

Abstract
Introduction:
The use of debating as an educational tool is increasing in popularity. Students who take part in debates can develop a range of skills such as confidence and communication as well as gaining a greater understanding of the topic discussed. Within this study we have evaluated an antibiotic-resistant debate kit, assessing the ability of the debate lesson to improve student knowledge and awareness around antibiotics.
Methods:
The debate lesson was delivered in seven schools across South West England to 235 students aged 13-16 years. Change in student knowledge was measured using before and after knowledge questionnaires. Student and teacher feedback and suggestions for improvements for the lesson were also collected through questionnaires and interviews.
Results:
Quantitative questionnaires found a significant improvement in knowledge for most areas covered in the debate, particularly around the use of antibiotics to treat colds and bacteria developing resistance. Teachers felt their students engaged well with the debate session and made suggestions for minor modifications that could improve the lesson.
Conclusions:
The results suggest that the e-Bug antibiotic resistant debate kit is able to improve knowledge in young people around antibiotics and antibiotic resistance. Furthermore, the lesson was enjoyed by students and therefore this resource should be promoted more widely to teachers and schools.
Keywords: Education, infection prevention, antimicrobial resistance, primary care, antibiotics, healthcare-associated infections, microbiology, young people, children
Introduction
Antibiotic resistance is a major worldwide public health threat (World Health Organization [WHO], 2014). Annually, 700,000 people die from antibiotic-resistant infections; it is estimated that by 2050 this could reach 10 million deaths a year if no action is taken (O’Neill, 2016).
There are a number of reasons why antibiotic resistance occurs (WHO, 2015). Overuse and misuse of antibiotics, and poor hygiene and infection control, that both facilitate resistance, can be reduced through appropriate education. Indeed, education is a key part of the Department of Health’s UK Five Year Antimicrobial Resistance Strategy 2013 to 2018 (Department of Health, 2013). By educating both professionals and the public, we can begin to address these issues and contribute to slowing the continuing emergence of antibiotic resistance.
Young people are our future generation of antibiotic users and prescribers. In addition, young people aged 15–24 years are four times more likely to take antibiotics that were not prescribed for them, than people aged > 25 years (Public Health England, 2014). Instilling important health messages around antibiotic use and hygiene at a young age can set healthy behaviours for life. By targeting young people, we can also potentially reach other family members as the messages can be taken home from schools and passed to others in the household. e-Bug is one such programme which educates young people on the important messages around antibiotics (McNulty et al., 2011).
e-Bug, operated by Public Health England, is a health education resource for children and young people, aged 4–18 years, that teaches about hygiene, infection, vaccinations and antibiotic resistance. The e-Bug resources include teaching materials for use in the classroom, such as lesson plans, worksheets and activities, as well as student websites which contain games, revision guides and other materials for students to use at home. e-Bug works with partners in 26 different countries across the world and the resources are available in 23 different languages. All the e-Bug resources are freely available at www.e-bug.eu for educators and students to download. Many of the e-Bug resources have been evaluated and found to significantly improve knowledge in young people (Hale et al., 2017; Hawking et al., 2013; Lecky et al., 2010; 2014; Young et al., 2017).
The e-Bug Antibiotic Resistance debate kit is part of these resources for young people. It was developed in collaboration with I’m a Scientist, an organisation which runs science outreach events such as online debates with scientists and develops educational debate kits for use in schools. The aim of the debate kit is to stimulate interest and discussion—about antibiotics, antibiotic use and antibiotic resistance—and to increase knowledge of intentions to use antibiotics more appropriately.
The debate kit was launched on the e-Bug England website in 2014 to coincide with European Antibiotic Awareness Day. The debate kit is aimed at students aged 11 years and over and is available for download from both the e-Bug teacher webpages and the e-Bug student webpages. In the first two years of launch, the activity had been downloaded 739 times with 3332 webpage views. The e-Bug team have also distributed hardcopies of the debate kit at conferences and events. The debate kit is also available for download from the I’m a Scientist webpage, where teachers can also request a hard copy be sent to their school or collect at I’m a Scientist events.
