

Abstract
BACKGROUND:
Eighty percent of women during their reproductive age experience some symptoms attributed to premenstrual phase of the menstrual cycle. Premenstrual syndrome (PMS) is characterized by emotional, behavioral, and physical symptoms that occur during late luteal phase of menstrual cycle and are relieved after the onset of menstruation. Aerobic exercise and yoga are one of the ways to reduce these symptoms. The aim of this study was to compare the effects of aerobic exercise and yoga on PMS.
MATERIALS AND METHODS:
A total of 72 participants of PMS, referred for physiotherapy treatment (mean age 28 years), were enrolled and allocated into two groups (Group A and B) by simple computerized randomization. Patients in Group A received aerobic exercise and in Group B received yoga movements for 40 min, 3 times a week for 1 month. The pain intensity (Visual Analog Scale) and PMS Scale were measured before, at the end of 15 days, and 1 month of treatment program.
RESULTS:
Data were analyzed by paired t-test, unpaired t-test, and one-way ANOVA; and the results showed that both aerobic exercise and yoga movements significantly reduced pain intensity and PMS symptoms. Significant reduction in PMS symptoms was found in patients treated with yoga compared to aerobic exercise; however, no significant difference was found in pain intensity between these two groups (P > 0.05).
CONCLUSION:
It is concluded that both aerobic exercise and yoga movements are effective in treating PMS; however, yoga is more effective in relieving the symptoms of PMS than aerobic exercise.
Keywords: Exercise, menstruation, premenstrual syndrome, Visual Analog Scale, yoga
Introduction
Adolescence has turned out to be unique which greatly affects the psychological and physiological system in the human body. Monthly menstrual cycle is considered to be the major factor responsible for such changes in females’ life which usually begins between the ages of 8 and 14 years,[1] about 2 years after the onset of puberty. The average age of menstruation is considered to be between 12 and 13 years. Females go through many psychological and physiological changes during their reproductive life, especially during menstrual cycles, which are commonly termed as premenstrual symptoms, and this disorder is known as premenstrual syndrome (PMS). These changes may initiate from 6 to 12 days prior to the menstruation cycle and last for 2–4 days after the onset of menstruation. The term PMS is used to describe a group of physiological, cognitive, affective, and behavioral symptoms that occur during the luteal phase of the menstrual cycle and resolve quickly at or within few days of the onset of menstrual cycle.[2]
The University of California at San Diego has developed the diagnostic criteria for PMS which mainly includes the presence of any one symptom during the 5 days before menses in each of the three previous cycles and these identified symptoms are affective symptoms (depression, angry outbursts, irritability, anxiety, confusion, and social withdrawal) and somatic symptoms (breast tenderness, abdominal bloating, headache, and swelling of extremities).[3]
Although majority of females, approximately 90% experience these symptoms during their childbearing age and around 5% of women experience severe symptoms which interfere with their daily activities; the true prevalence of PMS is difficult to be established due to disparity in availability and access to medical care, diagnostic criteria, self-treatment, and cultural practices. Research in the community has shown the prevalence of PMS to be from 5.9% upto 90%.[2] The pathophysiology of PMS is still indefinite, complex, multifactorial, and yet to be fully elucidated. It is anticipated to have influential effects of progesterone on neurotransmitters such as serotonin, opioids, catecholamine, and gamma-aminobutyric acid (GABA). Increased sensitivity to progesterone in women with underlying serotonin deficiency is also considered to be a responsible factor for this disorder.[3] Increased prolactin level or increased sensitivity to the effect of prolactin, insulin resistance and alteration of glucose metabolism, sensitivity to endogenous hormones, abnormal hypothalamic–pituitary–adrenal axis function, nutritional deficiencies, fluid and electrolyte imbalance, and genetic factors also seem to play a role for PMS.[2,3]
Till now, the main treatment goal for PMS has remained to ameliorate the symptoms and reducing their effects on daily activities. Although pharmacotherapy has dominated the treatments of PMS, recent clinical research has suggested the combination of pharmacotherapies (such as selective serotonin reuptake inhibitors, anxiolytic agents, gonadotropin-releasing hormone agonists, the diuretic spironolactone, nonsteroidal anti-inflammatory drugs, and combination oral contraceptives [OCs]) and nonpharmacotherapy treatments, namely, cognitive and behavioral therapies, aerobic exercises, reflexology, light therapy, massage therapy, dietary and nutritional modifications, etc., to treat premenstrual symptoms.[2]
Exercises increase the release of several neurotransmitters including natural endorphins (the natural painkillers), estrogen, dopamine and endogenous opiate peptides, as well as alter the production of hormone secretion, suppressing prostaglandin from being released and raising the estrone–estradiol ratio which acts to decrease endometrial proliferation and shunts blood flow away from the uterus.[4] Exercise may act as a distraction from intrusive thoughts and promote positive thoughts; reduce depression and improve mood and behavior.[5] Evidence suggests that aerobic exercise reduces negative effect on women who exercise regularly. It is also been said that frequent physical activity may, at least in part, reduce PMS and premenstrual symptoms.
Yoga is a Sanskrit word, meaning connection of the mind, body, emotions, logic, and attention to the action. Yoga exercise is composed of physical (asana), breathing (pranayama), and mental (pratyahara) practices, resulting in health, relaxation, and positive awareness.[6] Yoga is now recommended as a noninvasive method and easily accessed intervention for pain relief that is safe and cost-effective with minimal or no side effects. Moreover, regular practice of yoga has positive effects onthe menstrual cycle and psychobiological well-being probably by balancing the neuroendocrinal axis. Yoga reduces the stress induced negative effects to immune system by regulating positively the adjustment of immunoglobulin A and reduces harmful inflammatory secretions, which makes women with PMS comfortable.[7]
The present study aimed to compare the effectiveness of these two nonphramacotherapies, i.e., aerobic exercise and yoga in reducing the symptoms of PMS.
Materials and Methods
The approval was obtained from the Institutional Ethics Committee, H M Patel Center for Medical Care and Education, Karamsad, before initiating the trial (Ethical Code: IEC/HMPCMCE/76/faculty/11/107/17).
Study design
This was a parallel-group randomized trial.
Sampling method
The sampling method used was convenience sampling.
Study setting
The study was carried out at K M Patel Institute of Physiotherapy, Shree Krishna Hospital, Karamsad.
It was a single-centered, interventional, parallel group randomized trial. Seventy-two females with PMS, diagnosed by gynecologist, and referred for physiotherapy treatment were recruited for the study by convenience sampling based on inclusion and exclusion criteria. The written informed consent was obtained from all the recruited participants after explaining the purpose of study.
Inclusion criteria
Age between 16 and 45 years
No history of any mental and physical diseases
No history of joint, motion, muscle, and bone diseases that reduce their abilities of exercise
Not on any medication and mineral supplements during three menstrual cycles
Having regular menstrual cycles – 24–35 days
No incidents such as relatives’ death, marriage, or any medical emergency in the last 3 months
Females using nonhormonal contraception methods.
Exclusion criteria
Not able to tolerate physical exercise
Gynecological surgery
Professional athletes
Chronic disease: diabetes, hypertension, cardiac disease, infectious disease
Irregular and infrequent menstrual cycle
Using intrauterine devices, women on OCs, and hormonal therapy
Pregnancy.
Randomization was done using computer-generated random numbers. Participants were allocated by using sequentially numbered opaque-sealed envelopes into two groups: Group A and Group B. Females with PMS in Group A received aerobic exercises and in Group B received yoga movements [Figure 1].
Figure 1.
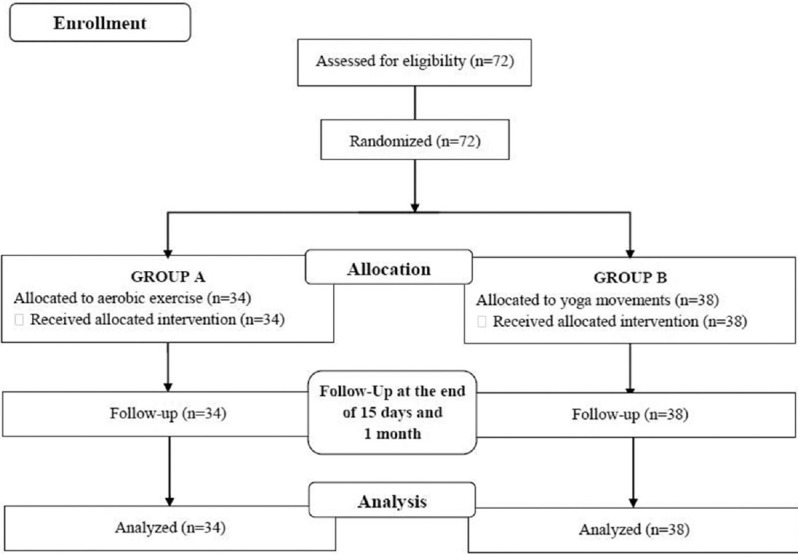
Enrollment of patients
Detailed history was obtained and examination for PMS was carried out for all the participants in both groups. They were assessed for their pain intensity using Visual Analog Scale (VAS) and symptoms of PMS were assessed by PMS Scale (PMSS).
Patients in both groups received treatment for 40 min, 3 times a week for 1 month that is for one menstrual cycle. Patients in Group A received aerobic exercise in the form of warm up and cool down (both for 5 min) and treadmill (30 min) based on Target Heart Rate (calculated using Karvonen formula at 60%–70% of heart rate reserve). Patients in Group B were given yoga movements, including 10 min of Kapalbharti Pranayam which includes automatic inhalation with short and forceful exhalations, 20 min of yoga movements (Cat-cow pose, Child's pose, Plank pose, Cobra pose – each for 5 min), and 10 min of meditation/relaxation in Savasana pose. All the participants were reassessed for pain intensity and premenstrual symptoms at the end of 15 days and 1 month of the treatment program.
Results
All 72 participants completed 1 month of intervention in both groups. The results of the study were recorded in terms of VAS and PMSS. Intra- and intergroup differences were compared so as to evaluate the effectiveness of two treatment approaches in PMS. Statistical analysis was done using SPSS 14 version software. Descriptive statistics such as frequency (%) and mean and standard deviation were calculated.
Both the groups were compared for age, body mass index, age of menarche, average duration of menstrual cycle, and interval between two menstrual cycles with independent t-test [Table 1] and no statically significant difference was found between two groups except for average duration of menstrual cycle which was found to be higher in group of patients allocated to yoga movements. Patients in both groups were also compared for baseline pain intensity and PMSS [Table 1]. No statistically significant difference was found with regard to pain intensity in both groups; however, patients in Group B (yoga) had higher score on PMSS compared to Group A (aerobic exercise) (P < 0.05).
Table 1.
Baseline comparison between two groups (independent t-test)
| Age | Groups | Mean±SD | P |
|---|---|---|---|
| Age (year) | Aerobic (n=34) | 28.35±8.574 | 0.938 |
| Yoga (n=38) | 28.21±6.913 | ||
| BMI (kg/m2) | Aerobic (n=34) | 26.34±5.073 | 0.436 |
| Yoga (n=38) | 25.36±5.509 | ||
| Age of menarche (years) | Aerobic (n=34) | 13.47±1.461 | 0.124 |
| Yoga (n=38) | 13.97±1.284 | ||
| Duration (days) | Aerobic (n=34) | 4.50±1.135 | 0.003* |
| Yoga (n=38) | 5.37±1.217 | ||
| Interval between two cycles (days) | Aerobic (n=34) | 30.26±2.968 | 0.185 |
| Yoga (n=38) | 29.39±2.542 | ||
| VAS | Aerobic (n=34) | 6.59±1.459 | 0.909 |
| Yoga (n=38) | 6.63±1.715 | ||
| PMSS | Aerobic (n=34) | 89.32±24.828 | 0.041* |
| Yoga (n=38) | 102.74±29.394 |
*P<0.05. SD=Standard deviation, BMI=Body mass index, VAS=Visual Analog Scale, PMSS=Premenstrual Syndrome Scale
Comparison in pain intensity (VAS) and PMSS within the groups at baseline, 15 days posttreatment, and at the end of 1 month of treatment program was carried out using one-way ANOVA for both groups [Table 2]. The results showed significant reduction both in pain intensity (VAS) and PMSS in both groups at the end ofthe treatment program (P < 0.05) proving that both aerobic exercises and yoga movements help in reducing the symptoms of PMS effectively.
Table 2.
Comparison of Visual Analog Scale and Premenstrual Syndrome Scale within the group one-way ANOVA
| Outcome measures | Groups | Mean±SD | P | ||
|---|---|---|---|---|---|
| Baseline value | At the end of 15 days | At the end of 1 month | |||
| VAS | Aerobic (n=34) | 6.588±1.458 | 5.941±1.824 | 3.676±1.854 | <0.00001* |
| Yoga (n=38) | 6.63±1.71 | 5.92±1.99 | 3.73±1.55 | <0.00001* | |
| PMSS | Aerobic (n=34) | 89.32±24.82 | 71±18.63 | 56.20±11.21 | <0.00001* |
| Yoga (n=38) | 102.73±29.39 | 76.78±19.11 | 57.26±9.46 | <0.00001* | |
*P<0.05. SD=Standard deviation, VAS=Visual Analog Scale, PMSS=Premenstrual Syndrome Scale
Difference/reduction in VAS and PMSS before and after 1 month of treatment was compared between two groups using independent t-test, which showed significant reduction in PMSS in Group B (yoga) compared to Group A (aerobic exercise); however, no significant difference was found with regard to reduction in pain intensity (VAS) between two groups at the end of treatment program (P < 0.05) [Table 3].
Table 3.
Comparison of difference/reduction in Visual Analog Scale and Premenstrual Syndrome Scale between two groups – independent t-test
| Comparison of difference | Aerobic (n=34) | Yoga (n=38) | P |
|---|---|---|---|
| Reduction in VAS, mean±SD | 2.97±1.83 | 2.89±2.06 | 0.87 |
| Reeducation in PMSS, Mean±SD |
33.11±17.9 | 44.44±23.54 | 0.02* |
*P<0.05. SD=Standard deviation, VAS=Visual Analogue Scale, PMSS=Premenstrual Syndrome Scale
Discussion
Efficacy of both aerobic exercise and yoga has been demonstrated in the literature among the females with menstrual disorders; however, no study has compared the effectiveness of these two treatment modalities. The present study aimed to compare the effectiveness of aerobic exercise and yoga on PMS. A total of 72 patients with PMS participated in the present study, and the results revealed significant reduction in pain intensity and PMS symptoms measured by VAS and PMSS, respectively, in both groups.
Vishnupriya and Rajarajeswaram, 2011 studied the effectiveness of aerobic exercise at different intensities in the management of PMS and concluded that moderate-intensity aerobic exercise should be encouraged as a potential measure for PMS.[8] It was further discussed that aerobic exercise intensely raises serum progesterone levels which may give positive benefits to alter mood and decrease stress via neurotransmitter systems (e.g., GABA, serotonin) modulated by sex steroids. The significant release of endorphin during exercises has been found to be associated with reduction in pain, anxiety, and depression in PMS, opposing the possible reduction in endorphin during the luteal phase.
Effectiveness of physical activity program on primary dysmenorrhea has been deliberated in literature with one of the possible mechanisms explained was the positive effect of physical activity on reduction in stress level which has been found to be associated with menstrual pain and other menstrual disorders. Increased stress level significantly raises the sympathetic activity leading to menstrual pain by significantly increasing the intensity of uterine contraction. Exercise helps to reduce and alter the stress level, thereby reduces the sympathetic activity leading to reduction in menstrual pain and other symptoms related to menstrual disorders.[9,10] Another possible mechanism explained by Sabaei et al. was based on the regulation of leptin during the menstrual cycle. Leptin is responsible for controlling the emotional behavior, and it significantly increases in women with PMS compared to women without PMS. High level of circulating leptin is associated with psychological symptoms of PMS. Many studies have demonstrated the effectiveness of exercise in reducing the blood leptin levels by 30%–34% and thus helping in reduction of behavioral symptoms of PMS.[11]
Effects of aerobic and stretching exercise were compared by Vaziri et al. which revealed that both aerobic and stretching exercise help alleviating the symptoms of menstrual disorders especially menstrual pain and no one treatment was superior to other.[10]
Yoga movements carried out in the present study included breathing exercises, meditation/relaxation, and four different yogic postures (cat-cow, child's pose, plank, and cobra). Cat-cow pose stretches the abdominal muscles, neck, and back and maintains the flexibility of the spine, and this pose is especially helpful for people with stiff backs. Child's pose stretches the lower back and hips and helps to relieve stress, decreases back discomfort, fatigue, gas, and bloating. Plank pose strengthens the arms, wrists, and spine, and the cobra pose stretches the chest and abdominal muscles and maintains the flexibility of the spine. It also improves poor posture and combats depression, lower back discomfort, and low energy.
Efficacy of yoga on menstrual pain and stress has been studied by Nag and Kodali among medical students and concluded that yogic exercises help controlling the menstrual pain and reduces the stress level. The possible mechanism explained was based on the level of serum interleukin 6 (IL-6). It has been found that yoga performers produce less IL-6 in response to stressor compared to nonyoga performers. Some yoga postures are also considered to be immune enhancing and restorative.[12] These results are comparable with the study carried out by Rakhshaee, who used cobra, cat, and fish poses and found significant reduction in menstrual pain intensity among adolescent females.[13] A comprehensive review of the literature has proven the role of yoga and pranayama on a variety of health outcomes and conditions, namely, hypertension, coronary atherosclerosis, serum lipid profile and body weight, cardiorespiratory efficiency and physical fitness, diabetes mellitus, neurohormonal activity, reproductive functions and pregnancy, stress and anxiety, mood and functioning, cancer, etc.[14]
Many mirroring reviews of yoga practices recommend that yoga can significantly reduce the effects of elevated stress responses and reduces both anxiety and depression through downregulating the hypothalamic–pituitary–adrenal axis which is activated in response to a physical or psychological stressor and is responsible for a chain of behavioral, physiological, and psychological responses in a human body. These changes are said to be due to the release of cortisol, epinephrine, and norepinephrine which can be regulated with a regular practice of yoga, ultimately leading to a healthy mind, body, and soul.[14] As stress and anxiety are proportionately related to the symptoms of PMS and menstrual pain, reduction in stress and anxiety with yoga can significantly reduce menstrual pain and symptoms of PMS.
Harinath et al. examined the effects of yoga for 3 months on melatonin secretion in healthy individuals and found significant increase in plasma melatonin level which may be responsible for overall sense of well-being.[15] Twelve weeks of yoga program has been found to be significantly effective in improving physical functions and reducing body aches, breast tenderness, abdominal cramps, and cold sweats in females with PMS.[7] Yoga has been found to have positive effects on activity of the central nervous system. Alpha-brain waves production due to regular yoga practice are directly related with state of peace, creativity, mood elevation, relaxation, and release of serotonin, thus leading yoga practitioners feel more relaxed.[16]
In the present study, patients enrolled in yoga movements had more reduction in PMSS compared to patients enrolled in aerobic exercise. Physical exercises and yoga movements have many similarities but also have obvious differences, emphasizing breathing regulation, peacefulness, and maintenance of body postures, which differentiate yoga from routine physical exercises. A review and comparison between yoga and physical exercise were conducted by Govindaraj et al., which concluded that yoga interventions are equal and/or superior to physical exercises in most outcomes.[6]
Conclusion
The results of this study showed that 1 month of regular aerobic exercise and yoga movements, both reduced pain intensity and symptoms of PMS in females with PMS. However, yoga movements were more beneficial in relieving the symptoms of PMS compared to aerobic exercise.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We acknowledge Dr. R. Harihara Prakash (PT), Professor & Head, K M Patel Institute of Physiotherapy, for permitting us to carry out this research work. We would like to thank our participants of the study for their consent and cooperation throughout the research work. We also thank the consultant of Obstetrics and Gynecology Department of Shree Krishna Hospital, Karamsad, for referring the patient for physiotherapy.
References
- 1.National Research Council (US) and Institute of Medicine (US) Forum on Adolescence. Adolescent Development and the Biology of Puberty. Adolescent Development and the Biology of Puberty: Summary of a Workshop on New Research. In: Kipke MD, editor. Washington (DC): National Academies Press (US); 1999. [Last accessed on 2018 Dec 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK224692/ [PubMed] [Google Scholar]
- 2.Tolossa FW, Bekele ML. Prevalence, impacts and medical managements of premenstrual syndrome among female students: Cross-sectional study in college of health sciences, Mekelle university, Mekelle, Northern Ethiopia. BMC Womens Health. 2014;14:52. doi: 10.1186/1472-6874-14-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dickerson LM, Mazyck PJ, Hunter MH. Premenstrual syndrome. Am Fam Physician. 2003;67:1743–52. [PubMed] [Google Scholar]
- 4.Sutar A, Paldhikar S, Shikalgar N, Ghodey S. Effect of aerobic exercises on primary dysmenorrhoea in college students. IOSR J Nurs Health Sci. 2016;5:20–4. [Google Scholar]
- 5.Craft LL, Perna FM. The benefits of exercise for the clinically depressed. Prim Care Companion J Clin Psychiatry. 2004;6:104–11. doi: 10.4088/pcc.v06n0301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Govindaraj R, Karmani S, Varambally S, Gangadhar BN. Yoga and physical exercise – A review and comparison. Int Rev Psychiatry. 2016;28:242–53. doi: 10.3109/09540261.2016.1160878. [DOI] [PubMed] [Google Scholar]
- 7.Kamalifard M, Yavari A, Jafarabadi MA, Ghaffarilaleh G, Kasb-Khah A. The effect of yoga on women's premenstrual syndrome: A randomized controlled clinical trial. Int J Womens Health Reprod Sci. 2017;5:2015–11. [Google Scholar]
- 8.Vishnupriya R, Rajarajeswaram P. Effects of aerobic exercise at different intensities in pre menstrual syndrome. J Obstet Gynaecol India. 2011;61:675–82. doi: 10.1007/s13224-011-0117-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mahvash N, Eidy A, Mehdi K, Toorzani Zahra M, Mani M, Shahla H. The effect of physical activity on primary dysmenorrhea of female university students. World Appl Sci J. 2012;17:1246–52. [Google Scholar]
- 10.Vaziri F, Hoseini A, Kamali F, Abdali K, Hadianfard M, Sayadi M. Comparing the effects of aerobic and stretching exercises on the intensity of primary dysmenorrhea in the students of universities of Bushehr. J Family Reprod Health. 2015;9:23–8. [PMC free article] [PubMed] [Google Scholar]
- 11.Sabaei Y, Sabaei S, Khorshidi D, Ebrahimpour S, Fallah-Rostami F. The association between premenstrual syndrome and physical activity and aerobic power in female high school students. Crescent J Med Biol Sci. 2015;2:53–8. [Google Scholar]
- 12.Nag U, Kodali M. Effect of yoga on primary dysmenorrhea and stress in medical students. IOSR J Dent Med Sci. 2013;4:69–73. [Google Scholar]
- 13.Rakhshaee Z. Effect of three yoga poses (cobra, cat and fish poses) in women with primary dysmenorrhea: A randomized clinical trial. J Pediatr Adolesc Gynecol. 2011;24:192–6. doi: 10.1016/j.jpag.2011.01.059. [DOI] [PubMed] [Google Scholar]
- 14.Sengupta P. Health impacts of yoga and pranayama: A state-of-the-art review. Int J Prev Med. 2012;3:444–58. [PMC free article] [PubMed] [Google Scholar]
- 15.Harinath K, Malhotra AS, Pal K, Prasad R, Kumar R, Kain TC, et al. Effects of hatha yoga and omkar meditation on cardiorespiratory performance, psychologic profile, and melatonin secretion. J Altern Complement Med. 2004;10:261–8. doi: 10.1089/107555304323062257. [DOI] [PubMed] [Google Scholar]
- 16.Wu WL, Lin TY, Chu IH, Liang JM. The acute effects of yoga on cognitive measures for women with premenstrual syndrome. J Altern Complement Med. 2015;21:364–9. doi: 10.1089/acm.2015.0070. [DOI] [PubMed] [Google Scholar]