

Abstract
Background
Use of a high-flow nasal cannula (HFNC) reduced postextubation respiratory failure (PERF) and reintubation rate compared to use of a low-flow oxygen system (LFOS) in low-risk patients. However, no obvious conclusion was reached for high-risk patients. Here, we sought to present the current status of HFNC use as adjunctive oxygen therapy in a clinical setting and to elucidate the nature of the protective effect following extubation.
Methods
The medical records of 855 patients who were admitted to the intensive care unit of single university hospital during a period of 5.5 years were analyzed retrospectively, with only 118 patients ultimately included in the present research. The baseline characteristics of these patients and the occurrence of PERF and reintubation along with physiologic changes were analyzed.
Results
Eighty-four patients underwent HFNC, and the remaining 34 patients underwent conventional LFOS after extubation. Physicians preferred HFNC to LFOS in the face of high-risk features including old age, neurologic disease, moderate to severe chronic obstructive pulmonary disease, a long duration of mechanical ventilation, low baseline arterial partial pressure of oxygen to fraction of inspired oxygen ratio, and a high baseline alveolar–arterial oxygen difference. The reintubation rate at 72 hours after extubation was not different (9.5% vs. 8.8%; P=1.000). Hypoxic respiratory failure was slightly higher in the nonreintubation group than in the reintubation group (31.9% vs. 6.7%; P=0.058). Regarding physiologic effects, heart rate was only stabilized after 24 hours of extubation in the HFNC group.
Conclusions
No difference was found in the occurrence of PERF and reintubation between both groups. It is worth noting that similar PERF and reintubation ratios were shown in the HFNC group in those with certain exacerbating risk factors versus not. Caution is needed regarding delayed reintubation in the HFNC group.
Keywords: airway extubation, high-flow nasal cannula, postextubation respiratory failure
INTRODUCTION
Postextubation respiratory failure (PERF) and reintubation are related to ventilator-associated pneumonia, mortality rates, and a longer stay both in the intensive care unit (ICU) and hospital in general [1]. Adjuvant oxygen therapy has commonly been used to prevent these undesirable events. The conventional low-flow oxygen system (LFOS) approach that includes a nasal cannula and facial mask has been used widely. However, more recently, a high-flow oxygen system (HFOS) including noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC) has been preferred due to its physiologic benefits [2-6].
NIV has been used as a substitute for LFOS in acute respiratory failure [2,7]. It has also recently been applied with adjuvant oxygen application after extubation and has shown lower PERF and reintubation rate than LFOS [2,7]. In terms of physiologic aspects, this device is helpful to reduce the arterial partial pressure of carbon dioxide (PaCO2) and increases the arterial partial pressure of oxygen (PaO2) relative to that of LFOS [2,6,7]. However, it cannot be universally used because of the inconvenient interface and its own associated complications (e.g., dyssynchrony, barotrauma, pneumonia) [8].
HFNC is a newly developed device that can supply heated and humidified gas at a relatively constant fraction of inspired oxygen (FiO2, 0.21–1.0) and flow rate (up to 60 L/min) [9]. This device has also demonstrated more physiologic benefits than LFOS. For example, it can wash out PaCO2 in an anatomical dead space and create a positive nasopharyngeal pressure that, in theory, consequently prevents alveolar collapse and increases lung volume [10,11]. Also, contrary to the dry oxygen supply, heated and humidified gas improves mucociliary function [9]. In addition, in comparison with NIV, which requires a sealed interface, HFNC has a more comfortable nasal cannula capable of allowing expectoration of sputum, so it can be used widely among both general and critically ill patients [5,6].
To ensure that these benefits are helpful after extubation, many studies have been conducted but have presented mixed results [4-6,12-16]. In low-risk patients, a large-scale study comparing HFNC with LFOS proved effective, but there was no obvious conclusion in the high-risk group.
Therefore, in this retrospective study, we tried to show the current status of HFNC use in the clinical setting and evaluate the efficacy of HFNC in PERF and reintubation in high-risk patients. Physiologic changes according to time were also analyzed to determine whether the benefit of HFNC plays a physiologic role in postextubation.
MATERIALS AND METHODS
Study Design and Populations
This was a retrospective study conducted in an ICU of a single center at Konyang University Hospital, Daejeon, Korea. The medical records of 855 patients who were admitted to the ICU and received mechanical ventilator therapy between November 2011 and March 2017 were reviewed. Seven hundred thirty-six patients were ultimately removed due to the study exclusion criteria (Figure 1). Patients who had at least one high-risk factor (e.g., age older than 65 years, body mass index higher than 30 kg/m2, Acute Physiologic and Chronic Health Evaluation (APACHE) II score greater than 12 points, duration of mechanical ventilation greater than 7 days, Charlson comorbidity index of 2 points or more, heart failure as a cause of intubation, moderate to severe chronic obstructive pulmonary disease (COPD), failure with first spontaneous breathing trial (SBT) were defined as high-risk patients for PERF and reintubation according to a previous study [6]. One patient who did not have any such risk factors was also excluded (Figure 1). Consequently, 118 patients were included in this study, 84 of whom had undergone HFNC, and the other 34 of whom had undergone conventional LFOS.
Figure 1.