The aim of this study was to investigate the ability of the debate kit to increase knowledge and awareness of antibiotic and antibiotic resistance in secondary school students aged 13–16 years. The study also looked at whether the effectiveness of the kit differed by gender, school type and location of the school. In addition, student and teacher views and opinions on the debate kit were gathered to inform on any improvements or modifications that could be made.
Methods
Ethics
Ethical approval for the study was granted from the University of the West of England’s Faculty Research Ethics Committee.
School recruitment
Secondary schools in three regions across South West England were recruited through convenience sampling to participate. Schools were purposively selected to recruit a range of school type, in rural and urban locations. Schools were approached via letter, email and phone call to describe the study in more detail. Seven schools (five rural and two city) agreed to participate. Three private schools, three state comprehensive schools and one University Technical College took part.
Lesson delivery
The e-Bug Antibiotic Resistance debate lesson was delivered in schools by a researcher (MB) in June and July 2016. The lesson was delivered to students in Years 9 and 10, ages 13–16 years. The lesson began with a short introduction on antibiotics and antibiotic resistance. Students were then split into groups of 4–6 to use the antibiotic debate kit. The Antibiotic Resistance debate kit focuses on the question: ‘Should the NHS tell GPs to give back-up prescriptions instead of immediate antibiotics wherever possible?’ and includes eight character cards each with different professional roles who express different opinions on the topic. Each student in a group was given a different character card and asked to take on that persona, presenting their character’s persona and opinions to the group. This included the character’s background and opinion on the topic, a fact around the topic and an issue the character faces. Students were then asked to discuss the questions about antibiotic use and resistance on the bottom of each character card. Through the different characters, students questioned and discussed the wider facts, myths and issues relating to antibiotic resistance stated by each persona or on the card, including: the relationship of antibiotic use to resistance; use of antibiotics in animals; activity of antibiotics against bacteria and viruses such as the common cold; and carriage and transmission of antibiotic resistant bacteria. Each group fed back their discussions to the rest of the class and voted (if time allowed) whether they considered that ‘Should the NHS tell GPs to give back-up prescriptions instead of immediate antibiotics wherever possible’.
Data collection
Students were asked to complete a knowledge questionnaire before the lesson began and again immediately after the lesson. The questionnaire included true/false, multiple-choice and open-ended questions around the topic of antibiotics and antibiotic resistance. The questionnaire was based on e-Bug evaluation questionnaires used in previous studies (Hale et al., 2017; Young et al., 2017). A copy of the questionnaire is included in Appendix 1.
Data on students’ enjoyment of the session were collected through Likert scale and open-ended questions regarding students’ opinions on the lesson and suggestions for improvement completed immediately after the lesson (Appendix 1).
Qualitative data were also collected through brief interviews with teachers who observed the lesson. Five teachers took part in the interviews and the data were recorded through researcher notes. The interviews explored teachers’ opinions on the lesson, how well they felt students engaged with the lesson and their suggestions for improvements.
Data analysis
All questionnaire data were entered into Excel. Knowledge data were imported into STATA version 14.2 for analysis. There were 17 knowledge questions, the first 14 of which were true/false with the last three being multiple choice. Questions for which there were no responses were treated as missing and excluded from the analysis. Question 10 was not analysed, as a minor typographical error was introduced into the final statement, making it open to misinterpretation. Mixed effects regression with the student as the random effect and period (before/after using the debate kit), region, school type and gender as fixed effects and, where necessary, McNemar’s test, were used to address the study aim. Each of the 16 questions and the derived percentage variable were analysed separately. When the outcome was binary, the regression model used was logistic and for the percentage outcome variable it was normal linear.
