

Abstract
Objectives
As new, effective therapies emerge for acute lymphoblastic leukaemia (ALL), the results of clinical trials need to relate to standard of care.
Methods
We used the population‐based Swedish ALL Registry to evaluate characteristics, treatment and long‐term outcome in 933 patients with diagnosis between 1997 and 2015.
Results
The median age was 53 years. The frequency of Philadelphia (Ph)‐positive leukaemia was 34% of examined B‐ALL with a peak incidence at 50‐59 years. Five‐year overall survival (OS) improved between 1997‐2006 and 2007‐2015; in patients 18‐45 years from 50% (95% CI 43‐57) to 65% (95% CI 58‐72), 46‐65 years from 25% (95% CI 18‐32) to 46% (95% CI 37‐55) and >65 years from 7% (95% CI 2.6‐11) to 11% (95% CI 5.9‐16) (P < 0.05). Men with Ph‐neg B‐ALL 46‐65 years had inferior OS compared with women (P < 0.01). Standardised mortality ratio was 5.7 (95% CI 5.0‐6.3) for patients who survived 5 years from diagnosis. In multivariable analysis, Ph‐positive disease was not associated with impaired prognosis but with lower risk of death in 2007‐2015.
Conclusions
In a population‐based cohort, OS has improved in adult ALL, especially for Ph‐positive disease but for middle‐aged men with Ph‐negative B‐ALL outcome was poor. Cure without late toxicity or relapse is still desired.
Keywords: acute lymphoblastic leukaemia, adult, Philadelphia‐positive
1. INTRODUCTION
Overall survival (OS) in adult acute lymphoblastic leukaemia (ALL) has improved over the last decades. A population‐based study from the Netherlands with patients with ALL diagnosed from 1989 to 2012 revealed improved survival for all patients younger than 70 years.1 The 5‐year OS was 75% for patients 18‐24 years but only 37% for patients between 40 and 59 years in recent years, a finding confirmed by others.2, 3, 4, 5
The improvement in OS seen in younger adults (predominantly in Philadelphia‐negative [Ph‐neg] ALL) has been connected to the introduction of paediatric‐inspired protocols with multidrug induction, high‐dose methotrexate and asparaginase, as well as risk‐adapted treatment according to disease‐ and response‐related factors.1, 6, 7 The toxicity profile has been found acceptable, at least to the age of 45 years.6, 8, 9 Later reports indicate that age‐adapted paediatric‐inspired therapy is feasible up to the age of 65 years.10 In Philadelphia‐positive (Ph‐pos) ALL, the introduction of tyrosine kinase inhibitors (TKI) has fundamentally changed clinical practice and rendered improved OS both with and without allogeneic hematopoietic stem cell transplantation (HSCT).5, 11, 12, 13, 14, 15
Taken together, there is convincing evidence of therapeutic advancements in the last decades. However, there is lack of knowledge on ALL outcome from population‐based studies that include information about Ph‐pos disease and allogeneic HSCT. We used the nationwide Swedish Acute Leukaemia Registry, later the Swedish ALL Registry, to investigate disease characteristics, treatment and survival in patients diagnosed with ALL between 1997 and 2015.
2. PATIENTS AND METHODS
2.1. The Acute Lymphoblastic Leukaemia Registry
Since 1958, both pathologists and clinicians are obliged to report every cancer at diagnose to the Swedish Cancer Registry. The dual reporting system improves coverage and accuracy. From the Cancer Registry, diagnosis‐specific quality registries have evolved. From 1997, patients with acute leukaemia were monitored in the nationwide but regionally based Acute Leukaemia Registry. In 2007, the registry became a web‐based system, divided into the Acute Myeloid Leukaemia (AML) Registry and the ALL Registry as part of the new centralised Blood Cancer Registry. The registry has been previously described in detail, and the first report on ALL incidence was published in 2010.16, 17, 18 Different cohort studies have been performed with identification of patients from the ALL Registry, but an analysis of the complete registry has never been published.19, 20, 21
Into the ALL Registry, the treating physicians prospectively report different variables (these have expanded over time) including date of diagnosis, WHO performance status (WHO‐PS), treatment intention (remission inducing or palliative approach), date of first complete remission (CR1) and allogeneic HSCT. Ideally, it includes annual reports on last date of follow‐up and any date of relapse. Vital status is updated from the Swedish Civil Citizen Registry. Registry monitoring is done by regional controllers, and a written national report is regularly compiled. The completion of the diagnosis registration form compared to the Cancer Registry was 100% for patients with ALL diagnosis between 2007 and 2012 and 98% for 2013 and 2014.22
The database for this study was merged from the “old” (1997‐2006) Acute Leukaemia Registry and the “new” (2007‐2015) ALL Registry with some variables recoded to enable overall analysis. Definitions are described in Data S1. Because some variables were only reported in the new registry, they were analysed solely for this period. No verification of the ALL diagnosis was done beyond the dual reporting system.
2.2. Genetic analysis
Since 2007, Ph‐pos disease was reported in the registry even though as early as 1997 Ph‐pos leukaemia was considered a high‐risk criterion in the national guidelines. The recommended methods of investigation were conventional cytogenetics, fluorescent in situ hybridization (FISH) and/or polymerase chain reaction (PCR).
In this study, the reported genetic analysis was validated and missing data were collected from the six central genetic laboratory facilities performing the analysis in Sweden. Patients not confirmed to be Ph‐pos ALL are labelled Ph‐neg ALL in this text—except when calculating Ph frequency and OS for B‐ALL. In the latter two analyses, patients not adequately examined (defined as normal karyotype with ≥20 metaphases, another karyotype with clonal abnormality, a negative FISH or a negative PCR for major and minor transcript) were considered to have missing data (details in Data S1).
2.3. Treatment
Treatment recommendations, as part of national guidelines, changed over time (details in Data S1 and Table S1). In brief, the Swedish protocol ABCDV/VABA was the main remission‐inducing protocol.23 After a pilot study, patients 18‐45 years with Ph‐neg ALL were treated according to the paediatric NOPHO ALL 2008 protocol.24 Hyper‐CVAD was recommended for T‐ALL cases between 2003 and 2009.25 For patients with Burkitt leukaemia, the NHL‐BFM‐90 protocol and subsequently the GMALL‐B‐ALL/NHL2002 were advocated.26, 27 For older patients, age‐adopted protocols such as the EWALL‐backbone were suggested.15 Addition of imatinib to chemotherapy backbones for Ph‐pos ALL was formally recommended in 2007 but was gradually introduced the years before.
