

Abstract
Background
Biliary intraepithelial neoplasia (BilIN) is often distinguished by what it is not: the precancerous lesions are not mass-forming, are not the cause of bile duct obstruction, and are small enough (less than 5 mm long) to evade detection by the naked eye. Here, we describe an atypical case of BilIN resembling cholangiocarcinoma (CC) that was large enough to be identified by diagnostic imaging and presented with obstructive jaundice caused by a hematoma in the common bile duct (CBD).
Case presentation
A 64-year-old man presented to our hospital with upper abdominal pain and anorexia. Initial laboratory examinations revealed increased total bilirubin and a computed tomography (CT) scan revealed a dilated CBD. Gastroenterologists performed an endoscopic sphincterotomy (EST), which revealed that the cause of obstructive jaundice was a hematoma in the CBD. Enhanced CT scan and magnetic resonance cholangiopancreatography (MRCP) performed after the hematoma was drained showed improved dilation of the CBD and an enhanced wall thickness of bile duct measuring 25 × 10 mm at the union of the cystic and common hepatic ducts. A cholangioscope detected an elevated tumor covered by sludge in the CBD, and we performed an extrahepatic bile duct resection and cholecystectomy. The postoperative course was uneventful and the pathological examination of the resected tumor revealed that although the ulcerated lesion had inflammatory granulation tissue, it did not contain the components of invasive carcinoma. Many consecutive intraepithelial micropapillary lesions spread around the ulcerated lesion, and the epithelial cells showed an increased nucleus-to-cytoplasm ratio, nuclear hyperchromasia, and architectural atypia. The pathological diagnosis was BilIN-1 to -2. Immunohistochemical staining showed that S100P was slightly expressed and MUC5AC was positive, while MUC1 was negative and p53 was not overexpressed.
Conclusion
We experienced an atypical case of BilIN mimicking CC that presented with obstructive jaundice caused by a hematoma in the CBD. Our case suggested that the occurrence of BilIN can be triggered by factors other than inflammation, and can grow to a size large enough to be detected by image analyses.
Keywords: Biliary intraepithelial neoplasia (BilIN), Cholangiocarcinoma, Bile duct
Background
Cholangiocarcinoma (CC) is the second most common primary liver cancer and carries a high post-resection morbidity and mortality rate [1, 2]. Most cases of CC are detected at advanced stages as patients are usually symptom-free until the disease progresses, so the outcome of CC is generally very poor [1]. To improve this outcome, it is important to be familiar with precancerous lesions for cancer therapy. The precursor lesions of carcinoma have been advocated as adenoma in the gastrointestinal tract, intraepithelial neoplasia in uterine cervical cancer, and leukoplakia in oral cancer [3, 4]. Biliary intraepithelial neoplasia (BilIN) has been described in the World Health Organization 2010 gastrointestinal tumor classification as one of the precursor lesions of CC along with intraductal papillary neoplasm (IPNB), mucinous cystic neoplasm (MCN), and adenoma [5–7]. BilIN usually occurs in the intrahepatic bile duct and occasionally in the extrahepatic bile duct [8, 9]. Its precancerous lesions are less than 5 mm long, do not form a mass, and do not cause a bile duct obstruction [10, 11]. Because of this, detection by image analysis is usually impossible, and the diagnosis entirely depends on pathological examination [12]. Most tumors in the bile duct that are detectable by macroscopic or radiological examinations contain a malignant component, so the typical morphological characteristics, natural course, and prognosis of BilIN without CC are not well understood. Here, we describe an atypical case of BilIN resembling CC that presented with obstructive jaundice caused by a hematoma in the common bile duct (CBD).