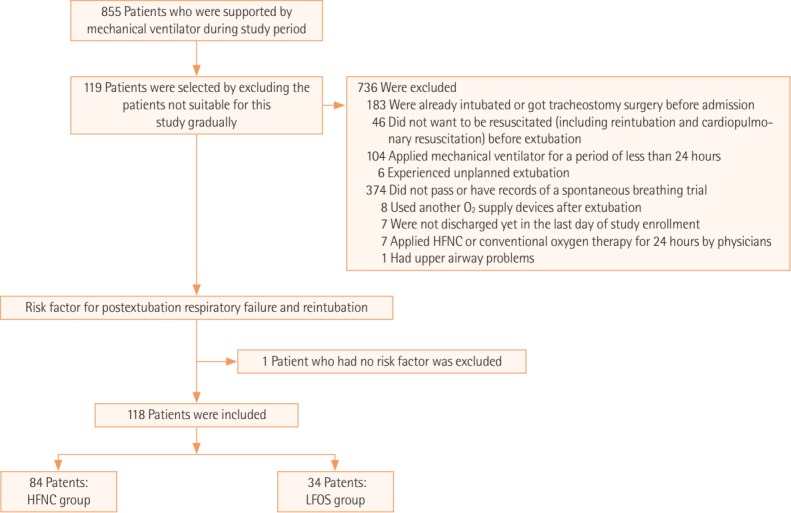
Study design and population. In 855 patients who experienced mechanical ventilator use during the analyzed periods, 737 who matched the exclusion criteria and/or who did not have risk factors were excluded. Finally, 118 patients were included and analyzed retrospectively. HFNC: high-flow nasal cannula; LFOS: low-flow oxygen system.
A physician evaluated the patient status each day and determined the possibility of extubation by awakening and a SBT according to the weaning protocol of the ICU of Konyang University Hospital. After and during the extubation, adjunctive O2 supply (HFNC or LFOS) was provided. HFNC was delivered by the Optiflow system or Airbo-2 (Fisher & Paykel Healthcare, Auckland, New Zealand). The supplied FiO2 and gas flow were operated and controlled by a bedside physician according to the patient’s conditions, respiratory effort, target oxygenation, and arterial blood gas analysis. After extubation, the patient’s condition was evaluated in terms of respiratory discomfort, arterial blood gas, and vital signs. When PERF occurred, reintubation was determined by the bedside physician. This study was approved by the Institutional Review Board of Konyang University Hospital (IRB No. 2017-11-006).
Data Collection
Data were collected from the medical records including the general characteristics of the patients, the cause of respiratory failure, arterial blood gas analysis findings, vital signs before intubation and after extubation, ventilator period, and interval to reintubation. PERF was defined according to three categories: hypercapnic respiratory failure (pH <7.35 and PaCO2 >45 mmHg), hypoxic respiratory failure (PaO2 <60 mmHg), and tachypneic respiratory failure (respiratory rate >35 breaths/min). Reintubation was also classified into three groups: early reintubation (reintubation in 72 hours after extubation), delayed reintubation (reintubation between 72 hours and 168 hours after extubation), and nonreintubation (no occurrence of reintubation up to 168 hours after extubation).
Statistical Analysis
Categorical and noncategorical variables are expressed as number (percentage) and median (25th–75th, interquartile range). Fisher exact test or the chi-square test was used to compare the categorical variables, and the Mann-Whitney U-test was used for comparisons of noncategorical variables. Changes in PaO2/FiO2, PaCO2, respiratory rate, and heart rate according to time were analyzed using the Friedman test. Post-hoc analysis of the Friedman test was conducted using the Wilcoxon rank-sum test when the Freidman test showed significance. A P-value less than 0.05 was considered statically significant. The IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) was used for data analysis.
RESULTS
Baseline Characteristics of the Enrolled Patients
The baseline characteristics of 118 patients suitable for this study are presented in Table 1. The cause of invasive mechanical ventilation and the APACHE II score did not differ between the groups. However, there were differences in underlying disease and high-risk factors. Patients who had more baseline neurologic diseases (32.1% vs. 11.8%, P=0.023), a long duration of mechanical ventilation before extubation (median, 120.3 vs. 81.93 hours; P=0.012), and longer hospital stay before extubation (median, 7.5 vs. 4.5 days; P=0.005) were more likely to be supported by HFNC. The HFNC group also showed a lower baseline PaO2/FiO2 versus the LFOS group (130.78 vs. 255.71 mmHg, P=0.001) and a higher baseline alveolar–arterial oxygen difference (183.25 vs. 56.12, P=0.003). Patients with certain high-risk factors such as age older than 65 years (77.4% vs. 58.8%; P=0.042) and moderate to severe COPD (19.0% vs. 0%; P=0.005) were more frequently found in the HFNC group.
Table 1.
