

Abstract
Aim
The open‐label, nonrandomized, phase II APEC study enrolled 167 patients with RAS wild‐type (wt) metastatic colorectal cancer (mCRC) to investigate the safety and efficacy of first‐line, every‐2‐weeks cetuximab plus investigator's choice of FOLFIRI or FOLFOX in this patient population.
Methods
A subgroup analysis of the APEC study population by primary tumor location was performed.
Results
A total of 130 patients (81.8%) had left‐sided and 29 (18.2%) had right‐sided mCRC. Median progression‐free survival (PFS), overall survival (OS) and overall response rate (ORR) were 14.0 months, 30.6 months and 68.5% for patients with left‐sided tumors and 8.9 months, 24.6 months and 51.7% for patients with right‐sided mCRC, concurring with pivotal phase III trial results. In patients with right‐sided tumors, median PFS was 15.4 months vs 8.3 months with cetuximab plus FOLFIRI vs cetuximab plus FOLFOX, respectively; median OS was 32.1 months vs 21.8 months with cetuximab plus FOLFIRI vs cetuximab plus FOLFOX, respectively.
Conclusion
The APEC tumor‐location subgroup analysis results were largely consistent with available literature regarding the equivalent efficacy of cetuximab plus FOLFIRI/FOLFOX in patients with left‐sided RAS wt mCRC. A trend toward improved efficacy with cetuximab plus FOLFIRI compared with cetuximab plus FOLFOX was observed in patients with right‐sided tumors; however, a direct comparison between groups cannot be made due to the nonrandomized study design. Nevertheless, the similar ORR observed with either chemotherapy backbone in patients with right‐sided RAS wt mCRC suggests a potential role for both regimens in this patient population when cytoreduction is a treatment goal.
Keywords: cetuximab, metastatic colorectal cancer, tumor location
1. BACKGROUND
Patients who present with metastatic colorectal cancer (mCRC) receive systemic therapy consisting of a targeted monoclonal antibody (mAb) and a chemotherapy backbone, and therapy selection is generally guided by one or more biomarkers (most commonly, mutations in the rat sarcoma [RAS] family genes). It is recommended that patients with mCRC that is RAS wild‐type (wt) receive an anti–epidermal growth factor receptor (EGFR) targeted therapy.1
Cetuximab, an immunoglobulin G1 (IgG1)‐isotype anti‐EGFR mAb, has been shown in several randomized, phase III trials to combine successfully, with similar efficacy and safety, with either of the doublet chemotherapy regimens available for the treatment of mCRC: FOLFIRI (infusional fluorouracil [5‐FU]/leucovorin/irinotecan) or FOLFOX (infusional 5‐FU/oxaliplatin/folinic acid [leucovorin]).2, 3 Currently, median survival in trials for patients with RAS wt mCRC receiving systemic therapy is ≥30 months,2, 3 although certain patient subpopulations have worse prognoses.4, 5 The location of the primary tumor within the colorectal tract (right vs left) has significant prognostic value for patient survival. Indeed, patients with right‐sided RAS wt tumors have a worse prognosis—that is, much poorer survival outcomes than patients with left‐sided tumors, regardless of the treatment received. In addition, right‐sidedness appears to have predictive value, as patients with right‐sided RAS wt mCRC have been shown to derive less benefit from treatment with cetuximab than patients with left‐sided RAS wt mCRC. By comparison, patients with left‐sided RAS wt tumors appear to fare better if treated with anti‐EGFR therapy plus chemotherapy versus bevacizumab plus chemotherapy.3, 6
The open‐label, nonrandomized, multicenter, phase II APEC trial demonstrated that first‐line cetuximab administered once every 2 weeks in combination with investigator's choice of either FOLFOX or FOLFIRI yielded good response and survival outcomes in an Asian patient population with RAS wt mCRC, with no new or unexpected safety findings.7 Furthermore, the APEC trial found no evidence for differences in efficacy between FOLFIRI and FOLFOX chemotherapy when combined with cetuximab in patients with RAS wt mCRC.7 In this subgroup analysis, we present the efficacy outcomes of the APEC trial by chemotherapy backbone for each tumor location.
