

Abstract
Tumor growth and metastasis in nasopharyngeal carcinoma (NPC) patients recent research stated that intracellular Hsp70 is a stress protein as the main factor for the growth, invasion and metastasis of NPC. To analyze intracellular Hsp70 protein expression of NPC patients which correlate with staging of NPC as clinical manifestation. Formalin-fixed paraffin-embedded biopsy specimens from 20 NPCs histopathology and clinically. The expression of intracellular Hsp70 was obtained using monoclonal antibody of Anti Human Hsp70 from Santa Cruz Biotechnology, California, USA. The assessment of the staining was performed with Remmele methode by Histopathologies doctor Consultant. 20 NPC patients met the inclusion and exclusion criteria. The data showed a negative intracellular of Hsp70 expression by 15% for all sample that consist of 1 patient of stage I, II, III, and none for stage IV. Then, followed by 25% of mild positive intracellular Hsp70 expression which consisted of 0 patient of stage I and III, 2 patients of stage II, and 3 patients of stage IV. Followed by 50% of moderate positive intracellular Hsp70 expression which consisted of 0 patient of stage I and II, 1 patient of stage III, and 9 patients of stage IV. Spearman test results test scored p = 0.001 with a correlation coefficient of 0.671. The correlation of intracellular Hsp70 protein expression with stage (I, II, III, and IV) in NPC patients was significant (p < 0.05). There was a correlation between increased intracellular Hsp70 expression and the stage of patients with nasopharyngeal carcinoma.
Keywords: Nasopharyngeal carcinoma, Intracellular Hsp70 protein expression, Staging status
Introduction
Nasopharyngeal carcinoma patients (NPC) is often discovered at an advanced stage. The advanced stage shows the tumor size and metastasis are bigger than in the early stages [1]. Tumor growth and metastasis in NPC patients allegedly as a role of some molecular biomarkers that have been identified in tumor specimens of NPC patients. Recent research stated that Heat Shock Protein 70 (Hsp70) is a stress protein that becomes a major factor for growth, invasion and NPC metastasis [2]. However, until now the research on Hsp70 correlation with NPC stage rarely performed in Surabaya, Indonesia.
The current prediction of NPC prognosis is generally based on clinical staging assessments, i.e., by assessing primary tumor (T), cervical (N)) metastases and distant metastasis (M). Many research found that in NPC patients with the same clinical stadium gives a different prognosis. This suggests that TNM assessments have not been able to provide precise predictions for NPC prognosis, so it is necessary to develop molecular biomarkers on NPCs that could help clinicians to improve prognostic prediction and therapeutic interventions in NPC patients [3].
The existence of non-self NPC is becaming a trigger to the immune response or immune surveillance that basically protective against a strange antigen called as cancer cell antigen. Immune surveillance of the body causes stress on NPC cells that ultimately secrete a protein such as Hsp70. The studies on NPCs show that high levels of Hsp70 in the nucleus are related to primary tumor (T) that has a classification, metastasis, death, and show a poor prognosis [4]. However, until now the correlation of intracellular Hsp70 expression and NPC cell progression has not been clearly identified [2].
The nasopharyngeal carcinoma cell is a normal nasopharyngeal cell that undergoing an increased transformation, as well as the morphological structure of surface proteins and proteins in cancer cells. The change of protein on the surface and inside the cancer cells will cause the introduction of the immune system by cytotoxic T cells, NK cells, and macrophages through immunological reactions. The introduction by the immune system will be captured by Fas receptors that activate Fas-associated protein with death domain (FADD) and Death-Associated Protein (DAXX), resulting in activation of caspase 8, Apaf 1, caspase 9 and caspase 3. Besides, the introduction by the immune system will cause stress on cancer cells, thus increasing Hsf1 protein and causing an increase of Hsp70. In the NPC cells obtained p53 protein (wild type) that activates the Hsp70 transcription factor, so Hsp70 were produced more [5].