Baseline characteristics of analyzed patients before intubation
| Characteristics | HFNC (n=84) | LFOS (n=34) | P-value |
|---|---|---|---|
| Male sex | 60 (71.4) | 20 (58.8) | 0.184 |
| Age (yr) | 73.0 (66.0–80.0) | 71.00 (55.75–81.25) | 0.454 |
| Height (cm) | 163.5 (158.0–170.0) | 155.50 (160.00–169.50) | 0.248 |
| Body weight (kg) | 56.65 (50.0–68.0) | 58.00 (52.00–65.00) | 0.983 |
| Body mass index (kg/m2) | 22.0 (18.8–24.5) | 23.11 (19.44–24.92) | 0.703 |
| Underlying disease | |||
| Diabetes mellitus | 19 (22.6) | 6 (17.6) | 0.549 |
| Hypertension | 31 (36.9) | 12 (35.3) | 0.869 |
| Malignant disease | 10 (11.9) | 4 (11.8) | 1.000a |
| Chronic respiratory disease | 47 (56.0) | 15 (44.1) | 0.244 |
| Chronic heart disease | 22 (26.2) | 7 (20.6) | 0.522a |
| Chronic liver disease | 1 (1.2) | 0 | 1.000a |
| Chronic renal disease | 11 (13.1) | 3 (8.8) | 0.755a |
| Neurologic disease | 27 (32.1) | 4 (11.8) | 0.023 |
| Cause of mechanical ventilation | |||
| Pneumonia | 45 (53.6) | 19 (55.9) | 0.819 |
| Airway disease | 13 (15.5) | 3 (8.8) | 0.119 |
| Hemoptysis | 3 (3.6) | 1 (2.9) | 1.000a |
| Drug intoxication | 14 (16.7) | 10 (29.4) | 0.119 |
| Post operation | 2 (2.4) | 0 | 1.000a |
| Heat failure | 3 (3.6) | 0 | 0.556a |
| Others | 4 (4.8) | 1 (2.9) | 1.000a |
| Type of respiratory failure at intubationb | |||
| Tachypneic respiratory failure | 6 (7.1) | 2 (5.9) | 1.000a |
| Hypercapnic respiratory failure | 38 (45.2) | 12 (35.3) | 0.322 |
| Hypoxic respiratory failure | 23 (27.4) | 6 (17.6) | 0.266a |
| Othersc | 22 (26.2) | 14 (41.2) | 0.109 |
| Severity index | |||
| APACHE II score at ICU admission | 22.0 (18.00–25.00) | 22.00 (19.00–25.25) | 0.466 |
| APACHE II score at extubation | 17.0 (14.0–19.0) | 16.50 (14.00–19.00) | 0.466 |
| Vital sign and arterial blood gas before intubation | |||
| Heart rate | 100.00 (85.00–120.00) | 107.50 (85.75–121.00) | 0.861 |
| Respiratory rate | 22.00 (18.00–27.50) | 22.00 (18.75–27.25) | 0.696 |
| PaCO2 (mmHg) | 41.75 (31.72–60.97) | 39.15 (32.15–53.55) | 0.671 |
| PaO2/FiO2 (mmHg) | 130.78 (83.76–259.29) | 255.71 (200.05–320.44) | 0.001 |
| (A–a) DO2 | 183.25 (50.71–412.68) | 56.12 (21.37–166.99) | 0.003 |
| Vital sign and arterial blood gas before extubation | |||
| Heart rate on ventilation | 84.50 (74.25–101.75) | 85.00 (68.00–90.25) | 0.198 |
| Respiratory rate on ventilation | 18.00 (16.00–21.00) | 17.00 (15.00–20.00) | 0.155 |
| PaCO2 on ventilation (mmHg) | 34.75 (30.05–40.35) | 34.40 (28.70–36.15) | 0.051 |
| PaO2/FiO2 on ventilation (mmHg) | 288.00 (208.31–363.81) | 333.75 (279.37–379.37) | 0.069 |
| (A-a) DO2 at spontaneous breathing trial | 138.71 (95.60–167.74) | 130.20 (88.29–130.20) | 0.478 |
| High risk patient | |||
| Age older than 65 years | 65 (77.4) | 20 (58.8) | 0.042 |
| Body mass index higher than 30 kg/m2 | 7 (8.3) | 2 (5.9) | 1.000a |
| Ventilator duration more than 7 days | 30 (35.7) | 7 (20.6) | 0.109 |
| Charlson comorbidity index of 2 or more | 33 (39.3) | 7 (20.6) | 0.052 |
| APACHE II score of more than 12 | 80 (95.2) | 32 (94.1) | 0.802 |
| Heart failure as a cause of intubation | 3 (3.6) | 0 | 0.556a |
| Moderate to severe COPD | 16 (19.0) | 0 | 0.005a |
| Failure with first SBT trial | 52 (61.9) | 17 (50.0) | 0.235 |
| Duration of mechanical ventilation before extubation (hr) | 120.3 (74.9–213.8) | 81.93 (47.45–139.09) | 0.012 |
| Hospital day before extubation trial (day) | 7.5 (4.00–10.75) | 4.5 (3.00–7.25) | 0.005 |
Values are presented as number (%) or median (interquartile range).
HFNC: high-flow nasal cannula; LFOS: low-flow oxygen system; APACHE: Acute Physiologic and Chronic Health Evaluation; ICU: intensive care unit; PaCO2: arterial partial pressure of carbon dioxide; PaO2/FiO2: ratio of arterial oxygen partial pressure to fractional inspired oxygen; (A–a) DO2: alveolar–arterial oxygen difference; COPD: chronic obstructive pulmonary disease; SBT: spontaneous breathing trial.
Fisher exact test;
Type of respiratory failure can be classified according to each group, if it satisfies both criteria;
Respiratory failure that was not satisfy each criterion.
The baseline laboratory findings in the two groups were also analyzed (Supplementary Table 1). In the baseline laboratory findings before intubation, a high neutrophil fraction (80.50% vs. 73.70%, P=0.045), high potassium level (4.15 vs. 3.76 mmol/L, P=0.003), and low calcium concentration (8.44 vs. 8.83 mmol/L, P=0.032) were shown in the HFNC group. Low albumin at extubation was also observed in the HFNC group (2.77 vs. 3.00 g/dl, P=0.010).