2. METHODS
Detailed design and methodology for the nonrandomized, phase II APEC study (NCT00778830) were previously described.7 The trial was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the ethics committees of all participating centers. All patients gave written informed consent before trial entry.
Briefly, 289 patients with previously untreated KRAS exon 2 (codon 12/13) wt mCRC and an Eastern Cooperative Oncology Group performance status of 0 or 1 were enrolled and assigned to a treatment by participating investigators (cetuximab plus FOLFIRI, n = 101; cetuximab plus FOLFOX, n = 188). Of these, 167 patients had RAS wt disease according to extended RAS analysis (cetuximab plus FOLFIRI, n = 57; cetuximab plus FOLFOX, n = 110). In this population, 159 patients were evaluable for outcome analysis by tumor location. Transverse colon tumors were included in the analysis and classified as right‐sided.
Patients received cetuximab (500 mg/m2) on day 1 of every 14‐day treatment cycle over 120 min for the first infusion, 90 min at the second infusion and 60 min at subsequent infusions. Based on investigator's choice, patients received either FOLFOX (oxaliplatin 100 mg/m2, leucovorin 200 mg/m2 L‐form or 400 mg/m2 racemic, then 5‐FU as a 400‐mg/m2 IV bolus and a 2400‐mg/m2 continuous infusion over 46 hours) or FOLFIRI (irinotecan 180 mg/m2, leucovorin 200 mg/m2 L‐form or 400 mg/m2 racemic, then 5‐FU as a 400‐mg/m2 IV bolus and a 2400‐mg/m2 continuous infusion over 46 hours). Treatment was continued until disease progression, unacceptable toxicity or withdrawal of patient consent. All patients included in this analysis received ≥1 dose of treatment.
The primary endpoint of the APEC trial was best overall response rate (ORR) as determined by Response Evaluation Criteria In Solid Tumors (RECIST) 1.0. Secondary endpoints included progression‐free survival (PFS), overall survival (OS) and safety. Statistical analysis was performed as previously described.7
3. RESULTS
A total of 130 patients with left‐sided RAS wt mCRC were identified (43 received every‐2‐weeks cetuximab plus FOLFIRI and 87 received every‐2‐weeks cetuximab plus FOLFOX). Twenty‐nine patients with right‐sided RAS wt mCRC were identified; 10 patients received cetuximab plus FOLFIRI and 19 received cetuximab plus FOLFOX. Baseline characteristics such as number of metastatic sites, presence of liver‐limited disease, and median age were reasonably balanced between tumor‐location subgroups who received cetuximab plus FOLFIRI or cetuximab plus FOLFOX. 4.6% and 24.1% of patients with left‐ and right‐sided mCRC, respectively, had BRAF mutations. Detailed baseline characteristics by tumor location and treatment arm are shown in Table 1.
Table 1.