2.4. Statistics
Fischer's exact test was used to compare categorical variables. Continuous variables were analysed with the Mann–Whitney U test. Survival was estimated using the Kaplan‐Meier method and differences compared with the log‐rank test. Univariable and multivariable Cox Regression analyses were used to determine hazard ratio (HR) of covariates included in the multivariable model.
Standardised mortality ratio (SMR) was calculated using indirect standardisation. Patients who had survived 5 years from ALL diagnosis were compared with the expected number of deaths in the Swedish population between 2002 and 2018. Patients were matched based on age, gender and calendar year at risk. When needed, the expected number of deaths was adjusted to account for incomplete follow‐up time at calendar year.
Because no imputation of missing data was done and no adjustment for multiplicity testing was performed, P‐values should be interpreted as explorative. Statistical analyses were performed with the SPSS‐software (IBM) v24 and v25 and R version 3.5.2 (R Core Team).
Vital status was followed until 31 May 2018. The study was approved by the regional ethical committee, Uppsala (Dnr 2016/349) and conducted in accordance with the Declaration of Helsinki.
3. RESULTS
3.1. Patients
We identified 937 patients 18 years or older diagnosed with ALL between 1997 and 2015. Three patients were excluded due to a known Philadelphia chromosome one, two and 6 years before ALL diagnosis as these patients were judged to have chronic myeloid leukaemia in lymphatic blast crisis. One patient was excluded because of a relapse of childhood leukaemia.
Patient characteristics of the remaining 933 patients are presented in Table 1. The B‐ALL cohort comprised 68%, T‐ALL 15% and Burkitt leukaemia 4%. The group of ALL Not Otherwise Specified (NOS) diminished from 22% in the old to 5% in the new registry.
Table 1.
Patient characteristics of the 933 patients divided by phenotype for the whole study period (1997‐2015) and in the new more detailed registry (2007‐2015)
| Variable name | All patients | Ph‐neg B‐ALL | Ph‐pos ALL | Ph‐pos ALL vs Ph‐neg B‐ALL | T‐ALL | Ta ‐ALL vs Ph‐neg B‐ALL | Burkitt leukaemia | Burkitt vs Ph‐neg B‐ALL | ALL NOS | ALL NOS vs Ph‐neg B‐ALL | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients, n | 933 | 468 | 176 | 135 | 41 | 122 | ||||||||||
| New/Old registry, n, (%) | 469/464 | 50/50 | 237/231 | 51/49 | 110/66 | 63/37 | 79/56 | 59/41 | 25/16 | 61/39 | 22/100 | 18/82 | ||||
| Age, years, median, range | 53 | 18‐95 | 54 | 18‐94 | 53 | 19‐87 | n.s | 37 | 18‐89 | P < 0.01 | 61 | 19‐87 | P = 0.03 | 64 | 18‐95 | P < 0.01 |
| Male/Female, n, (%) | 522/411 | 56/44 | 241/227 | 52/48 | 92/84 | 52/48 | n.s | 100/35 | 74/26 | P < 0.01 | 25/16 | 61/39 | n.s | 67/55 | 55/45 | n.s |
| B‐ALL, n, (%) | 635 | 68 | 468 | 100 | 167 | 95 | ||||||||||
| T‐ALL, n, (%) | 135 | 15 | 1 | 1 | 135 | 100 | ||||||||||
| Burkitt leukaemia, n, (%) | 41 | 4 | 0 | 0 | 41 | 100 | ||||||||||
| ALL NOS, n (%) | 122 | 13 | 8 | 4 | 122 | 100 | ||||||||||
| WHO‐PS, n (%) | ||||||||||||||||
| 0 | 214 | 23 | 99 | 21 | 48 | 27 | 41 | 30 | 5 | 12 | 24 | 20 | ||||
| 1 | 467 | 50 | 250 | 54 | 90 | 51 | 74 | 55 | 11 | 27 | 45 | 37 | ||||
| 2 | 122 | 13 | 66 | 14 | 20 | 11 | 7 | 5 | 8 | 19 | 23 | 19 | ||||
| 3 | 65 | 7 | 29 | 6 | 8 | 5 | 3 | 2 | 11 | 27 | 14 | 11 | ||||
| 4 | 40 | 4 | 14 | 3 | 1 | 1 | 6 | 5 | 6 | 15 | 13 | 11 | ||||
| Missing | 25 | 3 | 10 | 2 | 9 | 5 | 4 | 3 | 3 | 2 | ||||||
| Variables only in the new registry 2007‐2015 | ||||||||||||||||
| WBC ×109/L, median, range | 13 | 0.4‐904 | 6 | 0.4‐904 | 29 | 0.7‐477 | P < 0.01 | 33 | 1.3‐477 | P < 0.01 | 14 | 2.5‐89 | P < 0.01 | 7 | 0.6‐236 | n.s |
| Haemoglobin, g/L, median, range | 103 | 49‐180 | 99 | 50‐161 | 103 | 56‐180 | n.s | 118 | 49‐164 | P < 0.01 | 109 | 82‐158 | P < 0.01 | 106 | 66‐139 | n.s |
| Platelet count, ×109/L, median, range | 54 | 2‐1306 | 56 | 3‐409 | 46 | 2‐1306 | n.s | 68 | 11‐360 | n.s | 51 | 8‐257 | n.s | 53 | 10‐522 | n.s |
| CNS‐leukaemia involvement, normal, NA, n, (%) | 21;350;98 | 5;75;20 | 7;180;50 | 3;76;21 | 5;83;22 | 5;75;20 | 6;61;12 | 8;77;15 | 2;13;10 | 8;52;40 | 1;17;4 | 5;77;18 | ||||
Abbreviations: ALL, acute lymphoblastic leukaemia; CNS, central nervous system; NA, not available; NOS, not otherwise specified; Ph‐pos, Philadelphia‐positive; Ph‐neg, Philadelphia‐negative; WBC, white blood cell count; WHO‐PS, WHO Performance status.
Excluding the one patient with Ph‐pos T‐ALL.
