

Abstract
Benign vocal lesions are non-malignant growths of abnormal tissue on the vocal cords. The common benign lesions of vocal cord are singer’s nodule, polyps, papilloma, polypoidal degeneration and cysts. The aim of this study was to analyze the demographics such as age, sex, occupation, symptomatology, site of involvement. An objective evaluation of voice handicap was done pre and postoperatively using VHI-10 scale to see improvement in patient’s symptoms. In this prospective study, a total of 50 cases were selected with benign lesions in regional hospital of India. The pre and post operative assessment for voice handicap was assessed by VHI-10. Chi square test (SPSS 20.0 version) used to analyze result; value of p < 0.05 was taken significant. In this study of 50 patients, the benign lesions were most common in 20–29 age group. Male (70%) outnumbered females (30%). Most common was Vocal polyp (56%), followed by nodule (32%), cyst (10%) and papilloma (2%) respectively. All patients showed improvement after phonosurgery and postoperative speech therapy, being assessed by VHI-10 scale. The benign lesions of vocal cords produces symptoms which can vary from hoarseness to stridor, affect social functioning, work performance. Speech therapy following microlaryngeal surgery forms an essential part of treatment, to avoid recurrence. VHI-10 scale as found to be a useful and convenient tool in measuring patient voice handicap and to see improvement after surgery.
Keywords: Benign lesions, Vocal cords, Microlaryngeal surgery, Speech therapy, VHI-10
Introduction
Benign vocal lesions are non-malignant growths of abnormal tissue on the vocal cords. The common benign lesions of vocal cord are singer’s nodule, polyps, papilloma, polypoidal degeneration (Reinke’s edema) and cysts. Others are sulcus vocalis, mucosal bridge, intracordal cysts, vocal cord varices and anterior webs. Several factors can be responsible for the development of the benign vocal lesions such as vocal abuse, overuse or misuse of voice, chronic infections of upper airway, allergy, smoking and gastroesophageal reflux. Frequent coughing and throat-clearing also contribute to the mucosal irritation which worsens the voice [1–3].
Excessive mechanical trauma and stress in the mid-membranous area of vocal cord leads on to wound formation occurs. Subsequently remodelling of the superficial layer of the lamina propria and, to a lesser extent, epithelium results in the formation of vocal cord nodules, polyps, and cysts. Several studies have demonstrated that the pathologic changes in vocal cord polyps, nodules, and cysts occur within the superficial layer of the lamina propria [1, 4].
Voice disorders cause communication handicap which leads on to psychosocial problems and impaired quality of life [5, 6]. To assess voice handicap several scales have been developed e.g. Voice Handicap Index (VHI), Voice Related Quality Of Life (V-RQOL), Voice Activity and Participation Profile (VAPP), and The Voice Outcome Survey (VOS). The patient-based, voice-specific outcome measures can potentially provide more information than the biological and physiological variables that are associated with voice production, functional abilities and quality of life. VHI-10 is a powerful representation of the VHI that takes less time for the patient to complete, without loss of validity, the measurement properties of VHI-10 have been validated in other languages as well, which has rendered the tool essential to better understanding the impact of dysphonia in several life areas [7, 8].
The significance of benign lesions of the larynx lies in the importance of its function in speech and the contribution of the voice to one’s identity. Since these lesions are not malignant, they are usually not life threatening. A clinical diagnosis of nodules, polyps or cysts does not rule out a malignancy unless the lesion resolves with treatment or is benign on histopathological examination [1, 2].
Materials and Methods
This prospective, non-randomized, hospital based study was conducted in the Department of of Otolaryngology and Pathology, Pt. B.D. Sharma PGIMS, Rohtak (INDIA), on 50 consecutive patients of either sex, in the age group of 15–70 years. All patients underwent a detailed evaluation including history and general physical examination. All patients were selected on basis of having benign lesions of vocal folds based on clinical diagnosis, supported with indirect laryngoscopy. Patients with cervical spondylosis, osteoarthritis, caries spine and those in whom direct laryngoscopy was contraindicated were excluded. Later, patients, whose histopathology report came as premalignant or malignant, were also excluded from the study.
