

Abstract
Why are some children more socially anxious than others? One theory holds that socially anxious children are poor mindreaders, which hampers their social interactions; another that socially anxious children are advanced mindreaders leading to heightened self‐consciousness in social situations. To test these theories simultaneously, this study (N = 105, ages 8–12) assessed children's mindreading (accuracy in detecting mental states from the eye region), self‐consciousness (indexed as physiological blushing during public performance), and social anxiety levels. Results support both theories, showing a quadratic relation between mindreading and social anxiety. Low mindreading was related to clinical levels of social anxiety. High mindreading was related to subclinical levels of social anxiety through blushing. Our findings suggest two social‐cognitive pathways to heightened social anxiety.
From an early age, children are motivated to bond with others. In order to form and maintain such bonds, they internalize the norms of the group they belong to and they care about the impression they make on others (Gilbert & Trower, 2001; Tomasello, 2009). In late childhood and at the emergence of adolescence, relationships with others become increasingly important (Beidel & Turner, 1988). Consequently, at this age, children's concerns with being evaluated unfavorably increase (Westenberg, Drewes, Goedhart, Siebelink, & Treffers, 2004). For some children, these evaluative concerns become excessive, giving rise to high levels of social anxiety (Ollendick, Benoit, & Grills‐Taquechel, 2014).
Heightened social anxiety refers to the excessive fear of negative evaluation in social situations in which an individual is exposed to the possible judgment of others (American Psychiatric Association, 2013). Although it is clear that increased social anxiety is rooted in heightened concerns about being evaluated negatively by others (Clark & Wells, 1995; Rapee & Heimberg, 1997), it is less clear what underlies these concerns. Scholars have long speculated that these concerns result from impaired social cognition, that is, the abilities to understand other people (Banerjee & Henderson, 2001; Hezel & McNally, 2014; O'Toole, Hougaard, & Mennin, 2013). One such ability, the ability to accurately detect others’ mental states based on external cues (i.e., mindreading; Baron‐Cohen, Jolloffe, Mortimore, & Robertson, 1997), may be of particular importance for the development of evaluative fears and heightened social anxiety. This study investigated mindreading ability in relation to childhood social anxiety.
Mindreading
Mindreading allows people “to put themselves into the mind of the other person, and ‘tune in’ to their mental state” (Baron‐Cohen, Wheelwright, Hill, Raste, & Plumb, 2001, p. 241). Thus, mindreading enables the detection and recognition of others’ mental states based on external cues, such as people's facial expressions (Baron‐Cohen et al., 1997; Domes, Heinrichs, Michel, Berger, & Herpertz, 2007). For example, people may identify someone's sadness based on his or her facial expressions or someone's focus of attention based on his or her gaze.
Mindreading paves the way for more complex forms of mental state understanding, such as reasoning about mental states in the service of predicting and explaining others’ actions (Sabbagh, 2004). For example, people may infer that a person is sad because he or she did poorly on an exam only if they first recognized that the person is sad based on the sad facial expression (Sabbagh, 2004; Washburn, Wilson, Roes, Rnic, & Harkness, 2016). Thus, people are able to interpret and reason about others’ mental states accurately only if they are successful in recognizing those mental states.
One of the most commonly used tasks to assess the mindreading ability is the Reading the Mind in the Eyes Task (RMET; Baron‐Cohen et al., 2001), which asks people to recognize other people's mental states based on cues from the face. Unlike tests that require interpreting and reasoning about mental states, such as standard Theory of Mind tasks (Wellman & Liu, 2004), the Happé's Strange Stories (Happé, 1994), the Faux Pas Test (Baron‐Cohen, O'riordan, Stone, Jones, & Plaisted, 1999), and the Social Situations Task (Rogers, Viding, Blair, Frith, & Happe, 2006), the RMET is solely a mindreading test (Fertuck et al., 2009). Thus, the RMET indexes mindreading ability but not necessarily the ability to reason about others’ mental states and predict future actions (Baron‐Cohen et al., 2001).
Mindreading and Social Anxiety
Although a number of past studies have investigated sociocognitive skills in socially anxious children, the knowledge about mindreading ability in socially anxious children is currently scarce. Mindreading requires detection of peoples’ mental states based on external cues, most commonly facial expressions. Facial expressions are a major source of information about other people's mental states (Planalp, DeFrancisco, & Rutherford, 1996) and are particularly relevant for socially anxious individuals for whom others’ facial expressions may signal disapproval or rejection (Rapee & Heimberg, 1997). Thus, the ability to decode others’ facial expressions in order to recognize others’ mental states is especially relevant to study in socially anxious individuals as they may be particularly prone to show disturbances in this ability (Hezel & McNally, 2014; Washburn et al., 2016).
There are two overarching theories about the disturbances in mindreading related to social anxiety. One theory, which we refer to as the sociocognitive deficit theory, holds that poor mindreading ability may lead to a lack of or inaccurate beliefs about others, which can make social situations unpredictable and uncomfortable, resulting in fear and social anxiety (Hezel & McNally, 2014; O'Toole et al., 2013). Another theory, which we refer to as the advanced sociocognitive ability theory, holds that although advanced mindreading ability is typically advantageous in social settings, it may also lead to heightened self‐consciousness in social situations (Bechtoldt & Schneider, 2016), which, in turn, leads to more evaluative concerns and social anxiety (Hope & Heimberg, 1988; Tibi‐Elhanany & Shamay‐Tsoory, 2011). This study aims to integrate these two theories and put them to the test in the critical age of preadolescence.
Sociocognitive Deficit Theory
Socially anxious children are concerned with how other people may evaluate them and often fear and avoid social situations (Beidel, Turner, & Dancu, 1985; Bögels et al., 2010; Hudson & Rapee, 2000). The fear and avoidance of social situations may be rooted in children's deficits in recognizing other people's mental states and, consequently, poor understanding of other people's intentions and behaviors in social situations (Carpendale & Lewis, 2004; Colonnesi, Nikolić, de Vente, & Bögels, 2017). Not being able to decode accurately how other people feel or what other people think may lead to inaccurate beliefs about others and their behaviors. This may increase confusion and unpredictability in social situations, which may lead to fear and social anxiety (Colonnesi et al., 2017; O'Toole et al., 2013). Supporting this perspective, two studies found that adults with social anxiety disorder have more difficulties recognizing other people's mental states than adults without social anxiety disorder (Hezel & McNally, 2014; Washburn et al., 2016). Evidence in children is, however, currently lacking.
Past studies that investigated other sociocognitive abilities, but not mindreading specifically, discovered deficits in understanding others’ emotions in children with high social anxiety levels (Colonnesi et al., 2017) and adults with social anxiety disorder (O'Toole et al., 2013). Children with anxiety disorders (Broeren & Muris, 2009) and adults with social anxiety disorder (Hezel & McNally, 2014; Washburn et al., 2016) have also been found to display deficits in Theory of Mind—the ability to predict others’ behaviors based on their mental states (Wellman, 1990). Moreover, children with high social anxiety levels—particularly those with high levels of shy negative affect—have been found to display deficits in more complex sociocognitive skills, such as understanding others’ motives for deceptive self‐presentational displays as well as the ability to identify and interpret the consequences of an unintended faux pas (Banerjee & Henderson, 2001). Children with high social anxiety levels have also been found to display difficulties in attending to audience characteristics and adjusting to the attributes and preferences of a particular audience (Banerjee & Watling, 2010). Finally, children with anxiety disorders have been found to fail to cope with social exclusion by attending to others’ mental states, which indicates deficits in mental state understanding in affectively charged contexts (White et al., 2016). In sum, a number of past studies have suggested that deficits in sociocognitive skills may be related to greater social anxiety.
Advanced Sociocognitive Ability Theory
Typically, advanced sociocognitive abilities are seen as socially advantageous because they allow children to recognize and understand how their friends and significant others feel and think (Cutting & Dunn, 2002). This makes it easier for children to get along with others, have successful social interactions, and be prosocial (Caputi, Lecce, Pagnin, & Banerjee, 2012; Denham, 1986). However, advanced sociocognitive skills may also come at a cost: Children with advanced sociocognitive abilities may be more sensitive to other people's opinions of them and may easily become aware that they are an object of others’ attention and evaluation (Cutting & Dunn, 2002). This may give rise to heightened self‐consciousness and fear of negative evaluation—the core of social anxiety (Sutterby, Bedwell, Passler, Deptula, & Mesa, 2012). Thus, another theory of the role of sociocognitive abilities in social anxiety holds that advanced sociocognitive abilities may be related to social anxiety (Sutterby et al., 2012; Tibi‐Elhanany & Shamay‐Tsoory, 2011). According to this theory, individuals with advanced sociocognitive abilities, such as mindreading, spend more time observing others in social situations (Moore, Bosacki, & Macgillivray, 2011) and are more attuned to social cues from others (Baron‐Cohen et al., 2001). Consequently, they may easily become aware that they are a subject of other people's evaluation, which may be unfavorable and which can make them become highly self‐conscious (Bechtoldt & Schneider, 2016; Fenigstein, 1979). Heightened self‐consciousness in social situations, in turn, may lead to the increase in evaluative concerns (Banerjee, Benett, & Luke, 2012) and high levels of social anxiety (e.g., Hofmann, Heinrichs, & Moscovitch, 2004; Hope & Heimberg, 1988).
Although there is no direct support for advanced mindreading in socially anxious children, there is evidence of advanced mindreading in undergraduate female students with high levels of social anxiety (Sutterby et al., 2012). Also, there is indirect support for this theory from past studies that hypothesized that other sociocognitive abilities may be related to heightened social anxiety. For example, children with advanced Theory of Mind and emotion understanding have been found to be more sensitive to others’ criticism (Cutting & Dunn, 2002). Also, children and adolescents with advanced sociocognitive ability of recursive thinking were found to experience increased state anxiety (indexed as cortisol response) while anticipating giving a speech, suggesting that those with advanced social cognition may have evaluative concerns when anticipating being exposed to others’ evaluations (van den Bos, van Duijvenvoorde, & Westenberg, 2016). Finally, adults with social anxiety disorder have been found to attribute affective mental states to others more accurately than individuals without social anxiety disorder (Tibi‐Elhanany & Shamay‐Tsoory, 2011). Together, these studies suggest that advanced sociocognitive skills may be related to greater social anxiety.