Median age at ALL diagnosis was 53 years (range 18‐95 years) and was similar for Ph‐pos (53 years) and Ph‐neg B‐ALL (54 years). As expected, the T‐ALL cohort was younger (37 years) and mainly male. Burkitt and ALL NOS patients were significantly older (61 and 64 years) than the Ph‐neg B‐ALL. The WHO‐PS was 0‐1 in 73% of patients and 2 or more in 24%.
3.2. Frequency of Philadelphia‐positive ALL
Information about Ph‐pos disease was reported only in the new registry and therefore retrospectively collected for the old registry as mentioned above and in Data S1. Testing for Ph‐pos ALL increased over time from 59% in 1997‐2007 (272 of 464) to 88% in 2007‐2015 (411 of 469; P < 0.01). Of the 933 patients in the registry, 176 patients (19%) were confirmed to be Ph‐pos ALL (one T‐ALL, eight ALL NOS and the rest of B‐ALL phenotype). In the examined cohort, the incidence of Ph‐pos ALL was 26% and equivalent in the two registry periods (24% in 1997‐2006: 66 of 272 tested, 192 not tested/missing data; 27% in 2007‐2015: 110 of 411 tested, 58 not tested/missing data, P = ns). In examined B‐ALL (1997‐2015), the incidence was 34% (n = 635 B‐ALL; 167 Ph‐pos, 331 Ph‐neg and 137 with missing data). The Ph frequencies for different age cohorts are displayed in Figure 1. The highest incidence (47%) was found in patients 50‐59 years and did not increase further with age.
Figure 1.

Philadelphia‐positive disease of tested B‐ALL in different age groups
3.3. Descriptive variables only reported in the new registry 2007‐2015
The median white blood cell count (WBC) was higher in the Ph‐pos cohort as well as in the T‐ALL cohort compared with Ph‐neg B‐ALL (Table 1). Of Ph‐neg B‐ALL, 24% had a WBC of ≥30 × 109/L and 34% of T‐ALL patients had WBC of ≥100 × 109/L. Information about bulky disease was available for 425 (91%) patients and present in 25 patients (19 cases in T‐ALL [27% of 71 reported] and the remaining in B‐ALL [n = 1], Burkitt [n = 2] and ALL NOS [n = 3]).
3.4. Treatment and outcome
Survival analyses were done with patients divided into three age groups (18‐45, 46‐65 and >65 years) and for two time periods (1997‐2006 and 2007‐2015). Unless otherwise stated, comparisons between Ph‐pos and Ph‐neg ALL are done without further subgrouping.
3.5. Remission intention and early deaths
Details are described in Table 2. Intensive remission‐inducing chemotherapy was intended in 89% of patients and did not increase over time. In the total cohort (n = 930, excluding three without the exact date of diagnosis), 10% died within 30 days and 14% died within 60 days from diagnosis. For patients with remission as the treatment goal, deaths within 30 days diminished from 7% (30/405) in 1997‐2006 to 3% (12/420) in 2007‐2015 (P < 0.05). Death within 60 days decreased from 11% (45/405) to 6% (27/420) (P < 0.05). In patients without remission intention (median age 80 years, the majority not evaluated for Ph status), 44% (44/101) died within 30 days from diagnosis, which did not change over time.
Table 2.
Treatment intention, early deaths and complete remission rates for the whole study period (1997‐2015) and in the new, more detailed registry (2007‐2015) including treatment regimens
| All patients | 18‐45 y | 46‐65 y | >65 y | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Remission‐inducing Therapy Intended | ||||||||
| Yes; No (total)a | 827; 102 (929) | 89; 11 | 380; 1 (381) | 100; 0 | 258; 6 (264) | 98; 2 | 189; 95 (284) | 67; 33 |
| Ph‐pos ALL, Remission Inducing Yes; No | 169; 7 | 96; 4 | 66; 0 | 100; 0 | 65; 0 | 100; 0 | 38; 7 | 84; 16 |
| Ph‐neg ALL, Remission Inducing Yes; No | 658; 95 | 87; 13 | 314; 1 | 100; 0 | 193; 6 | 97; 3 | 151;88 | 63; 37 |
| CR achieved | ||||||||
| Yes; No (total) (if Remission‐inducing Therapy Intended) | 694; 91 (785) | 88 | 358; 11 (369) | 97 | 217; 28 (245) | 89 | 119; 52 (171) | 70 |
| Death within 30 d of diagnosisb | ||||||||
| Total (Remission Inducing; Not remission inducing) | 86 (42; 44) | 9 (5; 44) | 5 (4; 1) | 1 (1; 100) | 17 (15; 2) | 6 (6; 33) | 64 (23; 41) | 23 (12; 44) |
| Death within 60 d of diagnosis | ||||||||
| Total (Remission‐inducing; Not remission inducing) | 131 (72; 59) | 14 (9; 58) | 7 (6; 1) | 2 (2; 100) | 27 (25; 2) | 10 (10; 33) | 97 (41; 56) | 35 (22; 60) |
| Variables only in the new registry 2007‐2015 Regimens reportedc and CR achieved | ||||||||
| Intensive guidelinesd ± imatinib CR Yes; No (total) | 191; 16 (207) | 92 | 77; 1 (78) | 99 | 87; 5 (92) | 95 | 27; 10 (37) | 73 |
| NOPHO‐protocol 1992 or 2008, CR Yes; No (total) | 114; 1 (115) | 99 | 107; 1 (108) | 99 | 7; 0 (7) | 100 | 0 | |
| Age‐adopted ± imatinib CR Yes; No (total) | 42; 14 (56) | 75 | 0 | 4; 3 (7) | 57 | 38; 11 (49) | 78 | |
| GMALL CR Yes; No (total) | 15; 4 (19) | 79 | 7; 0 (7) | 100 | 3; 1 (4) | 75 | 5; 3 (8) | 63 |
Abbreviations: ALL, acute lymphoblastic leukaemia; CR, complete remission; Ph‐pos, Philadelphia‐positive; Ph‐neg, Philadelphia‐negative.
Four patients with missing data on remission intention, total n = 929.
Three patients with missing data on the exact date of diagnosis, total n = 926.
Regimens reported; for references, see Data S1.
Instructions for registration of treatment has changed over time and the exact intensive therapy given has not always been possible to report.