Preoperative Voice Assessment The preoperative assessment of benign lesions of vocal folds for voice handicap was assessed by VHI-10 scale.
Procedure
Patients were admitted a day before surgery after taking informed written consent. Surgery, to excise the lesion on vocal fold, was performed under general anaesthesia using a suspension video laryngoscope. The general surgical sequence was: general anaesthesia was given. The patient was placed in direct laryngoscopy position (Boyce position). The laryngoscope was placed and stabilised so that the glottis was clearly visualised. The camera was fixed on video laryngoscope. The lesion was excised with cold steel conventional dissection i.e. truncation surgery was done. Haemostasis was achieved and laryngoscope was withdrawn after spraying the larynx with 10% xylocaine. There was no serious complication during and after microlaryngoscopic surgery. Excised lesion of vocal folds was preserved in 10% formalin and was sent for histopathological examination.
Post-operative Patients were advised strict voice rest for first 2 days post operatively. Oral antibiotics (tab levofloxacin 500 mg one OD for 5 days), anti-histaminics (tab levocitrizine 5 mg one OD for 7 days) and proton pump inhibitors (cap pantoprazole 40 mg one BBF for 2 months) were prescribed. Patients were also advised steam inhalation and speech therapy for 3 months at the time of discharge and was kept on regular follow up.
Postoperative voice assessment was done after 4 weeks. Voice handicap was evaluated through postoperative VHI-10 scale.
Statistical Analysis Results were statistically analyzed by using unpaired t test for finding association between different symptoms and habits among different benign lesions and paired t test to assess the voice improvement. The significance level was set at p < 0.05.
Results
On the histopathological examination of biopsy specimen, out of 50 benign lesions of vocal cords, most common were vocal polyps (56%), followed by nodules (32%), and cysts (10%) respectively. There was only one case of papilloma (2%) in this study (Fig. 1). Benign lesions of vocal cords more commonly presented in male patients (70%) than females (30%). Among 28 cases of vocal polyp, males were 67.86% and females were 32.14%. Out of 16 cases of vocal nodules, 11 were males (68.75%) and five females (31.25%). Among 5 cases of vocal cyst, males were 80% and females were 20%. Only patient who had vocal papilloma was a male. The mean age of patients observed in the study was 39.98 ± 14.34 years (range 17–70 years) (Table 1 and Fig. 2). Among the 28 cases of vocal polyp, left vocal cord was most commonly involved (53.57%); followed by right (32.14%), and anterior commissure (14.29%). In vocal nodule 12 out of 16 cases of presented as bilateral vocal nodule (75%), followed by left side (18.75), and right side (6.25%). Out of five vocal cysts three cases involved right side, and two were on left side. Single case of papilloma was present on left vocal cord (Fig. 3).
Fig. 1.
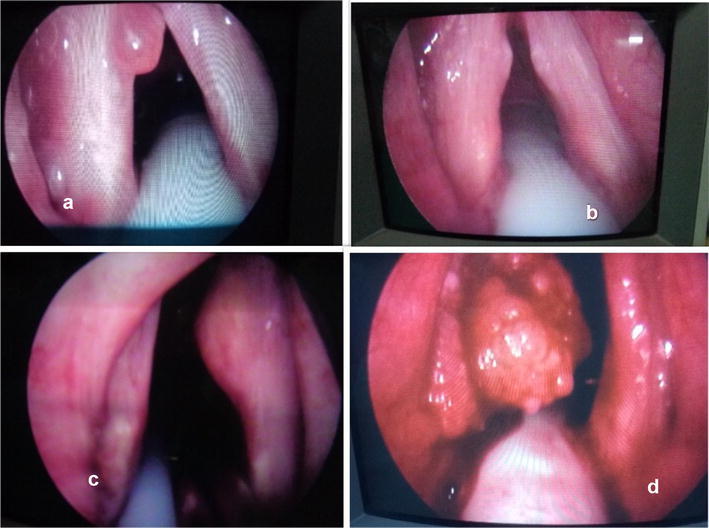
Images showing benign lesions of vocal cords (a polyp, b nodule, c cyst, d papilloma)
Table 1.