FADD and DAXX proteins function in the process of cancer death cell by functioning as a protein proapoptosis. While intracellular Hsp70 is a stress protein that serves to inhibit the process of apoptosis. The inhibited apoptotic process will cause increasing proliferation and metastasis of NPC cells with increasing clinical manifestations of the stage [6].
There is a difference of Hsp70 expression and a stage in NPC patients, i.e., at stage III + IV Hsp70 expression is bigger 6.034 than stage I + II [7]. Other studies suggested that the difference in Hsp70 expression in stage I: II: III: IV is 3: 4: 6: 9 3 [3]. Intracellular Hsp70 is a stress protein that correlated with tumor growth, but until now there is unknown intracellular Hsp70 expression that is correlated with various stages in NPC patients at Otolaryngology of Dr. Soetomo General Hospital Surabaya. Based on the above descriptions the researchers intend to examine the correlation of intracellular Hsp70 expression with various stages in NPC patients at Otolaryngology Dr. Soetomo General Hospital Surabaya.
Methods
An observational analytic research with the cross-sectional approach was applied in this study. The data taken since February to July 2014 at Oncology Unit (POSA at Installation of Anatomical Pathology (PA) Dr. Soetomo General Hospital Surabaya, and Laboratory of Medical Biology (Biomed), Faculty of Medicine, Universitas Brawijaya Malang. The samples used were NPC patients with histopathological results of a carcinoma WHO type I, II, III of various stages and had never received radiochemotherapy, while the sampling technique used was consecutive sampling. The inclusion criteria were Nasopharyngeal Carcinoma (NPC) patients who have sufficient paraffin blocks that examined in the intracellular of Hsp70 expression, while the exclusion criteria were the damaged or unqualified paraffin blocks at the time of IHC preliminary process.
The independent variables were intracellular Hsp70 expression and the dependent variable was NPC stage. The researchers performed anamnesis, clinical examination including the ears, nose, throat, head, and neck and determine the stage of the patient. Thus, determine the T (Tumor) from the head CT scan of the neck that focus on nasopharynx with and without contrast, N (Nodule) from the measurement using a ruler of the brand AMC-WP017 in centimeters, and M (Metastasis) that known from chest radiographs and liver function tests, the last determine the stages of NPC.
The researchers collected histopathologic examination results from the nasopharyngeal biopsy and looked for paraffin blocks that suited the patients in the Anatomy Pathology Installation (PA) of Dr. Soetomo General Hospital Surabaya. Also, the researchers sent paraffin blocks to the Laboratory of Medical Biology Faculty of Medicine Universitas Brawijaya Malang to performed immunohistochemical dissolution with Hsp70 antibody. Assessment and calculation of intracellular Hsp70 expression were performed by a specialist of Pathologist Anatomy consultant at Anatomical Pathology Installation (PA) Dr. Soetomo General Hospital. The researchers recorded the results of Hsp70 intracellular expression scales on the data collection sheets and analyzed the data.
The data obtained was analyzed by Spearman’s correlation test that used to determine the correlation between NPC stage and intracellular Hsp70 expression on NPC. The intracellular Hsp70 expression was assessed as an ordinal variable based on the scale described above and the NPC stage was assessed as an ordinal variable. The chosen level of significance was (α) = 0.05.
Results
The research was conducted at POSA Otolaryngology Dr. Soetomo General Hospital Surabaya from February to April 2014. The samples enrolled was 20 of Nasopharyngeal Carcinoma (NPC) patients. The recorded baseline data includes the distribution of patient data by sex, age, occupation, address, and ethnicity. Immunohistochemical examination results in the form of intracellular Hsp70 expression was on NPCs assessed that in Remmele scale index (RSI) by an anatomical independent pathologist of an independent consultant. Spearman’s test statistic test was used to determine the correlation between increased intracellular Hsp70 expression and stage (I, II, III, IV) on NPC.