3.6. Treatment intensity and complete remission
In the old registry, information about given treatment was restricted to (a) intensive/remission‐inducing, (b) palliative chemotherapy or (c) no treatment/supportive care. In the new registry, more detailed information was collected (Table 2). Of the patients with information about CR status and intention to treat into remission, 88% reached a CR1. In patients 18‐45, 46‐65 and >65 years, the CR rates were 97%, 89% and 70%, respectively (Table 2).
3.7. Overall survival
Five‐year OS improved in all age groups and increased from 50% (95% CI 43‐57) to 65% (95% CI 58‐72) in patients 18‐45 years, from 25% (95% CI 18‐32) to 46% (95% CI 37‐55) in patients 46‐65 years and from 7% (95% CI 2.6‐11) to 11% (95% CI 5.9‐16) in patients >65 years (P = <0.05, log‐rank for pairwise comparison; Figure 2). The corresponding median OS increased from 5.0 years (95% CI 1.3‐8.7) to the median OS not yet reached, from 1.4 years (95% CI 1.0‐1.8) to 3.6 years (95% CI 0.9‐6.2) and from 0.2 years (95% CI 0.1‐0.4) to 0.6 years (95% CI 0.4‐0.8) for the three age groups and the two time periods, respectively.
Figure 2.

Overall survival in the total cohort (n = 930) in 1997‐2006 and 2007‐2015. Five‐year overall survival improved in patients 18‐45 y from 50% (95% CI 43‐57) to 65% (95% CI 58‐72), in patients 46‐65 y from 25% (95% CI 18‐32) to 46% (95% CI 37‐55), and in patients >65 y from 7% (95% CI 2.6‐11) to 11% (95% CI 5.9‐16) (P = <0.05, log‐rank for pairwise comparison) [Colour figure can be viewed at http://wileyonlinelibrary.com]
When divided into Ph‐neg and Ph‐pos ALL, OS improved in all groups (P < 0.05 for pairwise comparison, log‐rank) except for Ph‐neg patients >65 years (P = ns, log‐rank; Figure 3A and B). In Ph‐pos ALL, only borderline significance was seen in patients 46‐65 years (P = 0.05, log‐rank; Figure 4A and B).
Figure 3.
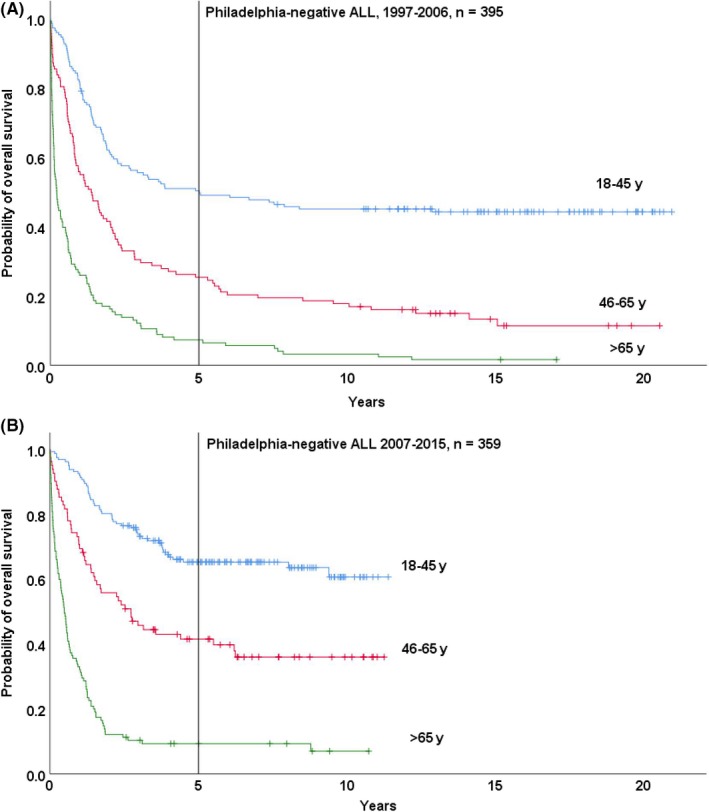
Overall survival (OS) in Philadelphia‐negative ALL in 1997‐2006 and 2007‐2015. A, Five‐year OS 1997‐2006 in patients 18‐45 y was 50% (95% CI 43‐58), in patients 46‐65 y 25% (95% CI 18‐33) and in patients >65 7% (95% CI 2‐12). B, Five‐year OS 2007‐2015 in patients 18‐45 y was 65% (95% CI 58‐73), in patients 46‐65 y 42% (95% CI 31‐53) and in patients >65 y 9% (95% CI 4‐15) [Colour figure can be viewed at http://wileyonlinelibrary.com]
Figure 4.

Overall survival (OS) in Philadelphia‐positive ALL in 1997‐2006 and 2007‐2015. A, Five‐year OS 1997‐2006 in patients 18‐45 y was 48% (95% CI 30‐67), in patients 46‐65 y 24% (95% CI 7‐41) and in patients >65 y 0%. B, Five‐year OS 2007‐2015 in patients 18‐45 y was 64% (95% CI 47‐81), in patients 46‐65 y 56% (95% CI 40‐72) and in patients >65 y 18% (95% CI 5‐31) [Colour figure can be viewed at http://wileyonlinelibrary.com]
Five‐year OS divided by phenotype and age group is presented in Table S2.
The standardised mortality ratio (SMR) was 5.7 (95% CI 5.0‐6.3) for patients that had survived 5 years from diagnosis (SMR—the number of deaths in the study cohort compared to the age‐adjusted expected deaths in the general population). The SMR decreased from 6.5 (95% CI 5.8‐7.8) to 3.8 (95% CI 2.8‐5.2) between 1997‐2006 and 2007‐2015, respectively. Median follow‐up for these patients in the SMR analysis was 10.7 years from diagnosis. Further subgroup analyses were not performed because of the size of the material.