Results of Extubation: PERF and Reintubation
The occurrences of reintubation and PERF were analyzed (Table 2). The early reintubation rate was eight of 84 (9.5%) and three of 34 (8.8%), respectively (P=1.000). The occurrences of all types of respiratory failures in both groups were 21 of 84 (25.0%) and 11 of 34 (32.4%), respectively (P=0.416). Subanalysis according to subtype of respiratory failure also did not show any statistical difference (Table 2). Hypoxic and hypercapnic respiratory failure occurred in seven of 84 (8.3%) and two of 84 (2.4%) patients in the HFNC group, respectively, and in four of 34 (11.8%) and three of 34 (8.8%) patients in the LFOS group.
Table 2.
Clinical outcome after extubation between two groups
| Variable | HFNC (n=84) | LFOS (n=34) | χ2 | P-value |
|---|---|---|---|---|
| Reintubation | ||||
| Early reintubation (in 72 hr) | 8 (9.5) | 3 (8.8) | - | 1.000a |
| Time to reintubation | 10.41 (1.51–62.37) | 5.00 (4.17–43.85) | 0.838b | |
| Reintubation in 168 hr | 15 (17.9) | 3 (8.8) | 1.528 | 0.216 |
| Time to reintubation | 69.00 (2.58–100.82) | 5.00 (4.17–43.85) | 0.260b | |
| Delayed reintubation (72–168 hr) | 7/76c (9.2) | 0/31c | - | 0.105a |
| Postextubation respiratory failure | ||||
| Hypoxia | 7 (8.3) | 4 (11.8) | - | 0.727a |
| Hypercapnia | 2 (2.4) | 3 (8.8) | - | 0.143a |
| Tachypnea | 14 (16.7) | 6 (17.6) | 0.017 | 0.898 |
| All types of respiratory failure | 21 (25.0) | 11 (32.4) | 0.662 | 0.416 |
| Clinical outcome | ||||
| Tracheostomy | 5 (6.0) | 1 (2.9) | - | 0.672a |
| In hospital mortality | 12 (14.3) | 3 (8.8) | - | 0.549a |
| Hospital day | 27.5 (16.0–49.7) | 14.50 (9.0–31.0) | - | 0.001b |
Values are presented as number (%) or median (interquartile range).
HFNC: high-flow nasal cannula; LFOS: low-flow oxygen system.
Fisher exact test;
Mann-Whitney U-test;
Number/total number.
In the additional analysis carried out during 168 hours, seven patients in the HFNC group had progressed to reintubation but showed no statistical difference in comparison with the LFOS group. The delayed reintubation rate was seven of 76 (9.2%) and none of 31, respectively (P=0.105). Occurrence of any type of respiratory failure in 48 hours in those who received HFNC was higher in the early reintubation group (6/8, 75.0%) and delayed reintubation group (4/7, 57.1%) versus the nonreintubation group (11/69, 15.9%; P=0.000). Time to reintubation, in-hospital mortality rate, and tracheostomy rate did not show a statistical difference between the two groups (Table 2). The hospital stay of the HFNC group was longer than that of the LFOS group (27.5 vs. 14.50 days; P=0.001).
Physiologic Effects of HFNC after Extubation
To elucidate the physiologic effects of HFNC on heart rate, respiratory rate, PaO2/FiO2, and PaCO2 compared with LFOS, patient vital signs and arterial blood gas after extubation were analyzed according to time. Prior to extubation, baseline heart rate, respiratory rate, PaCO2, and PaO2/FiO2 were not significantly different between the groups (Figure 2, Supplementary Table 2).
Figure 2.

Physiologic parameters after extubation. (A) Heart rate. (B) Respiratory rate. (C) Arterial partial pressure of carbon dioxide (PaCO2). (D) The ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2). LFOS: low-flow oxygen system; HFNC: high-flow nasal cannula; SBT: spontaneous breathing trial. aStatically significant difference between SBTs at each time after extubation; bStatically significant difference between HFNC and LFOS at the same time.
Heart rate during the SBT and at 1 hour after extubation was higher in the HFNC group (Mann-Whitney U-test, P=0.014 in SBT and P=0.018 at 1 hour after extubation extubation) . Compared with heart rate in SBT, the heart rate stabilized after 24 hours in the HFNC group (Friedman test, χ2= 27.033, P=0.000; Mann-Whitney U-test, P=0.001 at 24 hours after extubation and P=0.001 at 48 hours after extubation). No statistically significant difference was found in respiratory rate, PaCO2, and PaO2/FiO2 between each time compared with the parameters during the SPT.
Predictors for Reintubation and Delayed Reintubation in the HFNC Group
Variables including underlying disease, cause of mechanical ventilation, and high-risk factors were analyzed to determine the risk factors that influence reintubations (Table 3). No risk factors were found except longer hospital stay before extubation (9.00 [8.00–14.00] vs. 6.00 [4.00–10.00], P=0.036). There was no difference in the type of respiratory failure at intubation in the HFNC group. Although there was no significant difference, hypoxemic respiratory failure was more frequently found in the nonreintubation group versus the reintubation group (22/69 [31.9%] vs. 1/15 [6.7%], P=0.058).
Table 3.