The highest number of NPC patients in the age group of 40–49 years old was 9 cases (45.00%), followed by age group of 50–59 years old was 5 cases (25.00%) and of 20–29 years old was 3 cases (15.00%). The youngest patient was 22 years old and the oldest was 62 years old (Table 1). Based on sex, the number of male patients was higher by 12 patients (60.00%) than the female by 8 patients (40.00%) and the comparison between men and women was 1.5: 1 (Table 1).
Table 1.
Characteristics of subject by age
| Age (y/o) | Amount | % |
|---|---|---|
| 20–29 | 3 | 15.00 |
| 30–39 | 1 | 5.00 |
| 40–49 | 9 | 45.00 |
| 50–59 | 5 | 25.00 |
| 60–69 | 2 | 10.00 |
| Total | 20 | 100.00 |
| Sex | Amount | % |
|---|---|---|
| Male | 12 | 60.00 |
| Female | 8 | 40.00 |
| Total | 20 | 100.00 |
The results of the most ethnic groups in NPC patients were the Javanese by 15 patients (75.00%), the Madurese by 4 patients (20.00%) and the Dayak tribe by 1 patient (5.00%) (Table 2). Based on the result the type of job of the patients, farmer was 9 patients (45.00%) followed by entrepreneur 4 patients (20.00%) (Table 3). While the results of the analysis by the most obtained on the distribution of histopathology were WHO type III by18 patients (90.00%) followed by WHO type II by 2 patients (10.00%) (Table 4).
Table 2.
Characteristics of research subjects based on tribe of nations
| Tribe | Jumlah | % |
|---|---|---|
| Javanese | 15 | 75.00 |
| Maduranese | 4 | 20.00 |
| Dayak | 1 | 5.00 |
| Total | 20 | 100.00 |
Table 3.
Characteristics of subject research by type of job
| Job | Jumlah | % |
|---|---|---|
| Farmer | 9 | 45.00 |
| Factory-employee | 1 | 5.00 |
| Self-employee | 4 | 20.00 |
| Factory-security | 2 | 10.00 |
| Teacher | 1 | 5.00 |
| Housewives | 2 | 10.00 |
| Civil servant | 1 | 5.00 |
| Total | 20 | 100.00 |
Table 4.
Characteristics of research subjects by type of hispatology
| Histopatology | N | % |
|---|---|---|
| WHO type I | 0 | 0 |
| WHO type II | 2 | 10.00 |
| WHO type III | 18 | 90.00 |
| Total | 20 | 100.00 |
The result examination of Hsp70 intracellular expression on stage I NPC has not obtained an expression or negative (−) in 1 sample. In stage II NPC there was 1 sample with negative expression and 2 samples of weak positive expression (+). In stage III NPC we obtained 1 sample with negative expression and 1 sample of moderate positive expression (++). While in stage IV NPC, 3 samples were obtained with weak positive expressions and 9 samples with moderate positive expression, also 2 samples of strong positive expression (+++) (Table 5).
Table 5.
Correlation between intracellular Hsp70 expression and stage in nasopharyngeal carcinoma
| Intracellular Hsp70 expression (IRS scale) | Stage | Amount | % | |||
|---|---|---|---|---|---|---|
| I | II | III | IV | |||
| Negative (−) | 1 | 1 | 1 | 0 | 3 | 15.00 |
| Weak positive (+) | 0 | 2 | 0 | 3 | 5 | 25.00 |
| Moderate positive (++) | 0 | 0 | 1 | 9 | 10 | 50.00 |
| Strong positive (+++) | 0 | 0 | 0 | 2 | 2 | 10.00 |
| Total | 1 | 3 | 2 | 14 | 20 | 100.00 |
The weak Intracellular positive of Hsp70 expression was 15% of all samples. Moderately of positive intracellular Hsp70 expression was 25% of all samples, and there was an increase in the number of cells that gave positive, moderate and strong positive expressions at stage I, II, III, and IV. The results of Hsp70 intracellular immunohistochemical examination of NPC tissue were identified by the presence of dark brown color in the nucleus and cytoplasm of tumor cells. The observation and analysis of intracellular Hsp70 expression were performed with a binocular microscope with 400× magnification. Immunohistochemical painting results are shown in Figs. 1, 2, 3 and 4.