Blushing As an Index of Heightened Self‐Consciousness and Its Relation to Social Anxiety
Heightened self‐consciousness in social situations refers to the increased awareness of the self as a social object (Buss, 1980; Schlenker & Leary, 1982). A physiological marker of heightened self‐consciousness in social situations is blushing (Bögels, Alberts, & de Jong, 1996; Buss, 1980; Crozier, 2012; Leary, Britt, Cutlip, & Templeton, 1992). Blushing is an involuntary reddening of the face, neck, or upper chest in socially charged situations (Drummond, 2012; Leary & Meadows, 1991). People blush when they are concerned that other people may evaluate them negatively (Buss, 1980; Crozier, 2012; Leary & Meadows, 1991). Because fear of negative evaluation is at the very core of social anxiety (American Psychiatric Association, 2013), socially anxious individuals are thought to be particularly prone to blushing (Bögels & Reith, 1999; Bögels et al., 2010; Nikolić, Colonnesi, Vente, Drummond, & Bögels, 2015).
Blushing is assumed to first develop when children acquire abilities for self‐awareness and for understanding other people's minds, which give rise to the realization that other people may evaluate them negatively (Leary et al., 1992; Lewis, 2001). Children, like adults, blush when they are concerned about others’ possible unfavorable evaluation (Darwin, 1872/1998). Children with high levels of social anxiety, thus, display increased blushing in social situations in which they are exposed to others’ evaluations (Nikolić, Brummelman, Colonnesi, de Vente, & Bögels, 2018; Nikolić, Colonnesi, de Vente, & Bögels, 2016; Nikolić, de Vente, Colonnesi, & Bögels, 2016). Because socially anxious individuals may overestimate the extent to which they blush in social situations (Nikolić et al., 2015), self‐reports of blushing may not be reliable. Unlike self‐reports of self‐consciousness, which rely on interoceptive awareness (Turner, Scheier, Carver, & Ickes, 1978), physiological blushing provides an objective measure of the experience of heightened self‐consciousness in ambiguous social situations (Crozier, 2004).
Present Study
The aim of this study was to integrate and test hypotheses stemming from the two theories on the role of sociocognitive abilities in childhood social anxiety simultaneously. In line with the sociocognitive deficit theory, we hypothesized that deficits in mindreading would be associated with greater social anxiety in children. In line with advanced sociocognitive ability theory, we hypothesized that advanced mindreading would be related to greater social anxiety. To integrate these hypotheses, we modeled a quadratic relation between mindreading and child social anxiety. We further assumed that advanced mindreading would be related to greater social anxiety indirectly through heightened self‐consciousness (indexed through blushing). We, thus, predicted that advanced mindreading would be associated with more blushing, which in turn would be related to higher levels of childhood social anxiety. We tested all these hypotheses simultaneously, in a partial moderated mediation model (Figure 1). According to this model, (a) lower mindreading is directly related to higher levels of social anxiety and, (b) at the same time, mindreading is related to higher levels of social anxiety indirectly, through blushing, but depending on the individual's level of mindreading. Specifically, only high (but not low) levels of mindreading are related to higher social anxiety through blushing. To test this model, we measured 8‐ to 12‐year‐old children's mindreading abilities, physiological blushing during public performance, and social anxiety reported by children and parents.
Figure 1.
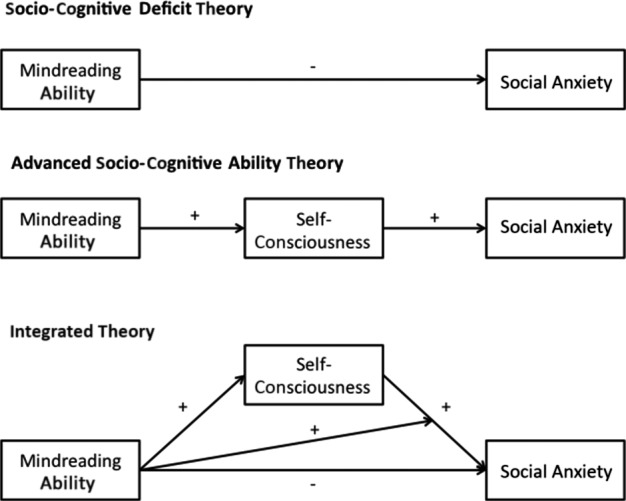
The moderated mediation model: Next to the direct negative effect of mindreading on social anxiety, the relation between mindreading and social anxiety is partially mediated by blushing but depending on the levels of mindreading. That is, blushing partially mediates the relation between high (but not low) mindreading and social anxiety. At low levels of mindreading, the model reduces to the sociocognitive deficit theory model; the lower the score on mindreading, the higher social anxiety, hence the greater the chances to develop clinical levels of social anxiety. At high levels of mindreading, the (positive) indirect effect from the advanced sociocognitive theory model dominates over the negative direct effect; children with high (but not low) levels of mindreading blush more, which in turn, relates to higher levels of social anxiety. At very high levels of mindreading, one, thus, also has higher chances to develop subclinical (and possibly clinical) levels of social anxiety.
Method
Participants
Participants were 105 children (56% girls) aged 8–12 (M = 9.50 years, SD = 1.18 year; 85% Caucasian) who were accompanied by one of their parents (77% mothers) aged 25–60 (M = 43.00 years, SD = 6.15 years) to the Family laboratory of the University of Amsterdam. They were recruited through public elementary schools in the Netherlands for a larger study about sociocognitive and physiological indices of social anxiety. Parents received information letters about the study, and those who signed in were invited to the laboratory. Families were recruited from low to upper‐class urban neighborhoods. Parents were relatively highly educated: 57% graduated from a university, 18% graduated from college, and 35% finished a high school or vocational education. Children received active informed parental consent prior to their participation in the study. The study was approved by the Ethics Review Board of the Faculty of Social and Behavioural Sciences at the University of Amsterdam.
Procedure and Measures
Social Anxiety
During the laboratory visit, both the child and the parent completed the Social Phobia and Anxiety Inventory adapted for children to index child's social anxiety (child report: Social Phobia and Anxiety Inventory for Children [SPAI‐C], parental report: SPAI‐C‐P, English version: Beidel, Turner, & Morris, 1995; Dutch version: Utens, Ferdinand, & Bögels, 2000). Both versions of the questionnaire consist of 26 items and a 3‐point Likert response scale (0 = never, 2 = always; child report: M = 11.99, SD = 8.19, α = .96; parental report: M = 11.43, SD = 8.56, α = .94). Sample items include: “I feel anxious when I am with other girls, boys, or adults and I am in the center of attention (when everyone is looking at me)” in the child report version and “My child feels anxious when she or he is with other girls, boys, or adults and she or he is in the center of attention (everyone is looking at her or him)” in the parent‐reported version.
Previous studies support the validity of the questionnaire. They have demonstrated high internal consistency of the SPAI‐C, α = .96 (Beidel, Turner, Hamlin, & Morris, 2000) and SPAI‐C‐P, α = .93 (Higa, Fernandez, Nakamura, Chorpita, & Daleiden, 2006). External and discriminative validity analyses have indicated that the SPAI can differentiate children with social anxiety disorder from children with other types of anxiety disorders as well as from healthy controls (Beidel et al., 2000). Mean scores of SPAI‐C for community samples reported in previous studies typically range from 9 to 11 (Aune & Stiles, 2009; Kuusikko et al., 2009; Storch, Masia‐Warner, Dent, Roberti, & Fisher, 2004). Mean scores of SPAI‐C for healthy controls range from 4 to 7 (Beidel et al., 1995; Kuusikko et al., 2009; Tuschen‐Caffier, Kühl, & Bender, 2011), whereas mean scores of SPAI‐C for subclinical levels of social anxiety disorder are around 13 (e.g., Tuschen‐Caffier et al., 2011). An empirically derived cut‐off score of 18 has been shown to best determine the presence or absence of social anxiety disorder (Beidel, Turner, & Morris, 1999), and this cut‐off score has been confirmed by studies in different samples (e.g., Kuusikko et al., 2009; Tuschen‐Caffier et al., 2011).
Of note, the average score of social anxiety in our sample was somewhat higher than those of other community samples (e.g., Aune & Stiles, 2009; Storch et al., 2004) and those of healthy control samples (e.g., Beidel et al., 2000; Tuschen‐Caffier et al., 2011), probably due to the self‐selection of our sample. Because our study was named “Shyness and self‐confidence in childhood,” parents with socially anxious children may have been more likely to participate.
Because child report and parent report were correlated in our study, r(95) = .50, p < .001, we first standardized the scores and then averaged them into a composite score of child social anxiety for the analyses. For the ease of interpretation and comparison with other samples, we report on unstandardized mean scores in descriptives and figures.
Mindreading
After completing the questionnaires, children joined the experimenter in the laboratory room where they sat in front of a computer screen and took part in the Child RMET (RMET‐C; Baron‐Cohen et al., 2001). The RMET‐C Test examines the mindreading ability of children (Baron‐Cohen et al., 2001). The test consists of 28 black‐and‐white photographs of the eye region of different people's faces, each depicting a specific state of mind (e.g., scared, happy, interested, thinking about something). The photographs appeared on the screen in front of the child along with four descriptions of different mental states beneath the picture. Each question contained one correct answer and three wrong answers. Children were asked to select the mental state that best described what the person in the photo was thinking or feeling. The number of correct responses was used to index the mindreading ability in children.