Predictor for reintubation in HFNC group
| Characteristics | Non-reintubation (n=69) | Reintubation (n=15) | P-value |
|---|---|---|---|
| Male sex | 49 (71.0) | 11 (73.3) | 1.000a |
| Age (yr) | 74.0 (65.50–80.50) | 72.00 (67.00–74.00) | 0.245 |
| Height (cm) | 162.0 (158.0–170.0) | 164.50 (160.00–165.00) | 0.711 |
| Body weight (kg) | 58.0 (50.0–70.0) | 55.30 (50.00–60.00) | 0.656 |
| Body mass index (kg/m2) | 22.7 (18.7–24.9) | 22.03 (19.59–23.44) | 0.717 |
| Underlying disease | |||
| Diabetes mellitus | 15 (21.7) | 4 (26.7) | 0.736a |
| Hypertension | 25 (36.2) | 6 (40.0) | 0.784 |
| Malignant disease | 6 (8.7) | 4 (26.7) | 0.073a |
| Chronic respiratory disease | 40 (58.0) | 7 (46.7) | 0.424 |
| Chronic heart disease | 18 (26.1) | 4 (26.7) | 1.000a |
| Chronic liver disease | 1 (1.4) | 0 | 1.000a |
| Chronic renal disease | 7 (10.1) | 4 (26.7) | 0.102a |
| Neurologic disease | 20 (29.0) | 7 (46.7) | 0.226a |
| Cause of mechanical ventilation | |||
| Pneumonia | 36 (52.2) | 9 (60.0) | 0.776 |
| Airway disease | 9 (13.0) | 4 (26.7) | 0.235a |
| Hemoptysis | 3 (4.3) | 0 | 1.000a |
| Drug intoxication | 13 (18.8) | 1 (6.7) | 0.447a |
| Post operation | 2 (2.9) | 0 | 1.000a |
| Heat failure | 3 (4.3) | 0 | 1.000a |
| Others | 3 (4.3) | 1 (6.7) | 0.552a |
| Type of respiratory failure at intubationb | |||
| Tachypneic respiratory failure | 5 (7.2) | 1 (6.7) | 1.000a |
| Hypercapnic respiratory failure | 31 (44.9) | 7 (46.7) | 0.902 |
| Hypoxic respiratory failure | 22 (31.9) | 1 (6.7) | 0.058a |
| Othersc | 15 (21.7) | 7 (46.7) | 0.058a |
| Severity index | |||
| APACHE II score at ICU admission | 22.0 (17.50–25.00) | 22.00 (19.00–25.00) | 0.516 |
| APACHE II score at extubation | 17.0 (15.0–19.0) | 16.00 (13.00–22.00) | 0.541 |
| Vital sign and arterial blood gas before intubation | |||
| Heart rate | 100.00 (84.00–124.50) | 101.00 (88.00–118.00) | 0.820 |
| Respiratory rate | 22.00 (18.00–26.00) | 22.00 (18.00–28.00) | 0.977 |
| PaCO2 (mmHg) | 44.90 (30.50–60.95) | 38.60 (32.00–86.00) | 0.356 |
| PaO2/FiO2 (mmHg) | 131.97 (86.90–256.19) | 120.86 (80.12–291.90) | 0.907 |
| (A–a) DO2 | 186.97 (48.71–411.96) | 179.53 (50.43- 465.58) | 0.532 |
| Vital sign and arterial blood gas before extubation | |||
| Heart rate on ventilation | 82.00 (73.50–101.00) | 87.00 (76.00–109.00) | 0.272 |
| Respiratory rate on ventilation | 18.00 (16.00–21.00) | 18.00 (15.00–20.00) | 0.366 |
| PaCO2 on ventilation (mmHg) | 34.60 (30.50–40.30) | 35.40 (27.70–46.80) | 0.717 |
| PaO2/FiO2 on ventilation (mmHg) | 286.75 (215.62–361.00) | 321.00 (165.75–400.00) | 0.939 |
| (A–a) DO2 at spontaneous breathing trial | 143.62 (110.02–166.10) | 123.42 (92.25–178.92) | 0.640 |
| High risk patient | |||
| Age older than 65 years | 53 (76.8) | 12 (80.0) | 1.000a |
| Body mass index higher than 30 kg/m2 | 6 (8.7) | 1 (6.7) | 1.000a |
| Ventilator duration more than 7 days | 22 (31.9) | 8 (53.3) | 0.116 |
| Charlson comorbidity index of 2 or more | 26 (37.7) | 7 (46.7) | 0.518a |
| APACHE II score of more than 12 | 66 (95.7) | 14 (93.3) | 0.552a |
| Heart failure as a cause of intubation | 3 (4.3) | 0 | 1.000a |
| Moderate to severe COPD | 15 (21.7) | 1 (6.7) | 0.282a |
| Failure with first SBT trial | 40 (58.0) | 12 (80.0) | 0.111 |
| Duration of mechanical ventilation before extubation (hr) | 117.15 (70.71–210.29) | 181.46 (82.83–273.66) | 0.197 |
| Hospital day before extubation trial (day) | 6.00 (4.00–10.00) | 9.00 (8.00–14.00) | 0.036 |
Values are presented as number (%) or median (interquartile range).
HFNC: high-flow nasal cannula; APACHE: Acute Physiologic and Chronic Health Evaluation; ICU: intensive care unit; PaCO2: arterial partial pressure of carbon dioxide; PaO2/FiO2: ratio of arterial oxygen partial pressure to fractional inspired oxygen; (A–a) DO2: alveolar–arterial oxygen difference; COPD: chronic obstructive pulmonary disease; SBT: spontaneous breathing trial.