Baseline characteristics by tumor sidedness in the phase II APEC study
| Patients with left‐sided mCRC | Patients with right‐sided mCRC | |||||
|---|---|---|---|---|---|---|
| Characteristic | Cetuximab + FOLFIRI (n = 43) | Cetuximab + FOLFOX (n = 87) | Total (n = 130) | Cetuximab + FOLFIRI (n = 10) | Cetuximab + FOLFOX (n = 19) | Total (n = 29) |
| Sex, n (%) | ||||||
| Male | 27 (62.8) | 59 (57.8) | 86 (66.2) | 7 (70.0) | 11 (57.9) | 18 (62.1) |
| Female | 16 (37.2) | 28 (32.2) | 44 (33.8) | 3 (30.0) | 8 (42.1) | 11 (37.9) |
| Age, years | ||||||
| Median | 56.0 | 59.0 | 57.5 | 59.5 | 53.0 | 56.0 |
| Min–max | 31–87 | 28–81 | 28–87 | 41–70 | 31–78 | 31–78 |
| Race, n (%) | ||||||
| White | 6 (14.0) | 16 (18.4) | 22 (16.9) | 2 (20.0) | 2 (10.5) | 4 (13.8) |
| Asian (Chinese) | 31 (72.1) | 42 (48.3) | 73 (56.2) | 7 (70.0) | 11 (57.9) | 18 (62.1) |
| Asian (non‐Chinese) | 6 (14.0) | 29 (33.3) | 35 (26.9) | 1 (10.0) | 6 (31.6) | 7 (24.1) |
| ECOG PS, n (%) | ||||||
| 0 | 28 (65.1) | 61 (70.1) | 89 (68.5) | 8 (80.0) | 10 (52.6) | 18 (62.1) |
| 1 | 15 (34.9) | 26 (29.9) | 41 (31.5) | 2 (20.0) | 9 (47.4) | 11 (37.9) |
| Number of metastatic sites, n (%) | ||||||
| 0 | 1 (2.3) | 0 | 1 (0.8) | 0 | 0 | 0 |
| 1 | 10 (23.3) | 23 (26.4) | 33 (25.4) | 2 (20.0) | 3 (15.8) | 5 (17.2) |
| 2 | 18 (41.9) | 32 (36.8) | 50 (38.5) | 5 (50.0) | 11 (57.9) | 16 (55.2) |
| 3 | 8 (18.6) | 23 (26.4) | 31 (23.8) | 1 (10.0) | 2 (10.5) | 3 (10.3) |
| >3 | 6 (14.0) | 9 (10.3) | 15 (11.5) | 2 (20.0) | 3 (15.8) | 5 (17.2) |
| Metastatic disease, n (%) | ||||||
| Liver metastasis only | 14 (32.6) | 26 (29.9) | 40 (30.8) | 5 (50.0) | 7 (36.8) | 12 (41.1) |
| Other metastasis | 28 (65.1) | 61 (70.1) | 89 (68.5) | 5 (50.0) | 12 (63.2) | 17 (58.6) |
| No metastasis | 1 (2.3) | 0 | 1 (0.8) | 0 | 0 | 0 |
| BRAF status, n (%) | ||||||
| Wild‐type | 39 (90.7) | 85 (97.7) | 124 (95.4) | 9 (90.0) | 13 (68.4) | 22 (75.9) |
| Mutated | 4 (9.3) | 2 (2.3) | 6 (4.6) | 1 (10.0) | 6 (31.6) | 7 (24.1) |
| Prior therapy, n (%) | ||||||
| Chemotherapy | 20 (46.5) | 18 (20.7) | 38 (29.2) | 2 (20.0) | 3 (15.8) | 5 (17.2) |
| Radiotherapy | 8 (18.6) | 10 (11.5) | 18 (13.8) | 1 (10.0) | 0 | 1 (3.4) |
| Surgery | 32 (74.4) | 62 (71.3) | 94 (72.3) | 4 (40.0) | 18 (94.7) | 22 (75.9) |
| Vaccines | 0 | 0 | 0 | 1 (10.0) | 0 | 1 (3.4) |
| Other | 2 (4.7) | 2 (2.3) | 4 (3.1) | 1 (10.0) | 1 (5.3) | 2 (6.9) |
Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; FOLFOX, infusional fluorouracil, oxaliplatin, and leucovorin; FOLFIRI, infusional fluorouracil, leucovorin, and irinotecan; mCRC, metastatic colorectal cancer.