Case distributions according to gender and age groups
| Age (years) | Gender | Benign lesions of vocal cords | |||||
|---|---|---|---|---|---|---|---|
| Polyp | Nodule | Cyst | Papilloma | Total | |||
| 10–19 | Male | 1 | 1 | 0 | 0 | 2 | 2 |
| Female | 0 | 0 | 0 | 0 | 0 | ||
| 20–29 | Male | 5 | 2 | 0 | 1 | 8 | 14 |
| Female | 3 | 2 | 1 | 0 | 6 | ||
| 30–39 | Male | 4 | 2 | 0 | 0 | 6 | 9 |
| Female | 1 | 2 | 0 | 0 | 3 | ||
| 40–49 | Male | 6 | 2 | 0 | 0 | 8 | 10 |
| Female | 2 | 0 | 0 | 0 | 2 | ||
| 50–59 | Male | 2 | 2 | 3 | 0 | 7 | 9 |
| Female | 2 | 0 | 0 | 0 | 2 | ||
| 60–69 | Male | 1 | 2 | 0 | 1 | 3 | 4 |
| Female | 1 | 0 | 0 | 0 | 1 | ||
| > 70 | Male | 0 | 0 | 1 | 0 | 1 | 2 |
| Female | 0 | 1 | 0 | 0 | 1 | ||
| Total | 28 | 16 | 5 | 1 | 50 | ||
Fig. 2.
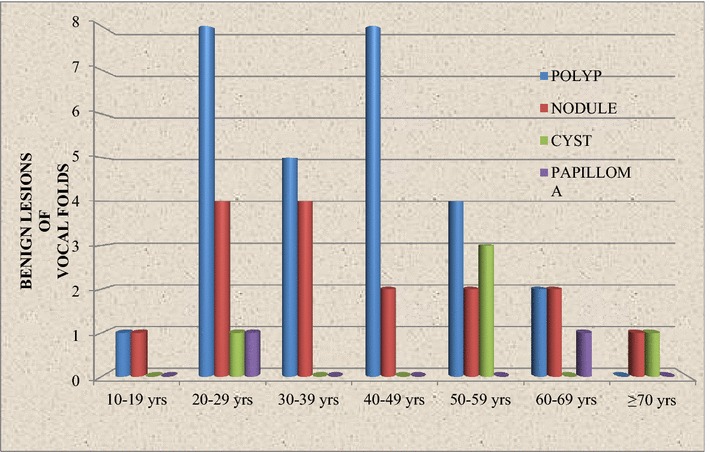
Benign lesions of vocal cords with relation to age and sex
Fig. 3.
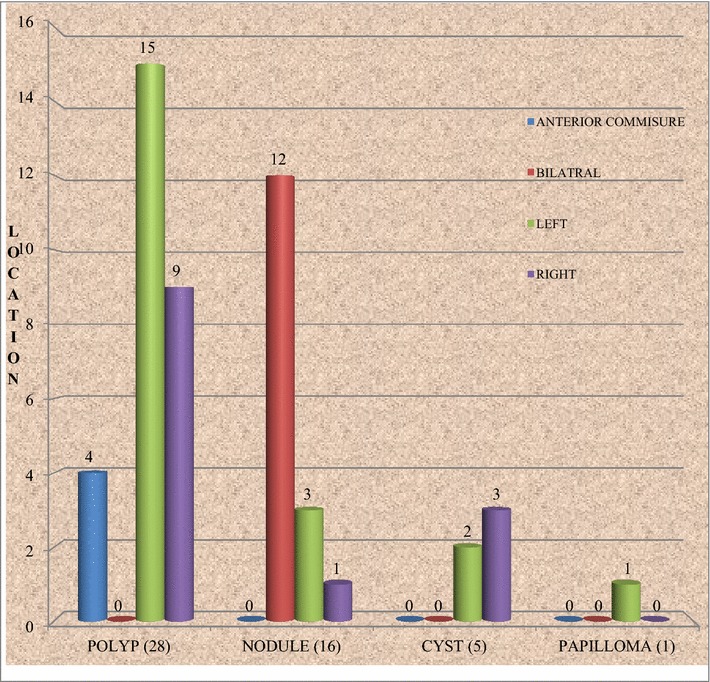
Site of origin of benign lesions of vocal cords
Mean duration of hoarseness was 12.14 ± 7.97 months (range 2–24 months) (Table 2). Vocal fatigue (58%) was the most common associated symptoms; others were throat pain (54%), throat irritation (22%) and respiratory difficulty (12%). Association of vocal fatigue, throat pain, throat irritation, and respiratory difficulty among different lesions was found significant (p = 0.01).