Blushing
Next, children were invited to sit in a chair in the same room and photoplethysmograph and thermometer sensors were attached to their right cheek to measure their blushing response. When sensors were attached, children sat silently and read a comic book for 2 min, during which we recorded the baseline blushing response. Afterward, children were invited to choose a song of their liking that they would perform on a podium. The children were informed that a woman would come into the room to record their performance and that she would give the recording to a “professional singer,” who would watch the recording of the performance in a room close by. After the woman with a camera entered the room and sat in front of the podium, the children were invited to stand on the podium and perform a song of their choice, in front of the experimenter and a camerawoman, who was “recording” the performance with a camera. After the child stood up, the experimenter announced the child's performance: “And now, [name of the child] will sing [name of the song] for us! You may begin!”. From this point, the blushing response to the performance was recorded (see Figure 2). All children sang for at least 30 s (mean duration = 51.94 s, SD = 20.17 s). To standardize the length of the blushing recording, the blushing response was calculated for the first 30 s of the performance because all children sang at least for 30 s.
Figure 2.

Experimental setting.
The blushing response during the 2‐min baseline and during the first 30 s of performance was measured with an infrared‐reflective photoplethysmograph device that was both direct current (DC) and alternating current (AC) coupled. The AC component represents the fast‐fluctuating blood flow depending on heart rate and corresponds to blood pulse amplitude (Allen, 2007). The DC component of the signal represents the static blood flow in the artery, vein, and tissue that varies slowly and corresponds to blood volume (Allen, 2007). The plethysmograph output signal was amplified and filtered (low‐pass, 0.75 Hz, 12 dB/oct for the “DC” signal; high pass, 0.5 Hz, 36 dB/oct for “AC” signal). The DC and AC output signals were converted to arbitrary values in the range of 0–65,535 (16‐bit ADC) at a speed of 200 S/s. Cheek temperature was monitored unilaterally with a platinum PT1000 temperature sensor fastened to the skin on the cheekbone, next to the infrared probe of the plethysmograph. To control for individual differences in skin characteristics, such as closeness and density of blood vessels (Drummond, 2012), we calculated the percentage increase from the 2‐min baseline to the first 30 s of the performance for all outcomes: blood pulse amplitude (AC reactivity), blood volume (DC reactivity), and cheek temperature (temperature reactivity). Higher values in reactivity indicate more blushing during the performance. Because this was the first study to measure blushing in older children, we did not have apriori hypotheses about how three indices of blushing would be related. The three physiological indices of blushing were not correlated (Table 1) and were analyzed as separate indices in the same models.
Table 1.
Descriptive Statistics and Correlations for Child's Mindreading, Mindreading2), AC Blushing, DC Blushing, Temperature Blushing, and Social Anxiety
| n | M (SD) | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|
| 1. Mindreading | 101 | 17.88 (3.27) | — | — | — | — | — |
| 2. Mindreading2 | 101 | 0.99 (1.16) | −.16 | — | — | — | — |
| 3. AC | 95 | 100.25 (103.02) | .26* | .04 | — | — | — |
| 4. DC | 94 | −11.48 (41.67) | .04 | .04 | −.04 | — | — |
| 5. Temperature | 94 | 1.01 (1.89) | −.16 | .14 | .08 | −.08 | — |
| 6. Social anxiety | 101 | 11.72 (7.35) | −.26** | .37* | .03 | .02 | .39*** |
Mindreading2 is squared mean‐centered mindreading variable. AC is blood pulse amplitude increase. DC is blood volume increase. Temperature is cheek temperature increase. Social anxiety is a standardized composite of child and parent report. AC = alternating current; DC = direct current.
*p < .050. **p < .010. ***p < .001.
Data Analyses
Detected outliers (± 3 SDs) were Winsorized by modifying their values to the closest observed values in the range of ± 3 SD (Keselman, Algina, Lix, Wilcox, & Deering, 2008). One outlier above the range of +3 SD was Winsorized for both AC and DC. To investigate whether both high and low mindreading relates to child social anxiety, we modeled a curvilinear relation between mindreading and childhood social anxiety. We computed mean centered mindreading2 and included it in the analyses next to the mindreading variable. In that way, we were able to investigate whether a significant quadratic relation existed next to the linear relation (Mc Donald, 2008). The curvilinear regression model was evaluated using IBM SPSS Statistics 24 (IBM Corporation, 2016).
To test our hypotheses leading to a quadratic relation between mindreading and social anxiety, that is, that low mindreading is directly related to high social anxiety, whereas mindreading is related to high social anxiety through blushing but depending on the level of mindreading, we fitted the moderated mediation model that is depicted in Figure 1. Specifically, we tested (a) whether lower mindreading predicted higher social anxiety directly; (b) whether the mediating role of self‐consciousness (indexed as blushing), in the relation between mindreading and social anxiety, existed next to the direct effect of mindreading on social anxiety; and (c) whether this partial mediation depended on the levels of mindreading, such that it existed only at high (not low) levels of mindreading.
The evaluation of this model was carried out step by step in R 3.2.3 (R Core Team, 2015) using the lavaan package (Rosseel, 2012). First, we fitted a saturated moderated mediation model based on our hypotheses. That is, both the blushing variables and mindreading were allowed to predict social anxiety, whereas levels of blushing and its effect on social anxiety were allowed to depend on mindreading. Residual variances and covariances were estimated freely. Next, we used model comparison to investigate whether the hypothesized mediation by blushing could be assumed full (no direct effect from mindreading to social anxiety), absent (only a direct effect from mindreading to social anxiety), or only partial (as the integrated model in Figure 1 implied). Subsequently, we investigated the roles of the different blushing indices (AC, DC, and temperature reactivity) in explaining the relation between mindreading and social anxiety. That is, one by one, we constrained the (moderated) path from a blushing measure to social anxiety to zero and evaluated the decrease in model fit. If this decrease would be significant, this would imply the (moderated) path was necessary; if not it could be removed from the model. This procedure resulted in a model in which only the necessary paths from different blushing indices to social anxiety were left. Next, we tested if the moderation itself was a necessary assumption or that mediation could exist without moderation. That is, we tested whether it is necessary to assume that the mediating role of blushing in the relation between mindreading and social anxiety indeed depends on the levels of mindreading. To do so, we fixed the moderation to zero. If this fixation would lead to a significant reduction in the model fit, the assumption of moderation would be necessary. Finally, we removed insignificant residual covariances to end up with a most parsimonious model. The results of both the saturated and the final model are reported in the result section.
To obtain parameter estimates and evaluate the goodness of fit of the path model, we used the maximum likelihood method. To overcome the concern regarding biased standard errors (e.g., due to the limited sample size), we calculated bias‐corrected bootstrap 95% confidence intervals (CIs) for all parameter estimates of the investigated effects with 5,000 replications. The maximum likelihood provided a chi‐square (χ2) test of model fit. A significant χ2 value indicates a discrepancy between the model implied and the observed covariance matrices, indicating that the model does not fit the data well. In addition to χ2, we used the root mean square error of approximation (RMSEA; Steiger & Lind, 1980), the comparative fit index (CFI; Bentler, 1990) and the Non‐Normed Fit Index (NNFI). RMSEA of .01, .05, and .08 indicates excellent, good, and mediocre fit, respectively (MacCallum, Browne, & Sugawara, 1996). CFI values above .95, and NNFI values above .90 indicate good fit (Hu & Bentler, 1999).
We compared nested models by means of log‐likelihood difference testing (at the significance level of α = .05). This results in a χ2‐statistic, where a significant difference indicates a significant difference in model fit. We compared non‐nested models using the Akaike information criterion (AIC; Akaike, 1987). The AIC penalizes for model complexity, and the lower the value the better the relative fit. We opted for full information maximum likelihood, in order to handle missing values, which were sporadically present. All tests were run at an alpha level of α = .05.
Results
Preliminary Analyses
Four children were excluded from the analyses because: (a) they were not fluent in Dutch (n = 1); (b) the electrodes for blushing were not properly attached to the cheek (n = 1); (c) the child was younger than 8 years old (n = 1); and (d) the child had an autism spectrum disorder diagnosis (n = 1). Eight children had missing values for physiological measures of blushing due to equipment failure. Children with missing values did not differ in their level of social anxiety from children without missing values in the analyses, t(103) = −0.21, p = .836.
Means, standard deviations, and zero‐order correlations between study variables are reported in Table 1. Higher mindreading was related to more blushing indexed through AC reactivity. Also, higher mindreading was related to lower levels of social anxiety. Mindreading2 was positively related to social anxiety. Finally, more blushing indexed through temperature reactivity was related to higher levels of social anxiety. Because none of the variables of interest was significantly related to age or sex, we did not include sex and age as covariates in the path models (all ps > .050).
Main Analyses
Quadratic Relation
To examine the hypothesized quadratic relation between mindreading and social anxiety, we first ran a regression analysis with mindreading and mean centered mindreading2 as predictors of childhood social anxiety. The model explained a significant amount of variance, R 2 = .18, F(2, 98) = 2.49, p < .001. The effect of the linear term was significant and negative, B = −1.57, β = −.21, SE = 0.69, 95% CI [−2.93, −0.21], p = .024. The effect of the quadratic term was significant as well, B = 18.58, β = .33, SE = 5.10, 95% CI [8.58, 28.58], p < .001, providing evidence for a quadratic relation between mindreading and social anxiety, with both lower and higher levels of mindreading relating to higher levels of social anxiety (Figure 3).
Figure 3.