Fig. 1.
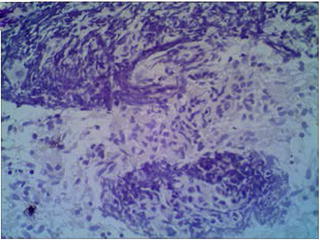
Intracellular Hsp70 painting results on KNF tissue with immunohistochemical techniques obtained negative intracellular Hsp70 expression (−)
Fig. 2.
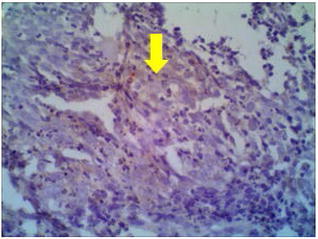
Intracellular Hsp70 painting results on KNF tissue with immunohistochemical techniques obtained weak intracellular Hsp70 expression (+)
Fig. 3.
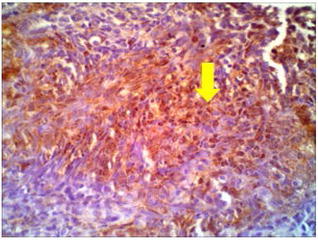
Intracellular Hsp70 painting results of KNF tissue with immunohistochemical technique obtained moderate positive intracellular Hsp70 expression (++)
Fig. 4.

Intracellular Hsp70 painting results on KNF tissue with immunohistochemical techniques obtained strong positive intracellular Hsp70 expression (+++)
Statistical analysis of the correlation between Hsp70 intracellular expression and NPC stage was calculated by Spearman’s test that obtained p = 0.001 and correlation coefficient was 0.671. Thus, intracellular Hsp70 expression and the stage I, II, III, and IV in NPC patients showed a significant correlation (p < 0.05) (Table 6).
Table 6.
Statistical analysis results of correlation Hsp70 intracellular expression and NPC stage
| IRS | Stadium | ||
|---|---|---|---|
| Spearman’s rho | |||
| IRS | Correlation coefficient | 1.000 | .671 |
| Sig. (2 tailed) | – | .001* | |
| N | 20 | 20 | |
| Stadium | Correlation coefficient | .671 | 1.000 |
| Sig. (2 tailed) | .001* | – | |
| N | 20 | 20 | |
* indicate statistically significant values, p < 0.05
Discussion
Research in Adam Malik Medan Hospital provided data that the highest number of Nasopharyngeal Carcinoma (NPC) patient was 28 (35.8%) cases in the group of 40–49 years old, followed by a group of 30–39 years old was 21.4%. The distribution of NPC patients by age, the incidence begins to increase at age 45–54 years old and then decreases after that. Most of NPC patients were found in the productive age of 30–59 years old (about 80%), with peak age between 40 and 49 years old and the highest incidence found in 40–60 years old [8, 9]. Within productive age, workers may have the possibility of higher exposure carcinogenic substances or pollution. EBV infection as one risk factor in NPC has a latency period in the infected nasopharyngeal cells, about 20–25 years without symptoms of primary EBV infection in childhood and asymptomatic. The process of malignancy in NPC occurs after latent infection that to cause a high incidence at the age of 40–60 years old [10].
Previous research was obtained comparison data between men and women by 4: 1 [11]. While the comparison of male and female in Adam Malik Medan Hospital was 2.5: 1 [12]. In the distribution of NPC patients by sex, the highest number of male patients found (70%), and the ratio between men and women was 3: 1 [8, 9]. The living habits such as smoking is going to increase the risk of NPC 2–6 times as well as exposure to steam, dust fumes and chemical gases in the workplace. While exposure to formaldehyde in the workplace increases the risk of NPC 2–4 times, and increased in workers who inhale firewood smoke, also the risk increases 2 times in workers who exposed to the industrial heat and combustion products [13].
