

Abstract
Aim
The aim of this review was to synthesize empirical evidence of family factors associated with participation of children with disabilities aged 5 to 12 years to inform the development of family‐centred participation‐fostering interventions.
Method
A systematic search was performed for articles published in English between 2001 and 2017 in MEDLINE, PsycINFO, CINAHL, Scopus, and ASSIA following the Preferred Reporting Items for Systematic Review and Meta‐Analysis (PRISMA) guidelines. Quality of evidence was appraised using the Research Triangle Institute Item Bank. Family factors associated with participation were identified and assessed using a multistage ‘semi‐quantitative’ approach.
Results
Thirty studies were included in the review. Four non‐modifiable ‘status’ factors consistently associated with participation were parental ethnicity, parental education, family type, and family socio‐economic status. Six modifiable ‘process’ factors with consistent associations with participation were parental mental and physical health functioning, parental self‐efficacy beliefs, parental support, parental time, family preferences, and activity orientation.
Interpretation
Rehabilitation professionals should direct their focus towards modifiable family factors as primary targets for family‐centred interventions. Strategies that can improve families’ access to information, counselling, and community support services are likely to support children's participation by empowering families and optimizing their health and well‐being.
What this paper adds
Non‐modifiable ‘status’ and modifiable ‘process’ factors are important in participation of children with disabilities.
Disadvantaged family circumstances shaped by status factors are associated with reduced participation.
Key process factors for intervention are parental mental and physical health and parental self‐efficacy beliefs.
Other important process factors for intervention are parental support and time, family preferences, and activity orientation.
What this paper adds
Non‐modifiable ‘status’ and modifiable ‘process’ factors are important in participation of children with disabilities.
Disadvantaged family circumstances shaped by status factors are associated with reduced participation.
Key process factors for intervention are parental mental and physical health and parental self‐efficacy beliefs.
Other important process factors for intervention are parental support and time, family preferences, and activity orientation.
This article is commented on by Anaby and Pozniak on page https://doi.org/10.1111/dmcn.14156 of this issue.
This article's abstract has been translated into Spanish and Portuguese.
Follow the links from the http://onlinelibrary.wiley.com/doi/10.1111/dmcn.14133/abstract to view the translations.
Factores familiares asociados con la participación de niños con discapacidad: un estudio sistemático
OBJETIVO
El objetivo de esta revisión fue sintetizar la evidencia empírica de los factores familiares asociados con la participación de niños con discapacidad entre los 5 y 12 años para informar el desarrollo de intervenciones que fomentan la participación centrada en la familia
METODO
Una búsqueda sistemática fue realizada en artículos publicados en ingles entre 2001 y 2017 en MEDLINE, PsycINFO, CINAHL, Scopus, y ASSIA de acuerdo con los items reportados preferentes para guías de Búsqueda Sistemática y Meta‐Análisis. La calidad de la evidencia fue evaluada utilizando el Banco de Items del Research Triangle Institute (RTI). Fueron identificados los factores familiares asociados con la participación y evaluados utilizando un enfoque semicuantitativo de varias etapas.
RESULTADOS
Fueron incluidos 30 estudios en esta revisión. Cuatro factores no modificables de ¨estado¨ asociados sistemáticamente con la participación fueron la etnia de los padres, el nivel de educación de los padres, el tipo de familia, y el estatus socioeconómico de las familias. Seis factores de ¨proceso ¨modificables con asociaciones consistentes con la participación fueron el funcionamiento de salud física y mental de los padres, creencia de autoeficacia de los padres, soporte parenteral, tiempo de los padres, preferencias familiares, y orientación a la actividad.
INTERPRETACION
Los profesionales de la rehabilitación deben dirigir su foco hacia los factores modificables como objetivo primario para las intervenciones centradas en la familia. Estrategias que puedan mejorar el acceso de las familias a la información , asesoramiento, y servicios de apoyo comunitario que apoyen la participación de los niños y empoderar a las familias y optimizar su salud y bienestar.
RESUMO
Fatores familiares associados com participação em crianças com incapacidades: uma revisão sistemática
OBJETIVO
O objetivo desta revisão foi sintetizar a evidência empírica de fatores familiares associados com participação de crianças com incapacidades de 5 a 12 anos para informar o desenvolvimento de intevenções centradas na família que promovam a participação.
MÉTODO
Uma busca sistemática foi realizada por artigos publicados em ingles entre 2001 e 2007 na Medline, PsycINFO, CINAHL, Scopus, e ASSIA seguindo as diretrizes para Itens preferidos a serem reportados em revisões sistemáticas. A qualidade da evidência foi avaliada usando o Banco de Itens Do Institututo do Triângulo das Pesquisas (ITR). Fatores familiares associados à participação foram identificados e avaliados usando uma abordagem semi‐quantitativa multi‐estágios.
RESULTADOS
Trinta estudos foram incluídos na revisão. Quatro fatores com estado “não‐modificável” consistentemente associados com participação foram etnia parental, educação parental, tipo de família e situação sócio‐econômica da família. Seis fatores de “processo” modificáveis com associações consistentes com participação foram saúde e funcionamento mental e físico dos pais, auto‐eficácia parental, apoio parental, tempo parental, preferências familiares e orientacões para atividades.
INTERPRETAÇÃO
Profissionais de reabilitação devem direcionar o foco para fatores familiares potencialmente modificáveis como alvos primários para intervenções centradas na família. Estratégias que podem melhorar o acesso da família a informação, aconselhamento e serviços de suporte na comunidade têm probabilidade de apoiar a participação da criança por empoderar famílias e otimizar sua saúde e bem estar.
Abbreviation
- RTI
Research Triangle Institute
The benefits of participation for physical and psychological health and well‐being of children with disabilities are well established.1, 2 Participation, broadly defined as ‘involvement in a life situation’,3 is linked to children's growth and development, and enables experiences of meaning and purpose.1, 4, 5 Optimizing participation of children with disabilities is an outcome desired by parents6, 7 and a primary goal of rehabilitation services.5 However, children with disabilities participate less frequently and in a narrower range of activities, and are generally less involved when they do participate compared to their peers without disabilities.7, 8, 9, 10 As a result, children with disabilities may lack the benefits linked to participation.