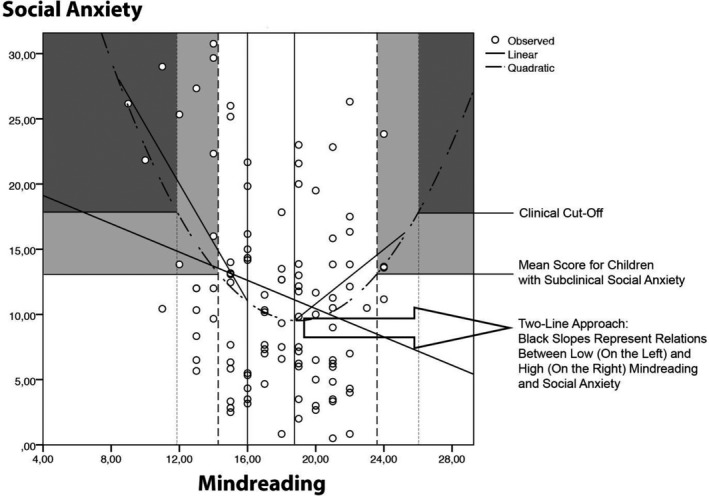
The relation between mindreading and social anxiety. On average, the relation is negative (dark gray straight line). However, the relation is curvilinear (semidotted black quadratic curve). The light gray and dark gray areas represent the regions at which mindreading levels predict subclinical and clinical levels of social anxiety, i.e., social anxiety scores of 13 and 18, respectively. Subclinical levels of social anxiety are predicted when mindreading scores are 13 or lower and 23 or higher; clinical levels of social anxiety are predicted when mindreading scores are 12 or lower and 26 or higher. At the mindreading scores of 21 or higher, the indirect effect of mindreading on social anxiety through blushing is significant.
Modeling a quadratic relation may, in some cases, suggest the existence of a quadratic trend when this trend actually does not exist (Simonsohn, 2017). Therefore, we additionally tested our hypotheses about both low and high mindreading being linked to higher social anxiety by employing the two‐lines approach (Simonsohn, 2017). Following this approach, two regression lines are fitted, one for “low” values of the predictor and another for the “high” values of the predictor. The quadratic relation is present if both slopes are statistically significant and have opposite signs. To overcome the concern regarding the limited sample size in these regression analyses (n = 38 for low scores and n = 31 for high scores), bias‐corrected bootstrap 95% CIs were calculated for the coefficients of the investigated effects with 1,000 replications. Breakpoints for lower and higher values of mindreading were set apriori following the RMET norms for children (Tonks, Williams, Frampton, Yates, & Slater, 2007). As children aged 9–12 on average score between 60% and 70% (16.8–19.6 correct answers), we set the breakpoint at 20 correct answers being the starting point for higher scores (30% of the total sample) and the breakpoint at 16 being the endpoint for lower scores (36% of the total sample) We separately fitted two regression lines for low and high scores of mindreading on child social anxiety. Both lines were significant and of opposite signs, β = −.42, B = −1.03, SE = 0.32, 95% CI [−1.62, −0.29], p = .009 for low scores and β = .34, B = 0.86, SE = 0.39, 95% CI [0.09, 1.62], p = .032 for high scores. Thus, the additional analysis confirmed that both lower and higher mindreading levels were linked to higher levels of child social anxiety.
Of note, the levels of social anxiety in children with low and high mindreading ability were not the same as can be seen from the asymmetrical shape of the function (Figure 3). The visual inspection of the figure reveals that, on one hand, at the lowest levels of mindreading, children reached the highest levels of social anxiety, which correspond to the levels of social anxiety found in children with diagnosed social anxiety disorder (e.g., Beidel et al., 2000; Kuusikko et al., 2009; Tuschen‐Caffier et al., 2011). On the other hand, at the highest levels of mindreading, children reached the levels of social anxiety that correspond to the levels of social anxiety found in children with subclinical levels of social anxiety (Tuschen‐Caffier et al., 2011).
Testing the Moderated Mediation Model
In line with the integrated theory, we modeled a moderated mediation model with blushing as a mediator of the relation between high (but not low) mindreading and child social anxiety (see Table 2 for models fit statistics, and Table 3 for effect sizes and CIs of the saturated model). This moderated mediation of blushing in the relation between mindreading and social anxiety was expected to be partial because we also assumed that mindreading related to social anxiety directly. The model fit comparison statistics showed that the partial mediation could not be omitted because the model with the full mediation resulted in a significant reduction in fit. Thus, a direct effect of mindreading on social anxiety was kept in the model. Next, removing the role of AC reactivity in the relation between mindreading and social anxiety resulted in a significant reduction in fit as well, and was retained in the model. The roles of DC and temperature reactivity in the relation between mindreading and social anxiety could be removed from the saturated model without significant reduction in model fit. Within that model, the moderation effect of mindreading on the relation between AC reactivity and social anxiety could not be removed without a significant worsening in model fit, so we retained it. Removing insignificant residual covariances led to a final model with 18 degrees of freedom. In this model, all residual covariances and correlations between interaction variables and mindreading were set to 0 (all were insignificant, as might be expected from the correlational structure among the blushing indices). For theoretical reasons, we kept the path from DC reactivity to social anxiety, despite it being insignificant. This final model did not fit significantly worse than the saturated model, Model 1, Δχ2(18) = 20.549, p = .303 and provided the lowest AIC. From this we conclude that: (a) the relation between mindreading and social anxiety was partially mediated, thus both the direct effect and indirect effect of mindreading on social anxiety existed; (b) AC reactivity (not DC or temperature reactivity) was the mediating variable in the relation between mindreading and social anxiety; and (c) that this partial mediation was moderated by mindreading. That is, AC reactivity mediated the relation between mindreading and social anxiety but depending on the level of mindreading. Specifically, AC reactivity mediated the relation between mindreading and social anxiety only for children with high levels of mindreading.
Table 2.
Model Fit Statistics for the Different Tested Models
| Model name | −2LL | χ2 | df | p | CFI | NNFI | RMSEA | RMSEA L | RMSEA U | RMSEA p | AIC | BIC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Saturated model | 4,178.45 | — | — | — | — | — | — | — | — | — | 4,266.45 | 4,381.51 |
| 2. No direct effect | 4,182.07 | 3.62 | 1 | .057 | 0.95 | −0.31 | .16 | .00 | .35 | .089 | 4,268.07 | 4,380.52 |
| 3. Role of AC removed | 4,190.64 | 12.19 | 2 | .002 | 0.82 | −1.55 | .23 | .12 | .35 | .007 | 4,274.64 | 4,384.48 |
| 4. Role of DC removed | 4,178.96 | 0.51 | 2 | .776 | 1.00 | 1.37 | .00 | .00 | .13 | .821 | 4,262.96 | 4,372.79 |
| 5. Role of temp removed | 4,183.60 | 5.16 | 2 | .076 | 0.94 | 0.21 | .13 | .00 | .26 | .127 | 4,267.60 | 4,377.44 |
| 6. Roles of both DC and temp removed | 4,184.38 | 5.93 | 4 | .205 | 0.97 | 0.76 | .07 | .00 | .18 | .318 | 4,264.38 | 4,368.98 |
| 7. Drop moderation | 4,188.52 | 10.07 | 5 | .073 | 0.91 | 0.49 | .10 | .00 | .19 | .152 | 4,266.52 | 4,368.51 |
| 8. Final model | 4,199.00 | 20.55 | 18 | .303 | 0.95 | 0.93 | .04 | .00 | .10 | .568 | 4,251.00 | 4,318.99 |
AC is blood pulse amplitude increase. DC is blood volume increase. Temp is cheek temperature increase. AC = alternating current; DC = direct current; CFI = comparative fit index; NNFI = Non‐Normed Fit Index; RMSEA = root mean square error of approximation; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Table 3.
Unstandardized and Standardized Coefficients for the Saturated Model
| Est | SE | SE boot | Bias | CI95Lower | CI95Upper | St. Est | |
|---|---|---|---|---|---|---|---|
| Direct effects | |||||||
| Mindreading on social anxiety | −1.35 | .70 | .84 | .06 | −3.01 | 0.29 | −.18 |
| Mindreading on AC reactivity | 2.17 | .82 | .85 | .00 | 0.71 | 4.03 | .26 |
| Mindreading on DC reactivity | 0.11 | .27 | .30 | .01 | −0.53 | 0.66 | .04 |
| Mindreading on temperature reactivty | −0.23 | .15 | .16 | .00 | −0.52 | 0.09 | −.16 |
| AC reactivity on social anxiety | −0.07 | .10 | .10 | .00 | −0.28 | 0.13 | −.07 |
| DC reactivity on social anxiety | 0.13 | .26 | .24 | −.02 | −0.32 | 0.62 | .04 |
| Temperature reactivity on social anxiety | 1.90 | .47 | .42 | .04 | 1.08 | 2.73 | .37 |
| Moderation effects | |||||||
| Mindreading × AC Reactivity on Social Anxiety | 0.19 | .08 | .09 | .00 | 0.02 | 0.38 | .25 |
| Mindreading × DC Reactivity on Social Anxiety | 0.12 | .21 | .25 | .02 | −0.32 | 0.64 | .06 |
| Mindreading × Temperature Reactivity on Social Anxiety | −0.60 | .36 | .34 | .02 | −1.22 | 0.12 | −.15 |
| Moderation indices | |||||||
| Social anxiety | 0.42 | .24 | .25 | .00 | 0.06 | 1.11 | .06 |
| AC reactivity | 0.01 | .04 | .09 | .02 | −0.10 | 0.31 | .00 |
| Temperature reactivity | 0.14 | .12 | .13 | .00 | −0.03 | 0.52 | .02 |
| Indirect effects | |||||||
| 1 SD below the mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivity | −0.56 | .40 | .46 | −.00 | −1.86 | 0.07 | −.08 |
| Mindreading on social anxiety via DC reactivity | 0.00 | .03 | .12 | −.03 | −0.21 | 0.27 | .00 |
| Mindreading on social anxiety via temperature reactivity | −0.58 | .39 | .43 | −.00 | −1.51 | 0.18 | −.08 |
| Mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivity | −0.15 | .22 | .25 | −.00 | −0.83 | 0.24 | −.02 |
| Mindreading on social anxiety via DC reactivty | 0.01 | .04 | .08 | −.01 | −0.08 | 0.35 | .00 |
| Mindreading on social anxiety via temperature reactivity | −0.44 | .30 | .32 | .00 | −1.12 | 0.14 | −.06 |
| 1 SD above the mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivity | 0.27 | .22 | .19 | −.00 | −0.02 | 0.75 | .05 |
| Mindreading on social anxiety via DC reactivty | 0.03 | .08 | .13 | .01 | −0.13 | 0.47 | .00 |
| Mindreading on social anxiety via temperature reactivity | −0.30 | .23 | .24 | .00 | −0.94 | 0.07 | −.03 |
AC reactivity is blood pulse amplitude increase. DC reactivity is blood volume increase. Temperature reactivity is temperature increase. AC = alternating current; DC = direct current.
The final model with the standardized estimates is depicted in Figure 4. The standardized and unstandardized paths and effects are displayed in Table 4, along with their CIs. When considering the individual parameters and their (bootstrapped) CIs, we can draw similar conclusions as above: there was a significant positive effect of mindreading on AC, and mindreading significantly moderated the effect of AC on social anxiety. As a result, the indirect effect of mindreading on social anxiety through AC was significantly moderated. In addition, according to the Johnson–Neyman region of significance procedure, the indirect effect became significant at levels of mindreading of about 1.1 SD above the mean, β = .06, B = 0.38, SE = 0.23, 95% CI [0.02, 0.90]. Thus, from a mindreading score of around 21, higher mindreading was significantly related to higher social anxiety levels through increased blushing.
Figure 4.
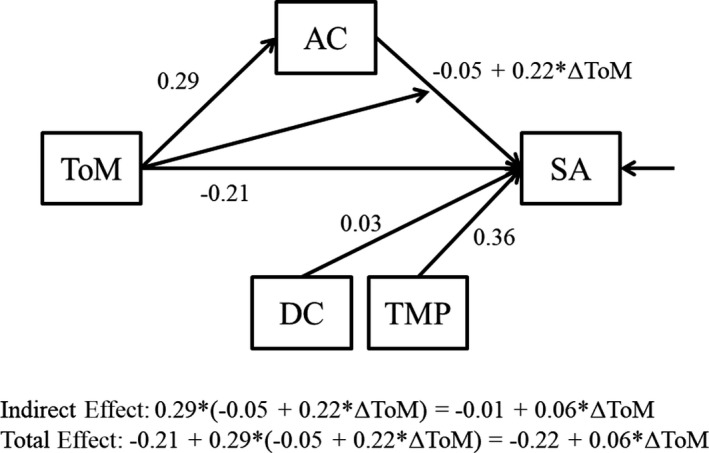
The final moderated mediation model including standardized estimates. AC = alternating current; DC = direct current; ToM = theory of mind; TMP = temperature; SA = social anxiety.
Table 4.
Unstandardized and Standardized Coefficients for the Final Model
| Est | SE | SE boot | Bias | CI95Lower | CI95Upper | St. Est | |
|---|---|---|---|---|---|---|---|
| Direct effects | |||||||
| Mindreading on social anxiety | −1.56 | .71 | .814 | .04 | −3.16 | −0.01 | −.21 |
| Mindreading on AC reactivity | 2.42 | .83 | .848 | .01 | 0.86 | 4.21 | .29 |
| AC reactivity on social anxiety | −0.05 | .10 | .101 | .00 | −0.25 | 0.15 | −.05 |
| DC reactivity on social anxiety | 0.09 | .26 | .237 | −.01 | −0.36 | 0.58 | .03 |
| Temperature reactivity on social anxiety | 1.86 | .48 | .441 | .03 | 0.10 | 2.75 | .36 |
| Moderation effects | |||||||
| Mindreading × AC Reactivity on Social Anxiety | 0.17 | .08 | .087 | .01 | 0.01 | 0.36 | .22 |
| Moderation indices | |||||||
| Social anxiety | 0.41 | .24 | .25 | .01 | 0.03 | 1.04 | .06 |
| Indirect effects | |||||||
| 1 SD below the mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivity | −0.52 | .42 | .467 | −.01 | −1.70 | 0.20 | −.08 |
| Mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivity | −0.11 | .24 | .258 | −.00 | −0.75 | 0.31 | −.02 |
| 1 SD above the mean level of mindreading | |||||||
| Mindreading on social anxiety via AC reactivty | 0.30 | .24 | .201 | .01 | −0.04 | 0.75 | .05 |
| “Total” effects | |||||||
| 1 SD below mean level of mindreading | −1.67 | .68 | .80 | .04 | −3.23 | −0.10 | −.22 |
| Mean level of mindreading | −2.07 | .74 | .90 | .03 | −3.92 | −0.37 | −.29 |
| 1 SD above mean level of mindreading | −1.26 | .70 | .77 | .05 | −2.81 | 0.23 | −.16 |
AC reactivity is blood pulse amplitude increase. DC reactivity is blood volume increase. Temperature reactivity is cheek temperature increase. AC = alternating current; DC = direct current.
In sum, these results are in support of our hypotheses that (a) lower mindreading is directly related to higher social anxiety, (b) higher mindreading is related to higher social anxiety indirectly, through blushing, (c) but this indirect effect of mindreading on social anxiety through blushing occurred only among children showing high levels of mindreading.
Discussion
Two theories about the role of social cognition in social anxiety exist: one holding that social anxiety is rooted in poor mindreading ability and another holding that social anxiety is rooted in advanced mindreading ability through increased self‐consciousness. In this study, we aimed to unify these two theories and test the integrative theory—that childhood social anxiety is associated with both low and advanced mindreading and that advanced mindreading is associated with social anxiety through heightened self‐consciousness. In support of this hypothesis, we found a quadratic relation between mindreading and childhood social anxiety, such that both poor and advanced mindreading abilities were related to higher childhood social anxiety levels. Advanced mindreading, but not low mindreading, was related to higher levels of social anxiety through increased blushing (AC, i.e., blood pulse amplitude). Thus, as hypothesized, advanced mindreading was related to heightened self‐consciousness indexed as more intense blushing, which, in turn, predicted greater childhood social anxiety. By unifying the two theories on the role of social cognition in social anxiety, our findings suggest two sociocognitive pathways to social anxiety in childhood.
Two Sociocognitive Pathways to Childhood Social Anxiety
In line with our integrated theory, the findings support the idea that there are two pathways to childhood social anxiety: one through deficits in sociocognitive abilities and another one through advanced sociocognitive abilities and heightened self‐consciousness. These findings have important implications for the cognitive models of social anxiety (Clark & Wells, 1995; Rapee & Heimberg, 1997). These models emphasize the role of negative interpretation bias in social anxiety, with socially anxious individuals interpreting ambiguous social cues as negative (Williams, Watts, MacLeod, & Mathews, 1988). Deficits in sociocognitive abilities, and low mindreading in particular, may facilitate this bias. Specifically, when children lack an ability to accurately assess how other people feel or think, there may be more room for social ambiguity and interpreting cues as negative.
To date, much less attention has been given to advanced sociocognitive abilities and heightened self‐consciousness in social anxiety. Although it has been assumed that socially anxious individuals are more self‐conscious in social situations than socially nonanxious individuals (e.g., Bögels et al., 1996; Hofmann, 2007), precursors of such heightened self‐consciousness in social anxiety have remained unknown. Here, we show that advanced social cognition, and mindreading in particular, is associated with heightened self‐consciousness indexed as blushing, which, in turn, relates to greater social anxiety. Thus, our study suggests that the impaired cognitive processes found in social anxiety may arise from both deficits and advanced sociocognitive abilities found in childhood.
Deficits in Sociocognitive Abilities and Childhood Social Anxiety
Our results showed that the levels of social anxiety were the highest at the lowest levels of mindreading. These levels of social anxiety have been previously reported in children with diagnosed social anxiety disorder (e.g., Beidel et al., 2000; Kuusikko et al., 2009; Tuschen‐Caffier et al., 2011). Therefore, our findings suggest that deficits in mindreading may be related to clinical levels of social anxiety. The finding that deficits in mindreading are associated with high social anxiety levels, and possibly social anxiety disorder, is in line with past studies that found that adults with social anxiety disorder show impairments in mindreading ability (Hezel & McNally, 2014; Washburn et al., 2016). These findings are also in line with some past studies in children that found deficits in other sociocognitive abilities, such as emotion understanding and Theory of Mind in relation to childhood social anxiety or to constructs closely related to social anxiety, such as temperamental shyness and behavioral inhibition (Banerjee & Henderson, 2001; Broeren & Muris, 2009; Colonnesi et al., 2017; White et al., 2016).
It is likely that children with deficits in mindreading display problems in social functioning because they have difficulties decoding others’ mental states, which in turn impairs their understanding of how other people feel and think. These difficulties may be an obstacle in predicting other people's behaviors in social situations. Ambiguity and uncertainty of others’ reactions may enhance confusion and fear in social situations that may, in the long run, lead to anxiety in social situations (Boelen & Reijntjes, 2009). Likely, social anxiety can also enhance the deficits in sociocognitive abilities because it may lead to fewer social experiences and fewer opportunities to “practice” social abilities, such as accurately detecting other people's mental states from external cues (Colonnesi et al., 2017). This may give rise to a vicious circle in which low sociocognitive abilities and high social anxiety reinforce each other over time. To reveal how this vicious circle between mindreading and social anxiety develops over time, longitudinal studies are needed.
Advanced Sociocognitive Abilities and Childhood Social Anxiety
To our knowledge, this study was the first to test the idea that advanced mindreading, and not only deficits in this ability, may relate to greater social anxiety in childhood. We found higher levels of mindreading to be related to greater social anxiety in children. This finding is in line with one past study that found advanced mindreading in highly socially anxious undergraduate female students (Sutterby et al., 2012) and with another study that found advanced emotion understanding in adults with social anxiety disorder (Tibi‐Elhanany & Shamay‐Tsoory, 2011). The finding is also in line with studies showing a positive relation between other sociocognitive skills and anxiety in children and adolescents (Cutting & Dunn, 2002; van den Bos et al., 2016).
We theorized that the advanced decoding of others’ mental states is related to child social anxiety because it gives rise to heightened self‐consciousness indexed as blushing, which, in turn, may lead to social anxiety. Our findings support this hypothesis. Children with advanced mindreading blush in social situations in which they are exposed to judgments of other people, likely because they easily become aware of the possibility that other people may judge them (and that this judgment may be negative). Blushing, in turn, may lead them to feel uncomfortable in social situations, behave more awkwardly, process social information in a biased way, and avoid similar situations in the future resulting in greater social anxiety in these children.
Our results showed that, with the increase in mindreading, children may reach heightened, subclinical levels of social anxiety (Tuschen‐Caffier et al., 2011). It might be possible that these slightly elevated levels of social anxiety are, in some cases, socially adaptive—because children with high mindreading abilities “read” others feelings and thoughts well, they may be more attentive to others and put more weight into what others think of them (Cutting & Dunn, 2002). This may direct them toward behaviors that promote cooperation and bonding with others (Gilbert & Trower, 2001). Future research should examine whether these elevated levels of social anxiety can indeed be adaptive for children's social functioning and whether children with high sociocognitive abilities are less likely to develop clinical levels of social anxiety than children with deficits in sociocognitive abilities.
Our results show that children with higher mindreading ability who blush in social settings show greater social anxiety. Yet, it is important to note that, after we account for this effect, children with higher mindreading, who do not blush in social situations, display lower levels of social anxiety. Thus, high mindreading, accompanied by a low blushing propensity, seems to be protective of high social anxiety levels. As many previous studies reported, children with highly developed sociocognitive skills seem to be socially competent and socially and academically successful (e.g., Trentacosta & Izard, 2007; Zerwas, Balaraman, & Brownell, 2004). This study adds to this accumulating evidence by showing that these children may also be at low risk for social anxiety but only when they are not highly self‐conscious.
Heightened Self‐Consciousness and Its Relation to Mindreading and Childhood Social Anxiety
The results of this study revealed, for the first time, that physiological blushing is related to sociocognitive abilities. Since Darwin (1872/1998), there has been an idea that blushing can appear only when certain sociocognitive abilities are acquired. This study shows that, indeed, better sociocognitive abilities are related to more blushing in social situations in which a child is exposed to others’ evaluations of them. Our study was also the first to find that blushing is related to social anxiety in the critical age of preadolescence, which extends previous findings on the relation between blushing and social anxiety in young children (Nikolić, Colonnesi, et al., 2016; Nikolić, de Vente, et al., 2016) and adults (Nikolić et al., 2015).
Of note, blushing indexed as blood pulse amplitude (AC) was related to mindreading and mediated the relation between advanced mindreading and social anxiety. Cheek temperature reactivity was related to social anxiety directly, regardless of the level of mindreading. Changes in blood pulse amplitude and temperature were not related. This is likely because blood pulse amplitude and temperature changes capture different aspects of the blush response. Blood pulse amplitude is a fast‐changing component of blood flow, whereas temperature changes occur slowly and are delayed compared to the fast‐changing blood pulse amplitude (Cooper & Gerlach, 2012; Drummond, 2012; Shearn, Bergman, Hill, Abel, & Hinds, 1990). Fast changes in blood flow are assumed to reflect transient states of embarrassment marked by short blushes that disappear quickly (Voncken & Bögels, 2009), whereas more slowly occurring changes in the blush response may reflect blushing that results from social stress due to prolonged social exposure (Nikolić, Colonnesi, et al., 2016; Voncken & Bögels, 2009). It is, thus, possible that children with advanced social understanding blushed while performing because they felt foolish and embarrassed by performing in front of others. Other children, who reacted with heightened temperature, may have blushed because they felt distressed in this situation. Because we did not have a priori hypotheses about how different indices of blushing would relate to mindreading and social anxiety, our explanation is post hoc and should be verified by future research.
Finally, blood volume was not related to other blushing indices, nor to mindreading and social anxiety. Similarly, in the only previous study that measured physiological blushing in young children, blood volume was not related to children's social anxiety, whereas blood pulse amplitude and temperature were related to children's social anxiety (Nikolić, Colonnesi, et al., 2016). It could, therefore, be that blood volume is not a valid measure to capture the blush response in childhood.
Limitations and Future Directions
Our study should be considered in view of some limitations. First, our sample consisted of Dutch children from urban neighborhoods. It would be interesting to investigate how sociocognitive abilities are related to social anxiety in other, for example, non‐Western cultures in which social norms and expectations, as well as the prevalence of social anxiety, differ compared to the Western cultures. Second, our study included a community non‐at‐risk sample of children; thus, we cannot generalize our findings to clinical samples of children. Future studies should include children with social anxiety disorder in order to investigate these processes in clinical populations. Nevertheless, our findings have important clinical implications showing that deficits in mindreading may be found in children with clinical levels of social anxiety. Mindreading could, therefore, be targeted in early childhood as a risk factor for the development of social anxiety disorder. Third, our study targeted one sociocognitive ability, namely mindreading. Thus, we cannot generalize on all aspects of social cognition. Future studies could also investigate curvilinear relations between other aspects of social cognition, such as emotion understanding and predicting others’ behaviors based on their mental states and childhood social anxiety. Fourth, our study was correlational precluding the investigations of the causal role of self‐consciousness in the relation between advanced mindreading and social anxiety. Future studies that investigate these relations may profit from using experimental designs to manipulate self‐consciousness. Finally, in our two‐lines approach, the analyses were conducted with two groups of children with high versus low mindreading ability, limiting the sample size; future studies employing this approach may benefit from larger sample sizes.
Conclusion
This study offers the first empirical evidence that socially anxious children display both low and advanced mindreading. Thus, there may be two sociocognitive pathways to high childhood social anxiety levels: one through deficits in mindreading and another one through advanced mindreading and heightened self‐consciousness. Whereas deficits in mindreading may pose risk for social anxiety disorder, high mindreading abilities may result in social sensitivity that is reflected in increased self‐consciousness and heightened concerns about others’ evaluations that do not necessarily develop in a disorder. Nevertheless, both of these disturbances in sociocognitive abilities may have an impact on children's social functioning in every‐day life leading them to fear and avoid social situations. Early prevention or intervention efforts targeting social anxiety may focus on children's sociocognitive abilities. For children with deficits in mindreading, these efforts may focus on enhancing sociocognitive abilities, whereas for children with advanced mindreading, they may focus on tackling the excessive mindreading and dealing with heightened self‐consciousness and sensitivity to others’ opinions.
This study was supported by an Innovation Research Vici NWO grant, number 453‐09‐001 to Susan M. Bögels. The writing of this article was supported, in part, by funding from the European Union's Horizon 2020 Research and innovation program under the Marie Sklodowska‐Curie grant agreement No 705217 to Eddie Brummelman. Milica Nikolić and Lisa van der Storm contributed equally to the study and, therefore, share first authorship.
References
- Akaike, H. (1987). Factor analysis and AIC. Psychometrika, 52, 317 10.1007/BF02294359 [DOI] [Google Scholar]
- Allen, J. (2007). Photoplethysmography and its application in clinical physiological measurement. Physiological Measurement, 28, 1–39. 10.1088/0967-3334/28/3/R01 [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author. [Google Scholar]
- Aune, T. , & Stiles, T. C. (2009). The effects of depression and stressful life events on the development and maintenance of syndromal social anxiety: Sex and age differences. Journal of Clinical Child & Adolescent Psychology, 4, 501–512. 10.1080/15374410902976304 [DOI] [PubMed] [Google Scholar]
- Banerjee, R. , Benett, M. , & Luke, N. (2012). Children's reasoning about self‐presentation following rule violations: The role of self‐focused attention. Child Development, 83, 1805–1821. 10.1111/j.1467-8624.2012.01813.x [DOI] [PubMed] [Google Scholar]
- Banerjee, R. , & Henderson, L. (2001). Social‐cognitive factors in childhood social anxiety: A preliminary investigation. Social Development, 10, 558–572. 10.1111/1467-9507.00180 [DOI] [Google Scholar]
- Banerjee, R. , & Watling, D. (2010). Self‐presentational features in childhood social anxiety. Journal of Anxiety Disorders, 1, 34–41. 10.1016/j.janxdis.2009.08.004 [DOI] [PubMed] [Google Scholar]
- Baron‐Cohen, S. , Jolloffe, T. , Mortimore, C. , & Robertson, M. (1997). Another advanced theory of mind: Evidence from very high functioning adults with autism or Asperger syndrome. Journal of Child Psychology and Psychiatry, 7, 813–822. 10.1111/j.1469-7610.1997.tb01599.x [DOI] [PubMed] [Google Scholar]
- Baron‐Cohen, S. , O'riordan, M. , Stone, V. , Jones, R. , & Plaisted, K. (1999). Recognition of faux pas by normally developing children and children with Asperger syndrome or high‐functioning autism. Journal of Autism and Developmental Disorders, 29, 407–418. 10.1023/a:1023035012436 [DOI] [PubMed] [Google Scholar]
- Baron‐Cohen, S. , Wheelwright, S. , Hill, J. , Raste, Y. , & Plumb, I. (2001). The “Reading the Mind in the Eyes” test revised version: A study with normal adults, and adults with Asperger syndrome or high‐functioning autism. Journal of Child Psychology and Psychiatry, 42, 241–251. 10.1017/S0021963001006643 [DOI] [PubMed] [Google Scholar]
- Bechtoldt, M. N. , & Schneider, V. K. (2016). Predicting stress from the ability to eavesdrop on feelings: Emotional intelligence and testosterone jointly predict cortisol reactivity. Emotion, 16, 815–825. 10.1037/emo0000134 [DOI] [PubMed] [Google Scholar]
- Beidel, D. C. , & Turner, S. M. (1988). Comorbidity of test anxiety and other anxiety disorders in children. Journal of Abnormal Child Psychology, 16, 275–287. 10.1007/BF00913800 [DOI] [PubMed] [Google Scholar]
- Beidel, D. C. , Turner, S. M. , & Dancu, C. V. (1985). Physiological, cognitive and behavioral aspects of social anxiety. Behaviour Research and Therapy, 23, 109–117. 10.1016/0005-7967(85)90019-1 [DOI] [PubMed] [Google Scholar]
- Beidel, D. C. , Turner, S. M. , Hamlin, K. , & Morris, T. L. (2000). The social phobia and anxiety inventory for children (SPAI–C): External and discriminative validity. Behavior Therapy, 31, 75–87. 10.1016/S0005-7894(00)80005-2 [DOI] [Google Scholar]
- Beidel, D. C. , Turner, S. M. , & Morris, T. L. (1995). A new inventory to assess childhood social anxiety and phobia: The social phobia and anxiety inventory for children. Psychological Assessment, 1, 73–79. 10.1037/1040-3590.7.1.73 [DOI] [Google Scholar]
- Beidel, D. C. , Turner, S. M. , & Morris, T. L. (1999). Psychopathology of childhood social phobia. Journal of the American Academy of Child & Adolescent Psychiatry, 6, 643–650. 10.1097/00004583-199906000-00010. [DOI] [PubMed] [Google Scholar]
- Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246. 10.1037/0033-2909.107.2.238 [DOI] [PubMed] [Google Scholar]
- Boelen, P. A. , & Reijntjes, A. (2009). Intolerance of uncertainty and social anxiety. Journal of Anxiety Disorders, 23, 130–135. 10.1016/j.janxdis.2008.04.007 [DOI] [PubMed] [Google Scholar]
- Bögels, S. M. , Alberts, M. , & de Jong, P. (1996). Self–consciousness, self‐focused attention, blushing propensity, and fear of blushing. Personality and Individual Differences, 21, 573–581. 10.1016/0191-8869(96)00100-6 [DOI] [Google Scholar]
- Bögels, S. M. , Alden, L. , Beidel, D. C. , Clark, L. A. , Pine, D. S. , Stein, M. B. , & Voncken, M. (2010). Social anxiety disorder: Questions and answers for the DSM–V. Depression and Anxiety, 27, 168–189. 10.1002/da.20670 [DOI] [PubMed] [Google Scholar]
- Bögels, S. M. , & Reith, W. (1999). Validity of two questionnaires to assess social fears: The Dutch Social Phobia and Anxiety Inventory and the Blushing, Trembling and Sweating Questionnaire. Journal of Psychopathology and Behavioral Assessment, 21, 51–66. 10.1023/A:102281222 [DOI] [Google Scholar]
- Broeren, S. , & Muris, P. (2009). The relation between cognitive development and anxiety phenomena in children. Journal of Child and Family Studies, 18, 702–709. 10.1007/s10826-009-9276-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss, A. H. (1980). Self‐consciousness and social anxiety. San Francisco, CA: WH Freeman. [Google Scholar]
- Caputi, M. , Lecce, S. , Pagnin, A. , & Banerjee, R. (2012). Longitudinal effects of theory of mind on later peer relations: the role of prosocial behavior. Developmental Psychology, 48, 257–270. 10.1037/a0025402. [DOI] [PubMed] [Google Scholar]
- Carpendale, J. I. , & Lewis, C. (2004). Constructing an understanding of mind: The development of children's social understanding within social interaction. Behavioral and Brain Sciences, 27, 79–96. 10.1017/S0140525X04000032 [DOI] [PubMed] [Google Scholar]
- Clark, D. M. , & Wells, A. (1995). A cognitive model of social phobia In Liebowitz M. & Heimberg R. G. (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). New York, NY: Guilford. [Google Scholar]
- Colonnesi, C. , Nikolić, M. , de Vente, W. , & Bögels, S. M. (2017). Social anxiety symptoms in young children: Investigating the interplay of theory of mind and expressions of shyness. Journal of Abnormal Child Psychology, 45, 997–1011. 10.1007/s10802-016-0206-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper, R. , & Gerlach, A. L. (2012). Measurement of the blush In Crozier W. R. & de Jong P. J. (Eds.), The psychological significance of the blush (pp. 222–241). Cambridge, UK: Cambridge University Press. [Google Scholar]
- Crozier, W. R. (2004). Self‐consciousness, exposure, and the blush. Journal of the Theory of Social Behavior, 34, 1–17. 10.1111/j.1468-5914.2004.00231.x [DOI] [Google Scholar]
- Crozier, W. R. (2012). Blushing and the private self In Crozier W. R. & de Jong P. J. (Eds.), The psychological significance of the blush (pp. 222–241). Cambridge, UK: Cambridge University Press; 10.1017/CBO9781139012850 [DOI] [Google Scholar]
- Cutting, A. , & Dunn, J. (2002). The cost of understanding other people: Social cognition predicts young children's sensitivity to criticism. Journal of Child Psychology and Psychiatry, 43, 849–860. 10.1111/1469-7610.t01-1-00047 [DOI] [PubMed] [Google Scholar]
- Darwin, C. 1998. The expression of the emotions in man and animals. New York, NY: Oxford University Press; 10.1037/10001-000 (Original work published 1872) [DOI] [Google Scholar]
- Denham, S. (1986). Social cognition, prosocial behavior, and emotion in preschoolers: Contextual validation. Child Development, 57, 194 10.2307/1130651 [DOI] [Google Scholar]
- Domes, G. , Heinrichs, M. , Michel, A. , Berger, C. , & Herpertz, S. C. (2007). Oxytocin improves “mind‐reading” in humans. Biological Psychiatry, 61, 731–733. 10.1016/j.biopsych.2006.07.015 [DOI] [PubMed] [Google Scholar]
- Drummond, P. D. (2012). Psychophysiology of the blush In Crozier W. R. & de Jong P. J. (Eds.), The psychological significance of blush (pp. 15–38). Cambridge, UK: Cambridge University Press; 10.1017/CBO9781139012850 [DOI] [Google Scholar]
- Fenigstein, A. (1979). Self‐consciousness, self‐attention, and social interaction. Journal of Personality and Social Psychology, 37, 75–86. 10.1037/0022-3514.37.1.75 [DOI] [Google Scholar]
- Fertuck, E. A. , Jekal, A. , Song, I. , Wyman, B. , Morris, M. C. , Wilson, S. T. , … Stanley, B. (2009). Enhanced “Reading the Mind in the Eyes” in borderline personality disorder compared to healthy controls. Psychological Medicine, 39, 1979–1988. 10.1017/S003329170900600X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert, P. , & Trower, P. (2001). Evolution and process in social anxiety In Crozier W. R. & Alden L. E. (Eds.), International handbook of social anxiety: Concepts, research and interventions relating to the self and shyness (pp. 259–279). Chichester, UK: Wiley. [Google Scholar]
- Happé, F. G. E. (1994). An advanced test of theory of mind: Understanding of story characters’ thoughts and feelings by able, mentally handicapped and normal children. Journal of Autism and Developmental Disorders, 24, 129–154. 10.1007/BF02172093. [DOI] [PubMed] [Google Scholar]
- Hezel, D. M. , & McNally, R. J. (2014). Theory of mind impairments in social anxiety disorder. Behavior Therapy, 45, 530–540. 10.1016/j.beth.2014.02.010 [DOI] [PubMed] [Google Scholar]
- Higa, K. C. , Fernandez, S. N. , Nakamura, B. J. , Chorpita, B. F. , & Daleiden, E. L. (2006). Parental assessment of childhood social phobia: Psychometric properties of the social phobia and anxiety inventory for children–parent report. Journal of Clinical Child and Adolescent Psychology, 4, 590–597. 10.1207/s15374424jccp3504_11 [DOI] [PubMed] [Google Scholar]
- Hofmann, S. G. (2007). Cognitive factors that maintain social anxiety disorder: A comprehensive model and its treatment implications. Cognitive Behaviour Therapy, 36, 193–209. 10.1080/16506070701421313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann, S. G. , Heinrichs, N. , & Moscovitch, D. A. (2004). The nature and expression of social phobia: Toward a new classification. Clinical Psychology Review, 24, 769–797. 10.1016/j.cpr.2004.07.004 [DOI] [PubMed] [Google Scholar]
- Hope, D. A. , & Heimberg, R. G. (1988). Public and private self‐consciousness and social phobia. Journal of Personality Assessment, 52, 626–639. 10.1207/s15327752jpa5204_3 [DOI] [PubMed] [Google Scholar]
- Hu, L. T. , & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Hudson, J. L. , & Rapee, R. M. (2000). The origins of social phobia. Behavior Modification, 24, 102–129. 10.1177/0145445500241006 [DOI] [PubMed] [Google Scholar]
- IBM Corporation . (2016). IBM SPSS statistics for windows, version 22.0. Armonk, NY: Author. [Google Scholar]
- Keselman, H. J. , Algina, J. , Lix, L. M. , Wilcox, R. R. , & Deering, K. N. (2008). A generally robust approach for testing hypotheses and setting confidence intervals for effect sizes. Psychological Methods, 13, 110–129. 10.1037/1082-989X.13.2.110 [DOI] [PubMed] [Google Scholar]
- Kuusikko, S. , Pollock‐Wurman, R. , Ebeling, H. , Hurtig, T. , Joskitt, L. , Mattils, M. L. , … Moilanen, I. (2009). Psychomatric evaluation of social phobia and anxiety inventory for children (SPAI‐C) and social anxiety scale for children‐revised (SASC‐R). European Child & Adolescent Psychiatry, 2, 116–124. 10.1007/s00787-010-0100-1 [DOI] [PubMed] [Google Scholar]
- Leary, M. , Britt, T. , Cutlip, W. , & Templeton, J. (1992). Social blushing. Psychological Bulletin, 112, 446–460. 10.1037/0033-2909.112.3.446 [DOI] [PubMed] [Google Scholar]
- Leary, M. , & Meadows, S. (1991). Predictors, elicitors, and concomitants of social blushing. Journal of Personality and Social Psychology, 60, 254–262. 10.1037/0022-3514.60.2.254 [DOI] [Google Scholar]
- Lewis, M. (2001). Origins of the self‐conscious child In Crozier W. R. & Alden L. E. (Eds.), International handbook of social anxiety: Concepts, research and interventions relating to the self and shyness (pp. 101–118). Sussex, UK: Wiley. [Google Scholar]
- MacCallum, R. C. , Browne, M. W. , & Sugawara, H. M. (1996). Power analyses and determination of sample size for covariance structure modeling. Psychological Methods, 1, 130–149. 10.1037/1082-989X.1.2.130 [DOI] [Google Scholar]
- Mc Donald, J. H. (2008). Handbook of biological statistics. Baltimore, MD: Sparky House. [Google Scholar]
- Moore, C. , Bosacki, S. L. , & Macgillivray, S. (2011). Theory of mind and social interest in zero‐acquaintance play situations. Child Development, 82, 1163–1172. 10.1111/j.1467-8624.2011.01602.x [DOI] [PubMed] [Google Scholar]
- Nikolić, M. , Brummelman, E. , Colonnesi, C. , de Vente, W. , & Bögels, S. M. (2018). When gushing leads to blushing: Inflated praise leads socially anxious children to blush. Behaviour Research and Therapy, 106, 1–7. 10.1016/j.brat.2018.04.003 [DOI] [PubMed] [Google Scholar]
- Nikolić, M. , Colonnesi, C. , de Vente, W. , & Bögels, S. M. (2016). Blushing in early childhood: Feeling coy or socially anxious? Emotion, 16, 475–487. 10.1037/emo0000131 [DOI] [PubMed] [Google Scholar]
- Nikolić, M. , Colonnesi, C. , Vente, W. , Drummond, P. , & Bögels, S. M. (2015). Blushing and social anxiety: A meta‐analysis. Clinical Psychology: Science and Practice, 22, 177–193. 10.1111/cpsp.12102 [DOI] [Google Scholar]
- Nikolić, M. , de Vente, W. , Colonnesi, C. , & Bögels, S. M. (2016). Autonomic arousal in children of parents with and without social anxiety disorder: A high risk study. Journal of Child Psychology and Psychiatry., 57, 1047–1055. 10.1111/jcpp.12563 [DOI] [PubMed] [Google Scholar]
- Ollendick, T. H. , Benoit, K. , & Grills‐Taquechel, A. E. (2014). Social anxiety in children and adolescents In Weeks J. W. (Ed.), The Wiley‐Blackwell handbook of social anxiety (pp. 181–200). West Sussex, UK: Wiley Blackwell. [Google Scholar]
- O'Toole, M. S. , Hougaard, E. , & Mennin, D. S. (2013). Social anxiety and emotion knowledge: A meta‐analysis. Journal of Anxiety Disorders, 27, 98–108. 10.1016/j.janxdis.2012.09.005 [DOI] [PubMed] [Google Scholar]
- Planalp, S. , DeFrancisco, V. , & Rutherford, D. (1996). Varieties of cues to emotion in naturally occurring situations. Cognition and Emotion, 10, 137 10.1080/026999396380303 [DOI] [Google Scholar]
- R Core Team . (2015). R (Version 3.2. 3) [Computer software]. Vienna, Austria: R Foundation for Statistical Computing. [Google Scholar]
- Rapee, R. M. , & Heimberg, R. G. (1997). A cognitive‐behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35, 741–756. 10.1016/S0005-7967(97)00022-3 [DOI] [PubMed] [Google Scholar]
- Rogers, J. , Viding, E. , Blair, R. J. , Frith, U. , & Happe, F. (2006). Autism spectrum disorder and psychopathy: Shared cognitive underpinnings or double hit? Psychological Medicine, 36, 1789–1798. 10.1017/S0033291706008853 [DOI] [PubMed] [Google Scholar]
- Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48, 1–36. [Google Scholar]
- Sabbagh, M. A. (2004). Understanding orbitofrontal contributions to theory‐of‐mind reasoning: Implications for autism. Brain and Cognition, 55, 209–219. 10.1016/j.bandc.2003.04.002 [DOI] [PubMed] [Google Scholar]
- Schlenker, B. R. , & Leary, M. R. (1982). Social anxiety and self‐presentation: A conceptualization model. Psychological Bulletin, 92, 641–669. 10.1037/0033-2909.92.3.641 [DOI] [PubMed] [Google Scholar]
- Shearn, D. , Bergman, E. , Hill, K. , Abel, A. , & Hinds, L. (1990). Facial coloration and temperature responses in blushing. Psychophysiology, 27, 687–693. 10.1111/j.1469-8986.1990.tb03194.x [DOI] [PubMed] [Google Scholar]
- Simonsohn, U. . (2017) Two‐lines: The first valid test of U‐shaped relationships. Retrieved from SSRN: https://ssrn.com/abstract=3021690
- Steiger, J. H. , & Lind, J. C. (1980). Statistically based tests for the number of factors. Paper presented at the annual spring meeting of the Psychometric Society, Iowa City, IA. [Google Scholar]
- Storch, E. A. , Masia‐Warner, C. , Dent, H. C. , Roberti, J. W. , & Fisher, P. H. (2004). Psychometric evaluation of the social anxiety scale for adolescents and the social phobia and anxiety inventory for children: Construct validity and normative data. Journal of Anxiety Disorders, 5, 665–679. 10.1016/j.janxdis.2003.09.002 [DOI] [PubMed] [Google Scholar]
- Sutterby, S. R. , Bedwell, J. S. , Passler, J. S. , Deptula, A. E. , & Mesa, F. (2012). Social anxiety and social cognition: The influence of sex. Psychiatry Research, 3, 242–245. 10.1016/j.psychres.2012.02.014 [DOI] [PubMed] [Google Scholar]
- Tibi‐Elhanany, Y. , & Shamay‐Tsoory, S. G. (2011). Social cognition in social anxiety: First evidence for increased empathic abilities. The Israel Journal of Psychiatry and Related Sciences, 48, 98–106. [PubMed] [Google Scholar]
- Tomasello, M. (2009). Why we cooperate. Cambridge, UK: MIT Press; 10.7551/mitpress/8470.001.0001 [DOI] [Google Scholar]
- Tonks, J. , Williams, W. , Frampton, I. , Yates, P. , & Slater, A. (2007). Assessing emotion recognition in 9–15‐years olds: Preliminary analysis of abilities in reading emotion from faces, voices and eyes. Brain Injury, 21, 623–629. 10.1080/02699050701426865 [DOI] [PubMed] [Google Scholar]
- Trentacosta, C. J. , & Izard, C. E. (2007). Kindergarten children's emotion competence as a predictor of their academic competence in first grade. Emotion, 7, 77–88. 10.1037/1528-3542.7.1.77 [DOI] [PubMed] [Google Scholar]
- Turner, R. G. , Scheier, M. F. , Carver, C. S. , & Ickes, W. (1978). Correlates of self‐consciousness. Journal of Personality Assessment, 42, 285–289. 10.1207/s15327752jpa4203_10 [DOI] [PubMed] [Google Scholar]
- Tuschen‐Caffier, B. , Kühl, S. , & Bender, C. (2011). Cognitive‐evaluative features of childhood social anxiety in a performance task. Journal of Behavior Therapy and Experimental Psychiatry, 42, 233–239. 10.1016/j.jbtep.2010.12.005 [DOI] [PubMed] [Google Scholar]
- Utens, E. M. W. J. , Ferdinand, R. F. , & Bögels, S. M. (2000). Nederlandse vertaling van de SPAI‐C (SPAI‐C NL). Rotterdam, The Netherlands: AZR‐Sophia/Erasmus Universiteit. [Google Scholar]
- van den Bos, E. , van Duijvenvoorde, A. C. , & Westenberg, P. M. (2016). Effects of adolescent sociocognitive development on the cortisol response to social evaluation. Developmental Psychology, 52, 1151–1163. 10.1037/dev0000133 [DOI] [PubMed] [Google Scholar]
- Voncken, M. J. , & Bögels, S. M. (2009). Physiological blushing in social anxiety disorder patients with and without blushing complaints: Two subtypes? Biological Psychology, 81, 86–94. 10.1016/j.biopsycho.2009.02.004 [DOI] [PubMed] [Google Scholar]
- Washburn, D. , Wilson, G. , Roes, M. , Rnic, K. , & Harkness, K. L. (2016). Theory of mind in social anxiety disorder, depression, and comorbid conditions. Journal of Anxiety Disorders, 37, 71–77. 10.1016/j.janxdis.2015.11.004 [DOI] [PubMed] [Google Scholar]
- Wellman, H. (1990). The child's theory of mind. Cambridge, UK: MIT Press. [Google Scholar]
- Wellman, H. M. , & Liu, D. (2004). Scaling of theory‐of‐mind tasks. Child Development, 75, 523–541. 10.1111/j.1467-8624.2004.00691.x. [DOI] [PubMed] [Google Scholar]
- Westenberg, M. P. , Drewes, M. J. , Goedhart, A. W. , Siebelink, B. M. , & Treffers, P. D. (2004). A developmental analysis of self‐reported fears in late childhood through mid‐adolescence: Social‐evaluative fears on the rise? Journal of Child Psychology and Psychiatry, 45, 481–495. 10.1111/j.1469-7610.2004.00239.x [DOI] [PubMed] [Google Scholar]
- White, L. O. , Klein, A. M. , von Klitzing, K. , Graneist, A. , Otto, Y. , Hill, J. , … Crowley, M. J. (2016). Putting ostracism into perspective: Young children tell more mentalistic stories after exclusion, but not when anxious. Frontiers in Psychology, 7, 1926 10.3389/fpsyg.2016.01926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, J. M. G. , Watts, F. N. , MacLeod, C. , & Mathews, A. (1988). Cognitive psychology and emotional disorders. Oxford, UK: Wiley. [Google Scholar]
- Zerwas, S. , Balaraman, G. , & Brownell, C. (2004). Constructing an understanding of mind with peers. Behavioral and Brain Sciences, 27, 130 10.1017/S0140525X04590039 [DOI] [Google Scholar]