

Abstract
In the Women’s Health Initiative randomized trial evaluating estrogen plus progestin after 5.6 years’ intervention and 8 years’ cumulative median follow-up, there were more lung cancer deaths in the hormone-treated group (P = .01). Now, after 6 years’ additional postintervention follow-up, the increase in lung cancer deaths was found to be attenuated (linear trend for difference over time, P = .042).
Introduction:
In the Women’s Health Initiative (WHI) estrogen plus progestin trial, after 5.6 years’ intervention and 8 years’ median follow-up, more women died from lung cancer in the hormone therapy group (hazard ratio [HR], 1.71; 95% confidence interval [CI], 1.16–2.52; P = .01). Now after 14 years’ median follow-up, we reexamined combined hormone therapy effects on lung cancer mortality.
Patients and Methods:
In the WHI placebo-controlled trial, 16,608 postmenopausal women aged 50 to 79 years and with an intact uterus were randomly assigned to once-daily 0.625 mg conjugated equine estrogen plus 2.5 mg medroxyprogesterone acetate (n = 8506) or placebo (n = 8102). Incidence and mortality rates for lung cancer were assessed from multivariant proportional hazard models.
Results:
After 14 years’ cumulative follow-up, there were 219 lung cancers (0.19% per year) in the estrogen plus progestin group and 184 (0.17%) in the placebo group (HR, 1.12; 95% CI, 0.92–1.37; P = .24). While there were more deaths from lung cancer with combined hormone therapy (153 [0.13%] vs. 132 [0.12%], respectively), the difference was not statistically significant (HR, 1.09; 95% CI, 0.87–1.38; P = .45). The statistically significant increase in deaths from lung cancer observed during intervention in women assigned to estrogen plus progestin was attenuated after discontinuation of study pills (linear trend over time, P = .042).
Conclusion:
The increased risk of death from lung cancer observed during estrogen plus progestin use was attenuated after discontinuation of combined hormone therapy.
Keywords: Estrogen plus progestin, Lung cancer, Lung cancer mortality, Randomized trial, Women’s Health Initiative
Introduction
In the Women’s Health Initiative (WHI) clinical trial evaluating estrogen plus progestin in postmenopausal women, after a median 5.6 years’ intervention and 8.0 years’ cumulative follow-up, there were 23% more lung cancers in the combined hormone therapy group, a nonsignificant difference (P = .16). However, more women died from lung cancer in the combined hormone therapy group (73 [yearly incidence 0.11%] vs. 40 [0.06%]; hazard ratio [HR], 1.71; 95% confidence interval [CI], 1.16–2.52; P = .01).1 In the WHI trial evaluating estrogen alone in postmenopausal women with prior hysterectomy, no effect on lung cancer incidence or outcome was observed.2 Findings from these trials led to the hypothesis that estrogen plus progestin adversely influences lung cancer outcome.
Results from observational studies of menopausal hormone therapy and lung cancer incidence have been mixed, with lower risk,3–5 no effect,6,7 and increased risk8,9 reported. However, 2 recent meta-analyses have associated hormone therapy use with significantly lower lung cancer incidence.10,11
Against this background, when the WHI clinical trial was updated after a median cumulative follow-up of 13 years, estrogen plus progestin did not influence lung cancer incidence (HR, 1.10; 95% CI, 0.89–1.35).12 In that report, deaths from and after lung cancer and findings by histology and smoking status were not reported. Therefore, we conducted analyses to determine whether the adverse effect of estrogen plus progestin on deaths from lung cancer observed during the intervention1 persisted during long-term postintervention follow-up.
