

Abstract
Lethal midline granuloma is a rare disease, characterised by progressive unrelenting necrosis and mutilation of nose, midline facial tissues and other respiratory passages. This particular type of disease is heterogeneous in its pathogenesis, non-specificity of symptoms obscures timely and correct diagnosis and is responsible for delay in of treatment which can be detrimental as this disease calls for immediate intervention. We present a case report of 60 year old female who gave short one-month history of clinical symptoms.
Keywords: Lethal mid line granuloma, T cell lymphoma, Chronic non specific inflammation, Lymphocytic infiltrate
Introduction
Lethal midline granuloma is a tumour responsible for the classical aggressive destruction of midface. This disease is characterised by necrotizing destructive mucosal lesions of upper aero digestive tract. The patients complain of rhinorrhoea, epistaxis, nasal obstruction, and pain. Also referred as Stewart’s granuloma, polymorphic reticulosis, and T/NK cell lymphomas. Here we present a case of T cell lymphoma in a 60 year old female who came with a short clinical history.
Case Report
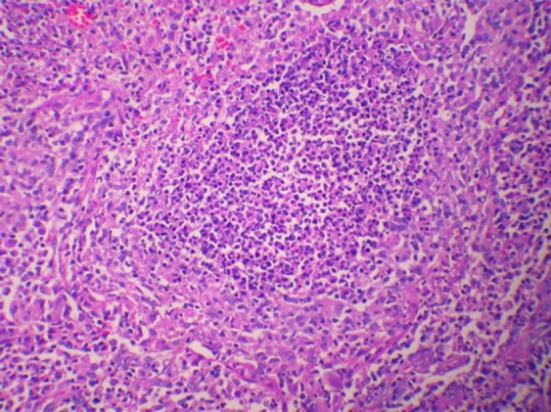
A 60 year old female presented with swelling and pain on the tip of the nose for 2 weeks. Patient also had treatment for nasal vestibulitis and was not subsiding so was referred to our hospital. There was h/o fever and mucopurulent discharge since a week. On examination there was diffuse redness of nose with scaling at the tip and crusting in the nasal cavity (Fig. 1). Patient was treated with a course of antibiotics and analgesics. After 2 weeks patient revisited our OPD with worsening of symptoms with blood tinged mucopurulent discharge on and off. On examination of nose erythematous hyper pigmented plaque with crusting present over ala of nose with destruction of columella, slough present over the floor of left nasal cavity (Fig. 2). Biopsy was taken which showed chronic non-specific inflammation. Patient was treated with antibiotics, antifungals, analgesics and alkaline nasal douching. Initially there was improvement for few days. But later the disease was progressive with worsening of symptoms, again biopsy was repeated twice which again showed chronic inflammation picture (Fig. 3). Patient was aggressively treated with broad spectrum IV antibiotics, antifungals, analgesics and alkaline nasal douching. In spite of all efforts disease was still progressive at the end of fourth week of hospital stay patient had destruction of nasal framework with depression of tip of the nose (Figs. 4 and 5). Biopsy was repeated from multiple sites of skin, nasal septum, finally case was discussed with pathologist, they concluded that microscopic features was suspicious of T cell lymphoma (Fig. 6) [1]. Patient was advised chemo radiation but patient defaulted treatment in our centre and went on discharge against medical advice. Hence we couldn’t not have the further follow up of the patient.
Fig. 1.

Erythematous plaque with scaling over tip of nose and crusting over columella of nose
Fig. 2.

Erythematous hyper pigmented plaque with crusting present over ala of nose with destruction of columella, slough present in the floor of nose
Fig. 3.
Chronic nonspecific inflammation
Fig. 4.

Hyper pigmented plaques with crusting present over ala of nose and tip extending towards nasolabial fold. Destruction of ala and columella with extension forwards philtrum with depression of tip
Fig. 5.

Diffuse crusting and slough with destruction of ala and columella
Fig. 6.

T cell lymphoma
The other head and neck findings were within normal limits.
Discussion
Lethal midline granuloma is a very rare disease. The term “lethal midline granuloma” was first described by MC Bride in 1897. Macroscopically look like necrotic granulomas and are characterised by destruction of nose and para nasal sinuses with erosion of soft tissues, bone and cartilages. Patient shows lethal and aggressive course with rapid destruction of nose and face (midline) therefore termed as “lethal midline granuloma”. Also referred as NK/T cell lymphoma. May occur at any age from 1st to 9th decade with male predominance. Seen mostly in Asian and Mexican region. The disease has been classically divided into three stages, i.e. prodromal stage, period of activity and terminal stage which is responsible for underlying thickening of mucosa, progressive destruction of nasal framework, palate, upper lip extending into aero digestive tract, gross mid facial destructive lesions, exhaustion, dissemination into distant sites and eventual death. The major symptoms are nasal stuffiness with or without nasal discharge. Oral or nasal ulcers with conjunctivitis may also occur. Morphologically it is characterised by extensive ulcerations with a diffuse lymphomatous infiltrate.
Disease is very much aggressive with rapid downhill course [2]. Untreated, this disease has a very high mortality reaching almost 100% due to septicaemia, perforation into blood vessels or penetration into brain leading to abscess. Wrang et al. reported chemotherapy followed by involved field external radiation beam to be beneficial in patients and prolonged progression free survival rates. The confusing clinical picture of this disease calls for high degree of suspicion for correct diagnosis and early intervention to prolong the patient survival.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Thakur JS, Mahajan A, Saluja M, Mohindroo NK. Deceptive nasal NK/T-cell lymphoma. Trop Doct. 2017;47(3):268–271. doi: 10.1177/0049475516684088. [DOI] [PubMed] [Google Scholar]
- 2.Shah SN, Mistry PR, Chauhan GR, Chauhan V, Pillai J. Nasal NK/T cell lymphoma presenting with perforation of palate: a case report and review of literature. J Clin Diagn Res. 2017;11(3):MD01–MD03. doi: 10.7860/JCDR/2017/24011.9356. [DOI] [PMC free article] [PubMed] [Google Scholar]