3.8. Allogeneic stem cell transplantation
Of the 827 patients in which treatment intention was remission‐inducing, 24% (n = 200) were reported allografted in CR1 and 46% of them had Ph‐pos ALL. The HSCT frequency in patients 18‐45 years was 35% (64/182) versus 32% (64/198) in 1997‐2006 and 2007‐2015, respectively (P = ns). In patients 46‐65 years, it increased from 21% (30/141) to 33% (39/117; P = 0.03), and in patients >65 years, no patient was allografted in 1997‐2006 and only 3% (3/105) in 2007‐2015. The corresponding 5‐year OS improved for patients 18‐45 years from 50% (95% CI 37‐62) to 66% (95% CI 54‐78; P = 0.01, log‐rank) and for patients 46‐65 years from 30% (95% CI 14‐46) to 60% (95% CI 43‐76; P = 0.05, log‐rank). The three patients over 65 years transplanted in 2007‐2015 were all deceased within 3 years of diagnosis. There was no difference in OS between Ph‐pos and other patients with ALL allografted in CR1 (P = ns).
3.9. Prognostic factors
To evaluate the impact of different variables on OS, univariable and multivariable analyses were done for the entire registry and for the later time period (2007‐2015) and are presented in Table S3. Known risk factors such as age and WHO‐PS were related to an increased risk of death. Ph‐positivity did not impair prognosis when looking at the whole cohort and was even associated with better OS in 2007‐2015. Survival was superior in patients receiving ALL diagnosis in 2007‐2015. Allogeneic HSCT in CR1 did not have a prognostic impact. No difference in OS was found between men and women in the total cohort or for the different phenotypes in the univariable analysis. Therefore, these were not included in multivariable analysis.
However, in patients 46‐65 years, males had inferior survival compared with women (5‐year OS 26% [95% CI 18‐34] versus 44% [95% CI 35‐52], P < 0.01, log‐rank). The difference was present in both time periods, but subgroup analysis revealed that the difference was significant only in the Ph‐neg B‐ALL cohort (n = 130); 5‐year OS for men was 20% (95% CI 9.7‐30) and for women 52% (95% CI 40‐64; P < 0.01, log‐rank). Information about treatment and CR status was reported for 122 patients, and all but one received treatment with remission intention with a CR rate of 89% (85% for males and 93% for females, P = ns). There were no significant differences between sexes regarding WHO‐PS at diagnosis, median age, median WBC, proportion of patients with WBC over 30 × 109/L or 100 × 109/L, or HSCT frequency in CR1. Multivariable analysis within the group revealed that sex and WHO‐PS were independent factors for OS (data not shown).
4. DISCUSSION
To our knowledge, this is the largest population‐based cohort presenting data on outcome in adult ALL including information about Ph‐pos disease and allogeneic HSCT.1, 2, 3, 5, 28 An important aspect of population‐based studies is to provide aggregated clinical information that is less susceptible to the inherent selection bias of randomised controlled trials. In line with this, we present a higher median age of 53 years at ALL diagnosis and, in a study population without an upper age limit, that the median age did not differ between Ph‐pos and Ph‐neg B‐ALL.28, 29, 30, 31 As expected, T‐ALL patients were younger and we can corroborate that Burkitt leukaemia/mature B‐ALL have a substantially higher median age (61 years) than other B‐ALL.28 We confirm a high frequency of Ph‐pos disease—26% of all tested patients and 34% of B‐ALL with a peak incidence in patients 50‐59 years. This is a higher frequency of Ph‐pos ALL than suggested by the landmark study of Moorman et al 28 but comparable to Wetzler et al32 and a more recent large Italian cohort study.33 On the other hand, we did not find a continuous age‐associated increase suggested in the Italian paper and by Secker‐Wetzler et al34 but these studies had an upper age limit of 60 years and a low overall Ph‐pos frequency, respectively. Furthermore, the peak incidence of Ph‐pos disease in the fifth decade with a plateau between 30‐60 years is in line with Moorman and the French trial from 1996.30 Because of thoroughly testing in the latter period, we suggest that our data represent and approach the true incidence and age distribution of Ph‐pos ALL in a northern European population.
In spite of a high median age in the total cohort, the intention to treat into remission was high (89%), especially in comparison with the 73% treated with curative intention in Denmark.3 In younger patients, 99% received remission‐inducing therapy, and in patients >65 years, the corresponding figure was 67%.
In Swedish AML patients, the attitude towards remission‐inducing therapy in the elderly has been shown to influence overall survival.16 Whether this applies to ALL has, to our knowledge, not been studied. However, the previously low testing for Ph‐pos disease together with the 30‐day mortality of 43% patients with palliative intention (median age 80 years) indicates that there is potential to improve outcome, especially in view of the possibility to use TKI in this patient group.35
The improvement in OS in Ph‐neg patients aged 18‐45 years corresponds to the change to the use of paediatric protocols (NOPHO ALL 2008 proceeded by a pilot with NOPHO ALL 1992). For patients 46‐65 years, a similar improvement was noted. We hypothesise that better supportive care, the addition of rituximab, older patients treated according to the paediatric protocols and the use of reduced intensity conditioning in allogeneic HSCT could have been beneficial.36, 37, 38 For the elderly Ph‐neg patients, no increase in OS was seen despite the introduction of an age‐adapted protocol.10, 21
In Ph‐pos patients, OS improved in all age groups. This reflects not only the efficacy but also the good tolerance of TKI and low‐dose chemotherapy suitable for older patients.12, 14, 39 In our previously detailed study of elderly patients from this cohort, similar outcome was seen in Ph‐pos ALL whether they were transplanted in CR1 or not at all.21 In the EBMT Registry, OS was also comparable in younger Ph‐pos patients regardless if they had undergone allogeneic or autologous HSCT.40