Table 2.
Mean duration of hoarseness
| Benign lesions of vocal cords | Duration of hoarseness (in months) (Mean ± SD) |
|---|---|
| Polyp | 10.32 ± 7.76 |
| Nodule | 15.25 ± 6.60 |
| Cyst | 14.20 ± 10.96 |
| Papilloma | 3.00 |
| p value | 0.134 |
Vocal abuse was found most commonly associated with vocal nodule (68.75%), followed by polyp (57.14%) and cyst (40.0%) respectively. Association of vocal abuse among different benign lesions of vocal cord was found statistically insignificant (p = 0.421). Among benign conditions of vocal cords, most common risk factor was drinking of tea/coffee (58%), followed by smoking (36%), and alcohol intake (18%). Association of these risk factors with benign lesions of vocal cord was found statistically significant (p = 0.01) (Table 3).
Table 3.
Associated symptoms among different benign vocal cord lesions
| Benign lesions of vocal cords | Associated symptoms | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Vocal fatigue | Throat pain | Throat irritation | Respiratory difficulty | ||||||
| Number of cases | Percentage (%) | Number of cases | Percentage (%) | Number of cases | Percentage (%) | Number of cases | Percentage (%) | ||
| Polyp | 28 | 19 | 67.86 | 15 | 53.57 | 12 | 42.86 | 5 | 17.86 |
| Nodule | 16 | 7 | 43.75 | 10 | 62.50 | 8 | 50.00 | 0 | 0.0 |
| Cyst | 5 | 2 | 40.0 | 2 | 40.0 | 2 | 40.0 | 0 | 0.0 |
| Papilloma | 1 | 1 | 100.0 | 0 | 0.0 | 0 | 0.0 | 1 | 100.0 |
| Total | 50 | 29 | 58.0 | 27 | 54.0 | 22 | 44.0 | 6 | 12.0 |
| p value | 0.01 | ||||||||
Out of total 50 patients house wives were most common (28%). They also formed the major group (93.3%) among females. Among benign lesions of vocal cords, next were businessman (14%), farmer (14%), students (10%), government servants (8%) and salesman (6%) (Table 4).
Table 4.
Distribution of patients by occupation
| Occupation | Male | Female | Total | Percentage |
|---|---|---|---|---|
| Accountant | 2 | 0 | 2 | 4 |
| Auto worker | 1 | 0 | 1 | 2 |
| Barber | 1 | 0 | 1 | 2 |
| Bhajan singer | 2 | 0 | 2 | 4 |
| Business | 7 | 0 | 7 | 14 |
| Farmer | 7 | 0 | 7 | 14 |
| Govt. service | 4 | 0 | 4 | 8 |
| Housewife | 0 | 14 | 14 | 28 |
| Nothing | 2 | 0 | 1 | 4 |
| Pandit, Puja | 1 | 0 | 1 | 2 |
| Salesman | 3 | 0 | 3 | 6 |
| Student | 5 | 0 | 5 | 10 |
| Teacher | 0 | 1 | 1 | 2 |
| Total | 35 | 15 | 50 | 100 |
One case initially diagnosed as Reinke’s edema onindirect laryngoscopy (IL) was found to be polyp ondirect laryngoscopy (DL). One out of two cases initially diagnosed as papilloma on IL was appreciated as vocal nodule on DL. Comparing of IL and DL finding was found to be statistically significant (p = 0.01).
Out of 28 diagnosed of vocal polyp cases on IL, 3 were reported vocal nodules on histopathology examination (HPE). Out of initial 14 diagnosed vocal nodule on IL, 2 cases were reported as vocal polyp on HPE. One cases initially diagnosed as Reinke’s edema on IL was found to be polyp on HPE. Out of two cases with diagnosis of papilloma on IL was reported polyp on HPE. Comparison between IL and HPE finding was statistically significant (p = 0.01).