Materials and Methods
Participants and Outcomes
The design of the WHI hormone therapy trial evaluating estrogen plus progestin has been described elsewhere.13,14 Post-menopausal women aged 50 to 79 years with an intact uterus were entered from 40 clinical centers in the United States from 1993 to 1998. Not eligible were women with previous breast cancer, any other cancer within 10 years except for nonmelanoma skin cancer, or women with an anticipated survival of less than 3 years. Menopausal hormone therapy users required a 3-month washout before entry. The trial was approved by institutional review boards at each clinical center, and participants provided written informed consent. Information on demographic and other variables, including tobacco use, was collected using standard questionnaires. Medication use was collected by interview and review of medication containers. Clinical outcome information was collected at 6-month intervals through March 2005 and then annually.
The primary study efficacy outcome was coronary heart disease, with a calculated sample size of 15,125 based on anticipated 21% risk reduction.13 The primary safety outcome was invasive breast cancer. Other primary end points as a component of a monitoring global index included stroke, hip fracture, pulmonary emboli, colorectal cancer, endometrial cancer, and death from any cause. Although lung cancer was not a predefined study outcome, reports of lung cancer were confirmed, initially at the clinical centers by centrally trained physician adjudicators after medical record review. Final adjudication was conducted at the WHI Clinical Coordinating Center using the Surveillance, Epidemiology and End Results coding system.15 Attribution of cause of death was based on medical record and death certificate review (Seattle, WA, USA). Linkage to the National Death Index was conducted serially.
Randomization and Masking
Women were randomly allocated to daily combined conjugated equine estrogens (0.625 mg/day) plus medroxyprogesterone acetate (2.5 mg/day) tablets (Prempro; Wyeth-Ayerst, Collegeville, PA, USA) or an identical-appearing placebo using a computerized permuted block algorithm stratified by age and randomization in the WHI dietary modification trial. Double-blind study drug dispensing utilized a secured database system and was implemented by the Clinical Coordinating Center (Seattle, WA, USA). Participants and clinical center physicians and staff were blinded to the randomization group, with unblinding only if needed to manage adverse events. Chest imaging was not protocol defined, and medical decisions regarding pulmonary findings were directed by community physicians.
Procedures
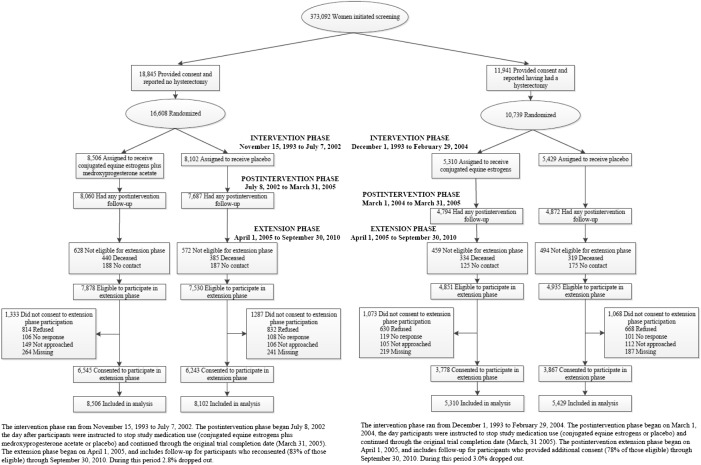
After 5 to 6 years (median), the intervention was ended when more risks than benefits with estrogen plus progestin were identified; participants were instructed to discontinue study drugs on July 8, 2002.13 Follow-up per protocol continued through March 31, 2005, the original trial termination date. Subsequent follow-up required reconsent, which was obtained from 12,788 participants, 83% of those surviving. The participant flow has been described elsewhere12 and is provided as a CONSORT diagram (Supplemental Figure 1 in the online version).
Statistical Analyses
Results for lung cancer incidence and deaths from lung cancer (those directly attributed to lung cancer) and deaths after lung cancer (regardless of cause) were assessed with time-to-event methods based on the intention-to-treat principle, which included all 16,608 randomized participants. Event times were defined relative to the randomization date. Cancer incidence rate comparisons are presented as HRs and 95% CIs from Cox proportional hazard models stratified by age, history of lung cancer, and randomization group in the WHI dietary modification trial.