Consequently, with the next generations of TKI it may not be necessary to use allogeneic HSCT in CR1 in younger patients with Ph‐pos ALL in deep remission. Impressive figures have been reported from the MD Anderson Institute with a 4‐year OS of 66% in patients in complete molecular remission (<10−4) at three months and treated with TKI but not eligible for HSCT.41 Yet, follow‐up in relation to normal life expectancy is relatively short and robust long‐term results are lacking. In our study, although 5‐year OS improved in the youngest age group, a plateau in the survival curve was seen only at that time, a finding that might be attributed to graft‐versus‐leukaemia effect in transplanted patients. We still await a randomised trial that supports cure with chemotherapy and TKI without detrimental late effects or TKI‐resistant relapses.40
When analysing prognostic factors, we confirmed that Ph‐pos disease was associated with better outcome in the later period 2007‐2015, a finding also revealed in recent studies.5, 42 Age, WBC count and WHO‐PS remained as high‐risk factors. This finding is well in line with both older and newer studies and might reflect the abovementioned shortage of treatments suitable for frail patients as well as clinician's choice of treatment intention with regard to age and WHO‐PS.42, 43, 44
This registry study was unable to confirm treatment‐correlated data. We suspect under‐reporting of HSCT frequency influenced the results even though our figures are almost identical with Dinmohamed et al1 that presented an allogeneic HSCT frequency of 25% (in our study this was 24%) and comparable outcome with a 5‐year OS of 66% in allografted patients 18‐39 years (in our study, 5‐year OS was 66% for patients 18‐45 years transplanted between 2007 and 2015). A cautious interpretation could be that since HSCT is recommended for high‐risk patients, the treatment seems to counterbalance the risk of relapse as previously proposed, with selection bias and transplant‐related mortality as possible confounders.37, 45, 46
As we noticed in our previous study of older patients,21 there was a pronounced difference in outcome between men and women in the Ph‐neg B‐ALL cohort of patients 46‐65 years, which we now confirm in a larger cohort and over a longer period. Inferior prognosis for males was previously reported from Poland and in historical childhood cohorts.47, 48 No explanation has emerged, and it is unclear whether this effect is due to the Swedish protocol ABCDV, male body mass, comorbidities or other unknown factors. Because of this and the insufficient long‐term survival in all middle‐aged patients, we have introduced a dose‐adjusted paediatric NOPHO 2008 protocol for Ph‐neg patients >45 years without an upper chronological age limit but biological age approaching 65 years.10
The present study provides important information on nationwide standard of care, where the nearly complete coverage of reported patients compared with the compulsory cancer registry adds strength to the material. Consequently, the selection bias was reduced, which is of particular importance regarding the elderly patients that are often excluded from randomised trials. The completeness of the diagnostic forms including descriptive data was high, and the Swedish social security number system makes OS undisputable. To further secure data accuracy, we confirmed and collected Ph status at the genetic laboratories. Nevertheless, diagnostic procedures have changed over time and were not centrally reviewed or certified and all patients were not properly evaluated. Being a registry‐based database, the study depends on the accuracy of the registry forms. From a previous detailed study of older patients from this cohort, the frequency of patients with diagnosis incorrectly registered (as lymphoblastic lymphoma or lymphatic blast crisis in chronic myelogenous leukaemia) was approximately 5%.21 In addition, outside randomised trials dubious diagnosis or results need to be considered and “exclusion criteria” do not exist, which leads to less stringent patient cohorts. It should also be noted that despite the high coverage and quality of vital status in the present and similar studies, follow‐up reports including HSCT and relapses are likely to be incomplete, limiting more profound analyses of, for example, treatment modalities. Nevertheless, population‐based studies are suitable as reference material when new drugs are introduced, especially if the registration trials have a narrow patient selection.49, 50
Furthermore, a SMR of 5.7 in patients who had survived 5 years from ALL diagnosis elucidates that the disease and relevant treatment have consequences beyond standard end‐points. As new potent immunotherapies enter the arena, their long‐term effects need thorough follow‐up, including comparison with current standard therapies, especially when a reachable goal for the majority of patients with ALL is now long‐time survivorship.
To conclude, in an unselected northern European adult population, the Ph‐pos frequency is 26% with an equal median age for Ph‐pos and Ph‐neg B‐ALL. An improvement in OS has evolved over time, especially for Ph‐pos patients. We speculate that the use of a paediatric protocol for Ph‐neg ALL and TKI for Ph‐pos patients are two main factors for improved survival. Nevertheless, males in Sweden 46‐65 years with Ph‐neg B‐ALL still have poor prognosis and are thus in need of better therapeutic strategies. A high SMR for long‐term survivors emphasises that new and less toxic treatments are highly anticipated for patients with ALL of all ages.
CONFLICT OF INTERESTS
The authors declare no conflict of interests.
AUTHOR CONTRIBUTION
EL and HH designed the study, did statistical analyses, evaluated data and wrote the manuscript. KK was the responsible physician of the registry during the whole study period. AL is the present responsible physician for the registry. All authors collected data and reviewed and approved the final draft.
Supporting information
ACKNOWLEDGEMENTS
Some statistical analyses were performed by Statisticon—Statistics and Research, Uppsala, Sweden. The authors would like to thank Hanna Rhodin and the Clinical Genetic/Chemical Centres at the university hospitals in Sweden for help with the collection of data for Philadelphia status. We would also like to thank Ann‐Sofie Hörstedt, Klaus Bjerregaard and the Regional Cancer Centre South for administrating the ALL quality registry, and last but not least, we thank all colleagues reporting to the registry.