For both sorts of regression, the following modelling procedure was adopted, wherein 5% was taken as the significance level with P value obtained from the Wald test. Two initial models were formed, each by a three-way interaction, a two-way interaction and their lower order terms. Both of these interactions involved period, the latter either with region (first of the two) or school type (second), while the former was with the remainder of school type, gender and region. These two initial models were simplified in a stepwise manner according to the significance of the interactions and the simplest convergent model reported in which all interactions were significant and produced meaningful results, if any. Where more than one interaction was significant in a model, the P values were obtained from that model while the ORs and the CIs were obtained from two simpler models each with just one of the two interactions, with the variable in the other interaction as purely a main effect. A measure of association (odds ratio [OR] for binary outcomes and percentage change for percentage outcome), together with the 95% confidence interval (CI) was obtained from either the model or the concordancy table, as appropriate.
Themes arising from the teacher interviews were summarised into a short report with quotes.
Results
A total of 235 students took part in the study across the seven schools: 235 students completed the survey and nearly all completed all before and after questions, with 227–235 answering each question. Five teachers were interviewed after the session, one from five of the schools who participated.
Quantitative results: students
The results for the true/false and multiple-choice questions (questions 1–17) are shown in Table 1. For the majority of questions, there was a significant improvement in knowledge after the debate lesson, as indicated by a P value of < 0.05. For example, with the first question ‘Antibiotics can cure the common cold’, students had > 7 times higher odds of answering correctly after the lesson. One of the largest improvements in knowledge was for question 4, ‘Only certain types of bacteria can become resistant’ (false), with students > 16 times higher odds of answering correctly after the lesson. Other questions with great improvement in knowledge included the question ‘Antibiotics can be used as painkillers’ (false), with correct answers going from 51% to 80%, and ‘Antibiotics don’t harm good bacteria’, with correct responses going from 64% to 87%. In the free text, 148 students, (63%) reported that antibiotics killed bacteria before the session; this increased to 212 (90%) after the session. Only one (0.5%) student reported ‘yes’ that they knew what a back-up antibiotic prescription was before the lesson and were able to explain this in the free-text answer; this increased to 136 (58%) after the debate.
Table 1.
Knowledge improvement scores by question for 235 students aged 13–16 years after using the debate kit in small groups.
| Question | Students before; after if different (n) |
Correct before teaching (%) | OR before teaching (95% CI) |
Correct after teaching (%) | OR after teaching (95% CI) |
P value | |
|---|---|---|---|---|---|---|---|
| 1 | Antibiotics can cure the common cold. | - | 80.0 | 1.0 | 96.2 | 7.34 (3.13–17.2) | < 0.001 |
| 2 | Antibiotics don’t harm ‘good’ bacteria. | - | 64.3 | 1.0 | 87.2 | 6.90 (3.44–13.8) | < 0.001 |
| 3 | There are more ‘bad’ bacteria than ‘good’ | ||||||
| Female | - | 80.5 | 1.0 | 71.5 | 0.45 (0.21–0.98) | 0.01 | |
| Male | 74.1 | 0.70 (0.26–1.87) | 81.3 | 1.34 (0.49–3.72) | |||
| 4 | Only certain type of bacteria can become resistant. | - | 48.1 | 1.0 | 80.4 | 16.2 (6.57–40.0) | < 0.001 |