Previous studies in 36 cases of NPC showed the most tribe infected was the Javanese by 31 patients (83.33%), Madurese by 5 patients (13.89%) and Dayak tribe by 1 patient (2.78%) [14]. Based on the results the most infected patients were from coastal areas. Because in coastal areas many people consume salted and smoked fish that containing nitrosamine, an important carcinogen for EBV activation. In this study, there were differences in the distribution of ethnic groups due to the largest population in the city of Surabaya as the location of research was the Javanese.
The most types of the job of the patients were farmers by 9 patients (45%) followed by self-employed 4 patients (20%) that consisting of 1 street vendor, 2 fish traders, and one furniture craftsman. Other studies have also found an increased risk of NPC occurring in workers who working in combustion-burning environments (ash, charcoal). The ratio of worker’s exposure cannot be determined because it was dependent on frequencies and endemic areas [15]. Smokers and occupational exposure to formaldehyde and wood dust were also a risk factor. There were several major chemicals that known to cause NPCs based on occupational exposure, such as bleach, acid and base agents, sulfuric acid, inks, formaldehyde, and pesticides. The risk of exposure for 10–20 years has a significant correlation with the incidence of NPC and calculated as a latent effect [16].
In the distribution of NPC patients based on histopathology, the highest was WHO type III by 18 patients (90%) and followed by WHO type II of 2 patients (10%), while WHO type I was not obtained. The most common type of NPC histopathology in Indonesia is WHO type III. Previous research was performed in Otolaryngology Dr. Soetomo General Hospital also showed the similar result [9]. WHO type III of nasopharyngeal carcinoma is common because in endemic areas it suspected the main cause of NPC is exposure to EBV infection. Nasopharyngeal carcinomas correlated with EBV that undifferentiated carcinoma (WHO type III) and non-keratinizing species (WHO type II).
Nonspecific predominant WHO type I and II of nasopharyngeal carcinoma were often found in adults and rarely in children, whereas WHO type III NPC was reported to occur in children with incident distributions in the second and fifth decades [17]. Nasopharyngeal carcinoma in Indonesia is mostly found in WHO type III [18]. In nasopharyngeal carcinoma, the increasing of intracellular Hsp70 often correlated with the influence of p53 (wild-type). There was a strong positive reciprocity between p53 (wild-type) and intracellular Hsp70. Active p53 (wild-type) proteins enter the nucleus into transcription factors for several genes, including intracellular Hsp70 encoding genes. The isolation of Hsp70 intracell gene promoter with p53 (wild-type) will cause the active transcription process, followed by the translation process. Therefore, the increase of p53 protein (wild-type) will be followed by an increase of intracellular Hsp70 [19]. In addition, stress induced by immunological reactions also increases intracellular Hsp70 by cellular stress responses to the environment that increases Hsf1 expression. Hsf1 transcription factor will drive the Hsp genes to form intracellular Hsp70. So the more stress the NPC cells receive, the higher the Hsp70 expression.
Spearman’s correlation results was obtained p = 0.001 with a correlation coefficient of 0.671. Thus, the increasing intracellular of Hsp70 expression and NPC stage was a significant correlation (p < 0.05). So the hypothesis of this study was proved that there was a positive correlation between intracellular Hsp70 expression (IRS scale) and NPC stage. The higher the intracellular of Hsp70 expression, the higher the stage of the NPC [2]. The similar results were reported that intracellular of Hsp70 was a major factor in NPC growth, invasion and metastasis. In certain cancer the patients treated with chemotherapy or radiotherapy, high levels of intracellular Hsp70 expression and correlated with therapy resistance and poor prognosis [19]. Other studies suggest that cancer-expressed Hsp serves to proliferate tumor cells, differentiation, invasion, metastasis, death, and immune system activation [20].