Median PFS for the total population of patients with RAS wt left‐sided mCRC in the APEC study (n = 130) was 14.0 months (95% [confidence interval] CI, 11.4–14.9), and median OS was 30.6 months (95% CI, 25.7–34.3). Median PFS for the total population of patients with RAS wt right‐sided mCRC in the APEC study (n = 29) was 8.9 months (95% CI, 5.5–15.4), and median OS was 24.6 months (95% CI, 13.8–31.2; Figure 1). Median PFS in patients with left‐sided tumors was 12.8 months (95% CI, 9.7–14.9) with cetuximab plus FOLFIRI and 14.2 months (95% CI, 11.2–16.2) with cetuximab plus FOLFOX. Median PFS in patients with right‐sided mCRC was 15.4 months (95% CI, 3.6–20.3) and 8.3 months (95% CI, 3.7–13.3) with cetuximab plus FOLFIRI or FOLFOX, respectively (Table 2, Figure 2). Median OS was 31.7 months (95% CI, 18.5–40.5) and 30.6 months (95% CI, 24.5–36.8) for patients with left‐sided tumors who received cetuximab plus FOLFIRI or FOLFOX, respectively. Median OS was 32.1 months (95% CI, 6.8–not evaluable) and 21.8 months (95% CI, 7.8–29.7) with cetuximab plus FOLFIRI or FOLFOX, respectively, in patients with right‐sided mCRC (Table 2, Figure 2).
Figure 1.
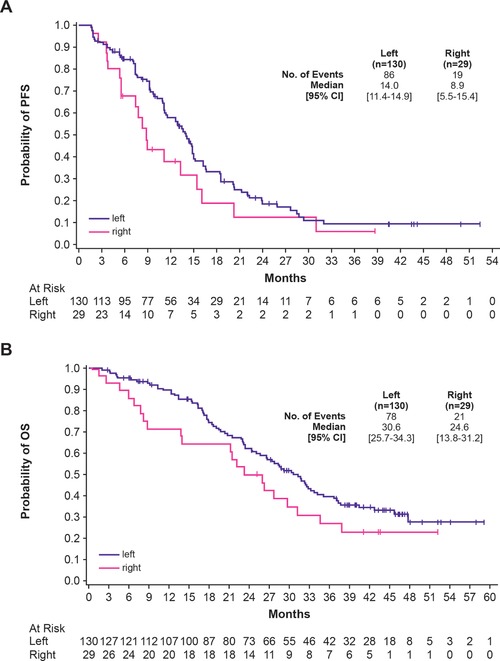
Progression‐free survival (A) and overall survival (B) according to sidedness group treated with either chemotherapy backbone in the phase II APEC study [Color figure can be viewed at http://wileyonlinelibrary.com]
Table 2.
Efficacy outcomes for cetuximab + FOLFOX and cetuximab + FOLFIRI by tumor sidedness in patients with RAS wt mCRC in the phase II APEC study
| Patients with left‐sided mCRC | Patients with right‐sided mCRC | |||||
|---|---|---|---|---|---|---|
| Efficacy outcome | Cetuximab + FOLFIRI (n = 43) | Cetuximab + FOLFOX (n = 87) | Total (n = 130) | Cetuximab + FOLFIRI (n = 10) | Cetuximab + FOLFOX (n = 19) | Total (n = 29) |
| Progression‐free survival, months | ||||||
| Median | 12.8 | 14.2 | 14.0 | 15.4 | 8.3 | 8.9 |
| 95% CI | 9.7–14.9 | 11.2–16.2 | 11.4–14.9 | 3.6–20.3 | 3.7–13.3 | 5.5–15.4 |
| Overall survival, months | ||||||
| Median | 31.7 | 30.6 | 30.6 | 32.1 | 21.8 | 24.6 |
| 95% CI | 18.5–40.5 | 24.5–36.8 | 25.7–34.3 | 6.8–NE | 7.8–29.7 | 13.8–31.2 |
| Response rate, % | ||||||
| Overall response rate | 74.4 | 65.5 | 68.5 | 50.0 | 52.6 | 51.7 |
| 95% CI | 58.8–86.5 | 54.6–75.4 | 59.7–76.3 | 18.7–81.3 | 28.9–75.6 | 32.5–70.6 |
| Resection rate, n (%) | 1 (2.3) | 13 (14.9) | 14 (10.8) | 1 (10.0) | 2 (10.5) | 3 (10.3) |
Abbreviations: FOLFOX, infusional fluorouracil, oxaliplatin, and leucovorin; FOLFIRI, infusional fluorouracil, leucovorin, and irinotecan; mCRC, metastatic colorectal cancer; NE, not evaluable; wt, wild type.
Figure 2.