| 5 | Farm animals use the most antibiotics | ||||||
| Private | - | 69.6 | 1.0 | 65.9 | 0.83 (0.48–1.42) | 0.003* | |
| State Secondary | 58.5 | 0.95 (0.28–3.25) | 81.7 | 3.35 (0.95–11.8) | |||
| UTC | 50.0 | 1.10 (0.30–4.07) | 83.3 | 6.21 (1.28–30.1) | |||
| 6 | Antibiotics can be used as painkillers. | - | 51.1 | 1.0 | 80.4 | 5.90 (3.35–10.4) | < 0.001 |
| 7 | New antibiotics can be easily created. | - | 83.8 | 1.0 | 92.3 | 3.00 (1.47–6.13) | 0.003 |
| 8 | You can only pass on antibiotic resistant bacteria if you have an infection. | ||||||
| Oxfordshire | - | 54.0 | 1.0 | 82.0 | 4.81 (1.76–13.2) | 0.001† | |
| Bristol | 60.8 | 3.11 (1.04–9.32) | 62.5 | 3.37 (1.12–10.1) | 0.02‡ | ||
| South Gloucestershire | 73.8 | 1.80 (0.55–5.86) | 61.5 | 0.96 (0.30–3.04) | |||
| Female | 65.9 | 1.0 | 61.8 | 0.82 (0.44–1.44) | |||
| Male | 59.8 | 0.79 (0.44–1.44) | 71.4 | 1.40 (0.47–2.91) | |||
| 9 | The more we use antibiotics, the more antibiotic-resistant microbes appear. | - | 87.2 | 1.0 | 93.2 | 2.40 (1.15–5.03) | 0.02 |
| 11 | People can carry antibiotic resistant bacteria without symptoms. | ||||||
| Oxfordshire | - | ||||||
| Female | 78.1 | 1.0 | 87.5 | 2.89 (0.52–16.0) | |||
| Male | 94.4 | 25.5 (0.97–670) | 66.7 | 1.02 (0.10–10.5) | 0.02 | ||
| Bristol | |||||||
| Female | 84.9 | 5.91 (0.54–64.5) | 81.8 | 4.22 (0.40–44.5) | |||
| Male | 83.3 | 4.84 (0.44–53.9) | 88.9 | 9.65 (0.79–118) | |||
| South Gloucestershire | |||||||
| Female | 84.0 | 0.63 (0.05–7.49) | 88.0 | 1.01 (0.08–13.2) | |||
| Male | 75.0 | 0.27 (0.03–2.52) | 95.0 | 3.69 (0.26–52.5) | |||
| 12 | People can’t die from an antibiotic-resistant infection. | 234; 235 | 82.1 | 1.0 | 86.4 | 1.57 (0.87–2.85) | 0.14 |
| 13 | Most antibiotics are prescribed by GPs outside of hospitals. | - | 80.4 | 1.0 | 85.5 | 1.55 (0.90–2.64) | 0.11 |
| 14 | Microbes can only be resistant to one type of antibiotics. | - | 72.3 | 1.0 | 85.5 | 3.23 (1.77–5.90) | < 0.001 |
| 15 | Antibiotics can kill a) bacteria only b) viruses only c) both |
234; 235 | 78.6 | 1.0 | 100.0 | n.e. (13.1–∞) | < 0.001 |
| 16 | How should you take antibiotics? a) until you feel better a) for the full length of the course b) make sure to save some for next time |
232; 233 | 88.7 | 1.0 | 100.0 | n.e. (6.56–∞) | < 0.001 |
| 17 | Who becomes resistant due to overuse of
antibiotics? a) people b) animals c) bacteria d) viruses |
227; 232 | 85.5 | 1.0 | 94.0 | 5.75 (1.96–22.9) | < 0.001 |
P value for interaction between period (before/after) and school type.
P value for interaction between period and region.
P value for interaction between period and gender.
P value for interaction between period, gender and region.
OR, odds ratio; CI, confidence interval.
For several of the questions in Table 1, change in knowledge differed significantly between one or more of gender, school type and region. For example, in question 5, ‘Farm animals use the most antibiotics’, students from state secondary or university technical colleges demonstrated a significant improvement in knowledge, whereas students from private schools had a slight decline in knowledge that was not significant.
For questions 15 and 16, all students answered correctly after the lesson and so an odds ratio value could not be estimated.
Qualitative results: students
Likert scale questions were used to assess students’ enjoyment of the debate session, as well as their opinion on the importance of antibiotic resistance and back-up antibiotic prescriptions. On average, students scored their enjoyment for the session as 7.13/10 and rated the importance of antibiotic resistance as 7.99/10. Responses to the Likert-scale questions are shown in Figure 1.
Figure 1.
