

Abstract
People with psychotic illnesses, such as schizophrenia, have high rates of unhealthy lifestyle factors, such as smoking and physical inactivity. Young people who seek help for mental health care, particularly those at high risk for psychosis, often also display high rates of these unhealthy behaviours. Although healthy living interventions have been applied to people with established psychosis, no attempt has been made to offer them to young people at risk for developing psychosis, despite potential benefits to mental and physical health. We propose that the COM‐B model (consisting of capability, opportunity and motivation) and behaviour‐change wheel might be an appropriate framework that mental health nurses and other health professionals could apply. Using a systematic and theoretically‐based approach to intervention development could result in effective methods of health promotion in this group. Further training and development for mental health nurses could encourage a greater integration of mental and physical health care.
Keywords: lifestyle, mental health nursing, physical health, ultra‐high risk
Introduction
The physical health disparities of people with schizophrenia and severe mental illness are an area of increasing concern (Shiers et al. 2015). Together with the unwanted side‐effects of antipsychotic medication, this increased morbidity is partly due to adverse lifestyle factors, including tobacco use, poor diet, and physical inactivity (Addy et al. 2012; Hennekens et al. 2005; Vancampfort et al. 2013). However, these lifestyle factors are also present from an early stage (first‐episode of psychosis (FEP)), and might even occur prior to the onset of psychosis, in those who are at ultra‐high risk (UHR) for psychosis or putatively ‘prodromal’ (Addington et al. 2015; Carney et al. 2016).
UHR individuals (otherwise referred to as the ‘at‐risk mental state’ (ARMS) group are characterized by the presence of attenuated psychotic symptoms, brief limited intermittent psychotic symptoms that spontaneously resolve, or genetic‐risk combined with recent decline in functioning (Yung et al. 2004). Within 3 years, we can expect approximately one‐third of UHR individuals to progress to a full‐threshold psychotic illness, with a large proportion developing schizophrenia (Nelson et al. 2013). Other psychological illnesses are also prevalent in this group, such as anxiety, mood, or substance use disorders (Addington et al. 2011; Lin et al. 2015), and many continue to function poorly, regardless of symptomatic remission (Cotter et al. 2014).
Existing interventions for UHR cohorts focus primarily on addressing poor mental health and providing supportive psychological therapies to prevent the onset of psychotic illnesses (van der Gaag et al. 2013; Yung et al. 2011). Physical health and lifestyle behaviours are generally not addressed or monitored routinely in services (Carney et al. 2015), and to date, healthy lifestyle interventions have not been applied to this group. This is despite potential benefits to future physical and mental health. First, if a UHR individual develops a FEP, he or she will almost certainly receive antipsychotic medication. The side‐effects of antipsychotics might then further exacerbate already compromised physical health due to the unhealthy lifestyle factors noted earlier (De Hert et al. 2006). Second, even if a psychotic illness does not develop, encouraging a healthy lifestyle might protect against future ill health and health implications arising from these unhealthy behaviours, such as continued tobacco use. Finally, there is evidence to suggest that high rates of unhealthy lifestyle factors could contribute to the onset of psychosis. This includes the use of high‐potency cannabis (Di Forti et al. 2014), tobacco (Gurillo et al. 2015), and physical inactivity (Koivukangas et al. 2010). Therefore, the UHR group represents an important target for health professionals when applying healthy lifestyle interventions. Mental health nurses might be an appropriate target to deliver such interventions, as they are frequently in contact with service users and are seen as having a holistic role in managing mental and physical health (Bradshaw and Pedley, 2012).
Unique Characteristics of the UHR Group
In addition to subthreshold psychotic symptoms, UHR individuals frequently report depression and anxiety (Fusar‐Poli et al. 2013; Yung et al. 2004). Although they are usually no different to their peers with regards to weight and body composition, they do have high levels of unhealthy lifestyle behaviours (Addington et al. 2015; Carney et al. 2016). Designing an intervention must take these characteristics into account. However, issues which usually have to be considered when developing lifestyle interventions for people with schizophrenia might not be relevant, such as long‐standing illness, high levels of negative symptoms, cognitive impairment, and antipsychotic side‐effects, such as weight gain and metabolic disturbance. We aimed to assess which behaviour‐change theories and techniques might be useful to underpin a healthy living intervention for the UHR group, given their unique characteristics. We also aimed to discuss how this can be related to clinical practice, and how mental health nurses might have an important role in promoting physical health.
Existing Interventions
Happell et al. (2012) discuss how physical health interventions are required to promote the well‐being of people with mental health difficulties. A focus on developing health‐behaviour interventions within the nursing and wider health‐care professions might encourage significant benefits in the general health of young people who use mental health services. One approach recommended by the Medical Research Council (Craig et al. 2008) is to use a theoretical background to develop methods of health promotion. A sound theoretical framework will assist the delivery of an intervention through the application of a well‐developed structure, based on the best available evidence (Hillsdon et al. 2004). The alternative is to simply apply interventions in the hope that they might work. However, behaviour change is a complex area, with many overlapping concepts and theories. The most common social cognition models applied to behaviour‐change research are social learning theory (Bandura, 1986), the Health Belief Model (Rosenstock, 1974), theory of planned behaviour (Ajzen, 1991), and the Transtheoretical Model (Prochaska and Velicer, 1997).
These models are useful to predict and explain human behaviour; however, their application to behaviour‐change interventions is less clear. National Institute for Health and Care Excellence (NICE) guidelines (2007) state that evidence supporting any specific psychological model to inform behaviour change is limited (Abraham et al. 2009). A recent meta‐analysis concluded that the relationship between the use of theory and effectiveness of an intervention is weak (Prestwich et al. 2014). Additionally, despite MRC (Craig et al. 2008) recommendations, many health‐behaviour interventions lack a clear and specific theoretical foundation (Davies et al. 2010; Hardeman et al. 2002; Prestwich et al. 2014). Even those that include a theoretical model often fail to link the mechanisms of change back to theoretical constructs (Michie and Prestwich, 2010; Prestwich et al. 2014). This could be due to the inconsistency in existing frameworks when describing how to apply theory to an intervention.