The need to identify effective interventions to foster children's participation is an urgent priority. Better knowledge about factors contributing to children's participation and interdependencies between them is central for informing participation‐fostering interventions. Previous reviews have examined personal and environmental factors that affect participation of children with disabilities.11, 12, 13, 14, 15, 16, 17 The most commonly identified factors were child age, sex, skills and functional abilities, preferences and enjoyment, parental values and preferences, supports and acceptance from others, and accessibility of physical environment.11, 12, 13, 14, 15, 16, 17 However, these reviews have described the influence of a wide range of factors on participation in specific activities11, 15, 17 or settings,14 focused predominantly on children with physical disabilities11, 13, 15, 17 or provided a narrative evaluation of the findings.11, 13, 14, 15, 16
Skills and competences shape participation, and are shaped by participation in safe and supportive life situations.4 Family plays a central role in facilitating children's skills and competence development.4, 18, 19, 20 During middle childhood (defined as ages 5–12y), a child's mastery of developmental challenges is strongly influenced by family experiences and dynamics of relationships among family members.21, 22 Differences in family experiences produce important variations in children's participation, which affect children's life experiences in and beyond this developmental period.21, 22 It is thus important to focus on the family unit and better understand family/parental factors contributing to children's participation,23, 24 especially in middle childhood. Better knowledge about family factors consistently associated with participation of children with disabilities will support the development of participation‐fostering family‐centred interventions. The current review therefore aimed to: (1) offer an up‐to‐date, targeted synthesis of empirical evidence of family factors associated with participation; and (2) assess the relative strength and consistency of these associations in children with disabilities aged 5 to 12 years.
Method
The Preferred Reporting Items for Systematic Review and Meta‐Analysis (PRISMA) guidelines25 was used for this review. A protocol was developed a priori and published in the database of prospectively registered systematic reviews (http://www.crd.york.ac.uk/PROSPERO; registration number: CRD42017078202).
Search strategy and screening
A systematic search was performed by a single researcher (SA) for articles published in English between January 2001 and September 2017 in MEDLINE (EBSCO), PsycINFO (EBSCO), CINAHL (EBSCO), Scopus (ProQuest), and ASSIA (ProQuest). Restrictions to the publication date were applied to capture the literature reflective of the World Health Organization's International Classification of Functioning, Disability and Health for Children and Youth3 conceptualization of participation as a health indicator influenced by a dynamic interaction between multiple factors unique to the child and the attitudinal, social, and physical environment. Search terms were determined after the detailed assessment of indexing terms applied to a ‘known’ set of articles meeting inclusion criteria for the review26 and finalized with an information specialist. A combination of subject headings and free‐text terms for disability, age of participants, participation, family factors, and study design was applied. The detailed search strategy for MEDLINE is supplied (Fig. S1, online supporting information). Additional studies were identified by a manual search of the reference lists of included articles and contents pages of Developmental Medicine and Child Neurology; Archives of Physical Medicine and Rehabilitation; Disability and Rehabilitation; Child: Care, Health and Development; and Research in Developmental Disabilities published from January 2012 to September 2017.
Initial electronic search yielded 2547 published articles. After removal of duplicates, 1532 titles and abstracts were screened for relevance by two independent researchers (SA and EC), resulting in 40 full‐text articles retrieved for further eligibility assessment. Twenty‐five articles corresponding to 21 individual studies met the inclusion criteria. Discrepancies in the agreement were resolved by consensus. A manual search identified additional nine studies (Fig. S2, online supporting information).
Articles were limited to peer‐reviewed publications in English aiming to establish the relationship between family factors and participation of children with disabilities aged 5 to 12 years (mean age <12y). Presence of disability was identified through diagnosis presented in the article or identification of other health or educational support provisions. To ensure inclusion of a wide range of articles, the International Classification of Functioning, Disability and Health for Children and Youth's conceptualization of participation as the child's ‘involvement in child‐relevant life situations’ was applied. Articles that considered known participation measures or in which participation items captured any combination of the International Classification of Functioning, Disability and Health for Children and Youth's nine Activities and Participation domains3 were included. Family factors were defined as factors pertinent to the parents or family unit as a whole including any socio‐demographic, psychological, behavioural, and parental health related factors. Only observational studies (i.e. prospective and retrospective cohort, case‐control, cross‐sectional) that reported quantitative evidence on associations of interest were included. Articles were excluded if they focused only on: (1) typically developing children, (2) wider community (e.g. neighbours or peers), (3) children's quality of life, behavioural difficulties, or (4) results were from case studies, conference posters, commentaries, or other grey literature.
Data extraction
Data extraction was performed using a standardized, prepiloted data extraction form by two researchers (SA and EC) independently. The following details were extracted: (1) generic information: study author(s), years of publication; (2) data describing study aims, design, and population; (3) details on family factors and participation outcome explored (i.e. activity types, settings, dimensions); and (4) study results and information for the assessment of the risk of bias. For studies including both children with and without disabilities of a wider age group, results pertinent to children with disabilities in the targeted age group were extracted unless no segregation of findings based on disability status and age group was provided.
Quality appraisal
Quality appraisal was performed by two independent researchers (SA and EC) using the adapted version of the Research Triangle Institute (RTI) Item Bank.27 The RTI Item Bank captures all the domains critical for evaluating observational studies and allows customization from the investigator based on research needs. The RTI Item Bank has high interrater reliability27 and has been previously used to assess the risk of bias and precision of observational studies.28, 29 The original RTI 29‐item tool was adapted to fit the review objectives. The tailored RTI 14‐item tool assessed the selection bias, detection bias, attrition bias, selective outcome reporting, confounding, and validity of interpretation of studies (Table SI, online supporting information). Possible response categories to each item were combinations of ‘yes’, ‘no’, ‘partially’, ‘cannot determine’, and ‘not applicable’. For ease of interpretation, the categories ‘cannot determine’ and ‘partially’ were collapsed into the ‘unclear risk of bias’ category. Agreement between two researchers was assessed by a joint probability agreement. All the discrepancies in opinion were resolved by consensus.