Out of 30 diagnosed cases of vocal polyp on Direct Laryngoscopy (DL), 4 cases were found to be vocal nodule on HPE. Among the 14 diagnosed cases of vocal nodule on DL, 2 were diagnosed as polyp on HPE. DL finding and HPE were same with respect to cyst and papilloma. Comparison between DL and HPE report was statistically significant (p = 0.01) (Fig. 4).
Fig. 4.
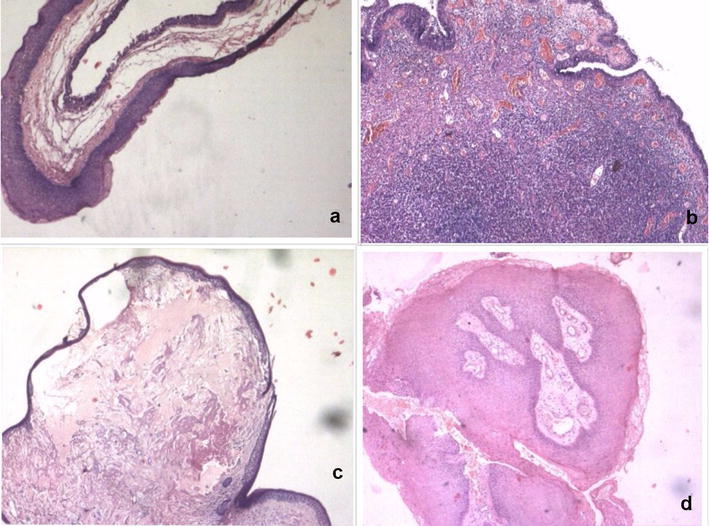
Images showing HPE of benign lesions of vocal cords (a polyp, b nodule, c cyst, d papilloma)
VHI-10 Score Preoperatively mean VHI-10 was 22.60 ± 2.45 and it was 11.26 ± 1.62 post operatively. Mean difference between preoperative and postoperative VHI-10 score was 10.84, depicting significant improvement in voice of the patients. The difference between pre and post-op VHI-10 was foundto be statistically significant (p = 0.01) (Tables 5, 6 and Fig. 5).
Table 5.
Mean VHI-10 score of pre and post-op (4 weeks) periods in benign lesions of vocal cords
| Benign lesions of vocal cords | VHI-10 SCORE (pre-op) | VHI-10 SCORE (post-op 4 weeks) | p value |
|---|---|---|---|
| Polyp | 22.96 | 12.07 | 0.01 |
| Nodule | 22.00 | 11.38 | 0.01 |
| Cyst | 22.60 | 11.20 | 0.01 |
| Papilloma | 22.00 | 12.00 | 0.01 |
| Total | 22.60 | 11.76 | 0.01 |
Table 6.
VHI-10 score in pre-op and post-op (4 weeks)
| VHI-10 (pre-op) | VHI-10 (post-op) | Mean difference | |
|---|---|---|---|
| Mean | 22.60 | 11.76 | 10.84 |
| p value | 0.01 | ||
Fig. 5.
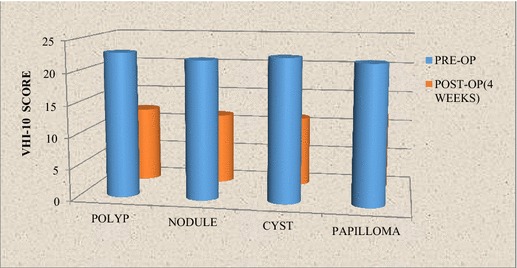
Pre and post-op (4 weeks) VHI-10 scores in various benign lesions of vocal cords
Discussion
Although benign lesions of vocal cords are not very rare, however these are of clinical interest and importance, as they interfere with the normal voice and ultimately speech, hence affecting one’s identity. Rarely, these may cause obstruction of the respiratory tract as in respiratory papillomatosis. Since these lesions are not malignant, they are usually not life threatening. It is mandatory to distinguish them from malignant laryngeal lesions by histopathology. A clinical diagnosis of nodules, polyps or cysts does not rule out a malignancy unless the lesion resolves with treatment or is reported benign on histopathological examination [1, 2].