Promoting Behaviour Change
Creating an intervention involves the initial difficulty of identifying which behaviour should be targeted to achieve a desired health outcome. For example, in a healthy living intervention for young people, the aim might be to promote weight loss, for which many types of behaviours could be targeted, including dietary intake, physical activity, and sedentary behaviour. Once a behaviour is identified, techniques to promote this change can be applied.
Behaviour‐change techniques (BCT) are the active components which make up an intervention, and are observable and replicable (Michie and Johnston, 2012). The behaviour‐change technique taxonomy consists of 93 'active ingredients' that can be used to facilitate behaviour change (Abraham and Michie, 2008; Michie and Johnston, 2012); for example, the use of goal setting and the provision of instructions in a physical activity intervention. Individual taxonomies have also been refined containing a smaller set of techniques, which could be most effective for smoking cessation (Michie et al. 2011b), or interventions for physical activity and diet (Michie et al. 2011a), and alcohol consumption (Michie et al. 2012).
NICE suggests a number of BCT that might be effective for driving behaviour change, including self‐monitoring techniques (NICE, 2007; NICE, 2014). Self‐monitoring involves recording behaviours (i.e. keeping a food diary), setting goals, and obtaining feedback (Abraham and Michie, 2008). NICE (2014) also suggest applying these techniques using remote methods via text messaging or mobile apps (NICE, 2014). Self‐monitoring techniques are recommended for the general population (Michie et al. 2009), obese adults and those with obesity related comorbidities (Dombrowski et al. 2012), and people with recently‐diagnosed diabetes (Hankonen et al. 2014).
Interventions For Clinical Populations
NICE guidelines (2014) emphasize that techniques used in lifestyle interventions should match service users' needs. Therefore, the characteristics of the UHR cohort need to be considered to ensure any new lifestyle interventions are appropriate. As noted earlier, health promotion for UHR individuals is currently limited. While interventions designed for the general population might not be appropriate, neither might those developed for people with schizophrenia. Given that UHR individuals frequently experience high levels of depression (Fusar‐Poli et al. 2014; Yung et al. 2004), we examined the techniques commonly used in populations with clinical depression to promote physical activity.
A recent Cochrane review examined the effectiveness of exercise interventions for depression (Cooney et al. 2014). Individuals with clinical depression from inpatient or community outpatient settings usually receive supervised, guided exercise sessions conducted by a professionally‐qualified physical activity trainer (Carta et al. 2008; Knubben et al. 2007; Martinsen et al. 1985; Mota‐Pereira et al. 2011; Pilu et al. 2007; Schuch et al. 2011). Individuals are also given information about correct exercise technique (Knubben et al. 2007), and receive positive feedback from trainers throughout sessions (Carta et al. 2008; Pilu et al. 2007). However, it is unclear whether other BCT are employed, as many studies lack sufficient detail for further analysis.
As UHR individuals present with subthreshold, emerging psychotic symptoms, we also considered physical activity interventions for people with early psychosis. Although there are many such interventions for people with schizophrenia (Firth et al. 2015), to date, only one review has assessed the active components of physical activity interventions for first‐episode samples (Rosenbaum et al. 2014). Similar to interventions for people with depression, the most common techniques employed are the provision of information and guidance about exercise (Alvarez‐Jimenez et al. 2006; Abdel‐Baki et al. 2013; Curtis et al. 2015a; Fredrikson et al. 2014; Killackey et al. 2011; Lin et al. 2011; Lovell et al. 2014; Smith et al. 2014), supervised sessions (Curtis et al. 2015a; Lin et al. 2011; Smith et al. 2014), and the use of goal setting (Fredrikson et al. 2014; Killackey et al. 2011). A further qualitative study found FEP individuals value the peer support of a training partner and an individualized approach to designing an exercise intervention (Firth et al. 2016).
Common techniques used for FEP populations and individuals with depression are the provision of a professionally‐qualified trainer who is available to supervise, demonstrate, and give instructions during exercise sessions. Therefore, increasing the opportunity to exercise by providing facilities, or allocating time for physical activity and enhancing a person's knowledge so they feel capable to exercise, might be particularly useful. Nonetheless, we should look further than the methods used for these patient groups, as they might not be the only effective techniques to employ for UHR individuals. Additionally, many existing interventions are vague and do not provide sufficient detail for replication.
COM‐B Model of Behaviour and Behaviour‐Change Wheel
Despite MRC (Craig et al. 2008) recommendations of using theory to guide intervention development, little advice is given on how mental health nurses and allied health professionals can apply theory to behaviour‐change interventions in practice, and how health professionals can select the most appropriate techniques to use. The behaviour‐change wheel is a new framework that aims to promote a systematic method of intervention development, (Michie et al. 2011c; Michie et al. 2015).
The behaviour‐change wheel has been described elsewhere (Michie et al. 2011c; Michie et al. 2015). To summarize, the behaviour‐change wheel is made up of three layers (Fig. 1). At the centre of the framework sits a theoretical model that proposes three ways in which a behaviour occurs: capability, opportunity, and motivation (the COM‐B model; Michie et al. 2011c; Michie et al. 2015). This helps identify which source of behaviour should be targeted. Surrounding the COM‐B model are intervention categories that provide methods to promote behaviour change and include education, persuasion, incentivization, coercion, training, restriction, environmental restructuring, modelling, and enablement (see Table 1 for examples and definitions from Michie et al. (2011c)). The final layer of the behaviour‐change wheel contains policy categories showing how intervention functions cab be applied on a wider scale (Michie et al. 2015).