Data analysis
Meta‐analysis was not feasible because of significant heterogeneity in study designs, family factors and participation activity types, settings, and dimensions measured. There was also incomplete reporting of findings (e.g. in some cases only significant results were reported) and statistics necessary for calculation of Pearson's zero‐order correlation coefficients or alternative effect sizes.30, 31 Attempts to obtain required statistical information resulted in only a few corresponding authors acknowledging the receipt of data requests. Direct combination of standardized regression beta coefficients30 was not appropriate because of substantial variations in covariates31 in each multivariate model. Imputation of missing Pearson's zero‐order correlations using the existing standardized regression beta coefficients32 was not considered because this approach results in biased findings.33
Results were therefore synthesized and interpreted by a single researcher (SA) using a multistage ‘semi‐quantitative’ approach.17, 34 If meta‐analysis is not possible, such an approach is superior to narrative reporting because it provides objective evidence on strength, direction, and consistency of associations.17 First, family factors assessing the same underlying construct but using different terms to describe it were combined into a single identifying factor (Table SII, online supporting information). Second, factors were classified into two major groups adapted from previous literature:35, 36 family ‘status’ and family ‘process’ factors. Third, for family factors examined by two or more studies two parameters were calculated:17, 34 (1) the number of studies that attempted to establish relationships between family factors and participation; and (2) the number of studies that established the relationship as significant (p<0.05). Then, the percentage of studies supporting the established relationship with participation was computed by dividing the number of studies that established a significant relationship by the total number possible. From the obtained percentage value, it was determined whether the family factor and participation outcome had a positive or negative association, inconsistent association, or no association. Family factors were considered to be associated with participation if at least 60 per cent of studies supported the established associations with the outcome.17, 34 The rules of classifying the consistency of evidence were adapted from previous research17, 34 and are summarized in Table 1.
Table 1.
Rules of classifying the strength of evidence (adapted from Sallis et al.)34
| % of studies supporting association | Coding | Code meaning |
|---|---|---|
| 0–33 | 0 | No association |
| 34–59 | ? | Inconsistent association |
| 60–100 | + | Positive association |
| – | Negative association |
Double summary codes ‘++’, ‘– –’, ‘00’ are applied when three or more studies support a positive/negative association or no association, and ‘??’ is applied to show that the factor has been studied frequently but findings are inconsistent.
Results
Thirty studies were included in the review. The detailed description of characteristics of these studies is supplied in Table SIII (online supporting information). Before 2010, only six articles18, 24, 37, 38, 39, 40 reporting on four unique samples of children with disabilities met our inclusion criteria. Six studies shared samples,9, 41, 42, 43, 44, 45 but differed substantially in the methodology and sample subgroups. These were retained as individual studies. Studies were conducted in Europe (n=9), Canada (n=7), United States (n=5), collaboratively between Canada and United States (n=2), Australia (n=4), and Israel (n=3). Except four longitudinal studies,24, 43, 44, 46 all studies used cross‐sectional design.
Quality appraisal
Most of the studies described the study populations and selection in sufficient detail. One study was at high risk of bias because of study subgroups incomparability by age.47 Eight studies included a convenience sample and were at unclear risk of selection bias. Study sample size ranged from 23 to 77 470 (weighted). None of the studies with a sample size of 67 or lower37, 39, 43, 48, 49, 50 provided sufficient justification on the adequacy of proposed sample sizes, hence, were rated at unclear risk of bias in external validity and precision. Measures used to collect data on family factors varied (Table SIII). Two studies, however, did not provide descriptions on how these data were obtained.9, 52 Participation was assessed using seven measurement tools (Table SIV, online supporting information) with the Children's Assessment of Participation and Enjoyment53 being the most frequently used measure. Six studies did not report on validity and reliability of the participation measures used and were rated at unclear risk of bias.51, 54, 55, 56, 57, 58 Out of four studies with longitudinal designs, one study was at high risk of attrition bias,43 while the remaining studies provided insufficient information to assess the attrition rate. Six studies provided inadequate adjustment for confounding variables in their analysis and were at unclear risk of bias. Taking into account the individual study's limitations, the findings were considered credible in 24 studies and partially credible in six of the included studies (Table SV, online supporting information). Nevertheless, no study was excluded from data synthesis. The agreement in the quality appraisal between two researchers was high (78%).
Family factors
This review identified findings in two major groups of family factors: ‘status’ and ‘process’ as illustrated in Figure 1. This taxonomy differentiates modifiable family process factors (what families experience and do) from non‐modifiable status factors (who families are).35, 36
Figure 1.
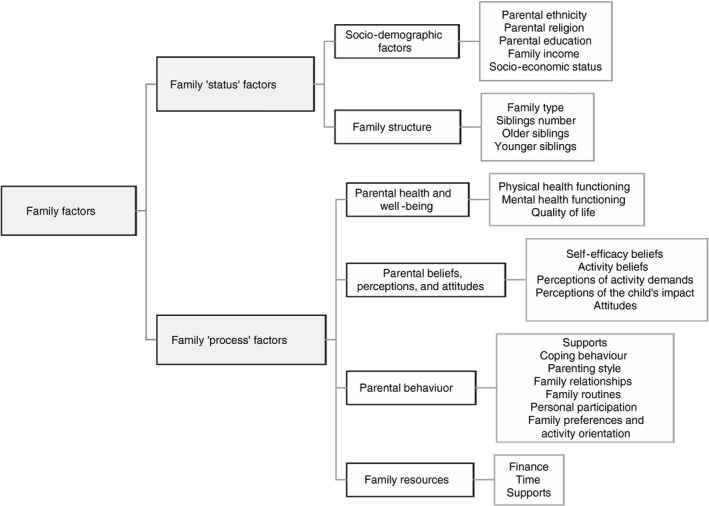
A taxonomy of family factors examined by the included studies
The review distinguished two subgroups of status factors: (1) family socio‐demographic factors and (2) family structure; and four subgroups of process factors: (1) ‘parental health and well‐being’, (2) ‘parental beliefs, perceptions, and attitudes’, (3) ‘parental behaviour’, and (4) ‘family resources’ (for details on how some factors were collapsed into a single identifying factor within each subgroup refer to Table SII. Evidence of the measures of association between each factor and participation dimensions, activity domains, and settings is summarized in Table SIII. Table 2 shows a summary of evidence on the consistency of associations for family factors examined in at least two studies (for the assessment rules refer to Table 1). The sections below describe the main findings. Associations that were studied most often are discussed first.
Table 2.