Fisher exact test;
Type of respiratory failure can be classified according to each group, if it satisfies both criteria;
Respiratory failure that was not satisfy each criterion.
To find the cause of delayed reintubation in the HFNC group, multiple variables were analyzed between the delayed reintubation group and nonreintubation group (Supplementary Table 3). There was no difference among these groups except more frequent basement renal disease (3/7 [42.9%] vs. 7/69 [10.1%], P=0.044) in the delayed-reintubation group.
DISCUSSION
An obvious benefit of HFNC in the context of the prevention of PERF and reintubation versus in the LFOS group at 72 hours after extubation was not observed in high-risk patients. Regarding physiologic aspects, HFNC might have helped to stabilize the heart rate, but no effect on stabilization of the respiratory rate, PaCO2, and PaO2/FiO2 was noted.
Contrary to the recent meta-analysis and several other articles that reported the superiority of HFNC over LFOS after extubation, in this study, no significant benefits were observed in preventing PERF and reintubation [4,17,18]. However, the results of previous studies cannot be generalized due to the limited constitution of study populations (Table 4) [4,17,18].
Table 4.
Literature review for previous studies comparing HFNC to other oxygen delivery devices after extubation
| Study | Study’s characteristics | Patient’s characteristics | Control | Reintubation | PERF | Physiologic aspect |
|---|---|---|---|---|---|---|
| Futier et al. [13] | Prospective RCT | Surgical patient after major abdominal surgery | LFOS | No difference | No difference | - |
| Dhillon et al. [16] | Retrospective | Critically ill surgical patient | LFOS | No differencea | - | - |
| Yu et al. [14] | Prospective RCT | Surgical patient after thoracoscopic lobectomy | LFOS | Less reintubation in HFNC | Less hypoxemic respiratory failure in HFNC | Better oxygenation, reduction of respiratory rate in HFNC |
| Hernández et al. [6] | Prospective RCT | High risk | NIV | Not inferior in HFNC | Not inferior in HFNC | No difference |
| Yoo et al. [5] | Retrospective | Mixed risk | NIV | No difference | - | - |
| Maggiore et al. [3] | Prospective RCT | Mixed risk | LFOSb | Less reintubation in HFNC | Less PERF in HFNC | Better oxygenation, reduction of respiratory rate in HFNC |
| Hernández et al. [4] | Prospective RCT | Low risk | LFOS | Less reintubation in HFNC | Less PERF in HFNC | No difference |
| Fernandez et al. [12] | Prospective RCT | Mixed risk, but include only hypercapnic patient | LFOS | No difference | No difference | - |
| Song et al. [15] | Prospective RCT | Mixed risk | LFOS | No difference | - | Better oxygenation, reduction of respiratory rate in HFNC |
| This study | Retrospective | High risk | LFOS | No difference | No difference | No differencec |
HFNC: high-flow nasal cannula; PERF: postextubation respiratory failure; RCT: randomized controlled trial; LFOS: low-flow oxygen system; NIV: noninvasive ventilation.
In multivariable analysis, HFNC is associated with a lower risk of reintubation;
This study only used the venturi mask as LFOS;
In this study, HFNC shows stabilization of the heart rate after extubation.
In postsurgical patients, HFNC has continued to show a benefit over LFOS after extubation [13,14,16]. However, it is not generalized to nonsurgical patients. Only three previous studies directly compared HFNC and LFOS in medical patients and presented confusing results (Table 4) [4,12,15]. Hernández et al. [4] showed a low PERF ratio and low reintubation rate in HFNC versus conventional LFOS in low-risk patients after extubation. However, this group did not compare the HFNC to LFOS in high-risk patients directly. Fernandez et al. [12] studied the efficacy of HFNC in high-risk patients who suffered from nonhypercapnic respiratory failure versus conventional LFOS but reported inconclusive results due to low recruitment. The other study conducted by Song et al. [15] in acute respiratory failure patients with mixed risk also failed to prove the protection of reintubation. In conclusion, according to the literature review, HFNC after extubation as adjunctive oxygen therapy in low-risk or postsurgical patients might be effective, but there is no conclusion regarding high-risk patients.
In our study, physicians preferred HFNC over LFOS in high-risk patients who were older than 65 years and had moderate to severe COPD and/or neurologic disease, which are wellknown risk factors for reintubation [19]. HFNC is also more likely to be applied in patients with a high baseline alveolar–arterial oxygen difference that implies impaired gas exchange and in those with longer ventilator duration before extubation, which is a risk factor for reintubation [1,20]. For these reasons, it is worth noting that similar PERF and reintubation ratios were shown in the HFNC patients who had more risk factors.
In the previous two studies, HFNC stabilized the respiratory rate and improved the oxygenation [15,21,22]. In the previous study by Frat et al. [22], in acute respiratory failure, HFNC is related to reduced mortality and low reintubation in severe hypoxemia patients (PaO2/FiO2 <200 mmHg) compared with standard oxygen and NIV. The authors [22] insisted that this effect originates from a reduction in work of breathing and improvement of gas exchange. However, these effects were not found in this study. The initial lower PaO2/FiO2 and high alveolar–arterial oxygen gradient in the HFNC group could explain these unfavorable results. Similar to previous studies, no reduction of PaCO2 was observed here [4,12,15]. This result differs from that in some other reports, which showed reduction in vitro and in other clinical situations, except for extubation. Therefore, PaCO2 reduction may not be expected generally in the use of HFNC after extubation.