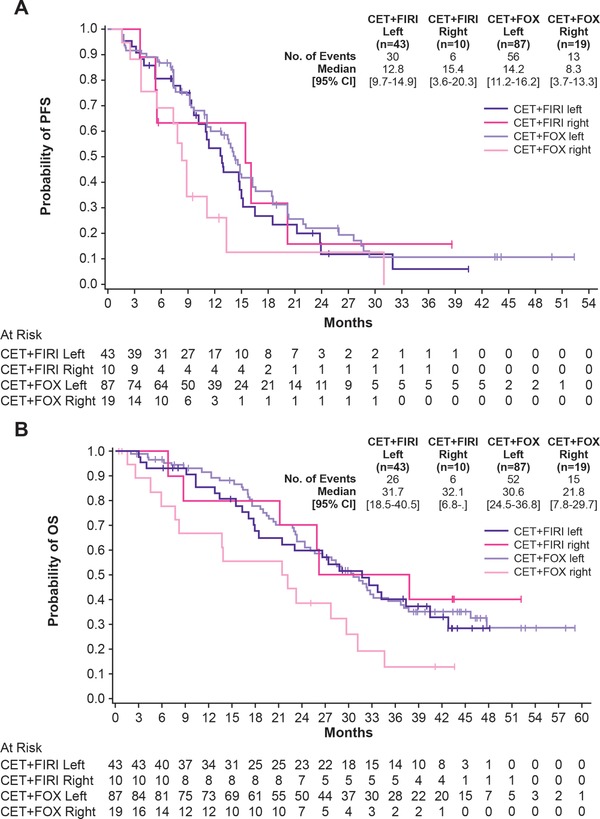
Progression‐free survival (A) and overall survival (B) according to treatment and sidedness group in the phase II APEC study [Color figure can be viewed at http://wileyonlinelibrary.com]
The ORR, which included complete and partial responses, observed with cetuximab plus FOLFIRI or FOLFOX in patients with left‐sided mCRC was 74.4% (95% CI, 58.8–86.5) and 65.5% (95% CI, 54.6–75.4), respectively. The ORR with cetuximab plus FOLFIRI or FOLFOX in patients with right‐sided mCRC was 50.0% (95% CI, 18.7–81.3) and 52.6% (95% CI, 28.9–75.6), respectively.
Few patients in the APEC trial underwent surgery for metastatic disease, but resection rates were similar between the left‐sided and right‐sided subgroups (10.8% and 10.3%, respectively).
The APEC study revealed no new safety findings for first‐line, every‐2‐weeks cetuximab plus doublet chemotherapy, mirroring the results from previous (including phase III) studies;2, 7, 8, 9 no safety analysis was performed for this tumor‐location subgroup analysis because, per data from the CRYSTAL (unpublished) and TAILOR trials,10 there is no evidence that the safety profile differs meaningfully between right‐ and left‐sided mCRC.
4. DISCUSSION
Here we present the tumor‐location subgroup analysis of the phase II APEC study population of patients with RAS wt mCRC. This is the first study to provide tumor‐location analyses for subgroups treated with the combination of every‐2‐weeks cetuximab plus FOLFIRI and cetuximab plus FOLFOX in parallel, and this thus serves as a hypothesis‐generating landmark study. Because the APEC study was not randomized, the distribution of patients with left‐sided versus right‐sided tumors as well as that of patients receiving FOLFOX versus FOLFIRI may be unbalanced; therefore, outcomes by tumor side and by chemotherapy backbone are not directly comparable. Other limitations of the study were the small sample size and the lack of a bevacizumab comparator arm.