The most common benign lesions of vocal cords are singer’s nodule, polyps, papilloma, polypoidal degeneration (Reinke’s edema) and cysts. Others are sulcus vocalis, mucosal bridge, intracordal cysts, vocal cord varices and anterior webs. Some studies have reported vocal polyp as most common benign lesion [9] whereas some found vocal nodule to be most common [10]. In the present study, majority of the benign lesions of vocal cords encountered were vocal polyps, vocal nodules, vocal cysts and a single case of papilloma with vocal polyp being most common. However, other benign lesions like intubation granuloma, contact ulcer granuloma, Reinke’s edema were not encountered. All patients presented with complain of hoarseness, of variable duration. Other associated symptoms were throat pain, vocal fatigue, throat irritation and respiratory difficulty.
Hegde et al. [11] found vocal cord polyp in majority (40.47%), other lesion in decreasing order were vocal nodules (28.57%); tuberculosis of larynx (14.30%), laryngocele (4.76%), laryngeal web (4.76%), epiglottic cysts (4.76%) and subglottic hemangioma (2.38%). Singh et al. [12] reported most common lesion to be vocal polyp (40.7%), followed by nodule (28.4%), papilloma (22.2%) and cyst (0.05%). Cecatto et al. [9] also reported vocal polyp was the most prevalent lesion (29.62%) amongst the benign lesions. Amed et al. [13] also reported that majority of the benign lesions of vocal cord were polyp (48%), followed by nodule (20%), and papilloma (04%). However, Chopra and Kapoor [10] reported most common lesion to be vocal nodules (33.33%), followed by vocal cysts (17.3%), and polyps (16%) in their study group. Similar results were also observed by Wani et al. [14] who found that vocal nodules were the commonest (37%), followed by vocal polyps (26%), Reinke’s edema (4%), intracordal cyst (4%), contact ulcer (3%), saccular cyst (2%) and papillomatosis (1%). Similar to most of these studies, vocal polyp was most common in our study.
Vocal Polyp Kambic et al. [15] observed most common age group of 40–50 year, and female predominance (52%) as compared to males (48%). Cecatto et al. [9] found mean age 46.9 years, with equal distribution among males and females and left vocal cord most frequently involved (56.25%). Martins et al. [16] reported vocal polyp more common in the age group of 41–60 years (51.31%) and reported slight preponderance among females. Whereas, we observed male preponderance with mean age 39.98 ± 14.34 years. But similar predominantly left vocal cord involvement. The reason of discordance was may be due to larger sample size of these studies and difference in association of risk factors, and different race and profession.
Vocal Nodule McGlashen reported that vocal nodules were bilateral, small swellings (less than 3 mm in diameter) that develop on the free edge of the vocal cord at approximately the mid-membranous portion [1], as was also observed in the present study. In our study, vocal nodules were bilaterally found in majority.
Vocal Cysts Our findings were similar to Shvero et al. [17], who reported mean age of 54 years in vocal cysts patients. Martins et al. [18] found vocal cyst to be unilateral in 93% and bilateral in 7% case. In our study vocal cyst were dominantly found on right side.
Symptoms of the Benign Lesions of Vocal Cords
Mean duration of hoarseness with benign lesion of vocal cords observed were similar to various other studies. Chopra et al. [10] reported majority of cases (68.6%) presented within 1 year and 14.9% between 1 and 2 years of the symptom of hoarseness. Cecatto et al. [9] found hoarseness was present in all cases (100%). Singh et al. [12] reported hoarseness in 69% cases. Hedge et al. [11] reported hoarseness in all the study group (100%), along with cough (23.81%), foreign body sensation in throat (19.05%), throat pain (9.52%), difficulty in swallowing (4.76%) and difficulty in breathing (2.38%). The duration of symptoms in their studies ranged from 1 month to 2 years; the mean duration of hoarseness was 3.93 ± 2.32 months. Martins et al. [16] found hoarseness (100%) in all cases of 1–5 years (50%). Wani et al. [14] found that the hoarseness was a predominant symptom in 73% patients, followed by cough (20%), foreign body sensation (19%), heart burn (17%), frequent throat clearing (13%) and low grade pain in (9%). Saudi reported hoarseness as main presentation in 54 cases (90%) and stridor in 6 cases (10%). The majority of the patients in his study (73.3%) presented within 1 year and 15% between 1 and 2 years of onset of hoarseness [19]. In our study, vocal fatigue (58%) was the most common associated symptoms; others were throat pain (54%), throat irritation (22%) and respiratory difficulty (12%).
