]. The differential diagnosis of lymphomas was considered because some of the diffuse large B cell lymphomas showed extensive emperipolesis [10] which is considered to be a characteristic histological picture of Rosai–Dorfman disease, but the difference is immunohistochemically numerous CD68-positive and S-100-negative histiocytes are present in diffuse large B-cell lymphomas [10]. The common differential diagnosis includes infectious lesions, granulomatous lesion, reactive lymphoid hyperplasia with sinus histiocytes (RLHSH), Langerhans cell histiocytosis (LCH), hemophagocytic syndrome and malignant lymphoma. The treatment in Rosai–Dorfman disease is nonspecific and depends on the site of involvement. Isolated lymphadenopathy may not be treated at all except for cosmetic reasons. However, if any vital organs are involved or if the lesion is causing some obstructive symptoms or pressure symptoms, aggressive treatment may be indicated. The medical treatment includes corticosteroids, chemotherapy, low dose interferon, antibiotics and radiation therapy. Radiation therapy is indicated for threatened function, such as cord compression and respiratory embarrassment [11, 12]. Response to treatment is highly variable with repeated remission and exacerbation episodes. Surgical treatment may be in the form of partial or total resections. In current patient diagnostic biopsy was performed. The tracheal shift because of mass effect had improved as mass reduced significantly. The patient had been followed for 8 months and patient responded very well to systemic steroids.
Conclusion
Rosai–Dorfman disease should be kept as a differential diagnosis in young patients presenting with massive cervical lymphadenopathy. Being a rare entity, high degree of clinical suspicion with typical histopathological features and immunohistochemistry are diagnostic. However, it is necessary that both clinicians and pathologist keep this entity in their list of differential diagnosis for massive lymphadenopathy.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no competing interests.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participant included in the study.
Contributor Information
Ashutosh Singh, Email: ashuenrapt@gmail.com.
Surendra Kumar Kanaujiya, Email: skkanaujia1@gmail.com.
References
- 1.Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease): review of entity. Semin Diagn Pathol. 1990;7(1):19–73. [PubMed] [Google Scholar]
- 2.Sanchez R, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: analysis of 113 cases with special emphasis on its extranodal manifestation. Lab Invest. 1977;36:21–22. [Google Scholar]
- 3.Goodnight JW, Wang MB, Sercarz JA, Fu YS. Extranodal Rosai–Dorfman disease of the head and neck. Laryngoscope. 1996;106(3 pt 1):253–256. doi: 10.1097/00005537-199603000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Juskevicius R, Finlay JL. Rosai–Dorfman disease of the parotid gland, cytologic and histopathologic findings with immunohistochemical correlation. Arch Pathol Lab Med. 2001;125:1348–1350. doi: 10.5858/2001-125-1348-RDDOTP. [DOI] [PubMed] [Google Scholar]
- 5.Lauwers GY, Perez-Atayde A, Dorfman RF, et al. The digestive system manifestations of Rosai–Dorfman disease (sinus histiocytosis with massive lymphadenopathy): review of 11 cases. Hum Pathol. 2000;31(3):380–385. doi: 10.1016/S0046-8177(00)80254-3. [DOI] [PubMed] [Google Scholar]
- 6.Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: an analysis of 14 deaths occurring in a patient registry. Cancer. 1984;54(9):1834–1840. doi: 10.1002/1097-0142(19841101)54:9<1834::AID-CNCR2820540911>3.0.CO;2-F. [DOI] [PubMed] [Google Scholar]
- 7.Fudenberg HH, Good RA, Hitzig W, et al. Classification of the primary immune deficiencies: WHO recommendation. N Engl J Med. 1970;283:656–657. doi: 10.1056/NEJM197009172831211. [DOI] [PubMed] [Google Scholar]
- 8.Middel P, Hemmerlein B, Fayyazi A, Kaboth U, Radzun HJ. Sinus histiocytosis with massive lymphadenopathy: evidence for its relationship to macrophages and for a cytokine-related disorder. Histopathology. 1999;35(6):525–533. doi: 10.1046/j.1365-2559.1999.00746.x. [DOI] [PubMed] [Google Scholar]
- 9.Pulsoni A, Anghel G, Falcucci P, Matera R, Pescarmona E, Ribersani M, Villia N, Mandelli F. Treatment of sinus histiocytosis with massive lymphadenopathy: report of case and literature review. Am J Hematol. 2002;69:67–71. doi: 10.1002/ajh.10008. [DOI] [PubMed] [Google Scholar]
- 10.Lopes LF, Bacchi MM, Coelho KI, Filho AA, Bacchi CE. Emperipolesis in a case of B-cell lymphoma: a rare phenomenon outside of Rosai–Dorfman disease. Ann Diagn Pathol. 2003;7(5):310–313. doi: 10.1016/j.anndiagpath.2003.06.002. [DOI] [PubMed] [Google Scholar]
- 11.Raveenathiran V, Dhanalakshmi M, Rao PH, Viswanathan P. Rosai–Dorfman disease: report of a 3 year old girl with critical review of treatment options. Eur J Pediatr Surg. 2003;13(5):350–354. doi: 10.1055/s-2003-43578. [DOI] [PubMed] [Google Scholar]
- 12.Jabali Y, Smrcka V, Pradna J. Rosai–Dorfman disease: successful long-term results by combination chemotherapy with prednisolone, 6-mercaptopurine, methotrexate and vinblastine: a case report. Int J Surg Pathol. 2005;13(3):285–289. doi: 10.1177/106689690501300311. [DOI] [PubMed] [Google Scholar]