The other studies have suggested that Hsp70 intranuclear was positively correlated with the classification of T, N, recurrence, metastasis, clinical stage, and histopathologic type. Hsp70 extracellular is known as a facilitator of the immune response that could interact with receptors on antigen cells that cause Hsp70, peptide and antigen reactions. In addition, intracellular of Hsp70 has a strong ability to induce T cell responses. The Hsp70 membrane plays a role in HLA-related immune responses that correlated with antitumor response in NPC cells. While the intranuclear Hsp70 has the opposite function as an effective protein in inhibiting tumor death cell through antiapoptosis pathways and prevent the occurrence of misfolding proteins caused by some stressors such as heat shock, hypoxia, and oxidative stress [7].
The role of intracellular Hsp70 in inhibiting apoptosis was through the extrinsic and intrinsic pathways at multiple levels in the apoptotic pathway. Inhibits the formation of functional apoptosome complexes by interacting directly with Apaf-1 and preventing procaspase gain 9 and 3. Intracellular Hsp70 has an anti-apoptotic role in the caspase-independent pathway by binding to AIF released by mitochondria by limiting translocation to nucleus [21]. Hsp70 intracellular could be translocation from the cytoplasm to the nucleus or nucleolus in the heat of stress and serves as a protection against mediated apoptotic stress and DNA damage, resulting in increased survival of tumor cells [7].
Conclusion
There was a correlation between increased intracellular Hsp70 expression and the stage of patients with Nasopharyngeal Carcinoma.
References
- 1.Ballenger JJ (1994) Karsinoma nasofaring. In: Ballenger JJ (ed) Dalam. Penyakit telinga hidung tenggorok kepala dan leher (alih bahasa). Edisi ke-13, edn. Bina Rupa Aksara, Jakarta
- 2.Peng ZLN, Huang D, Duan C, Li Y, Tang X. N,N′-dinitrosopiperazine-mediated heat-shock protein70-2 expression is involved in metastasis of nasopharyngeal carcinoma. J Pone. 2013;8(5):1–11. doi: 10.1371/journal.pone.0062908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liao Q, Zhao L, Chen X, Deng Y, Ding Y. Serum proteome analysis for profiling protein markers associated with carcinogenesis and lymph node metastasis in nasopharyngeal carcinoma. Clin Exp Metas. 2008;25(4):465–476. doi: 10.1007/s10585-008-9152-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Proctor CJ, Lorimer IA. Modelling the role of the Hsp70/Hsp90 system in the maintenance of protein homeostasis. PLoS ONE. 2011;6(7):e22038. doi: 10.1371/journal.pone.0022038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Srivastava P. Interaction of heat shock protein with peptides and antigen presenting cells: chaperoning of the innate and adaptive immune responses. Annu Rev Immunol. 2002;20:395–425. doi: 10.1146/annurev.immunol.20.100301.064801. [DOI] [PubMed] [Google Scholar]
- 6.Sreedhar CS. Heat shock proteins in the regulation of apoptosis: new strategies in tumor therapy: a comprehensive review. J Pharmther. 2004;101:227–257. doi: 10.1016/j.pharmthera.2003.11.004. [DOI] [PubMed] [Google Scholar]