Summary of family factors potentially associated with participation of children with disabilities
| Family factors | Number of studiesa | Related to participation | Not related to participation | Coding | ||
|---|---|---|---|---|---|---|
| Number of studiesb | Direction of associationc | Number of studiesd | % of studies supporting associatione | Associationf | ||
| Family status factors | ||||||
| Family socio‐demographic factors | ||||||
| Family incomeg | 12 | 740, 47, 49, 52, 54, 60, 79 | + | 519, 39, 56, 58, 62 | 58 | ?? |
| Parental education | 11 | 89, 40, 45, 47, 48, 50, 59, 60 | + | 319, 37, 44 | 73 | ++ |
| Socio‐economic status | 7 | 546, 48, 50, 55, 61 | + | 238, 43 | 71 | ++ |
| Parental ethnicity | 4 | 324, 46, 55 | − | 150 | 75 | − |
| Family structure | ||||||
| Family type (single‐parent) | 5 | 340, 55, 62 | − | 238, 50 | 60 | −− |
| Number of siblings | 2 | 237, 58 | 0 | |||
| Family process factors | ||||||
| Parental health and well‐being | ||||||
| Mental health functioning | 7 | 537, 39, 42, 43, 58 | + | 224, 59 | 71 | ++ |
| Physical health functioning | 2 | 224, 58 | +/− | 100 | +/− | |
| Parental beliefs, perceptions, and attitudes | ||||||
| Self‐efficacy beliefs | 3 | 250, 60 | + | 137 | 67 | + |
| Attitudes | 2 | 141 | + | 164 | 50 | ? |
| Perception of child's impact | 2 | 159 | + | 137 | 50 | ? |
| Parental behaviour | ||||||
| Supports (for the child) | 5 | 341, 57, 62 | + | 218, 64 | 60 | ++ |
| Family preferences and activity orientation | 2 | 218, 19 | + | 100 | ++ | |
| Family relationships | 2 | 218, 19 | 0 | |||
| Coping behaviour | 2 | 239, 43 | 0 | |||
| Family resources | ||||||
| Supports (for the family) | 3 | 158 | + | 243, 56 | 33 | 0 |
| Time | 2 | 258, 59 | + | 100 | + | |
aThe number of studies examined a particular association. bThe number of studies established an association as being significant (p<0.05). cThe prevailing direction of an association based on the frequency count. dThe number of studies that established an association as being insignificant. eThe percentage of studies supporting an association. fDouble summary codes ‘++’, ‘– –’ were applied when three or more studies supported a positive or negative association and ‘??’ when the factor was studied frequently but findings were inconsistent. Code ‘+/−’ was applied when studies differed in respect to the direction of established association. gThirteen studies examined the effect of income on participation; but two studies40, 80 shared the sample of children with disabilities and hence were counted as one study.
Socio‐demographic factors
Family income was studied most frequently, but findings showed inconsistent association with participation (Table 2). Parental education was consistently associated with participation with lower education predicting reduced participation.9, 40, 45, 48, 59, 60 However, in two studies,47, 50 higher education predicted reduced participation. Lower socio‐economic status46, 48, 50, 55, 61 was consistently associated with reduced participation. Hispanic ethnicity increased risk for non‐participation in organized activities,55 and having ethnicity other than white was associated with decreased participation in leisure activities.24 Indigenous Australian ethnicity was positively associated with participation in a single study.46 Parental religion was examined in a single study with no association with participation reported.50
Family structure
Family type was studied most frequently. Living in a single‐parent family was consistently associated with decreased participation in leisure activities.40, 55, 62 No study showed a significant association between a number of siblings and participation. The presence of an older or a younger sibling in the household was examined, each in a single study. The relationship was established only between the presence of an older sibling and participation in more household tasks for children with attention‐deficit/hyperactivity disorder.37
Parental health and well‐being
Parental mental health functioning, defined as a state of psychological, social, emotional well‐being in which parents can realize their potential and cope with the stresses of life,63 was the most frequently studied factor and the one consistently associated with participation. Parental stress was associated with reduced participation of children with cerebral palsy in leisure activities.39, 42, 43 Higher parental stress was also associated with reduced assistance provided to children with attention‐deficit/hyperactivity disorder to support their participation.37 Children of parents with better mental health functioning had better participation in interpersonal relationships.58 Parental physical functioning was consistently associated with participation, but the direction of associations varied across disabilities. A positive association was established for social participation of children with Down syndrome58 and a negative association for participation of children with physical disabilities in recreational activities.24 Parental quality of life was examined in a single study with a positive association established for participation in informal leisure activities.43
Parental beliefs, perceptions, and attitudes
Parental self‐efficacy beliefs were studied most often showing consistent positive association with participation.50, 60 Attitudes of family/greater community41, 64 and parental perceptions of the child's impact on the family37, 59 were associated with participation inconsistently (Table 2). Parental beliefs about activity and perceptions of activity demands were examined in a single study.51 Children of parents who shared negative beliefs about activity (e.g. physical activity too overstimulating) and perceived it to be difficult to make required arrangements for their children participated in fewer physical activities.51
Parental behaviour
Supports for the child from parents/greater community was studied most often.18, 41, 57, 62, 64 The presence of parental support was consistently positively associated with participation,41, 57 except in a single study where the association was negative.62 Family preferences18, 19 and activity orientation18, 19, 43 towards social and recreational activities were positively associated with children's participation in leisure activities. Parental coping behaviour39, 43 and family relationships (cohesion/conflict)18, 19 were not related to participation. Parenting style, parents’ personal participation, and family routines were examined, each in a single study. A positive relationship was established between parental prioritization of family routines and participation of children with attention‐deficit/hyperactivity disorder in household tasks.37 Negative parenting style59 and parents’ personal participation43 were not related to participation.
Available resources
Supports for the family were examined most frequently but no conclusive evidence was found to support an association with participation. Studies examining the effect of parental time availability on participation revealed a consistent positive association.58, 59 Absence of financial and time impact on family (measured as a single construct) was examined in a single study with no association with participation established.18 Another study, however, revealed significant differences between parents of children with disabilities compared to parents of typically developing peers in respect to finance and time being usually insufficient/inadequate to support their children's participation in the community.7
Discussion
This systematic review summarized the evidence for family factors associated with participation of children with disabilities aged 5 to 12 years. Family factors identified in the review were grouped according to a taxonomy which distinguishes non‐modifiable status factors from modifiable process factors. Status factors consistently associated with participation were parental ethnicity, parental education, family type, and socio‐economic status. Process factors with consistent associations were parental mental and physical health functioning, parental self‐efficacy beliefs, parental support, parental time, family preferences, and activity orientation. Implications of the key findings are discussed from theoretical, practical, and research perspectives.