Predisposing Factors Baitha et al. [20] found history of vocal abuse (23%), followed by smoking (13.63%), and tobacco chewing (8%). Saudi reported history of vocal abuse (45%), smoking (47%) and alcohol intake (7%). He also reported that the highest incidence was seen in housewives (25%) followed by school teachers (21.7%) and students (18.3%) among vocal polyp [19]. Whereas, in our study housewives were most commonly (30%) affected, followed by businessman (14%), farmer (14%), students (10%), government servants (8%) and salesman (6%). Chopra et al. [10] noted highest incident in housewives (25.3%), followed by shopkeepers (16.4%), businessmen (14.9%), students (12%), and teachers (10.4%), farmers (5.97%), salesman (3%) and others (10%).
VHI-10 comparison: Rosen et al. [21] noted statistically significant reductions in patients VHI scores following microsurgical excision and a program of pre and postoperative voice therapy. Amir et al. [22] received significantly lower score in pathological groups as compared to control group. Cecatto et al. [9] reported 95% of the patients showed some improvement on their voice, within 60 days after surgery. Hegde et al. [10] reported complete recovery (100%) postsurgery and speech therapy. Saudi reported majority of patients (90%) were totally symptom free after surgery and 10% had partial recovery of their symptoms [19]. In our study all patients were benefitted, assessed using VHI-10 score.
Conclusion
The benign lesions of vocal cords produces symptoms which can vary from hoarseness to stridor, can affect social functioning and work performance, and which have a significant emotional impact. Speech therapy following microlaryngeal surgery forms an essential part of treatment, to avoid recurrence. VHI-10 scale as found to be a useful and convenient tool in measuring patient voice handicap and to see improvement after surgery.
Compliance with Ethical Standards
Conflict of interest
Authors received no funding for this study and have no conflict of interest to disclose.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
References
- 1.McGlashen J. Disorders of the voice. In: Hibbert J, editor. Scott-Brown otolaryngology, head and neck surgery. 7. London: Edward Arnold; 2008. pp. 2192–2210. [Google Scholar]
- 2.Altman KW. Vocal cord masses. Otolaryngol Clin North Am. 2007;40:1091–1108. doi: 10.1016/j.otc.2007.05.011. [DOI] [PubMed] [Google Scholar]
- 3.Yadav S, Sahni J, Raj B, Chawla R, Yadav J, Singh B. Laryngeal cyst-causing haemoptysis. An unusual presentation. Indian J Chest Dis All Sci. 1986;28:50–51. [PubMed] [Google Scholar]
- 4.Johns MM. Update on the etiology, diagnosis and treatment of vocal cord nodules, polyps and cysts. Curr Opin Otolaryngol Head Neck Surg. 2003;11:456–461. doi: 10.1097/00020840-200312000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Murry T, Rosen CA. Outcome measurements and quality of life in voice disorders. Otolaryngol Clin North Am. 2000;33:905–916. doi: 10.1016/S0030-6665(05)70251-6. [DOI] [PubMed] [Google Scholar]
- 6.Halawa WE, Perez SS, Antonio CG. Measurement of vocal handicap in patients with vocal nodules and functional dysphonias. Egypt J Ear Nose Throat Allied Sci. 2011;12:121–124. doi: 10.1016/j.ejenta.2011.09.003. [DOI] [Google Scholar]