- 7.Cai MWX, Zhang J, Han H, Liu C, Bei J, et al. Expression of heat shock protein70 in nasopharyngeal carcinomas: different expression patterns correlate with distinct clinical prognosis. J Transl Med. 2012;10(96):1–10. doi: 10.1186/1479-5876-10-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mulyarjo (2002) Diagnosis dan penatalaksanaan karsinoma nasofaring. In: Mulyarjo D, Soedjak S, Wisnubroto, Harmadji SM, Hasanusi S, Artono R (eds) Dalam. Naskah Lengkap Pendidikan Kedokteran Berkelanjutan III Ilmu Kesehatan THT-KL. Surabaya: Laboratorium/SMF Ilmu Penyakit THT-KL FK Unair/RSUD Dr. Soetomo
- 9.Kentjono WA (2010) Karsinoma nasofaring: etiologi, gejala, diagnosis, deteksi dini, terapi dan pencegahan. In: Kentjono WA (ed) Dalam. Pelatihan deteksi dini kanker nasofaring untuk dokter umum di puskesmas. Dept/SMF Ilmu Kesehatan THT-KL FK Unair/RSUD Dr. Soetomo, Surabaya
- 10.Zeng MS. Pathogenesis and etiology of nasopharyngeal carcinoma. Nasopharyngeal Cancer Multidisciplinary Management. Berlin: Springer; 2010. pp. 12–20. [Google Scholar]
- 11.Suwondo S (2012) Validitas hasil pemeriksaan biopsi dengan tuntunan narrow band imaging pada penderita suspek karsinoma nasofaring. Dalam: Karya Akhir untuk memperoleh ijazah keahlian Ilmu Kesehatan Telinga Hidung Tenggorok Bedah Kepala dan Leher. Departemen/SMF Ilmu Kesehatan THT-KL FK UA/RSUD Dr. Soetomo Surabaya
- 12.Harahap MPH. Ekspresi vascular endothelial growth factor pada karsinoma nasofaring. Medan: Universitas Sumatra Utara Repository; 2009. [Google Scholar]
- 13.Chang ET, Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomark Prev. 2006;15(10):1765–1777. doi: 10.1158/1055-9965.EPI-06-0353. [DOI] [PubMed] [Google Scholar]
- 14.Arisakti MA (2013) Hubungan ekspresi vascular endothelial growth factor dengan nodul limfe servikal pada karsinoma nasofaring. Dalam: Karya Akhir untuk memperoleh ijazah keahlian Ilmu Kesehatan Telinga Hidung Tenggorok Bedah Kepala dan Leher, Surabaya
- 15.Ma JCS. The epidemiology of nasopharyngeal cancer. In: Lu JJ, Cooper JS, Lee AWM, editors. Nasopharyngeal Cancer Multidisciplinary Management. Berlin: Springer; 2010. pp. 2–6. [Google Scholar]
- 16.Li WRR, Gao DL, Fitzgibbons ED, Seixos NS, Camp JE, Wernli KJ, Astrakianakis G, Feng Z, Thomas DB, Checkoway H. Occupational risk factors for nasopharyngeal cancer among female textile workers in Shanghai China. Occup Environ Med. 2005;63:39–44. doi: 10.1136/oem.2005.021709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pathmanathan R. Pathology. In: Chong VJH, Tsao SY, editors. Nasopharyngeal carcinoma. Singapore: Armour Publishing; 1997. pp. 6–13. [Google Scholar]
- 18.Adham MKA, Muhtadi AI, Roezin A, Hermani B, Gondhowiardjo S, et al. Nasopharyngeal carcinoma in Indonesia: epidemiology, incidence, signs, and symptoms at presentation. J Cancer Res Ther. 2012;31:185. doi: 10.5732/cjc.011.10328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jones EL, Zhao MJ, Stevenson MA, Calderwood SK. The 70 kilodalton heat shock protein is an inhibitor of apoptosis in prostate cancer. Int J Hyperth. 2004;20(8):835–849. doi: 10.1080/02656730410001721807. [DOI] [PubMed] [Google Scholar]
- 20.Bhatt ANMR, Farooque A, Verma A, Dwarakanath BS. Cancer biomarkers—current perspectives. Indian J Med Res. 2010;132:129–149. [PubMed] [Google Scholar]
- 21.Arya R, Mallik M, Lakhotia SC. Heat shock genes-integrating cell survival and death. J Biosci. 2007;32(3):595–610. doi: 10.1007/s12038-007-0059-3. [DOI] [PubMed] [Google Scholar]