Chemotherapy backbone did not appear to affect the outcomes in patients with left‐sided RAS wt tumors because median PFS and OS were similar in both groups. Furthermore, both treatment combinations yielded a median OS of >30 months for these patients, in agreement with observations made in pivotal phase III studies in which cetuximab was administered on a weekly schedule.2, 3 Curiously, the data for both PFS and OS observed in patients with right‐sided RAS wt tumors suggested better outcomes with the FOLFIRI backbone than FOLFOX. Indeed, while the number of patients with right‐sided RAS wt mCRC in the APEC study was very low, every‐2‐weeks cetuximab plus FOLFIRI was associated with a median OS of >30 months compared with 21.8 months with FOLFOX in this subgroup. Additionally, first‐line cetuximab in combination with either chemotherapy backbone yielded ORRs of ≥50.0% in patients with right‐sided tumors and a similar rate of resection of metastases to that observed in patients with left‐sided tumors, which is consistent with the ORRs reported for patients with right‐sided RAS wt mCRC in the CRYSTAL (42% with cetuximab plus FOLFIRI), FIRE‐3 (53% with cetuximab plus FOLFIRI) and TAILOR (44% with cetuximab plus FOLFOX) studies.3, 10 Therefore, this study provides further evidence that this may potentially be a preferred combination therapy for right‐sided mCRC when cytoreduction is a key treatment goal. Thus, first‐line cetuximab plus FOLFOX or FOLFIRI can be considered for right‐sided RAS wt mCRC when the patient requires rapid tumor shrinkage to improve symptoms or facilitate resection. Finally, in agreement with previous observations, both cetuximab plus FOLFIRI and cetuximab plus FOLFOX yielded high response rates in patients with left‐sided RAS wt mCRC.3
Although the higher rate of BRAF mutations in cetuximab plus FOLFOX–treated patients with right‐sided disease may partially explain dissimilarities in PFS and OS between the FOLFOX and FOLFIRI cohorts, another possible explanation for the observed trends may be that the synergy between cetuximab and irinotecan observed in preclinical models11, 12 is sufficient to overcome some of the molecular mechanisms that limit the benefits of antitumor therapy in right‐sided mCRC. This was reinforced clinically in the BOND study, in which patients who were resistant to irinotecan had improved ORR and PFS when treated with cetuximab and irinotecan compared to cetuximab alone.13 Further investigation of these findings is required.
Consistent with pivotal phase III studies in first‐line weekly cetuximab plus chemotherapy, a prognostic effect of tumor sidedness was observed in patients with RAS wt mCRC receiving first‐line every‐2‐weeks cetuximab plus doublet chemotherapy in the APEC study. We suggest that the results of the tumor‐location subgroup analysis of the APEC trial confirm published observations on the efficacy of first‐line cetuximab in combination with either FOLFIRI or FOLFOX in patients with left‐sided tumors. Indeed, there appears to be no difference in survival between chemotherapy backbones on the left side. Additionally, the ORR in patients with right‐sided RAS wt mCRC was ≥50.0% in both treatment subgroups, providing evidence for the use of first‐line cetuximab plus FOLFIRI or FOLFOX in this patient population when tumor shrinkage/cytoreduction is a key treatment goal. Finally, the results of this subgroup analysis raise the possibility of a clinically relevant synergy between cetuximab and irinotecan, which may be associated with prolonged PFS and OS in patients with right‐sided RAS wt tumors; further investigation of this observation is warranted. In summary, these results serve to generate interesting hypotheses regarding the choice of chemotherapy backbone with first‐line cetuximab for the treatment of patients with right‐sided mCRC.
CONFLICT OF INTEREST
R.E. is an employee of Merck Healthcare KGaA, and holds shares of Merck Healthcare KGaA. W.C. is an employee of Merck Serono, China. P.G. has received research funding support from Merck Healthcare KGaA. All other authors declare no conflict of interest.
ACKNOWLEDGMENTS
Medical writing assistance was provided by Clinical Thinking, Inc. and funded by Merck Healthcare KGaA, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Clinical trial registration: NCT00778830.
AVAILABILITY OF DATA AND MATERIAL
All authors had access to the primary data.
AUTHORS’ CONTRIBUTIONS
All authors contributed equally to the conception of the intellectual content, interpretation of the data and writing of the manuscript. All authors also reviewed any revisions that were made and provided their final approval of the manuscript.