Figure 1.
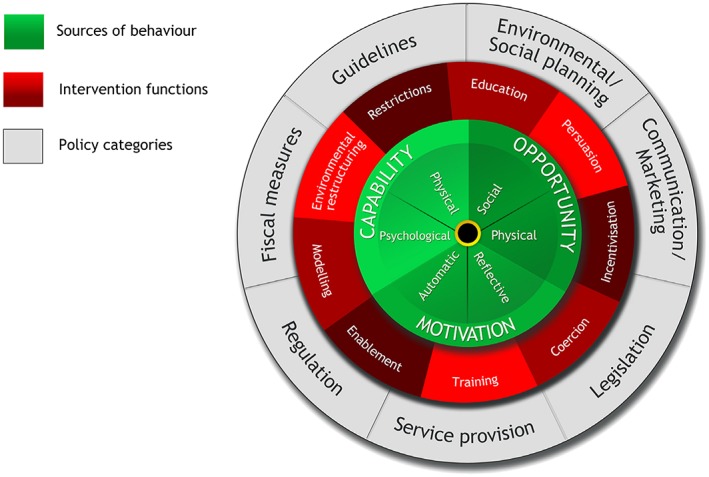
Behaviour change wheel Michie et al. (2011c). [Colour figure can be viewed at http://wileyonlinelibrary.com]
Table 1.
Possible intervention functions to encourage a healthy lifestyle in UHR cohorts
| Intervention class | Definition (from Michie et al. 2011, p7) | Example applied to a healthy living intervention for the UHR cohort |
|---|---|---|
| Education | Increasing knowledge or understanding | Provide instruction about exercise, increase understanding of why it is important for physical health. |
| Persuasion | Using communication to induce positive or negative feelings or simulate action | Discussing the benefits of a healthy lifestyle, such as improved mood, more energy; and provide general encouragement when behaviour is carried out. |
| Incentivization | Creating expectation of reward | Encourage goal setting, such as 2 hours per week exercise and allocating rewards when goals are met. |
| Coercion | Creating expectation of punishment or cost | Provide information about consequences of unhealthy habits; for example, smoking increases cancer risk. |
| Training | Imparting skills | Encourage the relevant skills to be developed that enable a person to be able to exercise, such as gym training. |
| Restriction | Using rules to reduce the opportunity to engage in the target behaviour (or to increase the target behaviour by reducing the opportunity to engage in competing behaviours) | Increase the minimum price of alcohol frequently used to target younger populations, such as alcopops. |
| Environmental restructuring | Changing the physical or social context | Private gym, diet, or behavioural support classes for young people who are taking part in the intervention with a trainer who has awareness of mental health. |
| Modelling | Providing an example for people to aspire to or imitate | Using a gym buddy system where UHR individuals are accompanied to exercise sessions by a peer or staff member. |
| Enablement | Increasing means/reducing barriers to increase capability or opportunity | Prompt practice of exercise sessions or cooking sessions, accompany an individual to gym until they feel confident to go alone. |
| Policy | ||
| communication/marketing | Using print/electronic/telephonic or broadcast media | Develop leaflets and materials to be used in the UHR service, which educate people about living a healthy lifestyle or provide warnings to stop smoking. |
| Guidelines | Creating documents that recommend or mandate practice, including changes to service provision | Ensure young people who access UHR services have a physical health assessment and are given information about their health. |
| Fiscal | Using the tax system to reduce or increase the financial cost | Increase taxation on tobacco and high‐sugar products. |
| Regulation | Establish rules or principles of behaviour or practice | Reduce adverts for fast food in areas populated by young people such as around colleges and replace with healthy food or gyms. |
| Legislation | Making or changing laws | Enforce limits on the amount of alcohol one person can buy if under the age of 21 years. |
| Environmental/social planning | Designing and/or controlling the physical or social environment | Encourage local areas to have accessible facilities, such as gyms and green spaces. |
| Service provision | Delivering a service | Encourage parity of esteem in mental health services. |
UHR, ultra‐high risk for psychosis.
Although a relatively new model, the COM‐B model has been successfully applied as a framework to the English Department of Health 2010 tobacco control strategy (Health, 2010), the NICE guidance on reducing obesity (NICE, 2006), medication adherence and management (Jackson et al. 2014; Sinnott et al. 2015), management of spinal cord injury (Bérubé et al. 2015), childhood obesity (Curtis et al. 2015b; Robinson et al. 2013), and promotion of safe‐sex practices (Newby et al. 2013). It has also recently been adopted by Improving Access to Psychological Therapy teams to guide the application of low‐intensity lifestyle interventions for psychological well‐being practitioners and other health professionals.
Application of the COM‐B model to a UHR cohort
We propose that the COM‐B model could be useful to develop a lifestyle intervention to promote the physical health of the UHR group. It provides a systematic and standardized approach to developing an intervention, and allows theoretically‐based BCT to be applied to guide behaviour change. Using clearly‐defined techniques proposed by the COM‐B model and behaviour‐change wheel taxonomy will ensure transparency and enable replication of an intervention (Abraham and Michie, 2008; Michie et al. 2011c). To date, there have been no published or recorded physical health interventions for the UHR group. We suggest that using a theoretically‐based framework to develop an intervention will provide a good baseline to conduct further research and develop health‐service provision for this population. In the present study, we outline how each of the three components of the behaviour‐change wheel could be addressed for the UHR cohort (Fig. 2).
Figure 2.