In line with findings of previous research,11, 13, 16 this review found consistent relationships between family socio‐economic disadvantage, parental mental and physical health functioning, and children's participation. There is strong theoretical support65 for the role of socio‐economic disadvantage in influencing children's outcomes through parental mental health and quality of interpersonal relationships. The family stress model65 suggests that parental psycho‐emotional problems (stress, anxiety, depression), triggered or exacerbated by a lack of material resources, have a direct negative impact on marital relationships. Accumulated tension from interpersonal problems ‘splits over’ into parent–child interaction and manifests itself in the form of negative or punitive parenting.65 Negative parental practices are associated with significant developmental difficulties for children, including behavioural problems, physical health difficulties, and problems in interpersonal relationships.66 These developmental difficulties are linked to reduced participation.1
Further, parental mental and physical health problems undermine parents’ confidence in their ability to successfully raise children, commonly referred to as parental self‐efficacy beliefs.67 Parents with low self‐efficacy beliefs are less likely to adopt effective parenting behaviour67 and provide safe and positive life situations for their children to participate in.50 This in turn may reinforce perceptions of low self‐efficacy beliefs and increase emotional tension in parents.67
It is important to consider that there may be a causal feedback loop. Parental stress and lower self‐efficacy beliefs might be caused by having and/or caring for a child with disability. Evidence suggests that parents, especially mothers of children with disability, are at increased risk of poor mental68, 69 and physical health functioning.69 This is a result of parental lack of ability to cope effectively with stressors caused by the demands of the child's illness.70
Given the importance of effective coping strategies in managing daily stressors, developing parental competence and their resilience might be promising targets for family‐centred rehabilitation. Further, based on evidence suggesting the effectiveness of direct support strategies in lowering stress levels in families,71 informing parents and referring them to existing counselling services, social parental networks, and respite services are important considerations.
Similar to previous reviews,11, 17 this review has identified that family preferences and activity orientation are important for children's participation. Families that are better oriented towards intellectual activities and participate more intensely in social‐recreational activities create more opportunities for their children's direct involvement in activities18, 19 and competence development for future participation. Given that parents are the planners of family routines,20, 72, 73 and behaviour is informed by knowledge, beliefs, and attitudes,20, 72 rehabilitation professionals may consider educating parents on the development of consistent family routines oriented towards active participation in recreational activities.
It was found that disadvantaged family circumstances (ethnic minority status, material, social, and educational deprivation) were associated with reduced participation. These findings were supported by large‐scale survey data and are consistent with the results of previous reviews.11, 13 Social disadvantage appears to affect participation irrespective of children's disability type and health support needs. Socio‐economically disadvantaged and single‐parent families face greater challenges in meeting the child's and family immediate needs within limited financial and time resources.74 Limited resources make it harder for parents to provide children with opportunities and experiences. Persistent lack of resources is also disruptive for parental psychological functioning and cohesive family relationships, and can result in less affectionate and more aggressive family climates.65 The latter negatively affects children's well‐being,65 their beliefs of what they can accomplish, and their beliefs in what they can become.66
It appears that disadvantaged families encounter stressors associated with their family situations (financial and time tension, inequalities, limited knowledge, inability to seek for needed services) which affect parental attitudes and behaviour and may account for the risk to children's well‐being and participation. While such circumstances are hard to modify, rehabilitation professionals may monitor disadvantaged families for factors amenable to change. Additionally, improving parental access to information (e.g. informing them of low‐cost or free‐of‐charge activities), community support programmes, financial service/schemes, and childcare funds might ease the financial and time tension placed on families and support participation. Advocacy efforts directed towards promoting the rights of disadvantaged families with childhood disability can also educate local authorities/policy makers and help to create conditions necessary for positive reforms and reallocation of available resources for social integration and inclusion.
Review findings supported an association between parental support and participation. However, no association with participation was found for other indicators of family dynamics: family relationships (cohesion/conflict), attitudes, and parenting style. These findings appear counterintuitive. However, (1) the effect of these factors was not examined extensively, and (2) an absence of direct association does not imply no association. The effect of these factors might be mediated by the other factors directly affecting participation. Positive family dynamics (emotional bond, helpful and encouraging patterns of interaction between family members) is a distinctive feature of cohesive families. Families that display these characteristics participate more in recreational activities18 which predicts more intense participation.18 Further, cohesive families exercise effective parenting behaviour which is linked with children's positive development and their social and psycho‐emotional functioning66 – the predictors of more intense participation in leisure activities.18 Rehabilitation professionals can inform and educate parents about the importance of family cohesive relationships, positive parenting, provision of supports, and opportunities in facilitating children's abilities to support participation in daily activities.
This review did not find a consistent association between family income and participation. This contradicts previous research13, 14, 16, 23 and earlier findings of this review that socio‐economic disadvantage is a barrier to participation. There is, however, evidence suggesting that income in isolation may not be an effective indicator of economic disadvantage. Low income infers economic disadvantage rather than directly measuring it,75 and it reveals little about real‐life experiences. High‐income families can still experience economic disadvantage through uncontrolled consumption or poor distribution of resources.76 Equally, low‐income families may be resource rich or have measures in place to alleviate disadvantage (e.g. through borrowing). It is difficulties meeting needs on available financial resources, gradually accumulating debt and ‘money worries’ that make families economically vulnerable.77
Future research
Results were derived from studies having predominantly cross‐sectional designs. Prospective studies are needed to confirm findings. Except in six studies, the remaining studies examined participation in leisure and recreational activities. Research on participation in other settings, particularly school, is required. Research modelling the relationships between socio‐economic disadvantage, parental mental and physical functioning, children's developmental outcomes, and participation using national longitudinal cohort data sets will help to identify and understand the factors across different international contexts. Findings also highlight the need for research on family dynamics and participation. Future research should consider measuring family economic vulnerability alongside family income to allow objective evaluations of economic disadvantage.
Strengths and limitations
This is the first review to systematically examine associations between family factors and participation in children with various disabilities aged 5 to 12 years. The review adhered to the PRISMA guidelines to ensure transparency and rigour in methodology. A multistage ‘semi‐quantitative’ approach was used to analyse the data, thereby reporting objective evidence on the measures of associations. However, a few limitations should be acknowledged. Participation is a complex construct resulting from a dynamic relationship between a cluster of factors unique to the child, their family, and wider environment. This review targeted family/parental factors only and as such did not extract and assess the effect of other factors important to participation. The selection of papers was restricted to those published in peer‐reviewed journals in English, which might have led to language and publication bias. Substantial heterogeneity in studies, selective reporting of findings, and incomplete reporting of essential statistics precluded correlational meta‐analysis. The strengthening of standard methods of reporting of observational studies (e.g. STROBE statement)78 would improve the ability to compare different studies, and facilitate future meta‐analysis.
Conclusion
This review emphasized the role of family factors in shaping participation of children with disabilities. Family status and process factors were associated with participation, with varying effects across disabilities and participation activity domains. It appears that disadvantaged family circumstances shaped by status factors may predispose families to a variety of stressors. The way parents evaluate and deal with these stressors may adversely affect parental health and well‐being, their subjective perceptions and behaviour, which in turn can pose the risk to children's well‐being and participation. Family status factors are hard to modify; hence, rehabilitation professionals should prioritize process factors as primary targets of individually tailored, family‐centred interventions. Key process factors for intervention are parental mental and physical health functioning, parental self‐efficacy beliefs, parental support, parental time, and family preferences and activity orientation. Strategies that can improve families’ access to information, counselling services, parental support networks, and/or community support programmes are likely to support children's participation by empowering families and optimizing their health and well‐being. Additionally, advocacy efforts promoting the rights of families with childhood disability at local and national level can be helpful in reshaping existing policy interventions to meet families’ needs more effectively and thereby improve outcomes for children.
Supporting information
Figure S1: Search strategy.
Figure S2: Flow diagram detailing study selection process.
Table SI: Research Triangle Institute 14‐item tool
Table SII: Factors combined into a single identifying factor
Table SIII: Summary of included studies
Table SIV: Description of validated tools applied to measure participation
Table SV: Quality appraisal based on the customized Research Triangle Institute 14‐item tool
Acknowledgements
The authors wish to thank Eleanor Curnow for assisting with screening and quality appraisal of studies, and for her continuous support and encouragement. This research was completed as part of a PhD funded by Lothian National Health Service and Queen Margaret University, Edinburgh, UK. The authors have stated that they had no interests that might be perceived as posing a conflict or bias.
References
- 1. King G, Law M, King S, Rosenbaum P, Kertoy MK, Young NL. A conceptual model of the factors affecting the recreation and leisure participation of children with disabilities. Phys Occup Ther Pediatr 2003; 23: 63–90. [PubMed] [Google Scholar]
- 2. Humphry R, Wakeford L. An occupation‐centered discussion of development and implications for practice. Am J Occup Ther 2006; 60: 258–67. [DOI] [PubMed] [Google Scholar]
- 3. World Health Organization . International Classification of Functioning, Disability and Health for Children and Youth: ICF‐CY. Switzerland, Geneva: WHO, 2007. [Google Scholar]
- 4. Law M. Participation in the occupations of everyday life. Am J Occup Ther 2002; 56: 640–9. [DOI] [PubMed] [Google Scholar]
- 5. Kielhofner G. A Model of Human Occupation: Theory and Application. Philadelphia, PA: Lippincott Williams & Wilkins, 2002. [Google Scholar]
- 6. Benjamin TE, Lucas‐Thompson RG, Little LM, Davies PL, Khetani MA. Participation in early childhood educational environments for young children with and without developmental disabilities and delays: a mixed methods study. Phys Occup Ther Pediatr 2017; 37: 87–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bedell G, Coster W, Law M, et al. Community participation, supports, and barriers of school‐age children with and without disabilities. Arch Phys Med Rehabil 2013; 94: 315–23. [DOI] [PubMed] [Google Scholar]
- 8. Law M, Anaby D, Imms C, Teplicky R, Turner L. Improving the participation of youth with physical disabilities in community activities: an interrupted time series design. Aust Occup Ther J 2015; 62: 105–15. [DOI] [PubMed] [Google Scholar]
- 9. Ullenhag A, Krumlinde‐Sundholm L, Granlund M, Almqvist L. Differences in patterns of participation in leisure activities in Swedish children with and without disabilities. Disabil Rehabil 2014; 36: 464–71. [DOI] [PubMed] [Google Scholar]
- 10. Fauconnier J, Dickinson HO, Beckung E, et al. Participation in life situations of 8–12 year old children with cerebral palsy: cross sectional European study. BMJ 2009; 338: b1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Bult MK, Verschuren O, Jongmans MJ, Lindeman E, Ketelaar M. What influences participation in leisure activities of children and youth with physical disabilities? A systematic review Res Dev Disabil 2011; 32: 1521–9. [DOI] [PubMed] [Google Scholar]
- 12. Shields N, King M, Corbett M, Imms C. Is participation among children with intellectual disabilities in outside school activities similar to their typically developing peers? A systematic review Dev Neurorehabil 2014; 17: 64–71. [DOI] [PubMed] [Google Scholar]
- 13. Shikako‐Thomas K, Majnemer A, Law M, Lach L. Determinants of participation in leisure activities in children and youth with cerebral palsy: systematic review. Phys Occup Ther Pediatr 2008; 28: 155–69. [DOI] [PubMed] [Google Scholar]
- 14. Anaby D, Hand C, Bradley L, et al. The effect of the environment on participation of children and youth with disabilities: a scoping review. Disabil Rehabil 2013; 35: 1589–98. [DOI] [PubMed] [Google Scholar]
- 15. Bloemen MA, Backx FJ, Takken T, et al. Factors associated with physical activity in children and adolescents with a physical disability: a systematic review. Dev Med Child Neurol 2015; 57: 137–48. [DOI] [PubMed] [Google Scholar]
- 16. Tonkin BL, Ogilvie BD, Greenwood SA, Law MC, Anaby DR. The participation of children and youth with disabilities in activities outside of school: a scoping review. Can J Occup Ther 2014; 81: 226–36. [DOI] [PubMed] [Google Scholar]
- 17. Li R, Sit CHP, Yu JJ, et al. Correlates of physical activity in children and adolescents with physical disabilities: a systematic review. Prev Med 2016; 89: 184–93. [DOI] [PubMed] [Google Scholar]
- 18. King G, Law M, Hanna S, et al. Predictors of the leisure and recreation participation of children with physical disabilities: a structural equation modeling analysis. Child Health Care 2006; 35: 209–34. [Google Scholar]
- 19. Palisano RJ, Chiarello LA, Orlin M, et al. Determinants of intensity of participation in leisure and recreational activities by children with cerebral palsy. Dev Med Child Neurol 2011; 53: 142–9. [DOI] [PubMed] [Google Scholar]
- 20. Rentinck IC, Gorter JW, Ketelaar M, Lindeman E, Jongmans MJ. Perceptions of family participation among parents of children with cerebral palsy followed from infancy to toddler hood. Disabil Rehabil 2009; 31: 1828–34. [DOI] [PubMed] [Google Scholar]
- 21. Collins WA, Madsen SD, Susman‐Stillman A. Parenting during middle childhood In: Bornstein MH, editor. Handbook of Parenting (volume 1). Mahwah, NJ: Erlbaum, 2005: 73–101. [Google Scholar]
- 22. Wise S. Family Structure, Child Outcomes and Environmental Mediators: An Overview of the Development in Diverse Families Study. Melbourne, Victoria: Australian Institute of Family Studies, 2003. [Google Scholar]
- 23. Anaby D, Law M, Hanna S, Dematteo C. Predictors of change in participation rates following acquired brain injury: results of a longitudinal study. Dev Med Child Neurol 2012; 54: 339–46. [DOI] [PubMed] [Google Scholar]
- 24. King G, McDougall J, Dewit D, Petrenchik T, Hurley P, Law M. Predictors of change over time in the activity participation of children and youth with physical disabilities. Child Health Care 2009; 38: 321–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Moher D,Liberati A, Tetzlaff J, Altman DG; PRISMA Group . Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. Int J Surg 2010; 8: 336–41. [DOI] [PubMed] [Google Scholar]
- 26. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, 2011. [Google Scholar]
- 27. Viswanathan M, Berkman ND. Development of the RTI item bank on risk of bias and precision of observational studies. J Clin Epidemiol 2012; 65: 163–78. [DOI] [PubMed] [Google Scholar]
- 28. Galland B, Spruyt K, Dawes P, McDowall PS, Elder D, Schaughency E. Sleep disordered breathing and academic performance: a meta‐analysis. Pediatrics 2015; 136: e934–46. [DOI] [PubMed] [Google Scholar]
- 29. Senra H, Barbosa F, Ferreira P, et al. Psychologic adjustment to irreversible vision loss in adults: a systematic review. Ophthalmology 2015; 122: 851–61. [DOI] [PubMed] [Google Scholar]
- 30. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to Meta‐Analysis. Chichester, UK: John Wiley & Sons, 2011. [Google Scholar]
- 31. Cooper H. Research Synthesis and Meta‐Analysis: A Step‐by‐Step Approach. Thousand Oaks, CA: Sage Publications, 2016. [Google Scholar]
- 32. Peterson RA, Brown SP. On the use of beta coefficients in meta‐analysis. J Appl Psychol 2005; 90: 175–81. [DOI] [PubMed] [Google Scholar]
- 33. Roth PL, Le H, Oh IS, Van Iddekinge CH, Bobko P. Using beta coefficients to impute missing correlations in meta‐analysis research: reasons for caution. J Appl Psychol 2018; 103: 644–58. [DOI] [PubMed] [Google Scholar]
- 34. Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc 2000; 32: 963–75. [DOI] [PubMed] [Google Scholar]
- 35. Fan X, Chen M. Parental involvement and students’ academic achievement: a meta‐analysis. Edu Psych Rev 2001; 13: 1–22. [Google Scholar]
- 36. Christenson SL, Rounds T, Gorney D. Family factors and student achievement: an avenue to increase students’ success. Sch Psychol Q 1992; 7: 178. [Google Scholar]
- 37. Dunn L, Coster WJ, Cohn ES, Orsmond GI. Factors associated with participation of children with and without ADHD in household tasks. Phys Occup Ther Pediatrics 2009; 29: 274–94. [DOI] [PubMed] [Google Scholar]
- 38. Imms C, Reilly S, Carlin J, Dodd KJ. Characteristics influencing participation of Australian children with cerebral palsy. Disabil Rehabil 2009; 31: 2204–15. [DOI] [PubMed] [Google Scholar]
- 39. Majnemer A, Shevell M, Law M, et al. Participation and enjoyment of leisure activities in school‐aged children with cerebral palsy. Dev Med Child Neurol 2008; 50: 751–8. [DOI] [PubMed] [Google Scholar]
- 40. Law M, King G, King S, et al. Patterns of participation in recreational and leisure activities among children with complex physical disabilities. Dev Med Child Neurol 2006; 48: 337–42. [DOI] [PubMed] [Google Scholar]
- 41. Colver A, Thyen U, Arnaud C, et al. Association between participation in life situations of children with cerebral palsy and their physical, social, and attitudinal environment: a cross‐sectional multicenter European study. Arch Phys Med Rehabil 2012; 93: 2154–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Parkes J, McCullough N, Madden A. To what extent do children with cerebral palsy participate in everyday life situations? Health Soc Care Com 2010; 18: 304–15. [DOI] [PubMed] [Google Scholar]
- 43. Bult MK, Verschuren O, Lindeman E, et al. Predicting leisure participation of school‐aged children with cerebral palsy: longitudinal evidence of child, family and environmental factors. Child Care Health Dev 2013; 39: 374–80. [DOI] [PubMed] [Google Scholar]
- 44. Tan SS, van der Slot WM, Ketelaar M, et al. Factors contributing to the longitudinal development of social participation in individuals with cerebral palsy. Res Dev Disabil 2016; 57: 125–35. [DOI] [PubMed] [Google Scholar]
- 45. Ullenhag A, Bult MK, Nyquist A, et al. An international comparison of patterns of participation in leisure activities for children with and without disabilities in Sweden, Norway and the Netherlands. Dev Neurorehabil 2012; 15: 369–85. [DOI] [PubMed] [Google Scholar]
- 46. McCormack J, Harrison LJ, McLeod S, McAllister L. A nationally representative study of the association between communication impairment at 4–5 years and children's life activities at 7–9 years. J Speech Lang Hear Res 2011; 54: 1328–48. [DOI] [PubMed] [Google Scholar]
- 47. Axelsson AK, Granlund M, Wilder J. Engagement in family activities: a quantitative, comparative study of children with profound intellectual and multiple disabilities and children with typical development. Child Care Health Dev 2013; 39: 523–34. [DOI] [PubMed] [Google Scholar]
- 48. Engel‐Yeger B, Hamed‐Daher S. Comparing participation in out of school activities between children with visual impairments, children with hearing impairments and typical peers. Res Dev Disabil 2013; 34: 3124–32. [DOI] [PubMed] [Google Scholar]
- 49. Khetani M, Marley J, Baker M, et al. Validity of the Participation and Environment Measure for Children and Youth (PEM‐CY) for Health Impact Assessment (HIA) in sustainable development projects. Disabil Health J 2014; 7: 226–35. [DOI] [PubMed] [Google Scholar]
- 50. Soref B, Ratzon NZ, Rosenberg L, Leitner Y, Jarus T, Bart O. Personal and environmental pathways to participation in young children with and without mild motor disabilities. Child Care Health Dev 2012; 38: 561–71. [DOI] [PubMed] [Google Scholar]
- 51. Must A, Phillips S, Curtin C, Bandini LG. Barriers to physical activity in children with autism spectrum disorders: relationship to physical activity and screen time. J Phys Act Health 2015; 12: 529–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Rosenberg L, Jarus T, Bart O. Development and initial validation of the Children Participation Questionnaire (CPQ). Disabil Rehabil 2010; 32: 1633–44. [DOI] [PubMed] [Google Scholar]
- 53. King GA, Law M, King S, et al. Children's Assessment of Participation and Enjoyment (CAPE) and Preferences for Activities of Children (PAC). San Antonio, TX: PsychCorp San Antonio, 2004. [Google Scholar]
- 54. Cavallo S, Majnemer A, Mazer B, Chilingaryan G, Ehrmann Feldman D. Participation in leisure activities among Canadian children with arthritis: results from a national representative sample. J Rheumatol 2015; 42: 1002–10. [DOI] [PubMed] [Google Scholar]
- 55. Houtrow A, Jones J, Ghandour R, Strickland B, Newacheck P. Participation of children with special health care needs in school and the community. Acad Pediatr 2012; 12: 326–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Mâsse LC, Miller AR, Shen J, Schiariti V, Roxborough L. Patterns of participation across a range of activities among Canadian children with neurodevelopmental disorders and disabilities. Dev Med Child Neurol 2013; 55: 729–36. [DOI] [PubMed] [Google Scholar]
- 57. Rekkedal AM. Factors associated with school participation among students with hearing loss. Scandinav J Disabil Res 2017; 19: 175–93. [Google Scholar]
- 58. Oates A, Bebbington A, Bourke J, Girdler S, Leonard H. Leisure participation for school‐aged children with Down syndrome. Disabil Rehabil 2011; 33: 1880–9. [DOI] [PubMed] [Google Scholar]
- 59. Marquis WA, Baker BL. Sports participation of children with or without developmental delay: prediction from child and family factors. Res Dev Disabil 2015; 37: 45–54. [DOI] [PubMed] [Google Scholar]
- 60. Rosenberg L, Bart O, Ratzon NZ, Jarus T. Personal and environmental factors predict participation of children with and without mild developmental disabilities. J Child Fam Stud 2013; 22: 658–71. [Google Scholar]
- 61. Shields N, Kearns C, Synnot A. The extent, context and experience of participation in out‐of‐school activities among children with disability. Res Dev Disabil 2015; 47: 165–74. [DOI] [PubMed] [Google Scholar]
- 62. Kamath S, Fayed N, Goodman C, Streiner DL, Ronen GM. Extracurricular participation among children with epilepsy in Canada. Epilepsy Behav 2016; 56: 118–22. [DOI] [PubMed] [Google Scholar]
- 63. World Health Organization . Promoting Mental Health: Concepts, Emerging Evidence, Practice: Summary Report. Geneva, Switzerland: WHO, 2004. [Google Scholar]
- 64. Furtado SR, Sampaio RF, Kirkwood RN, Vaz DV, Mancini MC. Moderating effect of the environment in the relationship between mobility and school participation in children and adolescents with cerebral palsy. Brazil J Phys Ther 2015; 19: 311–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Conger KJ, Rueter MA, Conger RD. The role of economic pressure in the lives of parents and their adolescents: the family stress model In: Crockett LJ, Silbereisen RK, editors. Negotiating Adolescence in Times of Social Change. New York, NY: Cambridge University Press, 2000: 201–23. [Google Scholar]
- 66. Garmezy N. Stress, competence, and development: continuities in the study of schizophrenic adults, children vulnerable to psychopathology, and the search for stress‐resistant children. Am J Orthopsychiatry 1987; 57: 159–74. [DOI] [PubMed] [Google Scholar]
- 67. Krech KH, Johnston C. The relationship of depressed mood and life stress to maternal perceptions of child behavior. J Clin Child Psychol 1992; 21: 115–22. [Google Scholar]
- 68. Majnemer A, Shevell M, Law M, Poulin C, Rosenbaum P. Indicators of distress in families of children with cerebral palsy. Disabil Rehabil 2012; 34: 1202–7. [DOI] [PubMed] [Google Scholar]
- 69. Lach LM, Kohen DE, Garner RE, et al. The health and psychosocial functioning of caregivers of children with neurodevelopmental disorders. Disabil Rehabil 2009; 31: 607–18. [DOI] [PubMed] [Google Scholar]
- 70. Cohen MS. Families coping with childhood chronic illness: a research review. Fam System Health 1999; 17: 149. [Google Scholar]
- 71. Allen S, Knott F. How do children's challenges to function and participation impact maternal stress? A survey of mothers of children with suspected developmental co‐ordination disorder. N Z J Occup Ther 2016; 63: 29–37. [Google Scholar]
- 72. Law M, Anaby D, Teplicky R, Khetani MA, Coster W, Bedell G. Participation in the home environment among children and youth with and without disabilities. Br J Occup Ther 2013; 76: 58–66. [Google Scholar]
- 73. Laws G, Radford J. Place, identity and disability In: Kearns RA, Gesler WM, editors. Putting Health into Place: Landscape, Identity, and Well‐Being. Syracuse, NY: Syracuse University Press, 1998: 77–101. [Google Scholar]
- 74. Corcoran M, Adams T. Race, Sex, and the Intergenerational Transmission of Poverty. Consequences of Growing up Poor. New York, USA: Russell Sage Foundation, 1997. [Google Scholar]
- 75. Pantazis C, Gordon D, Levitas R. Poverty and Social Exclusion in Britain: the Millennium Survey. Bristol, UK: Policy Press, 2006. [Google Scholar]
- 76. Treanor M. The effects of financial vulnerability and mothers’ emotional distress on child social, emotional and behavioural well‐being: a structural equation model. Sociology 2016; 50: 673–94. [Google Scholar]
- 77. Chambers R. Editorial introduction: vulnerability, coping and policy. IDS Bulletin 1989; 20: 1–7. [Google Scholar]
- 78. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med 2007; 4: e296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Anaby D, Law M, Coster W, et al. The mediating role of the environment in explaining participation of children and youth with and without disabilities across home, school, and community. Arch Phys Med Rehabil 2014; 95: 908–17. [DOI] [PubMed] [Google Scholar]
- 80. King G, Law M, Petrenchik T, Hurley P. Psychosocial determinants of out of school activity participation for children with and without physical disabilities. Phys Occup Ther Pediatr 2013; 33: 384–404. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1: Search strategy.
Figure S2: Flow diagram detailing study selection process.
Table SI: Research Triangle Institute 14‐item tool
Table SII: Factors combined into a single identifying factor
Table SIII: Summary of included studies
Table SIV: Description of validated tools applied to measure participation
Table SV: Quality appraisal based on the customized Research Triangle Institute 14‐item tool