Price T, Shen L, Ma B, et al. Phase II APEC trial: The impact of primary tumor side on outcomes of first‐line cetuximab plus FOLFOX or FOLFIRI in patients with RAS wild‐type metastatic colorectal cancer. Asia‐Pac J Clin Oncol. 2019;15:225–230. 10.1111/ajco.13154
Funding Information The trial was sponsored by Merck Healthcare KGaA, Darmstadt, Germany.
Robert Lim is currently associated with Icon SOC, Singapore.
REFERENCES
- 1. Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27:1386‐1422. [DOI] [PubMed] [Google Scholar]
- 2. Venook AP, Niedzwiecki D, Lenz HJ, et al. Effect of first‐line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild‐type advanced or metastatic colorectal cancer: a randomized clinical trial. JAMA. 2017;317:2392‐2401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Tejpar S, Stintzing S, Ciardiello F, et al. Prognostic and predictive relevance of primary tumor location in patients with RAS wild‐type metastatic colorectal cancer: retrospective analyses of the CRYSTAL and FIRE‐3 trials. JAMA Oncol. 2017;3:194‐201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Pietrantonio F, Petrelli F, Coinu A, et al. Predictive role of BRAF mutations in patients with advanced colorectal cancer receiving cetuximab and panitumumab: a meta‐analysis. Eur J Cancer. 2015;51:587‐594. [DOI] [PubMed] [Google Scholar]
- 5. Rowland A, Dias MM, Wiese MD, et al. Meta‐analysis of BRAF mutation as a predictive biomarker of benefit from anti‐EGFR monoclonal antibody therapy for RAS wild‐type metastatic colorectal cancer. Br J Cancer. 2015;112:1888‐1894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Venook AP, Niedzwiecki D, Innocenti F, et al. Impact of primary (1°) tumor location on overall survival (OS) and progression‐free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): analysis of CALGB/SWOG 80405 (Alliance). American Society of Clinical Oncology 2016 Annual Meeting; June 03–07, 2016; Chicago, IL.
- 7. Cheng AL, Cornelio G, Shen L, et al. Efficacy, tolerability, and biomarker analyses of once‐every‐2‐weeks cetuximab plus first‐line FOLFOX or FOLFIRI in patients with KRAS or all RAS wild‐type metastatic colorectal cancer: the phase 2 APEC study. Clin Colorectal Cancer. 2016;16:e73‐e88. [DOI] [PubMed] [Google Scholar]
- 8. Heinemann V, von Weikersthal LF, Decker T, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first‐line treatment for patients with metastatic colorectal cancer (FIRE‐3): a randomised, open‐label, phase 3 trial. Lancet Oncol. 2014;15:1065‐1075. [DOI] [PubMed] [Google Scholar]
- 9. Van Cutsem E, Lenz HJ, Köhne CH, et al. Fluorouracil, leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancer. J Clin Oncol. 2015;33:692‐700. [DOI] [PubMed] [Google Scholar]
- 10. Qin S, Li J, Wang L, et al. Efficacy and tolerability of first‐line cetuximab plus leucovorin, fluorouracil, and oxaliplatin (FOLFOX‐4) versus FOLFOX‐4 in patients with RAS wild‐type metastatic colorectal cancer: the open‐label, randomized, phase III TAILOR trial. J Clin Oncol. 2018. 10.1200/JCO.2018.78.3183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Liu X, Guo WJ, Zhang XW, Cai X, Tian S, Li J. Cetuximab enhances the activities of irinotecan on gastric cancer cell lines through downregulating the EGFR pathway upregulated by irinotecan. Cancer Chemother Pharmacol. 2011;68:871‐878. [DOI] [PubMed] [Google Scholar]
- 12. Mahtani RL, Macdonald JS. Synergy between cetuximab and chemotherapy in tumors of the gastrointestinal tract. Oncologist. 2008;13:39‐50. [DOI] [PubMed] [Google Scholar]
- 13. Gil Delgado M, Spano JP, Khayat D. Cetuximab plus irinotecan in refractory colorectal cancer patients. Expert Rev Anticancer Ther. 2007;7:407‐413. [DOI] [PubMed] [Google Scholar]