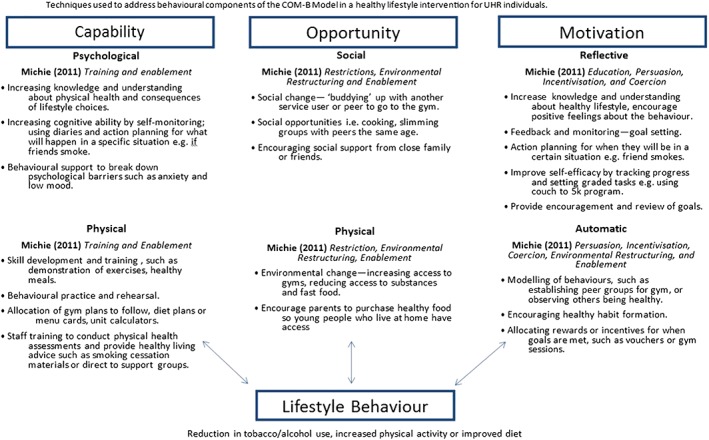
Techniques used to address capability, opportunity and motivation from the COM‐B model. [Colour figure can be viewed at http://wileyonlinelibrary.com]
Motivation
Amotivation or avolition is observed in some young UHR individuals, and can impact on a person's daily functioning (Piskulic et al. 2012). Targeting motivation according to the COM‐B model could involve increasing knowledge about exercise and diet, and discussing the benefits of living a healthy lifestyle. Goal setting and self‐monitoring, such as aiming for two gym sessions per week or eating five servings of fruit and vegetables daily, recorded in a diary might increase reflective motivation.
The concept of self‐efficacy has an important influence on motivation (Bandura, 1977; Schunk, 1995; Zimmerman et al. 1992). Self‐efficacy refers to an individual's belief in their own capacity to engage in a given behaviour (Bandura, 1977; Bandura, 1982). Motivation is enhanced when people have a greater sense of competency and self‐belief that they can complete a task (Schunk, 1995; Zimmerman et al. 1992). Empirical evidence suggests self‐efficacy has an important role in determining whether an individual engages in a given health behaviour and their motivation to change that behaviour (Holloway and Watson, 2002; Thirlaway and Upton, 2009). Programmes targeting self‐efficacy to increase healthy eating in adolescents are effective in improving dietary choices and increasing physical activity in adults (Fitzgerald et al. 2013; Lee et al. 2008; Olander et al. 2013). Despite this, self‐efficacy has not been explored in UHR individuals. However, in people with schizophrenia, a lack of self‐belief and low physical competence (i.e. low self‐efficacy) is related to physical inactivity (Vancampfort et al. 2011). Therefore, self‐efficacy could be an appropriate target for the UHR group.
Opportunity
Considering environmental factors and social opportunities could prove useful when developing interventions for the UHR group, as poor social environment, deprivation, and other socioeconomic factors are risk factors for psychosis, and UHR individuals tend to live in socially‐deprived areas (Allardyce et al. 2005; Cotter et al. 2015; O'Donoghue et al. 2015). Working with young people to change the context in which a behaviour usually does (or does not) occur might be helpful to promote a healthy lifestyle. For instance, if a person lives in a deprived area, rather than encouraging them to exercise outdoors, sessions could be conducted in local gyms in a safe environment. Thus, the environmental setting can be developed to be as conducive to an individual as possible. A supportive social environment could be created by conducting small group sessions with other participants who are also motivated to improve their physical health.
Capability
Enhancing psychological capability might focus on breaking down some of the psychological barriers young people experience. This could include providing behavioural support for low mood and high levels of anxiety experienced by UHR individuals. Physical capability could also be targeted using education and training intervention functions to demonstrate correct exercise techniques, such as following a gym workout with a trainer.
Relevance for Clinical Practice
It is not only the behaviours of UHR individuals that should be targeted to promote a healthier lifestyle. Clinical services also need to be aware that monitoring physical health is important, and interventions to improve physical health in the UHR cohort are required. This arises from recent findings, which suggest physical health and associated health behaviours are not monitored on a routine basis by UHR services (Carney et al. 2015). Happell et al. (2012) also argue that despite being a rising topic, more research is required in order to facilitate integrated care for physical and mental health needs. One way to address this is to equip mental health nurses with the ability to promote physical health in this group.
The important role mental health nurses can have to improve the general health of people with mental health difficulties has previously been recognized (Bradshaw and Pedley, 2012; Happell et al. 2011; Robson and Gray, 2007) First, as many have daily contact with service users, this time could be used to work together to address unhealthy lifestyle factors (Bradshaw and Pedley, 2012; Stanton et al. 2015). Schemes, such as ‘Making every contact count’, might be effective, where health professionals are trained to facilitate behaviour change at every contact with a client (Lawrence et al. 2016). Second, nurses make up the largest component of the health‐care workforce, which results in an increased chance of implementation if interventions are rolled out on a larger scale. Third, encouraging mental health nurses to focus on both the physical and mental health of an individual promotes a more holistic approach to health care; one that is required to address physical health disparities (De Hert et al. 2011).
The outer circle of the behaviour‐change wheel focuses on changes to policy to encourage wider‐scale behaviour change, such as service provision, or policy guidelines (Table 1). Mandatory training in physical health promotion for all health professionals could allow it to be incorporated into general nursing practice. This could include training for mental health nurses to conduct physical health assessments and provide advice about diet, or integrating a physical health specialist into mental health services (Happell et al. 2016). Changes to policy guidelines might also be an effective way to promote physical health, such as including reminders to conduct physical health checks on the files of service users.