- 7.Rosen CA, Lee AS, Osborne J, Zullo T, Murry T. Development and validation of the Voice Handicap Index-10. Laryngoscope. 2004;114:1549–1556. doi: 10.1097/00005537-200409000-00009. [DOI] [PubMed] [Google Scholar]
- 8.Smits R, De Jong HMF. The relation of vocal cord lesions and voice quality to voice handicap and psychosomatic well-being. J Voice. 2012;26:466–470. doi: 10.1016/j.jvoice.2011.04.005. [DOI] [PubMed] [Google Scholar]
- 9.Cecatto SB, Costa KS, Garcia RID, Haddad L, Angelico Junior FV, Rapoport P. Vocal cord polyps: clinical and surgical aspects. Rev Bras Otorrinolaringol. 2002;68:543–548. doi: 10.1590/S0034-72992002000400013. [DOI] [Google Scholar]
- 10.Chopra H, Kapoor M. Study of benign lesions undergoing miccrolaryngeal surgery. Indian J Otolaryngol Head Neck Surg. 1977;49:276–279. doi: 10.1007/BF02991291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hegde MC, Kamath PM, Bhojwani K, Peter R, Babu PR. Benign lesions of the larynx—a clinical study. Indian J Otolaryngol Head Neck Surg. 2005;57:35–38. doi: 10.1007/BF02907624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Singh M, Bandyopadhyay S, Gupta SC, Rai A. A study of manifestations of extrapulmonary tuberculosis in the ENT region. Indian J Otolaryngol Head Neck Surg. 2002;54:242–245. doi: 10.1007/BF02993115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ahmed SU, Kabir M, Alam KA, Hasan MD, Ahmed KU, Khan HS. Benign vocal cord lesions—a study of 25 cases. J Soc Otolaryngol Head Neck Surg Bangladesh. 2006;6:5–6. [Google Scholar]
- 14.Wani AA, Rehman A, Hamid S, Akhter M, Baseena S. Benign mucosal cord lesion as a cause of hoarseness of voice—a clinical study. Otolaryngology. 2012;2:3–4. [Google Scholar]
- 15.Kambic V, Radsel Z, Zargi M, Acko M. Vocal cord polyps: incidence, histology and pathogenesis. J Laryngol Otol. 1981;95:609–618. doi: 10.1017/S0022215100091167. [DOI] [PubMed] [Google Scholar]
- 16.Martin RH, Defaveri J, Domingues MA, Silva RD. Vocal polyps: clinical, morphological and immunohistochemical aspects. J Voice. 2011;25:98–106. doi: 10.1016/j.jvoice.2009.05.002. [DOI] [PubMed] [Google Scholar]
- 17.Shvero J, Koren R, Sandbank THJ, Feinmesser R, Gal R. Clinicopathologic study and classification of vocal cord cysts. Pathol Res Pract. 2000;196:95–98. doi: 10.1016/S0344-0338(00)80039-4. [DOI] [PubMed] [Google Scholar]
- 18.Martins RGH, Santana MF, Tavares ELM. Vocal cysts: clinical, endoscopic, and surgical aspects. J Voice. 2011;25:107–110. doi: 10.1016/j.jvoice.2009.06.008. [DOI] [PubMed] [Google Scholar]
- 19.Saudi S. Benign lesions of the vocal cords in different ages: prospective Study of 60 Cases. Middle East J Age Ageing. 2014;11:32–37. doi: 10.5742/MEAA.2014.92395. [DOI] [Google Scholar]
- 20.Baitha S, Raizada RM, Kennedy AK, Puttewar MP, Chaturvedi VN. Predisposing factors and etiology of hoarseness of voice. Indian J Otolaryngol Head Neck Surg. 2004;56:186–190. doi: 10.1007/BF02974347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rosen CA, Murry T, Zinn A, Zullo T, Sonbolian M. Voice Handicap Index change following treatment of voice disorders. J Voice. 2000;14:619–623. doi: 10.1016/S0892-1997(00)80017-X. [DOI] [PubMed] [Google Scholar]
- 22.Amir O, Tavor Y, Leibovitzh T, Ashkenazi O, Michael O, Primov-Fever A, Wolf M. Evaluating the validity of the Voice Handicap Index-10 (VHI-10) among Hebrew speakers. Otolaryngol Head Neck Surg. 2006;135:603–607. doi: 10.1016/j.otohns.2006.06.1252. [DOI] [PubMed] [Google Scholar]