Case presentation
A 64-year-old man presented to our hospital with upper abdominal pain, jaundice, and anorexia. He had diabetes and was a social drinker but a lifetime non-smoker. Computed tomography (CT) scan revealed a dilated CBD, and acute cholangitis was suspected. The patient was referred to our hospital and admitted to the gastroenterology department for further investigation and treatment. Initial laboratory examinations revealed a white blood count (WBC) of 9770/μL, hemoglobin of 12.4 g/dl, increased C-reactive protein (CRP) of 5.47 mg/dl, total bilirubin of 7.75 mg/dl, AST/ALT of 176/281 IU/L, alkaline phosphatase of 815 IU/L, and ɤ-GTP of 132 IU/L. The serum tumor markers carcinoembryonic antigen (CEA) was within the normal range at 2.6 ng/ml and cancer antigen 19–9 (CA19–9) was elevated at 1162 U/ml. Both hepatitis B surface antigen (HBsAg) and antibodies to hepatitis C virus (anti-HCV) were negative. A plain CT scan on admission showed a high-density accumulation spreading throughout the CBD, and the entire CBD was dilated (Fig. 1). Gastroenterologists performed endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic sphincterotomy (EST), during which a hematoma in the CBD was discovered. This revealed the reason for obstructive jaundice was not choledocholithiasis but the hematoma, which was subsequently drained through the incised Vater’s papilla (Fig. 2). A few days later, enhanced CT scan and magnetic resonance cholangiopancreatography (MRCP) were performed, and they showed improved dilation of the CBD and enhanced wall thickness of the bile duct measuring 25 × 10 mm at the union of the cystic and common hepatic ducts (Figs. 3 and 4). A cholangioscope detected an elevated tumor covered by sludge in the CBD (Fig. 5). The mucous membrane around the tumor showed redness and a malignant tumor was suspected. The result of the tumor biopsy revealed no malignant features in the histology, but the possibility of CC could not be denied from the macroscopic findings. We were consulted for surgical resection and performed an extrahepatic bile duct resection and cholecystectomy. Intraoperative rapid pathological diagnosis was performed, and we confirmed that the surgical margins in both the pancreatic and hepatic sides were cancer-free. The postoperative course was uneventful. The resected tumor had irregular elevated mucosa with an ulcerated lesion (Fig. 6a). The pathological examination of the resected tumor revealed that the ulcerated lesion had inflammatory granulation tissue; however, it did not contain the components of invasive carcinoma (Fig. 6b). Many consecutive intraepithelial micropapillary lesions spread around the ulcerated lesion, and the epithelial cells showed increased nucleus-to-cytoplasm ratio, nuclear hyperchromasia, and architectural atypia (Fig. 6c). The pathological diagnosis was BilIN-1 to -2. It also revealed that the BilIN-1 lesion spread through both the pancreatic and hepatic margins. Immunohistochemical staining showed that S100P was slightly expressed in the cytoplasm and MUC5AC was positive, while MUC1 was negative and p53 was not overexpressed (Fig. 6d–g).
Fig. 1.

Plain CT scan image on admission. Coronal section of plain CT showing the high-density area in the CBD (arrow) and the dilation of the CBD and intrahepatic bile duct
Fig. 2.

ERCP and the image of Vater’s papilla. ERCP showing a filling defect (arrows) in the CBD and a dilated CBD (a). EST revealed the defect was not choledocholithiasis but a hematoma in the CBD, and the hematoma was drained through the incised Vater’s papilla (b)
Fig. 3.

Enhanced CT scan images after EST. Enhanced CT scan showing improved dilation of the CBD and enhanced wall thickness (arrows) of the bile duct measuring 25 × 10 mm at the union of the cystic and common hepatic ducts (a, b)
Fig. 4.

The findings of MRCP. It shows a filling defect (arrows) at the union of the cystic and common hepatic ducts (a, b)
Fig. 5.