Time-varying HRs were calculated and plotted, with the use of the same regression model adjustments as those listed above. The models fit a smooth, nonparametric HR over the entire follow-up period. In addition, the time-varying HRs were estimated separately in the intervention and postintervention periods, and a test for a linear trend in each phase performed. Analyses were conducted for all lung cancers and lung cancer deaths.
Subgroup analyses (smoking status, age at study entry [decade], and previous hormone use) were examined in Cox proportional hazard models with P values from Wald χ2 statistics. Because 3 subgroups were examined, less than 1 statistically significant interaction was expected by chance alone. Additional sensitivity analysis adjusted for adherence, censoring women 6 months after they became nonadherent (defined as consuming < 80% of study pills or initiating nonprotocol hormone therapy), incorporating time-varying weights, inversely proportional to the estimated probability of remaining adherent.
A level of .05 was used for assessing the statistical significance of P values in all analyses. SAS 9.3 1 for Windows (SAS Institute, Cary, NC, USA), and R 2.15 (R Development Core Team, http://www.R-project.org/), were used for all analyses. All statistical tests were 2-sided. This study was registered with ClinicalTrials.gov ().
The study sponsor had input into the design and conduct of the study and participated in the review but not in the preparation of the report. The corresponding author had full access to all the study data and had final responsibility to submit the document for publication.
Results
Baseline demographic characteristics and disease risk factors, including age, race/ethnicity, and tobacco exposure, were balanced between randomization groups (Table 1). After 5.6 years’ (median) intervention and 14 years’ (median) cumulative follow-up, there were 219 lung cancers in the estrogen plus progestin group compared to 184 in the placebo group (yearly incidence 0.19% vs. 0.17%; HR, 1.12; 95% CI, 0.92–1.37; P = .24; Table 2).
Table 1.
Descriptive Characteristics of Participants at Baseline by Randomization Group
| Characteristic | Estrogen Plus Progestin (n = 8506) | Placebo (n = 8102) |
|---|---|---|
| Age at Screening | ||
| 50–59 years | 2837/8506 (33.4) | 2383/8102 (33.1) |
| 60–69 years | 3854/8506 (45.3) | 3655/8102 (45.1) |
| 70–79 years | 1815/8506 (21.3) | 1764/8102 (21.8) |
| Race/Ethnicity | ||
| White | 7141/8506 (84.0) | 6805/8102 (84.0) |
| Black | 548/8506 (6.4) | 574/8102 (7.1) |
| Hispanic | 471/8506 (5.5) | 415/8102 (5.1) |
| American Indian | 25/8506 (3.3) | 30/8102 (0.4) |
| Asian/Pacific Islander | 194/8506 (2.3) | 169/8102 (2.1) |
| Unknown | 127/8506 (1.5) | 109/8102 (1.3) |
| Body Mass Index | ||
| <25 kg/m2 | 1110/8506 (21.0) | 1096/8102 (20.3) |
| 25 to <30 kg/m2 | 1798/8506 (34.0) | 1915/8102 (35.5) |
| 30 kg/m2 | 2375/8506 (45.0) | 2385/8102 (44.2) |
| Prior Estrogen-Only Use | ||
| No | 7603/8506 (89.4) | 7237/8102 (89.3) |
| Yes | 903/8506 (10.6) | 864/8102 (10.7) |
| <5 years | 677/8506 (8.0) | 659/8102 (8.1) |