Future Recommendations
Interventions to promote physical health are required for UHR individuals due to high rates of unhealthy lifestyle factors such as physical inactivity and substance use. We recommend mental health nurses and wider health professionals use the principles of the COM‐B model and behaviour‐change wheel to develop a new healthy lifestyle intervention for the UHR group. Developing an intervention using this systematic method may have advantages over traditional approaches used to promote healthy living in mental healthcare settings, which are often not linked to any underlying theoretical framework, or developed structure and are applied on an ad‐hoc basis. Due to limited existing research, further qualitative research should be conducted with this population and the clinical staff prior to developing any intervention to identify what behaviour would be the most appropriate target. Determining the barriers to and facilitators of healthy lifestyle in the group, and establishing which behaviours they wish to change (e.g. smoking, diet, and physical activity) will be useful. The perspective of mental health professionals should also be considered to determine which interventions they believe are feasible and acceptable approaches to use.
Conclusion
Training mental health nurses and other health professionals to use the COM‐B model and behaviour change wheel could promote physical health for young people at risk for psychosis. Using a systematic and theoretically‐based approach to intervention development could result in effective methods of health promotion in this group. Given the lack of physical health research with the UHR group, we suggest that using a theoretically‐based framework to develop an intervention will provide a good baseline to conduct further research and develop health service provision for this population. The COM‐B model could be an appropriate framework to use, given the flexibility of the approach and ability to account for a wide range of behaviours. Additional training and development for mental health nurses could encourage a greater integration of mental and physical health care for young people in clinical services.
Acknowledgements
This work was supported by the Economic and Social Research Council (no. ES/J500094/1).
Rebekah Carney, MSc
Tim Bradshaw, RGN, RMn, PhD
Alison R. Yung, MD, FRANZCP
References
- Abdel‐Baki, A. , Brazzini‐Poisson, V. , Marois, F. , Letendre, É. & Karelis, A. D. (2013). Effects of aerobic interval training on metabolic complications and cardiorespiratory fitness in young adults with psychotic disorders: A pilot study. Schizophrenia Research, 149, 112–5. [DOI] [PubMed] [Google Scholar]
- Abraham, C. , Kelly, M. P. , West, R. & Michie, S. (2009). The UK National Institute for Health and Clinical Excellence public health guidance on behaviour change: A brief introduction. Psychology Health & Medicine, 14, 1–8. [DOI] [PubMed] [Google Scholar]
- Abraham, C. & Michie, S. (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology, 27, 379. [DOI] [PubMed] [Google Scholar]
- Addington, J. , Buchy, L. , Cadenhead, K. et al. (2015). Substance use in individuals at clinical high risk of psychosis. Schizophrenia Bulletin, 41, S104. [Google Scholar]
- Addington, J. , Cornblatt, B. A. , Cadenhead, K. S. et al. (2011). At Clinical High Risk for Psychosis: Outcome for Nonconverters. American Journal of Psychiatry, 168, 800–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Addy, P. H. , Radhakrishnan, R. , Cortes, J. A. & D'souza, D. C. (2012). Comorbid alcohol, cannabis, and cocaine use disorders in schizophrenia: epidemiology, consequences, mechanisms, and treatment. FOCUS: The Journal of Lifelong Learning in Psychiatry, 10, 140–53. [Google Scholar]
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211. [Google Scholar]
- Allardyce, J. , Gilmour, H. , Atkinson, J. , Rapson, T. , Bishop, J. & Mccreadie, R. (2005). Social fragmentation, deprivation and urbanicity: relation to first‐admission rates for psychoses. The British Journal of Psychiatry, 187, 401–6. [DOI] [PubMed] [Google Scholar]
- Alvarez‐Jimenez, M. , Gonzalez‐Blanch, C. , Vazquez‐Barquero, J. L. et al. (2006). Attenuation of antipsychotic‐induced weight gain with early behavioral intervention in drug‐naive first‐episode psychosis patients: A randomized controlled trial. The Journal of Clinical Psychiatry, 67, 1253–60. [DOI] [PubMed] [Google Scholar]
- Bandura, A. (1977). Self‐efficacy: toward a unifying theory of behavioral change. Psychological Review, 84, 191. [DOI] [PubMed] [Google Scholar]
- Bandura, A. (1982). Self‐efficacy mechanism in human agency. American Psychologist. [Google Scholar]
- Bandura, A. (1986). Social Foundations of Thought and Action: A Social Cognitive Theory. Upper Saddle River NJ: Prentice‐Hall. [Google Scholar]
- Bérubé, M. , Albert, M. , Chauny, J. M. et al. (2015). Development of theory‐based knowledge translation interventions to facilitate the implementation of evidence‐based guidelines on the early management of adults with traumatic spinal cord injury. Journal of Evaluation in Clinical Practice, 21, 1157–68. [DOI] [PubMed] [Google Scholar]
- Bradshaw, T. & Pedley, R. (2012). Evolving role of mental health nurses in the physical health care of people with serious mental health illness. International Journal of Mental Health Nursing, 21, 266–73. [DOI] [PubMed] [Google Scholar]
- Carney, R. , Bradshaw, T. & Yung, A. R. (2015). Monitoring of physical health in services for young people at ultra‐high risk of psychosis. Early Intervention in Psychiatry doi: 10.1111/eip.12288/abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carney, R. , Cotter, J. , Bradshaw, T. , Firth, J. & Yung, A. R. (2016). Cardiometabolic risk factors in young people at ultra‐high risk for psychosis: A systematic review and meta‐analysis. Schizophrenia Research, 170, 290–300. [DOI] [PubMed] [Google Scholar]
- Carta, M. G. , Hardoy, M. C. , Pilu, A. , et al. (2008). Improving physical quality of life with group physical activity in the adjunctive treatment of major depressive disorder. Clinical Practice and Epidemiology in Mental Health, 4, 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooney, G. M. , Dwan, K. , GreiG, C. A. et al. (2014). Exercise for depression. JAMA, 311(23), 2423–2423. [DOI] [PubMed] [Google Scholar]
- Cotter, J. , Drake, R. J. , Bucci, S. , Firth, J. , Edge, D. & Yung, A. R. (2014). What drives poor functioning in the at‐risk mental state? A systematic review. Schizophrenia Research, 159, 267–77. [DOI] [PubMed] [Google Scholar]
- Cotter, J. , Kaess, M. & Yung, A. (2015). Childhood trauma and functional disability in psychosis, bipolar disorder and borderline personality disorder: A review of the literature. Irish Journal of Psychological Medicine, 32, 21–30. [DOI] [PubMed] [Google Scholar]
- Craig, P. , Dieppe, P. , Macintyre, S. , Michie, S. , Nazareth, I. & Petticrew, M. (2008). Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ, 337, 1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis, J. , Watkins, A. , Rosenbaum, S. et al. (2015a). Keeping the body in mind: An individualised lifestyle and life‐skills intervention to prevent antipsychotic‐induced weight gain in first episode psychosis. Early Interv Psychiatry, 10(3), 267–276. [DOI] [PubMed] [Google Scholar]
- Curtis, K. E. , Lahiri, S. & Brown, K. E. (2015b). Targeting parents for childhood weight management: development of a theory‐driven and user‐centered healthy eating app. JMIR mHealth and uHealth, 3(2), e69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davies, P. , Walker, A. E. & Grimshaw, J. M. (2010). A systematic review of the use of theory in the design of guideline dissemination and implementation strategies and interpretation of the results of rigorous evaluations. Implementation Science, 5, 5908–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Hert, M. , Cohen, D. , Bobes, J. et al. (2011). Physical illness in patients with severe mental disorders. II. Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World Psychiatry, 10, 138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Hert, M. , Van Winkel, R. , Van Eyck, D. et al. (2006). Prevalence of diabetes, metabolic syndrome and metabolic abnormalities in schizophrenia over the course of the illness: A cross‐sectional study. Clinical Practice and Epidemiology in Mental Health, 2, 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Di Forti, M. , Sallis, H. , Allegri, F. et al. (2014). Daily use, especially of high‐potency cannabis, drives the earlier onset of psychosis in cannabis users. Schizophrenia Bulletin, 40, 1509–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DombrowskI, S. U. , Sniehotta, F. F. , Avenell, A. , Johnston, M. , Maclennan, G. & Araújo‐Soares, V. (2012). Identifying active ingredients in complex behavioural interventions for obese adults with obesity‐related co‐morbidities or additional risk factors for co‐morbidities: A systematic review. Health Psychology Review, 6, 7–32. [Google Scholar]
- Firth, J. , Cotter, J. , Elliott, R. , French, P. & Yung, A. (2015). A systematic review and meta‐analysis of exercise interventions in schizophrenia patients. Psychological Medicine, 45, 1343–61. [DOI] [PubMed] [Google Scholar]
- Firth, J. , Carney, R. , Jerome, L. , Elliott, R. , French, P. & Yung, A.R. (2016). The effects and determinants of exercise participation in first-episode psychosis: a qualitative study. BMC Psychiatry, 16(36), 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzgerald, A. , Heary, C. , Kelly, C. , Nixon, E. & Shevlin, M. (2013). Self‐efficacy for healthy eating and peer support for unhealthy eating are associated with adolescents' food intake patterns. Appetite, 63, 48–58. [DOI] [PubMed] [Google Scholar]
- Fredrikson, D. H. , Boyda, H. N. , Tse, L. et al. (2014). Improving metabolic and cardiovascular health at an early psychosis intervention program in Vancouver, Canada. Frontiers in Psychiatry, 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fusar‐Poli, P. , Borgwardt, S. , Bechdolf, A. et al. (2013). The psychosis high‐risk state: a comprehensive state‐of‐the‐art review. JAMA Psychiatry, 70, 107–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fusar‐Poli, P. , Nelson, B. , Valmaggia, L. , Yung, A. R. & Mcguire, P. K. (2014). Comorbid depressive and anxiety disorders in 509 individuals with an at‐risk mental state: Impact on psychopathology and transition to psychosis. Schizophrenia Bulletin, 40, 120–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurillo, P. , Jauhar, S. , Murray, R. M. & Maccabe, J. H. (2015). Does tobacco use cause psychosis? Systematic review and meta‐analysis. The Lancet Psychiatry, 2(8) 718–725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankonen, N. , Sutton, S. , Prevost, A. T. et al. (2014). Which behavior change techniques are associated with changes in physical activity, diet and body mass index in people with recently diagnosed diabetes? Annals of Behavioral Medicine, 49, 7–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Happell, B. , Davies, C. & Scott, D. (2012). Health behaviour interventions to improve physical health in individuals diagnosed with a mental illness: A systematic review. International Journal of Mental Health Nursing, 21, 236–47. [DOI] [PubMed] [Google Scholar]
- Happell, B. , Ewart, S. B. , Platania‐Phung, C. et al. (2016). Embedding a physical health nurse consultant within mental health services: Consumers' perspectives. International Journal of Mental Health Nursing, 25, 377–384. [DOI] [PubMed] [Google Scholar]
- Happell, B. , Platania‐Phung, C. & Scott, D. (2011). Placing physical activity in mental health care: A leadership role for mental health nurses. International Journal of Mental Health Nursing, 20, 310–8. [DOI] [PubMed] [Google Scholar]
- Hardeman, W. , Johnston, M. , Johnston, D. , Bonetti, D. , Wareham, N. & Kinmonth, A. L. (2002). Application of the theory of planned behaviour in behaviour change interventions: A systematic review. Psychology and Health, 17, 123–58. [Google Scholar]
- Health, D. O . 2010. A Smoke‐Free Future: A comprehensive tobacco control strategy for England London. [Cited 14 Jun 2016]. Available from: URL: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_111749. [Google Scholar]
- Hennekens, C. H. , Hennekens, A. R. , Hollar, D. & Casey, D. E. (2005). Schizophrenia and increased risks of cardiovascular disease. American Heart Journal, 150, 1115–21. [DOI] [PubMed] [Google Scholar]
- Hillsdon, M. , Foster, C. , Cavill, N. , Crombie, H. & Naidoo, B. (2004). The effectiveness of public health interventions for increasing physical activity among adults: a review of reviews: evidence briefing summary. London: Health Development Agency London. [Google Scholar]
- Holloway, A. & Watson, H. E. (2002). Role of self‐efficacy and behaviour change. International Journal of Nursing Practice, 8, 106–15. [DOI] [PubMed] [Google Scholar]
- Jackson, C. , Eliasson, L. , Barber, N. & Weinman, J. (2014). Applying COM‐B to medication adherence. Eur Health Psychol, 16, 7–17. [Google Scholar]
- Killackey, E. , Anda, A. L. , Gibbs, M. et al. (2011). Using internet enabled mobile devices and social networking technologies to promote exercise as an intervention for young first episode psychosis patients. BMC Psychiatry, 11, 80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knubben, K. , Reischies, F. M. , Adli, M. , Schlattmann, P. , Bauer, M. & Dimeo, F. (2007). A randomised, controlled study on the effects of a short‐term endurance training programme in patients with major depression. British Journal of Sports Medicine, 41, 29–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koivukangas, J. , Tammelin, T. , Kaakinen, M. et al. (2010). Physical activity and fitness in adolescents at risk for psychosis within the Northern Finland 1986 Birth Cohort. Schizophrenia Research, 116, 152–8. [DOI] [PubMed] [Google Scholar]
- Lawrence, W. , Black, C. , Tinati, T. et al. (2016). ‘Making every contact count’: Evaluation of the impact of an intervention to train health and social care practitioners in skills to support health behaviour change. Journal of Health Psychology, 21, 138–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, L.‐L. , Arthur, A. & Avis, M. (2008). Using self‐efficacy theory to develop interventions that help older people overcome psychological barriers to physical activity: A discussion paper. International Journal of Nursing Studies, 45, 1690–9. [DOI] [PubMed] [Google Scholar]
- Lin, A. , Wood, S. J. , Nelson, B. , Beavan, A. , Mcgorry, P. & Yung, A. R. (2015). Outcomes of nontransitioned cases in a sample at ultra‐high risk for psychosis. American Journal of Psychiatry, 172, 249–58. [DOI] [PubMed] [Google Scholar]
- Lin, J. , Lam, M. , Chiu, C. , et al. (2011). The impacts of yoga and exercise on neuro‐cognitive function and symptoms in early psychosis. Schizophrenia Bulletin, 37, 171–1. [Google Scholar]
- Lovell, K. , Wearden, A. , Bradshaw, T. et al. (2014). An exploratory randomized controlled study of a healthy living intervention in early intervention services for psychosis: the INTERvention to encourage ACTivity, improve diet, and reduce weight gain (INTERACT) study. The Journal of Clinical Psychiatry, 75, 498–505. [DOI] [PubMed] [Google Scholar]
- Martinsen, E. W. , Medhus, A. & Sandvik, L. (1985). Effects of aerobic exercise on depression: A controlled study. British Medical Journal (Clinical Research Ed.), 291, 109–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , Abraham, C. , Whittington, C. , Mcateer, J. & Gupta, S. (2009). Effective techniques in healthy eating and physical activity interventions: A meta‐regression. Health Psychology, 28, 690. [DOI] [PubMed] [Google Scholar]
- Michie, S. , Ashford, S. , Sniehotta, F. F. , Dombrowski, S. U. , BishoP, A. & French, D. P. (2011a). A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO‐RE taxonomy. Psychology & Health, 26, 1479–98. [DOI] [PubMed] [Google Scholar]
- Michie, S. , Atkins, L. & West, R. (2015). The behaviour change wheel: A guide to designing interventions London: Silverback. [Google Scholar]
- Michie, S. , Hyder, N. , Walia, A. & West, R. (2011b). Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addictive Behaviors, 36, 315–9. [DOI] [PubMed] [Google Scholar]
- Michie, S. & Johnston, M. (2012). Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychology Review, 6, 1–6. [Google Scholar]
- Michie, S. & Prestwich, A. (2010). Are interventions theory‐based? Development of a theory coding scheme. Health Psychology, 29, 1. [DOI] [PubMed] [Google Scholar]
- Michie, S. , Van Stralen, M. M. & West, R. (2011c). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science: IS, 6, 42–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , Whittington, C. , Hamoudi, Z. , Zarnani, F. , Tober, G. & West, R. (2012). Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction, 107, 1431–40. [DOI] [PubMed] [Google Scholar]
- Mota‐Pereira, J. , Silverio, J. , Carvalho, S. , Ribeiro, J. C. , Fonte, D. & Ramos, J. (2011). Moderate exercise improves depression parameters in treatment‐resistant patients with major depressive disorder. Journal of Psychiatric Research, 45, 1005–11. [DOI] [PubMed] [Google Scholar]
- Nelson, B. , Yuen, H. P. , Wood, S. J. et al. (2013). Long‐term follow‐up of a group at ultra high risk (‘prodromal’) for psychosis: the PACE 400 study. JAMA Psychiatry, 70, 793–802. [DOI] [PubMed] [Google Scholar]
- Newby, K. V. , French, D. P. , Brown, K. E. & Lecky, D. M. (2013). Increasing young adults' condom use intentions and behaviour through changing chlamydia risk and coping appraisals: Study protocol for a cluster randomised controlled trial of efficacy. BMC Public Health, 13, 528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NICE (2006). Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children London: NICE. [PubMed] [Google Scholar]
- NICE (2007). Behaviour change at population, community and individual levels (Public Health Guidance 6) London: NICE. [Google Scholar]
- NICE (2014). Behaviour change: individual approaches (Public Health Guidance 49) London: NICE. [Google Scholar]
- O'donoghue, B. , Yung, A. R. , Wood, S. et al. (2015). Neighbourhood characteristics and the rate of identification of young people at ultra‐high risk for psychosis. Schizophrenia Research, 169(1‐3), 214–216. [DOI] [PubMed] [Google Scholar]
- Olander, E. K. , Fletcher, H. , Williams, S. , Atkinson, L. , Turner, A. & French, D. P. (2013). What are the most effective techniques in changing obese individuals' physical activity self‐efficacy and behaviour: A systematic review and meta‐analysis. International Journal of Behavioral Nutrition and Physical Activity, 10, 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pilu, A. , Sorba, M. , Hardoy, M. C. et al. (2007). Efficacy of physical activity in the adjunctive treatment of major depressive disorders: preliminary results. Clinical Practice and Epidemiology in Mental Health, 3, 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piskulic, D. , Addington, J. , Cadenhead, K. S. et al. (2012). Negative symptoms in individuals at clinical high risk of psychosis. Psychiatry Research, 196, 220–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prestwich, A. , Sniehotta, F. F. , Whittington, C. , Dombrowski, S. U. , Rogers, L. & Michie, S. (2014). Does theory influence the effectiveness of health behavior interventions? Meta‐analysis. Health Psychology, 33, 465. [DOI] [PubMed] [Google Scholar]
- Prochaska, J. O. & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American Journal of Health Promotion, 12, 38–48. [DOI] [PubMed] [Google Scholar]
- Robinson, E. , Higgs, S. , Daley, A. J. et al. (2013). Development and feasibility testing of a smart phone based attentive eating intervention. BMC Public Health, 13, 639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robson, D. & Gray, R. (2007). Serious mental illness and physical health problems: A discussion paper. International Journal of Nursing Studies, 44, 457–66. [DOI] [PubMed] [Google Scholar]
- Rosenbaum, S. , Tiedemann, A. , Sherrington, C. , Curtis, J. & Ward, P. B. (2014). Physical activity interventions for people with mental illness: a systematic review and meta‐analysis. The Journal of Clinical Psychiatry, 75, 964–74. [DOI] [PubMed] [Google Scholar]
- Rosenstock, I. M. (1974). The health belief model and preventive health behavior. Health Education Monographs, 2, 354–86. [DOI] [PubMed] [Google Scholar]
- Schuch, F. , Vasconcelos‐Moreno, M. , Borowsky, C. & Fleck, M. (2011). Exercise and severe depression: preliminary results of an add‐on study. Journal of Affective Disorders, 133, 615–8. [DOI] [PubMed] [Google Scholar]
- Schunk, D. H. (1995). Self‐efficacy, motivation, and performance. Journal of Applied Sport Psychology, 7, 112–37. [Google Scholar]
- Shiers, D. , Bradshaw, T. & Campion, J. (2015). Health inequalities and psychosis: Time for action. The British Journal of Psychiatry, 207, 471–3. [DOI] [PubMed] [Google Scholar]
- Sinnott, C. , Mercer, S. W. , Payne, R. A. , Duerden, M. , Bradley, C. P. & Byrne, M. (2015). Improving medication management in multimorbidity: development of the MultimorbiditY COllaborative Medication Review And DEcision Making (MY COMRADE) intervention using the Behaviour Change Wheel. Implementation Science, 10, 132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, J. , Williams, B. , Band, M. et al. (2014). SHAPE (Supporting Health and Promoting Exercise) Project for young people with psychosis. Early Intervention in Psychiatry, 8, 122–123.23458284 [Google Scholar]
- Stanton, R. , Happell, B. & Reaburn, P. (2015). Investigating the exercise‐prescription practices of nurses working in inpatient mental health settings. International Journal of Mental Health Nursing, 24, 112–20. [DOI] [PubMed] [Google Scholar]
- Thirlaway, K. & Upton, D. (2009). The psychology of lifestyle: Promoting healthy behaviour London: Routledge. [Google Scholar]
- Van Der Gaag, M. , Smit, F. , Bechdolf, A. et al. (2013). Preventing a first episode of psychosis: meta‐analysis of randomized controlled prevention trials of 12 month and longer‐term follow‐ups. Schizophrenia Research, 149, 56–62. [DOI] [PubMed] [Google Scholar]
- Vancampfort, D. , Probst, M. , Scheewe, T. et al. (2013). Relationships between physical fitness, physical activity, smoking and metabolic and mental health parameters in people with schizophrenia. Psychiatry Research, 207, 25–32. [DOI] [PubMed] [Google Scholar]
- Vancampfort, D. , Probst, M. , Sweers, K. , Maurissen, K. , Knapen, J. & De Hert, M. (2011). Relationships between obesity, functional exercise capacity, physical activity participation and physical self‐perception in people with schizophrenia. Acta Psychiatrica Scandinavica, 123, 423–30. [DOI] [PubMed] [Google Scholar]
- Yung, A. R. , Phillips, L. J. , Nelson, B. et al. (2011). Randomized controlled trial of interventions for young people at ultra high risk for psychosis: 6‐month analysis. The Journal of Clinical Psychiatry, 72, 430–40. [DOI] [PubMed] [Google Scholar]
- Yung, A. R. , Phillips, L. J. , Yuen, H. P. & Mcgorry, P. D. (2004). Risk factors for psychosis in an ultra high‐risk group: psychopathology and clinical features. Schizophrenia Research, 67, 131–42. [DOI] [PubMed] [Google Scholar]
- Zimmerman, B. J. , Bandura, A. & Martinez‐Pons, M. (1992). Self‐motivation for academic attainment: The role of self‐efficacy beliefs and personal goal setting. American Educational Research Journal, 29, 663–76. [Google Scholar]