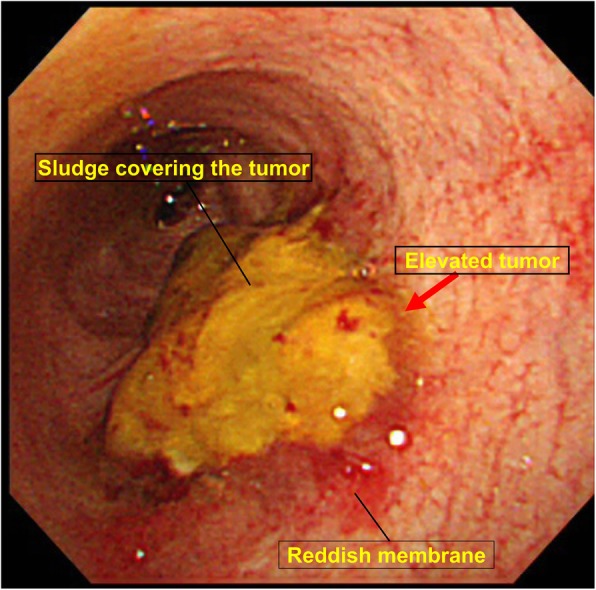
The findings of cholangioscope. It detected an elevated tumor covered by sludge in the common bile duct. The mucous membrane around the tumor showed redness and a malignant tumor was suspected
Fig. 6.

The macroscopic and pathological findings of the resected tumor. Arrows showing the irregular elevated mucosa with an ulcerated lesion of the resected tumor (a). The pathological examination of the resected tumor revealed that the ulcerated lesion had inflammatory granulation tissue but did not contain invasive carcinoma (b) (hematoxylin and eosin). Many consecutive intraepithelial micropapillary lesions spread around the ulcerated lesion (arrows), and the epithelial cells showed an increased nucleus-to-cytoplasm ratio, nuclear hyperchromasia, and architectural atypia (c) (hematoxylin and eosin, × 200). The pathological diagnosis was BilIN-1 to -2. Immunohistochemical staining showed that S100P was slightly expressed in the cytoplasm and MUC5AC was positive. MUC1 was negative and p53 was not overexpressed (d S100P, e MUC1, f MUC5AC, g p53) (× 200)
Discussion
BilIN has been defined by Zen et al. in 2005 as microscopic lesions of flat or low-papillary dysplastic epithelium [13, 14]. BilIN is regarded as the biliary counterpart of pancreatic intraepithelial neoplasia (PanIN) [11]. It is characterized by the pathological findings of irregular nuclei, cell dysplasia and irregular polarity in cytology [12]. The microscopic appearances of BilIN are classified as flat, pseudopapillary or micropapillary [12, 15]. BilIN is divided into three grades (BilIN-1, BilIN-2, and BilIN-3) based on the following histological features: degree of cellular atypia, nuclear pseudostratification and apical surface protrusions, and loss of cellular polarity [1]. Low-grade and high-grade dysplasia are abbreviated as BilIN-1 and -2, and in situ carcinoma as BilIN-3 [4]. BillN is considered to progress with increasing neoplastic potential, with BilIN-3 shifting to CC in the multistep carcinogenesis sequence [14]. Metaplastic changes of the epithelium of the bile duct can be induced by chronic inflammation, and patients often have a preceding chronic biliary disease like primary sclerosing cholangitis (PSC), choledocholithiasis, and pancreaticobiliary malfunction. with BilIN [12, 16].
In our case, there were two atypical findings regarding BilIN. One is that it occurred in a patient with no history of a prior biliary disease or chronic inflammation. Although the mucosa around the tumor showed redness, the range was limited to the junction of the cystic and common hepatic ducts. The other atypical finding is the large tumor size of 25 × 10 mm. Although BilIN is usually unrecognizable by macroscopy, the tumor was clearly detected in CT and could be observed as an elevated mass in the cholangioscope. To the best of our knowledge, it was larger than any other case of BilIN without CC reported in the literature so far and was therefore very difficult to differentiate from CC. These two findings in our case suggest that the occurrence of BilIN can be triggered by factors other than inflammation and that the tumor can grow to a size large enough to be detected by image analyses without shifting to CC.
The tumor was ulcerated and hemorrhaging in the CBD when the patient was referred to our hospital. In our case, obstructive jaundice caused by the hematoma in the CBD led to the detection of BilIN before progressing to CC. CC is not a major cause of hemobilia, which is present in only 3% of cases [17]. It was unclear why and when the tumor developed the ulcer and bleeding. It is also unknown that BIlIN itself causes stenosis of the bile duct and obstructive jaundice. In PanIN, the stenosis of the main pancreatic duct combined with distal ductal dilatation and obstructive pancreatitis is often observed [18]. However, PanIN itself is not considered to cause duct stenosis, because PanIN is almost flat with no intraductal proliferation, but inflammation or fibrosis [18]. The inflammation detached dysplastic epithelium and leaked pancreatic juice may cause further inflammation, fibrosis, and finally the stenosis [18]. According to this discussion, we speculate that BilIN itself also does not cause bile duct stenosis as well as PanIN, but if it combined with some inflammation, it could cause the destruction of bile duct epithelium, the stenosis of the bile duct, and obstructive jaundice.
It is important to detect precursor lesions early in cancer therapy, although the prognosis of BilIN without CC has not been clarified and a uniform treatment guideline is lacking. And unlike endoscopic resection for adenoma in the gastrointestinal tract, a minimally invasive treatment in the bile duct has yet to be developed. The only curative treatment for BilIN prior to malignant transformation is surgical resection [10]. In surgical resection for CC, an inspection of the resection margin often reveals the presence of BilIN [13]. It is well-established that resection with a cancer-free margin is crucial for curative therapy, but the clinical significance of BilIN in the surgical margin is unclear and additional resection is still controversial. Matthaei et al. reported that BilIN found in the surgical margin of biliary tract cancer resection in 53%; however, it does not require additional resection because the patients with BilIN-positive at the surgical margin and BilIN-negative did not differ significantly regarding overall survival [13]. They also reported that survival even of patients with BilIN-3 was not shorter than that of patients without any BilIN at margin [13]. Several studies also reported as well but the number of patients reported was small, so further study with a larger population and longer term is required [19, 20]..
Many molecular and genetic alternations have been found to occur and accumulate in BilIN during the multistep process of cholangiocarcinogenesis [12, 21]. The expression pattern of molecules in the tumor tissue biopsy related to cell cycle and carcinogenesis might be helpful in the preoperative diagnosis of BilIN and differentiation from CC. Representative molecules considered that can be upregulated in BilIN are p21, p53, cyclin D1, S100P, MUC1, and MUC5AC [2, 11, 12]. Some of them can be upregulated in CC too [11, 12]. On the other hand, most BilIN shows negativity for MUC2 [22]. The expression of MUC1 is increased along with the progression of histological grade in BilIN and associated with a poorer outcome in CC [2, 23]. MUC5AC expresses in the early stage of cholangiocarcinogenesis [24]. Recent studies showed the expression of S100P was increased in BilIN-2 and -3 as well as cholangiocarcinoma, and Sato et al. proposed the diagnostic algorithm of histological grading of BilIN including the expression of S100P in the cytoplasm that helps the grading of BilIN1–3 [12, 18, 25]. The expression level of p53 is very low not enough to be detected by immunohistochemistry in non-neoplastic cells because its half-life is normally very short [11]. P53 is mutated in a large number of malignant neoplasms, then mutated p53 can be detected immunohistochemically based on its overexpression [11]. Nakanishi et al. reported that p53 was significantly upregulated in BilIN-3 and CC compared with BilIN-1 and -2, and suggested that the expression of p53 might be involved in the acquisition of invasive growth in CC [11]. Such research on BilIN is crucial to elucidate the multistep carcinogenesis sequence from BilIN to CC. In our case, the tumor showed weak expression of S100P, positive MUC5AC, negative MUC1, and not overexpressed p53, which is consistent with the pathological features of BilIN-1 and BilIN-2.
Conclusion
We experienced an atypical case of BilIN mimicking CC that presented with obstructive jaundice caused by a hematoma in the CBD. Our case suggested that the occurrence of BilIN can be triggered by factors other than an inflammatory condition and can potentially grow to a size large enough to be detected by diagnostic imaging.
Acknowledgements
We would like to thank Brandi Jones for the English language editing.
Abbreviations
- Anti-HCV
Antibodies to hepatitis C virus
- BilIN
Biliary intraepithelial neoplasia
- CA19–9
Cancer antigen 19–9
- CBD
Common bile duct
- CC
Cholangiocarcinoma
- CEA
Carcinoembryonic antigen
- CRP
C-reaction protein
- CT
Computed tomography
- ERCP
Endoscopic retrograde cholangiopancreatography
- EST
Endoscopic sphincterotomy
- HBsAg
Hepatitis B surface antigen
- IPNB
Intraductal papillary neoplasm of bile duct
- MCN
Mucinous cystic neoplasm
- MRCP
Magnetic resonance cholangiopancreatography
- PanIN
Pancreatic intraepithelial neoplasia
- PSC
Primary sclerosing cholangitis
- WBC
White blood cell
Authors’ contributions
NY designed the report, analyzed the data, and wrote the manuscript. TA, AI, KM, KI, YT, EO, SM, SS, NS, KK, AS, AI, YS, GH, TO, and MT collected the patient’s clinical data. YK and YN performed the pathological diagnosis and immunohistochemistry. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
Data supporting the conclusions of this study are included in this published article.
Ethics approval and consent to participate
Ethics approval was obtained from our hospital’s review broad (RON19-0701).
Consent for publication
Written informed consent was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Lendvai G, Szekerczes T, Illyes I, Dora R, Kontsek E, Gogl A, Kiss A, Werling K, Kovalszky I, Schaff Z, Borka K. Cholangiocarcinoma: classification, histopathology and molecular carcinogenesis. Pathol Oncol Res; 2018. 10.1007/s12253-018-0491-8. [DOI] [PubMed]
- 2.Zen Y, Sasaki M, Fujii T, Chen TC, Chen MF, Yeh TS, Jan YY, Huang SF, Nimura Y, Nakanuma Y. Different expression patterns of mucin core proteins and cytokeratins during intrahepatic cholangiocarcinogenesis from biliary intraepithelial neoplasia and intraductal papillary neoplasm of the bile duct--an immunohistochemical study of 110 cases of hepatolithiasis. J Hepatol. 2006;44(2):350–358. doi: 10.1016/j.jhep.2005.09.025. [DOI] [PubMed] [Google Scholar]
- 3.Jang KT, Ahn S. Tumoral versus flat intraepithelial neoplasia of pancreatobiliary tract, gallbladder, and ampulla of Vater. Arch Pathol Lab Med. 2016;140(5):429–436. doi: 10.5858/arpa.2015-0319-RA. [DOI] [PubMed] [Google Scholar]
- 4.Zen Y, Aishima S, Ajioka Y, Haratake J, Kage M, Kondo F, Nimura Y, Sakamoto M, Sasaki M, Shimamatsu K, Wakasa K, Park YN, Chen MF, Atomi Y, Nakamura Y. Proposal of histological criteria for intraepithelial atypical/proliferative biliary epithelial lesions of the bile duct in hepatolithiasis with respect to cholangiocarcinoma: preliminary report based on interobserver agreement. Pathol Int. 2005;55:180–188. doi: 10.1111/j.1440-1827.2005.01816.x. [DOI] [PubMed] [Google Scholar]
- 5.Bosman F, Caarneiro F, Hruban R, Theise N. WHO classification of tumors of the digestive system. 4. Lyon: IARC; 2010. [Google Scholar]
- 6.Sohn WJ, Jo S. A huge intraductal papillary mucinous carcinoma of the bile duct treated by right trisectionectomy with caudate lobectomy. World J Surg Oncol. 2009;7:93. doi: 10.1186/1477-7819-7-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akbarzadeh L, Geramizadeh B, Kazemi K, Nikeghbalian S, Malekhosseini S. Biliary intraepithelial Neoplasia (BilIN) in primary sclerosing cholangitis: the first report from Iran. Hepat Mon. 2016;16(12):e38726. doi: 10.5812/hepatmon.38726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang W, Chen W, Li K, Wang J. Successful treatment of biliary intraepithelial neoplasia in the common bile duct via local excision: a case report. Oncol Lett. 2016;11(5):3142–3144. doi: 10.3892/ol.2016.4336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ohtani H, Ishida H, Ito Y, Yamaguchi T, Koizumi M. Autoimmune pancreatitis and biliary intraepithelial neoplasia of the common bile duct: a case with diagnostically challenging but pathogenetically significant association. Pathol Int. 2011;61(8):481–485. doi: 10.1111/j.1440-1827.2011.02684.x. [DOI] [PubMed] [Google Scholar]
- 10.Jung W, Kim B. Biliary intraepithelial neoplasia: a case with benign biliary stricture. Korean J Hepatol. 2011;17(4):328–330. doi: 10.3350/kjhep.2011.17.4.328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nakanishi Y, Zen Y, Kondo S, Itoh T, Itatsu K, Nakanuma Y. Expression of cell cycle-related molecules in biliary premalignant lesions: biliary intraepithelial neoplasia and biliary intraductal papillary neoplasm. Hum Pathol. 2008;39(8):1153–1161. doi: 10.1016/j.humpath.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 12.Sato Y, Sasaki M, Harada K, Aishima S, Fukusato T, Ojima H, Kanai Y, Kage M, Nakanuma Y, Tsubouchi H. Hepatolithiasis subdivision of intractable hepatobiliary disease study Group of Japan (chairman, Hirohito Tshubouchi): pathological diagnosis of flat epithelial lesions of the biliary tract with emphasis on biliary intraepithelial neoplasia. J Gastroenterol. 2014;49(1):64–72. doi: 10.1007/s00535-013-0810-5. [DOI] [PubMed] [Google Scholar]
- 13.Matthaei H, Lingohr P, Strasser A, Dietrich D, Rostamzadeh B, Glees S, Roering M, Mohring P, Scheerbaum M, Stoffels B, Kalff JC, Schafer N, Kristiansen G. Biliary intraepithelial neoplasia (BilIN) is frequently found in surgical margins of biliary tract cancer resection specimens but has no clinical implications. Virchows Arch. 2015;466(2):133–141. doi: 10.1007/s00428-014-1689-0. [DOI] [PubMed] [Google Scholar]
- 14.Zen Y, Adsay NV, Bardadin K, Colombari R, Ferrell L, Haga H, Hong SM, Hytiroglou P, Kloppel G, Lauwers GY, Leeuwen DJ, Notohara K, Oshima K, Quaglia A, Sasaki M, Sessa F, Suriawinata A, Tsui W, Atomi Y, Nakanuma Y. Biliary intraepithelial neoplasia: an international interobserver agreement study and proposal for diagnostic criteria. Mod Pathol. 2007;20(6):701–709. doi: 10.1038/modpathol.3800788. [DOI] [PubMed] [Google Scholar]
- 15.Kendall T, Verheij J, Gaudio E, Evert M, Guido M, Goeppert B, Carpino G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019;39(Suppl 1):7–18. doi: 10.1111/liv.14093. [DOI] [PubMed] [Google Scholar]