| 5 to <10 years | 134/8506 (1.6) | 109/8102 (1.3) |
| >10 years | 92/8506 (1.1) | 96/8102 (1.2) |
| Prior Estrogen Plus Progestin Use | ||
| No | 6990/8506 (82.2) | 6706/8102 (82.8) |
| Yes | 1516/8506 (17.8) | 1396/8102 (17.2) |
| <5 years | 1050/8506 (12.3) | 997/8102 (12.3) |
| 5 to <10 years | 315/8506 (3.7) | 258/8102 (3.2) |
| >10 years | 151/8506 (1.8) | 141/8102 (1.7) |
| Recent Hormone Use | ||
| No | 6277/8506 (73.8) | 6020/8102 (74.3) |
| Past <5 years | 727/8506 (8.6) | 679/8102 (8.4) |
| Past 5 to <10 years | 335/8506 (3.9) | 310/8102 (3.8) |
| Past >10 years | 609/8506 (7.2) | 599/8102 (7.4) |
| Current (3-month washout) | 554/8506 (6.5) | 491/8102 (6.1) |
| Oral Contraceptive Use (Ever) | 3695/8506 (43.3) | 3447/8102 (42.5) |
| Years Since Menopause | ||
| <10 years | 827/8506 (19.0) | 817/8102 (18.3) |
| 10–19 years | 1292/8506 (29.7) | 1333/8102 (29.8) |
| >20 years | 2230/8506 (51.3) | 2319/8102 (51.9) |
| Tobacco Exposure | ||
| Smoking Status | ||
| Never | 4178/8420 (49.6) | 3999/7994 (50.0) |
| Past | 3362/8420 (39.9) | 3157/7994 (39.5) |
| Current | 880/8420 (10.5) | 838/7994 (10.5) |
| No. of Cigarettes per Day | ||
| <25 | 3345/4097 (81.6) | 3175/3873 (82.0) |
| >25 | 752/4097 (18.4) | 698/3873 (18.0) |
| Years Smoked | ||
| <30 | 2563/4109 (62.4) | 2422/3912 (61.9) |
| >30 | 1546/4109 (37.6) | 1490/3912 (38.1) |
| Pack-Years of Smoking | ||
| Never smoker | 4178/8228 (50.8) | 3999/7822 (51.1) |
| <5 | 1119/8228 (13.6) | 1004/7822 (12.8) |
| 5 to <20 | 1168/8228 (14.2) | 1140/7822 (14.6) |
| >20 | 1763/8228 (21.4) | 1679/7822 (21.5) |
| Lung cancer (>10 years prior) | 3/8435 (<0.1) | 2/8036 (<0.1) |
Because of rounding, percentages might not all total 100. Includes 331 women previously randomized to estrogen-alone group who were reassigned to estrogen plus progestin group after protocol change, as previously described. For current users, 3-month washout period required before entry. Current and previous smokers were combined when estimating total number of cigarettes per day, years smoked, and past years of smoking.
Table 2.
Lung Cancer Incidence and Mortality by Randomization Group (n = 16,608)
| Characteristic | Placebo, n (% Per Year) | E+P, n (% Per Year) | Hazard Ratio (95% CI) | P |
|---|---|---|---|---|
| Incidence | ||||
| Lung cancer | 184 (0.17) | 219 (0.19) | 1.12 (0.92–1.37) | .24 |
| Non–small-cell lung cancer | 125 (0.11) | 160 (0.14) | 1.23 (0.97–1.55) | .08 |
| Small-cell lung cancer | 20 (0.02) | 23 (0.02) | 1.09 (0.60–1 98) | .78 |
| Mortality: Deaths From: | ||||
| From lung cancer | 132 (0.12) | 153 (0.13) | 1.09 (0.87–1.38) | .45 |
| From non-small-cell lung cancer | 85 (0.08) | 109 (0.09) | 1.23 (0.92–1.63) | .16 |
| From small-cell lung cancer | 17 (0.02) | 21 (0.02) | 1.16 (0.61–2.21) | .64 |
| After diagnosis of lung cancer | 149 (0.14) | 170 (0.15) | 1.08 (0.87–1.34) | .50 |
| From non-small-cell lung cancer | 100 (0.09) | 124 (0.11) | 1.19 (0.91–1.54) | .20 |
| From small-cell lung cancer | 18 (0.02) | 22 (0.02) | 1.15 (0.62–2.15) | .65 |
Stratified by age group at randomization, history of lung cancer, and randomization arm in dietary modification trial.