In this study, patients who received HFNC had lower PaO2/FiO2 versus those who received LFOS. Although not statistically significant, considering the more frequent preintubation hypoxemic respiratory failure in the nonreintubation group, which was expected to be improved by HFNC and have no effect on respiratory rate and PaCO2, HFNC may play a role more in in nonhypercapnic respiratory failure than ventilatory failure after extubation.
To determine who will obtain a benefit from HFNC after extubation in high-risk patients, a subanalysis was performed. Longer hospital stay before extubation, which reflects the possibility of poor patient condition, might be linked with a higher risk for reintubation.
Although no statistical difference was shown in time to reintubation and time to respiratory failure, it is worth noting that a tendency of delayed reintubation was shown in the HFNC group like in previous research [5,12]. The reason for the tendency of delayed reintubation in our study is not clear. In subanalysis, when considering the risk factors for delayed reintubation, there was no significant difference except in basement renal disease between the delayed-reintubation group and non-reintubation group. Considering that more than 50% of patients in the delayed-reintubation group already suffered respiratory failure within 48 hours, there is a possibility of a physician’s hesitancy to complete early reintubation due to an expectation about HFNC’s stabilizing effect. Also, there is the possibility of HFNC hiding the aggravation of PERF, resulting in erroneous determination of extubation success. Further evaluation is needed to clarify this undesirable complication.
Our study has several strengths. First, compared with the previous studies that only included limited characteristics [4,12], the patients in this study had more diverse characteristics including hypercapnic respiratory failure. Second, in this study, we provided information about the physiologic changes and serial arterial blood gas analysis findings after extubation with a longer duration than in the previous studies. Therefore, we can better comment on the long-term effects of HFNC after extubation. Third, due to the nature of retrospective studies, this study reflects a real-world situation without artificial interventions.
This study also has some limitations. First, due to the study design (single-center, retrospective investigation), confounding factors and bias may be present. Furthermore, important information including parameters of the mechanical ventilator that were unrecorded in the medical record could not be analyzed. For this reason, the well-known predictors for PERF and reintubation including rapid shallow breathing index, maximal inspiratory pressure, and modified burns wean assessment program outcomes could not be analyzed [23]. Second, we only compared HFNC to LFOS and did not compare it to NIV. To clarify the benefit of HFNC on postextubation, especially in high-risk patients, additional study including NIV is necessary. Third, the number of study participants and reintubation rates are too small to show statistical significance. The findings on who receives benefit from HFNC and who will progress to delayed reintubation cannot be deemed statistically significant due to the small number of study participants.
In conclusion, no difference was observed in the PERF and reintubation ratios between the HFNC and LFOS groups at 72 hours after extubation. It is better to understand HFNC after extubation does not work than to do further prospective randomized controlled studies to clarify this efficacy and concern in high-risk patients. Caution is needed due to the tendency of delayed reintubation of the HFNC group. In terms of physiologic aspects, HFNC after extubation might be linked to stabilization of the heart rate after extubation.
HIGHLIGHTS
▪ In high-risk patients, no difference was found in occurrence of postextubation respiratory failure (PERF) and reintubation between the high-flow nasal cannula (HFNC) and low-flow oxygen system groups.
▪ Physicians preferred applying HFNC in riskier patients. It is worth noting that similar PERF and reintubation ratios were shown in the HFNC patients with more risk factors versus less.
▪ When implementing HFNC in high-risk patients, caution is needed due to the possibility of delayed reintubation.
Footnotes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: SJK. Data curation: ML. Formal analysis: ML. Methodology: SJK. Visualization: ML. Writing - original draft: ML. Writing - review & editing: JHK, IBJ, JWS, MJN, SJK.
SUPPLEMENTARY MATERIALS
The online-only supplement data are available with this article online: https://doi.org/10.4266/acc.2018.00311.