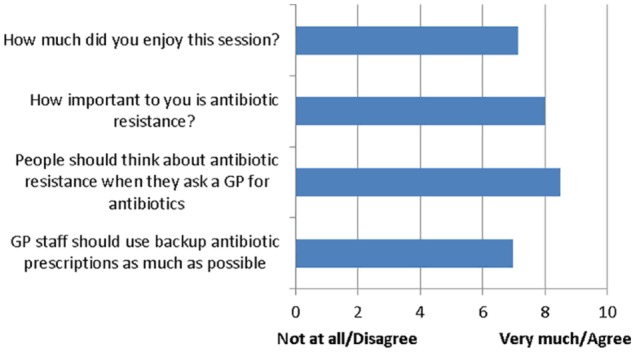
Responses to the Likert-scale questions.
Students were asked what they enjoyed most about the debate session; 217 students answered: 59 responded taking part in group discussions; and 46 responded the character cards. Other commonly occurring responses were learning new things (n = 41) and the debating aspect (n = 36).
When commenting on aspects they least enjoyed about the session, the majority of students (n = 129) either left this question blank or said there was nothing they did not enjoy about the session. Fourteen students mentioned too much text to read on the cards and 10 mentioned taking part in the debate. However, only 10 students mentioned the debate in a negative connotation, as oppose to 36 students who enjoyed this aspect of the session. Suggestions for improvements included an accompanying PowerPoint or video with more interactivity and more character cards.
Qualitative results: teachers
Of the five teachers interviewed after the lesson, two had heard of e-Bug before the study, but none had previously used the materials. The majority of teachers thought that their students engaged well with the session. One teacher thought a small number of students did not engage well; however, this school ran the session as an afterschool lesson and therefore the setting did not reflect a normal day-to-day lesson. Almost all teachers described running debates in their school ‘occasionally’ and all thought the e-Bug antibiotic resistance debate was useful for their students and would consider running it again. Suggestions for improvements included voting in class, reducing the amount of text on the cards, an accompanying PowerPoint presentation, and a worksheet for students to write down their ideas.
Discussion
Summary of results
The results from student knowledge change questionnaires suggest the e-Bug antibiotic resistance debate kit is able to improve knowledge in students aged 13–16 years about antibiotics, their activity and the use of back-up antibiotics. Knowledge improved around a variety of issues, including misconceptions around antibiotics curing the common cold or being used as painkillers, as well as antibiotic resistance and which bacteria can develop resistance. Students were positive about the lesson and the use of back-up/delayed antibiotics.
When comparing the knowledge change between gender, school type and region, it can be seen that there is no notable difference between these variables. For question 5, state secondary schools and university technical colleges had a greater knowledge change compared to private schools; however, this was not replicated for other questions. Likewise, with gender and region, where certain questions showed a greater knowledge improvement for one variable over the other, but no theme was replicated across multiple questions. Therefore, the results suggest that the debate kit was able to improve knowledge for all students who took part in the study. Differences between school type and regions may be due to previous coverage of the topic in those schools.
Strengths and limitations of the study
A total of 235 students took part in this study from seven schools of differing types and locations. Therefore, data were collected from a wide range of students. Delivery of the lesson by one researcher ensured a consistent teaching approach was used across the different schools; however, this may not reflect a day-to-day lesson given by the normal teaching staff. Having an external visitor deliver the lesson in school could have increased student interest and attention to the lesson. In addition, one school ran the lesson as an afterschool session which could have affected student perceptions on the lesson. The debate kit was evaluated over two year groups, with an age range of 13–16 years, so results may not be transferable to other age groups, as knowledge gain may be greater in younger students or less in older students. However, older students aged > 16 years may find the debate more interesting as they are learning to self -care and visit the health professional more often without a parent or guardian. As the debate kit is designed for a wider age range, it would be useful to evaluate it in younger and older students, or even in the community or under graduate students, as we have had anecdotal feedback to say the resources would be useful in pharmacy, nursing and medical students, and community groups. The results showed an increase in knowledge before and after the lessons, but the debate question asking if GP staff should use back-up prescriptions were only used after the lesson, so we cannot know if opinions had changed. However, we do know that only one student answered that they knew a back-up antibiotic was before the lesson. All the classes that did vote on the debate question with a show of hands had a majority indicating that GP staff should use back-up prescriptions wherever possible. Their main reasoning was that the students would prefer potentially a few days of discomfort before taking the antibiotics to bacteria becoming resistance due to over and improper use. Unfortunately, we do not know about long-term knowledge retention as it was not possible to do long-term follow-up as students were not available to the researcher at a later date. A few questions may have been misinterpreted by students leading to higher or lower results than expected. For example, > 94% of boys answered question 11 (‘People can carry antibiotic-resistant bacteria without symptoms’) correctly before the lesson which is very high. This may be that they did not understand the phrase ‘without symptoms’ or missed the word as it appeared on its own on the second line. The learning for this question and question 8 on carriage of resistant organisms was only on one of the character cards and the wording was not exactly as in the question. If not all the cards were discussed fully by participants, and/or the facilitator did not discuss fully all the facts in the debate cards, less-able pupils may not have been able to interpret the questions correctly.