One hundred seventy women in the combined hormone therapy group died after being diagnosed with lung cancer compared to 149 in the placebo group (0.15% vs. 0.14%, respectively; HR, 1.08; 95% CI, 0.87–1.34; P = .50). Of these deaths, 153 (0.13%) in the combined hormone therapy group and 132 (0.12%) in the placebo group were from lung cancer (HR, 1.09; 95% CI, 0.87–1.38; P = .45). None of the differences was statistically significant (Table 2).
Sensitivity analyses, adjusting for nonadherence, provided similar results for lung cancer incidence (HR, 1.20; 95% CI, 0.90–1.16) and deaths from lung cancer (HR, 1.20; 95% CI, 0.81–1.77).
In the prior analysis, after 8 years’ follow-up, there were more deaths from lung cancer in the combined hormone therapy group (73 deaths vs. 40 deaths in the hormone therapy and placebo groups, respectively, P = .01).1 In marked contrast, in the current analysis, during the 6 years’ (median) additional postintervention follow-up, the findings were reversed in that there were somewhat fewer deaths from lung cancer in the combined hormone therapy group (80 deaths vs. 92 deaths, respectively).
To address this apparent change in the risk pattern, we examined whether there was a difference in rate of deaths from lung cancer over time. Comparison of the death rates between the estrogen plus progestin and placebo groups from randomization date finds HRs consistently above 1 through year 9 beginning in the third year (Table 3).
Table 3.
Lung Cancer Death by Year Since Randomization
| Years Since Randomization | Placebo, n (% Per Year) | E+P, n (% Per Year) | Hazard ratio (95% CI) |
|---|---|---|---|
| 1 | 2 (0.02) | 2 (0.02) | 0.96 (0.13–6.78) |
| 2 | 8 (0.10) | 4 (0.05) | 0.48 (0.14–1.59) |
| 3 | 3 (0.04) | 9 (0.11) | 2.89 (0.78–10.66) |
| 4 | 6 (0.08) | 10 (0.12) | 1.59 (0.58–4.37) |
| 5 | 9 (0.11) | 11 (0.13) | 1.17 (0.48–2.82) |
| 6 | 7 (0.09) | 13 (0.16) | 1.78 (0.71–4.45) |
| 7 | 9 (0.12) | 12 (0.15) | 1.28 (0.54–3.03) |
| 8 | 7 (0.09) | 19 (0.24) | 2.59 (1.09–6.16) |
| 9 | 8 (0.11) | 11 (0.14) | 1.31 (0.53–3.27) |
| 10 | 13 (0.18) | 13 (0.17) | 0.96 (0.44–2.06) |
| 11 | 13 (0.18) | 9 (0.12) | 0.66 (0.28–1.55) |
| 12 | 15 (0.22) | 17 (0.24) | 1.08 (0.54–2.16) |
| 13 | 13 (0.22) | 12 (0.19) | 0.87 (0.40–1.91) |
| 14+ | 19 (0.16) | 11 (0.08) | 0.53 (0.25–1.12) |
| Total | 132 (0.12%) | 153 (0.13%) |
Subsequently, the combined hormone therapy effect on death from lung cancer was attenuated. The test for linear trend over time was statistically significant (P = .042), suggesting the increased risk of death from lung cancer in the estrogen plus progestin users decreased after both randomization groups stopped taking study pills after 5.6 years’ (median) active intervention (Table 3, Figure 1).
Figure 1.