Lennmyr E, Karlsson K, Ahlberg L, et al; On behalf of the Swedish Adult Acute Lymphoblastic Leukaemia Group (SVALL) . Survival in adult acute lymphoblastic leukaemia (ALL): A report from the Swedish ALL Registry. Eur J Haematol. 2019;103:88–98. 10.1111/ejh.13247
Funding information
EL and HH received grants from the Lions Cancer Foundation Uppsala and support from the Uppsala University and Uppsala County Council/Region agreement on medical training and clinical research (ALF)
REFERENCES
- 1. Dinmohamed AG, Szabo A, van der Mark M, et al. Improved survival in adult patients with acute lymphoblastic leukemia in the Netherlands: a population‐based study on treatment, trial participation and survival. Leukemia. 2016;30:310‐317. [DOI] [PubMed] [Google Scholar]
- 2. Dores GM, Devesa SS, Curtis RE, Linet MS, Morton LM. Acute leukemia incidence and patient survival among children and adults in the United States, 2001–2007. Blood. 2012;119:34‐43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Toft N, Schmiegelow K, Klausen TW, Birgens H Adult acute lymphoblastic leukaemia in Denmark. A national population‐based retrospective study on acute lymphoblastic leukaemia in Denmark 1998–2008. Br J Haematol. 2012;157:97‐104. [DOI] [PubMed] [Google Scholar]
- 4. Guru Murthy GS, Venkitachalam R, Mehta P. Trends in survival outcomes of B‐lineage acute lymphoblastic leukemia in elderly patients: analysis of Surveillance, Epidemiology, and End Results database. Leuk Lymphoma. 2015;56:2296‐2300. [DOI] [PubMed] [Google Scholar]
- 5. Igwe IJ, Yang D, Merchant A, et al. The presence of Philadelphia chromosome does not confer poor prognosis in adult pre‐B acute lymphoblastic leukaemia in the tyrosine kinase inhibitor era ‐ a surveillance, epidemiology, and end results database analysis. Br J Haematol. 2017;179:618‐626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Huguet F, Leguay T, Raffoux E, et al. Pediatric‐inspired therapy in adults with Philadelphia chromosome‐negative acute lymphoblastic leukemia: the GRAALL‐2003 study. J Clin Oncol. 2009;27:911‐918. [DOI] [PubMed] [Google Scholar]
- 7. DeAngelo DJ, Stevenson KE, Dahlberg SE, et al. Long‐term outcome of a pediatric‐inspired regimen used for adults aged 18–50 years with newly diagnosed acute lymphoblastic leukemia. Leukemia. 2015;29:526‐534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Toft N, Birgens H, Abrahamsson J, et al. Toxicity profile and treatment delays in NOPHO ALL2008‐comparing adults and children with Philadelphia chromosome‐negative acute lymphoblastic leukemia. Eur J Haematol. 2016;96:160‐169. [DOI] [PubMed] [Google Scholar]
- 9. Huguet F, Chevret S, Leguay T, et al. Intensified therapy of acute lymphoblastic leukemia in adults: report of the randomized GRAALL‐2005 Clinical Trial. J Clin Oncol. 2018;36(24):2514–2523 Jco2017768192 [DOI] [PubMed] [Google Scholar]
- 10. Ribera JM, Garcia O, Gil C, et al. Comparison of intensive, pediatric‐inspired therapy with non‐intensive therapy in older adults aged 55–65 years with Philadelphia chromosome‐negative acute lymphoblastic leukemia. Leuk Res. 2018;68:79‐84. [DOI] [PubMed] [Google Scholar]
- 11. Ottmann OG, Wassmann B, Pfeifer H, et al. Imatinib compared with chemotherapy as front‐line treatment of elderly patients with Philadelphia chromosome‐positive acute lymphoblastic leukemia (Ph+ALL). Cancer. 2007;109:2068‐2076. [DOI] [PubMed] [Google Scholar]
- 12. Vignetti M, Fazi P, Cimino G, et al. Imatinib plus steroids induces complete remissions and prolonged survival in elderly Philadelphia chromosome‐positive patients with acute lymphoblastic leukemia without additional chemotherapy: results of the Gruppo Italiano Malattie Ematologiche dell'Adulto (GIMEMA) LAL0201‐B protocol. Blood. 2007;109:3676‐3678. [DOI] [PubMed] [Google Scholar]
- 13. Brissot E, Labopin M, Beckers MM, et al. Tyrosine kinase inhibitors improve long‐term outcome of allogeneic hematopoietic stem cell transplantation for adult patients with Philadelphia chromosome positive acute lymphoblastic leukemia. Haematologica. 2015;100:392‐399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chalandon Y, Thomas X, Hayette S, et al. Randomized study of reduced‐intensity chemotherapy combined with imatinib in adults with Ph‐positive acute lymphoblastic leukemia. Blood. 2015;125:3711‐3719. [DOI] [PubMed] [Google Scholar]
- 15. Rousselot P, Coude MM, Gokbuget N, et al. Dasatinib and low‐intensity chemotherapy in elderly patients with Philadelphia chromosome‐positive ALL. Blood. 2016;128:774‐782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Juliusson G, Billstrom R, Gruber A, et al. Attitude towards remission induction for elderly patients with acute myeloid leukemia influences survival. Leukemia. 2006;20:42‐47. [DOI] [PubMed] [Google Scholar]
- 17. Juliusson G, Antunovic P, Derolf A, et al. Age and acute myeloid leukemia: real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood. 2009;113:4179‐4187. [DOI] [PubMed] [Google Scholar]
- 18. Juliusson G, Karlsson K, Hallbook H. Population‐based analyses in adult acute lymphoblastic leukemia. Blood. 2010;116(6):1011‐1011; author reply 1012. [DOI] [PubMed] [Google Scholar]
- 19. Kozlowski P, Astrom M, Ahlberg L, et al. High curability via intensive reinduction chemotherapy and stem cell transplantation in young adults with relapsed acute lymphoblastic leukemia in Sweden 2003–2007. Haematologica. 2012;97:1414‐1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kozlowski P, Astrom M, Ahlberg L, et al. High relapse rate of T cell acute lymphoblastic leukemia in adults treated with Hyper‐CVAD chemotherapy in Sweden. Eur J Haematol. 2014;92:377‐381. [DOI] [PubMed] [Google Scholar]
- 21. Kozlowski P, Lennmyr E, Ahlberg L, et al. Age but not Philadelphia positivity impairs outcome in older/elderly patients with acute lymphoblastic leukemia in Sweden. Eur J Haematol. 2017;99(2):141–149. [DOI] [PubMed] [Google Scholar]
- 22. https://www.cancercentrum.se/samverkan/cancerdiagnoser/blod-lymfom-myelom/akut-lymfatiskt-leukemi-all/kvalitetsregister/
- 23. Hallbook H, Simonsson B, Ahlgren T, et al. High‐dose cytarabine in upfront therapy for adult patients with acute lymphoblastic leukaemia. Br J Haematol. 2002;118:748‐754. [DOI] [PubMed] [Google Scholar]