Comparison to other literature
The I’m a Scientist company, who developed the debate kit in collaboration with e-Bug, undertook a short teacher evaluation of the Antibiotic Resistance debate kit between September 2015 and November 2015 (I’m a Scientist, 2015). A random sample of 100 teachers who had requested a hard copy of the debate kit was asked if they had used it. From those who responded, 33% (20/61) said they had used the debate kit with their students. In a larger survey of all teachers who had requested the debate kit, 51 teachers who had used the debate kit completed feedback questions. Of these, 65% of teachers had used the kit more than once and 94% planned to use it again in the future; 63% rated the debate kit overall as ‘excellent’, with the remaining 37% rating it as ‘pretty good’. All teachers said that their students were now more aware of the issues surrounding antibiotics. These results are similar to those we obtained in this study, with all teachers interviewed saying they thought the kit was useful and that they would consider using it again.
Other studies have also assessed the use of debating as an educational tool. Koklanaris et al. compared teaching through lectures with teaching through debates and found that students who took part in debates had a higher knowledge gain compared to those who attended lectures on the same topic (Koklanaris et al., 2008). This suggests students learn more effectively through active participation rather than passive learning.
The majority of published studies around debating have investigated the benefits of competitive debating and debating teams; however, the study by Kennedy (2009) evaluated self-assessed knowledge change following an in-class debate with university students training to be teachers. Over half of the students were nervous about taking part in the debate but after the debate 86% said they would consider using debating as a teaching method with their students. Participants reported an increase in knowledge following the debates.
In a 2005 study, debating was evaluated in a secondary school in London with students aged 12–15 years through questionnaires and interviews (Jerome, 2005). As with our study, these students enjoyed taking part in a debate with most citing the opportunity to develop skills and build confidence as the main reason. Teachers interviewed in this study also spoke positively about debating.
Future work
Feedback from students and teachers suggests the e-Bug Antibiotic Resistance debate kit was received well and that the lesson was enjoyed by those who took part. Suggestions for improvements included an accompanying PowerPoint presentation and worksheet for students to record notes and ideas. These modifications will be made and the materials made available on the e-Bug website for educators to use. With debating now included in the England National Curriculum for Citizenship and English, it is likely to become a more popular learning tool in schools for a range of subjects. Future work could look more broadly at the use of debating in schools, investigating not just knowledge change, but also behaviour change as a result. When using the resources to maximise learning, the educators should give an introduction to the session about antibiotic resistance, including the meaning of any difficult concepts such as ‘without symptoms’ and carriage. Educators should also try to ensure all the cards and their content are discussed fully in the class. It would be useful to provide a short questionnaire with the debate kit so that educators or community leaders can assess knowledge and intentions changes after its use.
Supplemental Material
Supplemental material, 2019.04.03_Appendix_1_Knowledge_Questionnaire for Using debate to educate young people in schools about antibiotic use and resistance: A before and after evaluation using a questionnaire survey by Vicki L Young, Mark Berry, Neville Q Verlander, Andy Ridgway and Cliodna AM McNulty in Journal of Infection Prevention
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Peer review statement: Not commissioned; blind peer-reviewed.