Time-Varying Effects of Estrogen Plus Progestin on Lung Cancer Death. Smoothed Time-Varying Hazard Ratios and Their 95% Confidence Intervals (Dashed Line) Comparing Estrogen Plus Progestin Users and Nonhormone Users From Study Entry. Models Are Stratified by Age Group at Randomization, Prior Lung Cancer, and Dietary Modification Trial Randomization Arm
Considering lung cancer histology subgroups, somewhat more women were diagnosed with non–small-cell lung cancer in the estrogen plus progestin group (160 [0.14%] vs. 125 [0.11%], respectively; HR, 1.23; 95% CI, 0.97–1.55; P = .09). The non–small-cell cancers were more likely to be poorly differentiated (HR, 1.72; 95% CI, 1.04–2.83; P = .03) and somewhat more likely to be diagnosed with distant metastases (HR, 1.35; 95% CI, 0.93–1.97; P = .11; Table 4). Although there were more deaths from non–small-cell lung cancer in the combined hormone therapy group, the difference was not statistically significant (109 deaths [0.09%] vs. 85 [0.08%], respectively; HR, 1.23; 95% CI, 0.92–1.63; P = .16) (Table 2). The effect of combined hormone therapy on death from lung cancer was not modified by age at screening, pervious hormone treatment, or smoking status (Figure 2). The number of small-cell lung cancers was limited, and no significant differences emerged among randomization groups for either incidence or deaths from or after lung cancer.
Table 4.
Incidence of Non–Small-Cell Lung Cancer by Tumor Stage and Grade
| Characteristic | Placebo, n (% Per Year) | E+P, n (% Per Year) | Hazard Ratio (95% CI) | P |
|---|---|---|---|---|
| Non-Small-Cell Lung Cancer Histology | ||||
| Adenocarcinoma | 60 (0.05) | 73 (0.06) | 1.17 (0.83–1.64) | .47 |
| Squamous cell | 32 (0.03) | 28 (0.02) | 0.84 (0.50–1.39) | .33 |
| Large cell/neuroendocrine | 10 (0.01) | 15 (0.01) | 1.46 (0.66–3.26) | .35 |
| Unspecified | 23 (0.02) | 44 (0.04) | 1.82 (1.10–3.01) | .05 |
| Non-Small-Cell Lung Cancer Stage | ||||
| Local | 28 (0.03) | 29 (0.03) | 1.00 (0.59–1.68) | .99 |
| Regional | 29 (0.03) | 38 (0.03) | 1.26 (0.77–2.04) | .35 |
| Distant metastases | 47 (0.04) | 67 (0.06) | 1.35 (0.93–1.97) | .11 |
| Non-Small-Cell Lung Cancer Grade | ||||
| Well differentiated | 12 (0.01) | 12 (0.01) | 0.99 (0.44–2.20) | .97 |
| Moderately differentiated | 27 (0.02) | 26 (0.02) | 0.92 (0.54–1.57) | .75 |
| Poorly differentiated | 24 (0.02) | 43 (0.04) | 1.72 (1.04–2.83) | .03 |
| Anaplastic | 7 (0.01) | 5 (<0.01) | 0.67 (0.21–2.12) | .50 |
Stratified by age group at randomization, history of lung cancer, and randomization assignment in dietary modification trial.
Figure 2.

Cumulative Risk of Death From Lung Cancer by Study Group and Selected Baseline Characteristics. Cumulative Risk for Death From Lung Cancer Over Entire 14-Year (Median) Study Period. HRs, 95% CIs, and P Values Are From Cox Proportional Hazard models Stratified according to Age, Previous Lung Cancer, and Randomization Assignment in Dietary Modification Trial. Dotted Line Represents Overall HR for Deaths Attributed to Lung Cancer. *P Value is From Wald χ2 Test for Interaction Between Given Characteristic and Treatment Group. †Data for Smoking Status Were Not Available for 2 Women in Combined Hormone Therapy Group
Abbreviations: CI = confidence interval; HR = hazard ratio.
In exploratory analyses to allow comparison to observational studies, median survival for women diagnosed with non–small-cell lung cancer, measured from diagnosis date, was 13.8 months (interquartile range 3.3–39.0) in the combined hormone therapy group compared to 17.6 months (interquartile range 4.5–47.8) in the placebo group. After 5 years from diagnosis, mortality was 78% in the combined hormone therapy group and 71% in the placebo group (HR, 1.19; 95% CI, 0.89–1.59; P = .24).
With respect to smoking status, the yearly cancer incidence in the placebo group current smokers (0.70% per year) was substantially higher than in placebo group former smokers (0.19%) and especially never smokers (0.05%). Deaths from lung cancer were also substantially higher in placebo group participants who were current smokers at entry (0.49%) than in former smokers (0.14%) and never smokers (0.03%). However, the lung cancer outcomes were not higher in any estrogen plus progestin smoking status subgroup. When subgroups (smoking status, age at study entry [decade], prior hormone use) were examined for potential interaction, none was significant at the .05 level (Figure 2).
Discussion
With additional postintervention follow-up of the WHI randomized, placebo-controlled trial, the statistically significant increase in deaths from lung cancer observed during intervention in the estrogen plus progestin group was attenuated. The prior report on lung cancer findings included 8 years’ cumulative follow-up with 113 deaths from lung cancer.1 Now, with an additional 6 years’ (median) postintervention follow-up and 285 deaths from lung cancer, significant differences between randomization groups were no longer observed (153 deaths vs. 132 deaths, respectively; P = .55). Although the early findings could have been due to the play of chance, the statistically significant change in the year-to-year death rate over time suggests that the early adverse effect of estrogen plus progestin use on lung cancer mortality dissipated with termination of combined hormone therapy use.
An increase in deaths from lung cancer for women receiving estrogen and progestin therapy is biologically plausible. The non–small-cell lung cancers in the combined hormone therapy group were more likely to be poorly differentiated (P = .03), a potential clinical manifestation of estrogen’s ability to stimulate angiogenesis.16,17 In an earlier report from this trial, the non–small-cell lung cancers in the estrogen plus progestin group were also significantly more likely to be diagnosed with distant metastasis (40 cases [0.06%] vs. 22 cases [0.03%]; HR, 1.71; 95% CI, 1.02–2.88; P = .04).1 The change in clinical stage after intervention, where lung cancers with distant metastasis were no longer significantly higher in the combined hormone therapy group after intervention ended, suggests lung cancer mortality risk may be limited to some period around the time of estrogen and progestin exposure.
Preclinical findings and gender differences in lung cancer outcome are suggestive of hormonal influence.18,19 Lung cancer survival rates are higher in women than in men,20–22 older women have longer survival compared to younger women while no age effect is observed in men,23 and high estradiol concentrations have been associated with higher risk of deaths from lung cancer.24 Preclinical evidence supports a role of aromatase and estrogen signaling in the development and progression of lung cancer.18,19 Our randomized trial findings are also suggestive of an influence of exogenous estrogen plus progestin use on lung cancer outcome, at least around the time of active use.
Six observational studies have examined hormone therapy and survival after a lung cancer diagnosis. In one report of 489 women with lung cancer, significantly higher risk of death after lung cancer was described in the 86 hormone therapy users in analyses combining all hormone therapy regimens.25 In 2 reports, no association between hormone use and lung cancer outcome was observed.26,27 In an older report, nonspecified hormone therapy was associated with a lower risk of death from lung cancer.28 In 2 recent reports, a lower risk of death after lung cancer was associated with estrogen plus progestin29 as well as with estrogen alone30 use. We could identify no reports of lung cancer mortality relating survival to the date of hormone therapy initiation, as we report here.
Hormone therapy effects on lung cancer in the WHI randomization clinical trials for both estrogen plus progestin (no incidence increase but suggestive of an increase in deaths from lung cancer)1 in the current report and for estrogen alone (null effect)2 are in contrast to 2 recent meta-analyses of observational studies.10,11 In those reports, a statistically significant, lower lung cancer incidence was associated with hormone therapy,11 with one analysis finding lower lung cancer incidence with both estrogen alone and with estrogen plus progestin use.10 We cannot reconcile the WHI randomized trial findings with observational study meta-analysis results. However, cohort studies entering participants on menopausal hormone therapy may reflect time-related bias. For example, a woman who has been receiving hormone therapy for 8 years before entering the cohort has a “guarantee time,”31 because during that period she could not have been diagnosed with lung cancer (as she would not be eligible for the cohort). This problem could be overcome by including in analyses only women who initiated hormone therapy after entering a cohort.