REFERENCES
- 1.Epstein SK. Decision to extubate. Intensive Care Med. 2002;28:535–46. doi: 10.1007/s00134-002-1268-8. [DOI] [PubMed] [Google Scholar]
- 2.Nava S, Gregoretti C, Fanfulla F, Squadrone E, Grassi M, Carlucci A, et al. Noninvasive ventilation to prevent respiratory failure after extubation in high-risk patients. Crit Care Med. 2005;33:2465–70. doi: 10.1097/01.ccm.0000186416.44752.72. [DOI] [PubMed] [Google Scholar]
- 3.Maggiore SM, Idone FA, Vaschetto R, Festa R, Cataldo A, Antonicelli F, et al. Nasal high-flow versus venturi mask oxygen therapy after extubation: effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med. 2014;190:282–8. doi: 10.1164/rccm.201402-0364OC. [DOI] [PubMed] [Google Scholar]
- 4.Hernández G, Vaquero C, González P, Subira C, Frutos-Vivar F, Rialp G, et al. Effect of postextubation high-flow nasal cannula vs conventional oxygen therapy on reintubation in lowrisk patients: a randomized clinical trial. JAMA. 2016;315:1354–61. doi: 10.1001/jama.2016.2711. [DOI] [PubMed] [Google Scholar]
- 5.Yoo JW, Synn A, Huh JW, Hong SB, Koh Y, Lim CM. Clinical efficacy of high-flow nasal cannula compared to noninvasive ventilation in patients with post-extubation respiratory failure. Korean J Intern Med. 2016;31:82–8. doi: 10.3904/kjim.2016.31.1.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hernández G, Vaquero C, Colinas L, Cuena R, González P, Canabal A, et al. Effect of postextubation high-flow nasal cannula vs noninvasive ventilation on reintubation and postextubation respiratory failure in high-risk patients: a randomized clinical trial. JAMA. 2016;316:1565–74. doi: 10.1001/jama.2016.14194. [DOI] [PubMed] [Google Scholar]
- 7.Ornico SR, Lobo SM, Sanches HS, Deberaldini M, Tófoli LT, Vidal AM, et al. Noninvasive ventilation immediately after extubation improves weaning outcome after acute respiratory failure: a randomized controlled trial. Crit Care. 2013;17:R39. doi: 10.1186/cc12549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carron M, Freo U, BaHammam AS, Dellweg D, Guarracino F, Cosentini R, et al. Complications of non-invasive ventilation techniques: a comprehensive qualitative review of randomized trials. Br J Anaesth. 2013;110:896–914. doi: 10.1093/bja/aet070. [DOI] [PubMed] [Google Scholar]
- 9.Nishimura M. High-flow nasal cannula oxygen therapy in adults. J Intensive Care. 2015;3:15. doi: 10.1186/s40560-015-0084-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fricke K, Tatkov S, Domanski U, Franke KJ, Nilius G, Schneider H. Nasal high flow reduces hypercapnia by clearance of anatomical dead space in a COPD patient. Respir Med Case Rep. 2016;19:115–7. doi: 10.1016/j.rmcr.2016.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Frizzola M, Miller TL, Rodriguez ME, Zhu Y, Rojas J, Hesek A, et al. High-flow nasal cannula: impact on oxygenation and ventilation in an acute lung injury model. Pediatr Pulmonol. 2011;46:67–74. doi: 10.1002/ppul.21326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fernandez R, Subira C, Frutos-Vivar F, Rialp G, Laborda C, Masclans JR, et al. High-flow nasal cannula to prevent postextubation respiratory failure in high-risk non-hypercapnic patients: a randomized multicenter trial. Ann Intensive Care. 2017;7:47. doi: 10.1186/s13613-017-0270-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Futier E, Paugam-Burtz C, Godet T, Khoy-Ear L, Rozencwajg S, Delay JM, et al. Effect of early postextubation high-flow nasal cannula vs conventional oxygen therapy on hypoxaemia in patients after major abdominal surgery: a French multicentre randomised controlled trial (OPERA) Intensive Care Med. 2016;42:1888–98. doi: 10.1007/s00134-016-4594-y. [DOI] [PubMed] [Google Scholar]
- 14.Yu Y, Qian X, Liu C, Zhu C. Effect of high-flow nasal cannula versus conventional oxygen therapy for patients with thoracoscopic lobectomy after extubation. Can Respir J. 2017;2017:7894631. doi: 10.1155/2017/7894631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Song HZ, Gu JX, Xiu HQ, Cui W, Zhang GS. The value of highflow nasal cannula oxygen therapy after extubation in patients with acute respiratory failure. Clinics. 2017;72:562–7. doi: 10.6061/clinics/2017(09)07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dhillon NK, Smith EJT, Ko A, Harada MY, Polevoi D, Liang R, et al. Extubation to high-flow nasal cannula in critically ill surgical patients. J Surg Res. 2017;217:258–64. doi: 10.1016/j.jss.2017.06.026. [DOI] [PubMed] [Google Scholar]
- 17.Huang HW, Sun XM, Shi ZH, Chen GQ, Chen L, Friedrich JO, et al. Effect of high-flow nasal cannula oxygen therapy versus conventional oxygen therapy and noninvasive ventilation on reintubation rate in adult patients after extubation: a systematic review and meta-analysis of randomized controlled trials. J Intensive Care Med. 2018;33:609–23. doi: 10.1177/0885066617705118. [DOI] [PubMed] [Google Scholar]
- 18.Ni YN, Luo J, Yu H, Liu D, Liang BM, Yao R, et al. Can high-flow nasal cannula reduce the rate of reintubation in adult patients after extubation? A meta-analysis. BMC Pulm Med. 2017;17:142. doi: 10.1186/s12890-017-0491-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med. 1998;158:1855–62. doi: 10.1164/ajrccm.158.6.9712135. [DOI] [PubMed] [Google Scholar]
- 20.Lee KH, Hui KP, Chan TB, Tan WC, Lim TK. Rapid shallow breathing (frequency-tidal volume ratio) did not predict extubation outcome. Chest. 1994;105:540–3. doi: 10.1378/chest.105.2.540. [DOI] [PubMed] [Google Scholar]
- 21.Rittayamai N, Tscheikuna J, Rujiwit P. High-flow nasal cannula versus conventional oxygen therapy after endotracheal extubation: a randomized crossover physiologic study. Respir Care. 2014;59:485–90. doi: 10.4187/respcare.02397. [DOI] [PubMed] [Google Scholar]
- 22.Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372:2185–96. doi: 10.1056/NEJMoa1503326. [DOI] [PubMed] [Google Scholar]
- 23.Jeong ES, Lee K. Clinical application of modified burns wean assessment program scores at first spontaneous breathing trial in weaning patients from mechanical ventilation. Acute Crit Care. 2018;33:260–8. doi: 10.4266/acc.2018.00276. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.