Supplemental material: Supplemental material for this article is available online.
References
- Department of Health. (2013). UK Five Year Antimicrobial Resistance Strategy 2013 to 2018. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/244058/20130902_UK_5_year_AMR_strategy.pdf
- Hale AR, Young VL, Grand A, McNulty CA. (2017) Can gaming increase antibiotic awareness in children? A mixed-methods approach. JMIR Serious Games 5: e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawking MK, Lecky DM, Verlander NQ, McNulty CA. (2013) Fun on the farm: evaluation of a lesson to teach students about the spread of infection on school farm visits. PLoS One 8: e75641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- I’m a Scientist. (2015) Antibiotic Resistance Debate Kit Evaluation Report. Available at: https://debate.imascientist.org.uk/files/2015/12/Antibiotics-DK-Evaluation.pdf.
- Jerome L, Algarra B. (2005). Debating debating: a reflection on the place of debate within secondary schools. The Curriculum Journal 16: 493–508. [Google Scholar]
- Kennedy RR. (2009) The power of in-class debates. Active Learning in Higher Education 10: 225–236. [Google Scholar]
- Koklanaris N, MacKenzie AP, Fino ME, Arslan AA, Seubert DE. (2008) Debate preparation/participation: an active, effective learning tool. Teaching and Learning in Medicine 20: 235–238. [DOI] [PubMed] [Google Scholar]
- Lecky DM, Hawking MK, Verlander NQ, McNulty CA. (2014) Using interactive family science shows to improve public knowledge on antibiotic resistance: does it work? PLoS One 9: e104556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lecky DM, McNulty CA, Touboul P, Herotova TK, Benes J, Dellamonica P, Verlander NQ, Kostkova P, Weinberg J.and e-Bug Working Group. (2010) Evaluation of e-Bug, an educational pack, teaching about prudent antibiotic use and hygiene, in the Czech Republic, France and England. Journal of Antimicrobial Chemotherapy 65: 2674–2684. [DOI] [PubMed] [Google Scholar]
- McNulty CA, Lecky DM, Farrell D, Kostkova P, Adriaenssens N, Koprivova Herotova T, Holt J, Touboul P, Merakou K, Koncan R, Olczak-Pienkowska A, Avo AB, Campos J.and e-Bug Working Group. (2011) Overview of e-Bug: an antibiotic and hygiene educational resource for schools. Journal of Antimicrobial Chemotherapy 66 (Suppl. 5), v3–12. [DOI] [PubMed] [Google Scholar]
- O’Neill J. (2016). Tackling drug-resistant infections globally: final report and recommendations. London: Review of AMR; Available at: https://amr-review.org/. [Google Scholar]
- Public Health England. (2014) Entrenched misconceptions about antibiotics revealed in new survey. London: Public Health England; Available at: https://www.gov.uk/government/news/entrenched-misconceptions-about-antibiotics-revealed-in-new-survey. [Google Scholar]
- World Health Organization. (2014) Antimicrobial Resistance: Global report on surveillance. Geneva: WHO; Available at: http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf. [Google Scholar]
- World Health Organization. (2015). Causes of Antibiotic Resistance. Geneva: WHO. [Google Scholar]
- Young VL, Cole A, Lecky DM, Fettis D, Pritchard B, Verlander NQ, Eley CV, McNulty CA. (2017) A mixed-method evaluation of peer-education workshops for school-aged children to teach about antibiotics, microbes and hygiene. Journal of Antimicrobial Chemotherapy 72: 2119–2126. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, 2019.04.03_Appendix_1_Knowledge_Questionnaire for Using debate to educate young people in schools about antibiotic use and resistance: A before and after evaluation using a questionnaire survey by Vicki L Young, Mark Berry, Neville Q Verlander, Andy Ridgway and Cliodna AM McNulty in Journal of Infection Prevention