- 24. Toft N, Birgens H, Abrahamsson J, et al. Results of NOPHO ALL2008 treatment for patients aged 1–45 years with acute lymphoblastic leukemia. Leukemia. 2018;32:606‐615. [DOI] [PubMed] [Google Scholar]
- 25. Kantarjian HM, O'Brien S, Smith TL, et al. Results of treatment with hyper‐CVAD, a dose‐intensive regimen, in adult acute lymphocytic leukemia. J Clin Oncol. 2000;18:547‐561. [DOI] [PubMed] [Google Scholar]
- 26. Reiter A, Schrappe M, Tiemann M, et al. Improved treatment results in childhood B‐cell neoplasms with tailored intensification of therapy: A report of the Berlin‐Frankfurt‐Munster Group Trial NHL‐BFM 90. Blood. 1999;94:3294‐3306. [PubMed] [Google Scholar]
- 27. Hoelzer D, Walewski J, Dohner H, et al. Improved outcome of adult Burkitt lymphoma/leukemia with rituximab and chemotherapy: report of a large prospective multicenter trial. Blood. 2014;124:3870‐3879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Moorman AV, Chilton L, Wilkinson J, Ensor HM, Bown N, Proctor SJ. A population‐based cytogenetic study of adults with acute lymphoblastic leukemia. Blood. 2010;115:206‐214. [DOI] [PubMed] [Google Scholar]
- 29. Preti HA, O'Brien S, Giralt S, Beran M, Pierce S, Kantarjian HM. Philadelphia‐chromosome‐positive adult acute lymphocytic leukemia: characteristics, treatment results, and prognosis in 41 patients. Am J Med. 1994;97:60‐65. [DOI] [PubMed] [Google Scholar]
- 30. Cytogenetic abnormalities in adult acute lymphoblastic leukemia: correlations with hematologic findings outcome. A Collaborative Study of the Group Francais de Cytogenetique Hematologique. Blood. 1996;87:3135‐3142. [PubMed] [Google Scholar]
- 31. Pullarkat V, Slovak ML, Kopecky KJ, Forman SJ, Appelbaum FR. Impact of cytogenetics on the outcome of adult acute lymphoblastic leukemia: results of Southwest Oncology Group 9400 study. Blood. 2008;111:2563‐2572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Wetzler M, Dodge RK, Mrozek K, et al. Prospective karyotype analysis in adult acute lymphoblastic leukemia: the cancer and leukemia Group B experience. Blood. 1999;93:3983‐3993. [PubMed] [Google Scholar]
- 33. Chiaretti S, Vitale A, Cazzaniga G, et al. Clinico‐biological features of 5202 patients with acute lymphoblastic leukemia enrolled in the Italian AIEOP and GIMEMA protocols and stratified in age cohorts. Haematologica. 2013;98:1702‐1710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Secker‐Walker LM, Prentice HG, Durrant J, Richards S, Hall E, Harrison G. Cytogenetics adds independent prognostic information in adults with acute lymphoblastic leukaemia on MRC trial UKALL XA. MRC Adult Leukaemia Working Party. Br J Haematol. 1997;96:601‐610. [DOI] [PubMed] [Google Scholar]
- 35. Gökbuget N. How I treat older patients with ALL. Blood. 2013;122:1366‐1375. [DOI] [PubMed] [Google Scholar]
- 36. Maury S, Chevret S, Thomas X, et al. Rituximab in B‐Lineage Adult Acute Lymphoblastic Leukemia. N Engl J Med. 2016;375:1044‐1053. [DOI] [PubMed] [Google Scholar]
- 37. Rosko AE, Wang HL, de Lima M, et al. Reduced intensity conditioned allograft yields favorable survival for older adults with B‐cell acute lymphoblastic leukemia. Am J Hematol. 2017;92:42‐49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Jones GL, Will A, Jackson GH, Webb NJ, Rule S. Guidelines for the management of tumour lysis syndrome in adults and children with haematological malignancies on behalf of the British Committee for Standards in Haematology. Br J Haematol. 2015;169:661‐671. [DOI] [PubMed] [Google Scholar]
- 39. Rousselot P, Coudé MM, Gokbuget N, et al. Dasatinib and low-intensity chemotherapy in elderly patients with Philadelphia chromosome-positive ALL. Blood 2016. 128(6):774-782. 10.1182/blood-2016-02-700153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Giebel S, Labopin M, Potter M, et al. Comparable results of autologous and allogeneic haematopoietic stem cell transplantation for adults with Philadelphia‐positive acute lymphoblastic leukaemia in first complete molecular remission: An analysis by the Acute Leukemia Working Party of the EBMT. Eur J Cancer. 2018;96:73‐81. [DOI] [PubMed] [Google Scholar]
- 41. Short NJ, Jabbour E, Sasaki K, et al. Impact of complete molecular response on survival in patients with Philadelphia chromosome‐positive acute lymphoblastic leukemia. Blood. 2016;128:504‐507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Miller KC, Al‐Kali A, Shah MV, et al. Elderly acute lymphoblastic leukemia: a Mayo Clinic study of 124 patients. Leuk Lymphoma. 2019;60(4):990‐999. [DOI] [PubMed] [Google Scholar]
- 43. Legrand O, Marie JP, Marjanovic Z, et al. Prognostic factors in elderly acute lymphoblastic leukaemia. Br J Haematol. 1997;97:596‐602. [DOI] [PubMed] [Google Scholar]
- 44. Pulte D, Jansen L, Gondos A, et al. Survival of adults with acute lymphoblastic leukemia in Germany and the United States. PLoS ONE. 2014;9:e85554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Dhedin N, Huynh A, Maury S, et al. Role of allogeneic stem cell transplantation in adult patients with Ph‐negative acute lymphoblastic leukemia. Blood. 2015;125(16):2486‐2496. quiz:2586. [DOI] [PubMed] [Google Scholar]
- 46. Giebel S, Marks DI, Boissel N, et al. Hematopoietic stem cell transplantation for adults with Philadelphia chromosome‐negative acute lymphoblastic leukemia in first remission: a position statement of the European Working Group for Adult Acute Lymphoblastic Leukemia (EWALL) and the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. 2018. [Epub ahead of print]. 10.1038/s41409-018-0373-4 [DOI] [PubMed] [Google Scholar]
- 47. Baumer JH, Mott MG. Sex and prognosis in childhood acute lymphoblastic leukaemia. Lancet. 1978;2:128‐129. [DOI] [PubMed] [Google Scholar]
- 48. Robak T, Szmigielska‐Kaplon A, Wrzesien‐Kus A, et al. Acute lymphoblastic leukemia in elderly: the Polish Adult Leukemia Group (PALG) experience. Ann Hematol. 2004;83:225‐231. [DOI] [PubMed] [Google Scholar]
- 49. Booth CM, Tannock IF. Randomised controlled trials and population‐based observational research: partners in the evolution of medical evidence. Br J Cancer. 2014;110:551‐555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Estey EH, Gale RP, Sekeres MA. New drugs in AML: uses and abuses. Leukemia. 2018;32:1479‐1481. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials