

ABSTRACT
Aim
Previous investigations have shown that end‐stage renal disease (ESRD) is associated with an increased risk of malignancies. The aim of this study was to explore the association between ESRD in patients undergoing maintenance haemodialysis (HD) and the incidence of malignancies according to age.
Methods
We analysed a nationwide cohort retrieved from Taiwan's National Health Insurance Research Database to study the incidence of malignancies in patients who were and were not receiving HD. One million beneficiaries were randomly selected and followed from 2005 to 2013. Of these 1 000 000 patients, 3055 developed ESRD and commenced maintenance HD during this period. For each HD patient, four age‐, gender‐ and diabetes‐matched controls were selected from the database (n = 12 220). We further stratified the patients according to age. The study endpoint was the occurrence of malignancy.
Results
The incidence rates of malignancy were 6.8% and 4.9% in the HD and control groups, respectively. Competing risk regression analysis indicated that age, HD, male gender and diabetes were associated with an increased risk of malignancy. When further stratified according to age, the odds ratios of developing cancer were 5.8, 1.9, 1.9 and 1.5 among the HD patients aged <40 years, 40–49 years, 50–59 years and 60–69 years, respectively.
Conclusion
The patients with ESRD who received HD had a significantly higher cumulative risk of malignancy, especially those with a young age. Therefore, specialized cancer screening protocols for young HD patients might help to prolong their lifespan.
Keywords: end‐stage renal disease, haemodialysis, malignancy, young adults
SUMMARY AT A GLANCE
End‐stage kidney disease is associated with an increased risk of many malignancies. This epidemiological study from Taiwan reviews the incidence rates of malignancies in a large haemodialysis cohort compared to a control group, revealing a higher cumulative risk of malignancies especially in those of a young age on dialysis.
There is a graded increase in the incidence of cancer among the general population, chronic kidney disease (CKD) patients, end‐stage renal disease (ESRD) patients on dialysis and kidney transplant patients.1, 2, 3, 4, 5 It has been reported that the prevalence rates of genitourinary malignancies, liver cancer, thyroid cancer, multiple myeloma and lymphoma are higher in ESRD patients compared to the general population.5 The possible pathophysiological pathways include disturbance of the immune system, chronic infection with oncogenic viruses, chronic inflammation, nutritional deficiency, impaired DNA repair, accumulation of carcinogenic compounds and reduction of anti‐oxidant capacity.6 In addition, the underlying disease leading to ESRD, such as renal cystic disease, diabetes mellitus, smoking, obesity, hypertension, infection, analgesic abuse and the use of Chinese herbal products containing aristolochic acid may predispose such patients to the development of malignancies.7, 8
The incidence and prevalence rates of patients with ESRD receiving maintenance haemodialysis (HD) are high in Taiwan.9 In the general population, malignant neoplasms are prevalent in the elderly and negatively impact patient outcomes. Previous studies have reported that the risk of malignancies in patients with ESRD decreases with advancing age.8, 10 However, most previous studies have been limited by including patients with ESRD who were and were not receiving maintenance dialysis, and a lack of information on personal habits.8, 10, 11 These limitations may have skewed the results due to confounding caused by the unadjusted underlying risk factors and competing risk of mortality. Furthermore, it has been reported that the HD procedure itself may affect the incidence of malignancies due to bioincompatibility of the dialysis equipment, waterborne toxins in the dialysate, silicone particles from dialysis tubing, accumulation of carcinogens or efflux of di‐(2‐ethylhexyl) phthalate from the blood circuit contributing to immunosuppression and the development of malignancy.12 Considering the positive correlation between the length of HD and onset of malignancies,10, 13 the aim of the present study was to investigate the incidence of malignancies in patients with newly confirmed ESRD who initiated maintenance HD. In addition, to thoroughly evaluate the relationship between the incidence of cancer and age in patients undergoing HD, we stratified the incidence of malignancies in these patients according to age.
METHODS
Data source
This nationwide population‐based cohort study was conducted using the National Health Insurance Research Database (NHIRD) released by the Taiwan National Health Research Institute. The NHI program covers 99.9% of the population in Taiwan (about 23.2 million people in 2012). The data contained in the NHIRD includes original claims files and registration data submitted by almost all medical institutions in Taiwan.
The Longitudinal Health Insurance Database (LHID) 2005 contains all of the registration and claims data of 1 000 000 subjects enrolled in 2005 who were randomly sampled from the beneficiaries of the NHI program from January 1st 2005 to January 1st 2006. There are approximately 25.68 million individuals in this registry. There was no significant difference in the gender distribution (χ 2 = 0.008, df = 1, P = 0.931) between the patients in the LHID2005 and the original NHIRD. All clinical diagnoses are recorded according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) codes. The accuracy of the diagnoses of major diseases in the claims database, such as CKD, coronary artery disease and cerebrovascular events has been validated14, 15 Furthermore, under the NHI program in Taiwan, certain severe diseases, such as ESRD with dialysis and malignancy, can be identified using the Registry for Catastrophic Illness Patient Database. Patients with ESRD must receive lifelong maintenance dialysis, and patients with biopsy proof of malignant disease are eligible for a catastrophic illness certificate. Catastrophic illness certificate holders are exempt from paying insurance premiums and co‐payments. Therefore, all certification applications are carefully reviewed by the Bureau of NHI, and a catastrophic illness certificate can be considered to indicate an accurate and reliable diagnosis. The records and information of the patients were de‐identified prior to analysis to ensure patient anonymity. This study was approved by the Ethics Institutional Review Board of Chang Gung Memorial Hospital.
Study design and patient setting
We enrolled 3055 of the 1 000 000 subjects in the LHID 2005 who developed ESRD and commenced maintenance HD (those who had catastrophic illness registration cards of ESRD with dialysis) between January 1, 2005 and December 31, 2013. The exclusion criteria were subjects who had received regular renal replacement therapy before the study period, those who had undergone renal transplantation, and those aged below 18 years. For each enrolled HD patient, four controls matched for age, gender and diabetes at the same index date (n = 12 220) were enrolled from the remaining subjects (n = 996 945) (Fig. 1). We further stratified the patients by age. The study endpoint was the occurrence of malignancy. Comorbidities including hypertension, dyslipidaemia, coronary artery disease, stroke, peripheral vascular disease and smoking were also recorded. All associated International Classification of Diseases, Ninth Revision, Clinical modification (ICD‐9‐CM) codes are available in Table S1. The index date was defined as the date when the patient was issued with a catastrophic illness certificate for ESRD with dialysis. The follow‐up period was defined as the time from the index date to December 31 2013, or whenever the patients developed malignancy, died or were lost to follow‐up.
Figure 1.
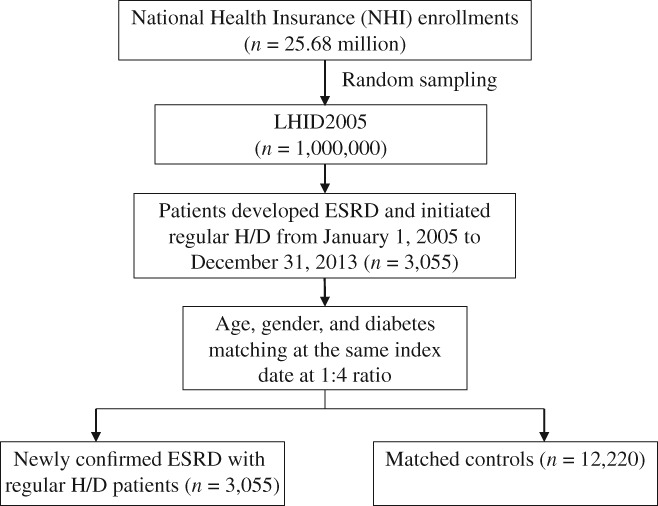
Flowchart of study enrolment. From 2005 to 2013, a total of 3055 patients from 1 million subjects in the NHIRD developed ESRD and received regular HD. For each HD patient, four age‐, gender‐ and diabetes‐matched controls (n = 12 220 patients) were selected from the NHIRD on the same date as the HD patients were enrolled. ESRD, end‐stage renal disease; HD, haemodialysis; LHID, Longitudinal Health Insurance Database; NHIRD, National Health Insurance Research Database.
Statistical analysis
Descriptive statistics were expressed as mean and standard deviation unless otherwise stated. In the primary analysis, we compared the HD group with the matched control group. All numerical variables were tested for normality using the Kolmogorov–Smirnov test. The Student's t‐test was used to compare the mean values of continuous variables and normally distributed data between groups, and the Mann–Whitney U test was used for other data. Categorical data were tested using the χ2 test. Death is a competing risk for the development of malignancy. As patients receiving dialysis have a relatively higher risk of mortality compared to the general population, we used a competing risk regression model for multivariate analysis.16 The cumulative incidence function curves of malignancy in different age groups were plotted. All statistical tests were two‐tailed, and a P value of <0.05 was considered to be statistically significant. Data were analyzed using SAS version 9.0 statistical software SAS, EG (SAS Institute Inc., Cary, NC, USA).
RESULTS
Baseline characteristics of the study population
Table 1 shows the demographic data and clinical characteristics of the study cohort. Among the 3055 patients in the HD group, 52.8% were male and 66.5% had diabetes mellitus. The mean patient age was 59.7 ± 14.1 years. Compared to the matched controls, the HD group had a higher burden of comorbidities.
Table 1.
Baseline characteristics of the study population and matched controls
| Variables | Haemodialysis (n = 3055) | Control (n = 12 220) | P value |
|---|---|---|---|
| Age, mean (years) | 59.7 ± 14.1 | 59.7 ± 14.1 | NS (1.000) |
| Age group, n (%) (years) | |||
| <40, n (%) | 178 (5.8%) | 712 (5.8%) | NS (1.000) |
| 40–49, n (%) | 316 (10.3%) | 1264 (10.3%) | NS (1.000) |
| 50–59, n (%) | 690 (22.6%) | 2760 (22.6%) | NS (1.000) |
| 60–69, n (%) | 738 (24.2%) | 2952 (24.2%) | NS (1.000) |
| 70–79, n (%) | 781 (25.6%) | 3124 (25.6%) | NS (1.000) |
| >80, n (%) | 352 (11.5%) | 1408 (11.5%) | NS (1.000) |
| Male gender, n (%) | 1612 (52.8%) | 6448(52.8%) | NS (1.000) |
| Diabetes mellitus, n (%) | 2031 (66.5%) | 8124 (66.5%) | NS (1.000) |
| Hypertension, n (%) | 2890 (94.6%) | 6576 (53.8%) | <0.001 |
| Dyslipidaemia, n (%) | 1917 (62.8%) | 4708 (38.5%) | <0.001 |
| Coronary artery disease, n (%) | 1399 (45.8%) | 2867 (23.5%) | <0.001 |
| Stroke, n (%) | 1030 (33.7%) | 2444 (20.0%) | <0.001 |
| Peripheral vascular disease, n (%) | 415 (13.6%) | 797 (6.5%) | <0.001 |
| Smoking, n (%) | 26 (0.9%) | 8 (0.1%) | <0.001 |
Values in bold are statistically significant (P < 0.05).
Risk factors for malignancy in the HD and control groups
In the present study, 813 patients had newly diagnosed malignancy (209 in the HD group and 604 in the control group). The incidence rates of malignancy were 6.8% for the HD group and 4.9% for the control group (Table 2). The occurrence rates of Kaposi's sarcoma (0.1% vs 0.0%, P = 0.005), genitourinary organ (1.6% vs 0.8%, P < 0.001), lymphatic and hematopoietic tissue (0.5% vs 0.2%, P = 0.004), and liver (1.4% vs 1.0%, P = 0.017) malignancies were significantly higher in the HD group, while those of oral, pharynx, digestive organ and peritoneum, respiratory and intrathoracic organ, bone, connective, skin and breast malignancies and those of other unspecified sites of malignancy were not different between the two groups. Multivariate analysis revealed that HD (hazard ratio (HR) = 1.893, 95% confidence interval (CI) = 1.594–2.249, P < 0.001) was an independent prognostic indicator of malignancy after adjusting for age, gender, diabetes mellitus, hypertension, dyslipidaemia, coronary artery disease, stroke, peripheral vascular disease and smoking. Age (HR = 1.034, 95% CI = 1.028–1.040, P < 0.001), male gender (HR = 1.680, 95% CI = 1.456–1.938, P < 0.001), diabetes mellitus (HR = 1.283, 95% CI = 1.082–1.521, P = 0.004) and hypertension (HR = 1.288, 95% CI = 1.072–1.547, P = 0.007) were also identified to be independent risk factors for the development of malignancy (Table 3).
Table 2.
Incidence of cancer in the haemodialysis patients and matched controls
| Variables | Haemodialysis (n = 3055) | Control (n = 12 220) | P value |
|---|---|---|---|
| Male gender | 1612 (52.8%) | 6448 (52.8%) | NS (1.000) |
| Age | 59.7 ± 14.1 | 59.7 ± 14.1 | NS (1.000) |
| Diabetes mellitus | 2031 (66.5%) | 8124 (66.5%) | NS (1.000) |
| All types of malignancy | 209 (6.8%) | 604 (4.9%) | <0.001 |
| Malignant neoplasm of the lip, oral cavity and pharynx | 16(0.5%) | 38 (0.3%) | NS (0.076) |
| Malignant neoplasm of digestive organs and peritoneum | 91 (3.0%) | 295 (2.4%) | NS (0.075) |
| Malignant neoplasm of respiratory and intrathoracic organs | 18 (0.6%) | 110 (0.9%) | NS (0.092) |
| Malignant neoplasm of bone, connective tissue, skin, and breast | 11 (0.4%) | 49 (0.4%) | NS (0.746) |
| Kaposi's sarcoma | 2 (0.1%) | 0 (0.0%) | 0.005 |
| Malignant neoplasm of genitourinary organs | 49 (1.6%) | 96 (0.8%) | <0.001 |
| Malignant neoplasm of other and unspecified sites | 52 (1.7%) | 173 (1.4%) | NS (0.240) |
| Malignant neoplasm of lymphatic and hematopoietic tissue | 15 (0.5%) | 24 (0.2%) | 0.004 |
| Malignant neoplasm of the liver | 44 (1.4%) | 116 (1.0%) | 0.017 |
Values in bold are statistically significant (P < 0.05).
Table 3.
Competing risk regression analysis of all cancers
| Variables | Coefficient | Hazard ratio | 95% Confidence interval | P value |
|---|---|---|---|---|
| Haemodialysis | 0.638 | 1.893 | 1.594–2.249 | <0.001 |
| Male gender | 0.519 | 1.680 | 1.456–1.938 | <0.001 |
| Age | 0.034 | 1.034 | 1.028–1.040 | <0.001 |
| Diabetes mellitus | 0.249 | 1.283 | 1.082–1.521 | 0.004 |
| Hypertension | 0.253 | 1.288 | 1.072–1.547 | 0.007 |
| Dyslipidaemia | −0.003 | 0.997 | 0.856–1.161 | NS (0.967) |
| Coronary artery disease | 0.053 | 1.054 | 0.900–1.235 | NS (0.512) |
| Stroke | −0.047 | 0.954 | 0.809–1.124 | NS (0.573) |
| Peripheral vascular disease | 0.026 | 1.026 | 0.815–1.292 | NS (0.828) |
| Smoking | 0.089 | 1.093 | 0.272–4.395 | NS (0.901) |
Values in bold are statistically significant (P < 0.05).
Impact of age on the development of malignancy in the HD and control groups
Overall, the incidence of malignancy was higher in the HD group (6.8% vs 4.9%, P < 0.001). Among the control group, the incidence rates of malignancy were proportional to age; while this increased trend of malignancy with advanced age was not obvious in the HD group. Compared with the controls, the odds ratio (OR) of malignancy in the HD group gradually reduced with age as follows: <40 years: OR = 5.788, 3.9% vs 0.7%, P < 0.001; 40–49 years: OR = 1.859, 4.8% vs 2.6%, P = 0.004; 50–59 years: OR = 1.945, 6.1% vs 3.2%, P < 0.001; 60–69 years: OR = 1.510, 7.7% vs 5.3%, P = 0.010; 70–79 years: OR = 1.099, 7.7% vs 7.0%, P = 0.535; and > 80 years: OR = 1.107, 8.0% vs 7.2%, P = 0.649. The HD patients <70 years had significantly higher proportions of malignancies than the controls in all age strata. Figure 2 demonstrates the higher risks of malignancy in the HD group compared to the control group during the follow‐up period, especially in the younger patients.
Figure 2.
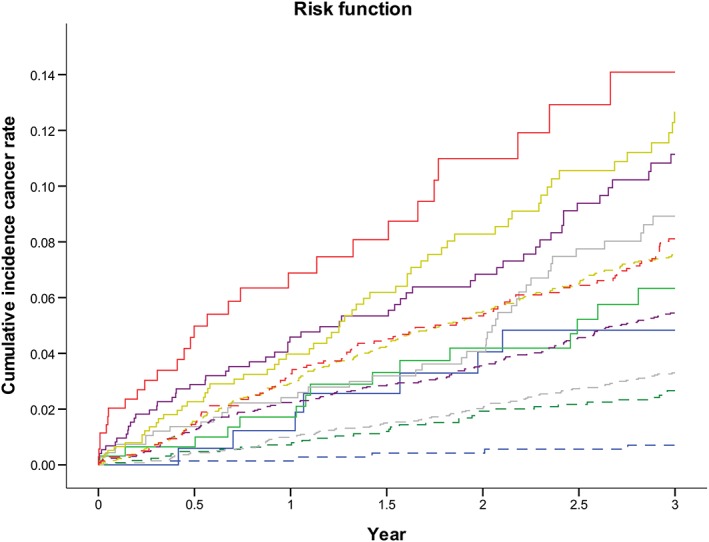
Cumulative incidence rates of cancer in the 3055 HD patients and 12 220 controls. Patients were stratified according to age. The cumulative incidence curves illustrated that the HD patients had a higher risk of malignancy than the controls in the same age group, and especially the younger patients. HD, haemodialysis. ( ) HD 00∼39, (
) HD 00∼39, ( ) HD 40∼49, (
) HD 40∼49, ( ) HD 50∼59, (
) HD 50∼59, ( ) HD 60∼69, (
) HD 60∼69, ( ) HD 70∼79, (
) HD 70∼79, ( ) HD 80up, (
) HD 80up, ( ) non HD 00∼39, (
) non HD 00∼39, ( ) non HD 40∼49, (
) non HD 40∼49, ( ) non HD 50∼59, (
) non HD 50∼59, ( ) non HD 60∼69, (
) non HD 60∼69, ( ) non HD 70∼79, (
) non HD 70∼79, ( ) non HD 80up.
) non HD 80up.
DISCUSSION
In the present study, the total incidence rate of cancer was 6.8% in the HD group, which is consistent with previous reports.13, 17 The patients undergoing HD had significantly increased risks of all types of malignancies; particularly, those of the genitourinary organs, liver and lymphatic and hematopoietic tissues (Table 2). We also found that HD, age, male gender, diabetes mellitus and hypertension were significantly associated with an increased risk of developing malignancy (Table 3). Compared with the age‐, gender‐ and diabetes‐matched controls, the HD patients aged younger than 70 years had a significantly higher incidence of malignancy. Moreover, this increased risk of malignancy among the HD patients was even more obvious in the younger patients (Table 4).
Table 4.
Incidence of cancer in the haemodialysis patients and matched controls in different age groups
| Age group, n (%) (years) | Haemodialysis (n = 3055) | Control (n = 12 220) | Odds ratio | P value |
|---|---|---|---|---|
| Total, n (%) | 209 (6.8%) | 604 (4.9%) | 1.412 | <0.001 |
| <40, n (%) | 7 (3.9%) | 5 (0.7%) | 5.788 | 0.004 |
| 40–49, n (%) | 15 (4.8%) | 33 (2.6%) | 1.859 | 0.048 |
| 50–59, n (%) | 42 (6.1%) | 89 (3.2%) | 1.945 | <0.001 |
| 60–69, n (%) | 57 (7.7%) | 155 (5.3%) | 1.510 | 0.010 |
| 70–79, n (%) | 60 (7.7%) | 220 (7.0%) | 1.099 | NS (0.535) |
| >80, n (%) | 28 (8.0%) | 102 (7.2%) | 1.107 | NS (0.649) |
Values in bold are statistically significant (P < 0.05).
Renal impairment impacts the homeostatic balance of fluids and solutes and the removal of waste products from the blood.18 The accumulation of uremic toxins and metabolic acidosis impairs humoral and cell‐mediated immunity.19 Nutritional abnormalities that are prevalent among patients undergoing HD, such as insufficiency of trace elements and vitamin D20, 21 can also make the patients more susceptible to viral‐mediated cancers, including human papillomavirus (HPV)‐associated genital cancers, and hepatitis virus‐associated liver cancers.22 Epidemiological investigations have indicated that patients with ESRD have a higher prevalence of urinary tract malignancies with different pathological features compared to the general population.3, 4 Risk factors such as analgesic abuse, smoking, obesity, the use of Chinese herbal products, groundwater intake, ethyl benzenes, phenacetin, hypertension, diabetes, chronic diuretic use and other underlying primary renal diseases may also be responsible for the development of urinary tract malignancies.18 Chronic hepatitis is a common disease in Taiwan,23 and patients undergoing HD have been shown to have higher risks of hepatitis B virus (HBV) and hepatitis C virus (HCV) compared to the general population,11 possibly due to blood contamination by instruments, machines and medical personnel during routine procedures and more frequent blood transfusions. This may also account for the observed increased risk of liver cancer in HD patients. Moreover, HD patients are more frequently exposed to erythropoietin, immunosuppressants and heavy metals during treatment or due to the nature of the underlying disease, all of which may be associated with carcinogenesis or the apoptosis of cells with damaged DNA and neoplastically transformed cells. These findings could, at least partially, explain the increased incidence of hematologic and lymphatic malignancies among patients undergoing HD.24, 25
End‐stage renal disease is associated with significant morbidity and mortality, and higher rates of cardiovascular complications have been reported in HD patients independently of traditional risk factors, such as hypertension, diabetes and dyslipidemia.2 Compared to relatively young patients, older HD patients are more likely to die from other causes before developing malignancy.10 Weng et al.13 suggested that the risk of cancer is lower than estimated in ESRD patients as they grow older. Our results further clearly demonstrated that the incidence of cancer in the HD patients aged younger than 70 years was significantly higher than that of the general population. Moreover, this trend was even more significant with decreasing age. In Taiwan, the incidence of malignancies has been steadily increasing and become very distinct between male and female patients during the last few decades.17 Moreover, diabetes mellitus is a well‐known risk factor for cancer and also one of the most common causes of ESRD in younger patients.6, 26 The strengths of the present study are that it compared HD patients with age‐, gender‐ and diabetes‐matched control patients, and more precisely evaluated the impact of HD on the incidence of cancer in a wide range of age groups.
Because a considerable number of chronic HD patients might develop malignancies without obvious symptoms, the timely diagnosis is challenging for investigators and clinicians. Cancer screening for an individual is predicated on the risk of developing cancer and the cost‐effectiveness of detecting the cancer. In the literature, general routine cancer screening of ESRD patients is not recommended because the expected remaining lifetime of most dialysis patients is shorter than the time lived to develop malignancy, and therefore cancer screening in dialysis patients does not seem to be cost‐effective in view of the survival benefit. Most clinicians would agree that cancer screening should target patients most likely to benefit.27 In Taiwan, HD patients younger than 60 years old have an average life expectancy of more than 10 years (Figure S1), and our study highlights the significantly high incidence of cancer, particularly of genitourinary organs, liver and lymphatic and hematopoietic malignancies in these patients. The average 5‐year survival rates of genitourinary tract and liver malignancies in the general population are 48.8% and 14.8%, respectively,28, 29 while the prognoses of these malignancies are even worse in CKD and ESRD patients.23, 30 Routine screening for genitourinary and liver malignancies may therefore be beneficial for young HD patients. The increased risk of cancer among ESRD patients may largely be due to the effects of underlying renal or urinary tract diseases (as in acquired renal cystic disease) and an increased susceptibility to viral carcinogenesis.6 Dialysis patients frequently have no urinary output, and a lack of urinary tract symptoms might delay the diagnosis of urinary tract malignancies compared to the general population.31 Acquired cystic disease and prolonged exposure to analgesics and cyclophosphamide are the most common risk factors contributing to the higher incidence of urinary tract malignancies. Young HD patients with increased cancer risk factors might be appropriate candidates for yearly prostate‐specific antigen tests for prostate cancer screening. Annual imaging studies for renal cell carcinoma should also be considered in patients on maintenance dialysis over 3 years and on the waiting list for kidney transplantation.32 Epidemiological studies have shown that HPV infection is a strong risk factor for cervical and other genital malignancies. HPV DNA test, HPV vaccine and annual Papanicolaou smears for cervical cancer screening might also be recommended in young female HD patients, especially in transplant candidates.32 Infection with HBV or HCV is a predisposing factor for the development of liver cancer. For dialysis patients who have chronic HBV or HCV infection, clinical symptoms and signs of active liver disease should be closely monitored, and liver enzymes, serum albumin level, complete blood counts, prothrombin time, serum α‐foetal protein level and liver ultrasound should be followed up regularly, and anti‐viral treatment is also recommended.33, 34 Lymphatic and hematopoietic malignancies vary in aetiology and survival.35 It has been reported that there are no significant differences in stage at diagnosis for lymphatic and hematopoietic malignancies between dialysis patients and the general population.31 Because of the high incidence of anaemia and the use of anti‐coagulants, complete blood count tests are usually followed up regularly in dialysis patients. This may bring lymphatic and hematopoietic abnormalities to attention earlier. Extra routine screening for lymphatic and hematopoietic malignancies might be not cost‐effective. However, due to the increased incidence of lymphatic and hematopoietic malignancies, young HD patients should avoid occupational exposure to benzene, arsenic and radiation, certain daily supplies with chemical contents including di‐(2‐ethylhexyl) phthalate, bisphenol A, vinclozolin and dichlorodiphenyltrichloroethane and viral infection such as human immunodeficiency virus infection.36, 37 On the basis of our study results, we suggest that more attention should be paid to teaching young HD patients how to avoid the well‐known risk factors for genitourinary tract, liver and lymphatic and hematologic malignancies. Future personalized and specialized cancer screening protocols for young HD patients might help to detect malignancies early and allow for timely interventions and prolong the lifespan of such patients. Further well‐powered research is needed to study this issue.
There are several limitations to this study. First, the HD patients had a high frequency of physician visits, which might have led to increased incidence rates of some malignancies, and may have had various effects on cancer stage at diagnosis due to the lack of consistent guidelines on cancer screening in these patients.31 Second, this study was a large cohort observational study, which lacked information on biochemistry parameters. Correlations between the patients’ characteristics and clinical outcomes could not be thoroughly explored. Third, the study was conducted on a homogeneous group of Asian ethnicity, which limits the generalizability of our findings to other different patient populations. Fourth, diseases were defined according to diagnostic codes, so some mild diseases with trivial symptoms or conditions occurring outside the medical health system could have been underestimated. Finally, the predictive accuracy of a competing risk regression model has its own limitations.
In conclusion, we found that the patients undergoing HD had a significantly increased risk of genitourinary tract, liver, lymphatic and hematologic malignancies, and the young HD patients had an even higher risk compared to the general population. Young HD patients may require more intensive cancer prevention strategies to improve their outcomes.
DISCLOSURE
We have no conflict of interest to report.
Supporting information
Fig. S1 (a) Comparison of life expectancy between the general population and patients with end‐stage renal disease undergoing chronic dialysis in Taiwan. (b) Comparison of life expectancy among haemodialysis, peritoneal dialysis, and transplant patients in Taiwan.
Table S1 List of the International Classification of Disease, Ninth Revision, Clinical modification (ICD‐9‐CM) diagnostic and procedure codes.
ACKNOWLEDGEMENTS
This work was funded by Chang Gung Memorial Hospital Research Program (Grant CMRPG2B0141) and the Ministry of Science and Technology of Taiwan (Grant MOST 107‐2321‐B–182‐004). The authors thank the statistical assistance and wish to acknowledge the support of the Maintenance Project of the Biostatistical Consultation Center (Grant CLRPG2C0021, CLRPG2C0022, CLRPG2C0023, CLRPG2C0024, CLRPG2G0081) at Chang Gung Memorial Hospital for study design and monitor, data analysis and interpretation.
REFERENCES
- 1. Vajdic CM, McDonald SP, McCredie MRE et al Cancer incidence before and after kidney transplantation. JAMA 2006; 296: 2823–31. [DOI] [PubMed] [Google Scholar]
- 2. Wong G, Hayen A, Chapman JR et al Association of CKD and cancer risk in older people. J. Am. Soc. Nephrol. 2009; 20: 1341–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Liang J‐A, Sun L‐M, Yeh J‐J, Sung F‐C, Chang S‐N, Kao C‐H. The association between malignancy and end‐stage renal disease in Taiwan. Jpn. J. Clin. Oncol. 2011; 41: 752–7. [DOI] [PubMed] [Google Scholar]
- 4. Russo P. End stage and chronic kidney disease: Associations with renal cancer. Front. Oncol. 2012; 2: 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Lin MY, Kuo MC, Hung CC et al Association of dialysis with the risks of cancers. PLoS One 2015; 10: e0122856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Maisonneuve P, Agodoa L, Gellert R et al Cancer in patients on dialysis for end‐stage renal disease: An international collaborative study. Lancet 1999; 354: 93–9. [DOI] [PubMed] [Google Scholar]
- 7. Lai M‐N, Wang S‐M, Chen P‐C, Chen Y‐Y, Wang J‐D. Population‐based case–control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010; 102: 179–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wang S‐M, Lai M‐N, Chen P‐C, Wang J‐D. Increased risk of urothelial cancer in young and middle aged patients with end‐stage renal disease. J. Formos. Med. Assoc. 2015; 114: 52–7. [DOI] [PubMed] [Google Scholar]
- 9. Yang W‐C, Hwang S‐J, Taiwan Society of Nephrology . Incidence, prevalence and mortality trends of dialysis end‐stage renal disease in Taiwan from 1990 to 2001: The impact of national health insurance. Nephrol. Dial. Transplant. 2008; 23: 3977–82. [DOI] [PubMed] [Google Scholar]
- 10. Lin H‐F, Li Y‐H, Wang C‐H, Chou C‐L, Kuo D‐J, Fang T‐C. Increased risk of cancer in chronic dialysis patients: A population‐based cohort study in Taiwan. Nephrol. Dial. Transplant. 2011; 27: 1585–90. [DOI] [PubMed] [Google Scholar]
- 11. Shebl FM, Warren JL, Eggers PW, Engels EA. Cancer risk among elderly persons with end‐stage renal disease: A population‐based case–control study. BMC Nephrol. 2012; 13: 65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ou J‐H, Pan C‐C, Lin JS‐N et al Transitional cell carcinoma in dialysis patients. Eur. Urol. 2000; 37: 90–4. [DOI] [PubMed] [Google Scholar]
- 13. Weng S‐F, Chiu Y‐H, Jan R‐L et al Death does matter—Cancer risk in patients with end‐stage renal disease: A Nationwide population‐based study with competing risk analyses. Medicine 2016; 95: e2512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Winkelmayer WC, Schneeweiss S, Mogun H, Patrick AR, Avorn J, Solomon DH. Identification of individuals with CKD from Medicare claims data: A validation study. Am. J. Kidney Dis. 2005; 46: 225–32. [DOI] [PubMed] [Google Scholar]
- 15. Cheng C‐L, Lee C‐H, Chen P‐S, Li Y‐H, Lin S‐J, Y‐H KY. Validation of acute myocardial infarction cases in the national health insurance research database in Taiwan. J. Epidemiol. 2014; 24: 500–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Mohammad KA, Bari W. Fine and gray competing risk regression model to study the cause‐specific under‐five child mortality in Bangladesh. BMC Int. Health Hum. Rights 2017; 17: 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Chien C‐C, Han M‐M, Chiu Y‐H et al Epidemiology of cancer in end‐stage renal disease dialysis patients: A national cohort study in Taiwan. J. Cancer 2017; 8: 9–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Chow W‐H, Dong LM, Devesa SS. Epidemiology and risk factors for kidney cancer. Nat. Rev. Urol. 2010; 7: 245–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Kim HY, Yoo T‐H, Hwang Y et al Indoxyl sulfate (IS)‐mediated immune dysfunction provokes endothelial damage in patients with end‐stage renal disease (ESRD). Sci. Rep. 2017; 7: 3057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. González EA, Sachdeva A, Oliver DA, Martin KJ. Vitamin D insufficiency and deficiency in chronic kidney disease. Am. J. Nephrol. 2004; 24: 503–10. [DOI] [PubMed] [Google Scholar]
- 21. Eljaoudi R, Errasfa M, Benyahia M et al Copper, zinc and selenium imbalance in Moroccan haemodialysis patients and its correlation to lipid peroxidation. Int. J. Res. Med. Sci. 2017; 3: 2079–85. [Google Scholar]
- 22. Peces R. Malignancy and chronic renal failure. Saudi J. Kidney Dis. Transpl. 2003; 14: 5. [PubMed] [Google Scholar]
- 23. Weng P‐H, Hung K‐Y, Huang H‐L, Chen J‐H, Sung P‐K, Huang K‐C. Cancer‐specific mortality in chronic kidney disease: Longitudinal follow‐up of a large cohort. Clin. J. Am. Soc. Nephrol. 2011: CJN. 09011010; 6: 1121–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Szenajch J, Wcislo G, Jeong J‐Y, Szczylik C, Feldman L. The role of erythropoietin and its receptor in growth, survival and therapeutic response of human tumor cells: From clinic to bench—A critical review. Biochim. Biophys. Acta. 2010; 1806: 82–95. [DOI] [PubMed] [Google Scholar]
- 25. Tsai CC, Wu CL, Kor CT et al Prospective associations between environmental heavy metal exposure and renal outcomes in adults with chronic kidney disease. Nephrology (Carlton) 2018; 23: 830–6. [DOI] [PubMed] [Google Scholar]
- 26. Tsai T‐C, Chen Y‐C, Lo C‐W et al Incidence and renal survival of ESRD in the young Taiwanese population. Clin. J. Am. Soc. Nephrol. 2014; 9: 302–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Saini SD, van Hees F, Vijan S. Smarter screening for cancer: Possibilities and challenges of personalization. JAMA 2014; 312: 2211–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Mondaini N, Palli D, Saieva C et al Clinical characteristics and overall survival in genitourinary sarcomas treated with curative intent: A multicenter study. Eur. Urol. 2005; 47: 468–73. [DOI] [PubMed] [Google Scholar]
- 29. Momin BR, Pinheiro PS, Carreira H, Li C, Weir HK. Liver cancer survival in the United States by race and stage (2001‐2009): Findings from the CONCORD‐2 study. Cancer 2017; 123: 5059–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Farivar‐Mohseni H, Perlmutter AE, Wilson S, Shingleton WB, Bigler SA, Fowler JE Jr. Renal cell carcinoma and end stage renal disease. J. Urol. 2006; 175: 2018–21. [DOI] [PubMed] [Google Scholar]
- 31. Taneja S, Mandayam S, Kayani ZZ, Kuo YF, Shahinian VB. Comparison of stage at diagnosis of cancer in patients on dialysis versus the general population. Clin. J. Am. Soc. Nephrol. 2007; 2: 1008–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Holley JL. Screening, diagnosis, and treatment of cancer in long‐term dialysis patients. Clin. J. Am. Soc. Nephrol. 2007; 2: 604–10. [DOI] [PubMed] [Google Scholar]
- 33. Wong PN, Fung TT, Mak SK et al Hepatitis B virus infection in dialysis patients. J. Gastroenterol. Hepatol. 2005; 20: 1641–51. [DOI] [PubMed] [Google Scholar]
- 34. Henderson WA, Shankar R, Gill JM et al Hepatitis C progressing to hepatocellular carcinoma: The HCV dialysis patient in dilemma. J. Viral Hepat. 2010; 17: 59–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Krok‐Schoen JL, Fisher JL, Stephens JA et al Incidence and survival of hematological cancers among adults ages >/=75 years. Cancer Med. 2018; 7: 3425–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Descatha A, Jenabian A, Conso F, Ameille J. Occupational exposures and haematological malignancies: Overview on human recent data. Cancer Causes Control 2005; 16: 939–53. [DOI] [PubMed] [Google Scholar]
- 37. Gucalp A, Noy A. Spectrum of HIV lymphoma 2009. Curr. Opin. Hematol. 2010; 17: 362–7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig. S1 (a) Comparison of life expectancy between the general population and patients with end‐stage renal disease undergoing chronic dialysis in Taiwan. (b) Comparison of life expectancy among haemodialysis, peritoneal dialysis, and transplant patients in Taiwan.
Table S1 List of the International Classification of Disease, Ninth Revision, Clinical modification (ICD‐9‐CM) diagnostic and procedure codes.