- 16.Rougemont AL, Genevay M, McKee TA, Gremaud M, Mentha G, Rubbia-Brandt L. Extensive biliary intraepithelial neoplasia (BilIN) and multifocal early intrahepatic cholangiocarcinoma in non-biliary cirrhosis. Virchows Arch. 2010;456(6):711–717. doi: 10.1007/s00428-010-0899-3. [DOI] [PubMed] [Google Scholar]
- 17.Umeda R, Nakamura Y, Masugi Y, Shinoda M, Hosoe N, Ono Y, Fujimura T, Yamagishi Y, Higuchi H, Ebinuma H, Hozawa S, Tanabe M, Hashimoto S, Sakamoto M, Kitagawa Y, Hibi T. Hemobilia due to biliary intraepithelial neoplasia associated with Zollinger-Ellison syndrome. Clin J Gastroenterol. 2012;5(3):189–194. doi: 10.1007/s12328-012-0296-3. [DOI] [PubMed] [Google Scholar]
- 18.Yokode M, Akita M, Fujikura K, Kim MJ, Morinaga Y, Yoshikawa S, Terada T, Matsukiyo H, Tajiri T, Abe-Suzuki S, Itoh T, Hong SM, Zen Y. High-grade PanIN presenting with localised stricture of the main pancreatic duct: a clinicopathological and molecular study of 10 cases suggests a clue for the early detection of pancreatic cancer. Histopathology. 2018;73(2):247–258. doi: 10.1111/his.13629. [DOI] [PubMed] [Google Scholar]
- 19.Wakai T, Shirai Y, Moroda T, Yokoyama N, Hatakeyama K. Impact of ductal resection margin status on long-term survival in patients undergoing resection for extrahepatic cholangiocarcinoma. Cancer. 2005;103(6):1210–1216. doi: 10.1002/cncr.20906. [DOI] [PubMed] [Google Scholar]
- 20.Sasaki R, Takeda Y, Funato O, Nitta H, Kawamura H, Uesugi N, Sugai T, Wakabayashi G, Ohkohchi N. Significance of ductal margin status in patients undergoing surgical resection for extrahepatic cholangiocarcinoma. World J Surg. 2007;31(9):1788–1796. doi: 10.1007/s00268-007-9102-7. [DOI] [PubMed] [Google Scholar]
- 21.Sato Yasunori, Harada Kenichi, Sasaki Motoko, Nakanuma Yasuni. Histological Characterization of Biliary Intraepithelial Neoplasia with respect to Pancreatic Intraepithelial Neoplasia. International Journal of Hepatology. 2014;2014:1–7. doi: 10.1155/2014/678260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ainechi S, Lee H. Updates on precancerous lesions of the biliary tract: biliary precancerous lesion. Arch Pathol Lab Med. 2016;140(11):1285–1289. doi: 10.5858/arpa.2015-0396-RS. [DOI] [PubMed] [Google Scholar]
- 23.Park SY, Roh SJ, Kim YN, Kim SZ, Park HS, Jang KY, Chung MJ, Kang MJ, Lee DG, Moon WS. Expression of MUC1, MUC2, MUC5AC and MUC6 in cholangiocarcinoma: prognostic impact. Oncol Rep. 2009;22(03):649–657. doi: 10.3892/or_00000485. [DOI] [PubMed] [Google Scholar]
- 24.Sasaki M, Nakanuma Y, Kim YS. Characterization of Apomucin expression in intrahepatic cholangiocarcinomas and their precursor lesions: an immunohistochemical study. Hepatology. 1999;24(5):1074–1078. doi: 10.1002/hep.510240516. [DOI] [PubMed] [Google Scholar]
- 25.Nakanuma Y, Uchida T, Sato Y, Uesaka K. An S100P-positive biliary epithelial field is a preinvasive intraepithelial neoplasm in nodular-sclerosing cholangiocarcinoma. Hum Pathol. 2017;60:46–57. doi: 10.1016/j.humpath.2016.10.003. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data supporting the conclusions of this study are included in this published article.