Study strengths include the randomized double-blind, placebo-controlled design; the large study size; detailed and balanced tobacco exposure information; long follow-up; and adjudicated lung cancer outcomes. Information on treatment after diagnosis was not available, and the limitations of post hoc analyses are recognized. This WHI trial evaluated one specific hormone therapy regimen, and the findings may not apply to use of other agents or schedules.
In summary, the statistically significant increase in deaths from lung cancer observed during estrogen plus progestin intervention was attenuated after discontinuation of combined hormone therapy. Our lung cancer findings reinforce the value of long-term follow-up of randomized clinical trials. Differences between these findings and those from the preponderance of observational studies cannot be reconciled.
Clinical Practice Points
Preclinical evidence and gender differences in lung cancer clinical outcome suggest that estrogen signaling may be involved in lung cancer incidence and outcome. Against this background, the WHI conducted 2 full-scale, randomized, placebo-controlled trials evaluating estrogen plus progestin (in women with an intact uterus) and estrogen alone (in women with prior hysterectomy) to determine their relative benefits and risks.
A significantly increased risk of all cancers observed after stopping the estrogen plus progestin trial prompted an examination of lung cancers in both trials. Estrogen alone had no influence on lung cancer. In contrast, estrogen plus progestin significantly increased deaths from lung cancer by 71% (P = .01). Current smokers had their already high risk of lung cancer death increased by an additional 46%.
Now, after 14 years’ cumulative follow-up, a difference between randomization groups for deaths from lung cancer is no longer observed; a statistically significant change in the year-to-year death rate occurred with termination of combined hormone therapy use (linear trend over time, P = .042).
An increase in poorly differentiated cancers provides a likely mediator of the adverse lung cancer outcome. Postmenopausal women considering estrogen plus progestin use, especially those with a smoking history, should be made aware that this additional risk exists and that it begins to abate upon stopping combined hormone therapy use.
Supplementary Material
{kind=link}
Acknowledgments
The WHI program is reported by the National Heart, Lung and Blood Institute, National Institutes of Health, Department of Health and Human Services through contracts N01WH22110, 24152, 32100–2, 32105–6, 32108–9, 32111–13, 32115, 32118–32119, 32122, 42107–26, 42129–32, and 44221. We acknowledge the dedicated efforts of investigators and staff at the WHI clinical centers, the WHI Clinical Coordinating Center, and the National Heart, Lung and Blood program office (http://www.whi.org/). We also recognize the WHI participants for their extraordinary commitment to the WHI program.
The WHI Investigators comprise the following personnel: Program Office: Jacques Roscoe, Shari Ludlum, Dale Burden, Joan McGowan, Leslie Ford, and Nancy Geller (National Heart, Lung, and Blood Institute, Bethesda, MD). Clinical Coordinating Center: Garnet Anderson, Ross Prentice, Andrea LaCroix, and Charles Kooperberg (Fred Hutchinson Cancer Research Center, Seattle, WA). Investigators and Academic Centers: JoAnn E, Manson (Brigham and Women’s Hospital, Harvard Medical School, Boston, MA); Barbara V. Howard (MedStar Health Research Institute/Howard University, Washington, DC); Marcia L. Stefanick (Stanford Prevention Research Center, Stanford, CA); Rebecca Jackson (The Ohio State University, Columbus, OH); Cynthia A. Thompson (University of Arizona, Tucson/Phoenix, AZ); Jean Wactawski-Wende (University at Buffalo, Buffalo, NY); Marian Limacher (University of Florida, Gainesville/Jacksonville, FL); Robert Wallace (University of Iowa, Iowa City/Davenport, IA); Lewis Kuller (University of Pittsburgh, Pittsburgh, PA); Rowan T. Chlebowski (Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, CA); Sally Shumaker (Wake Forest University School of Medicine, Winston-Salem, NC). WHI Memory Study: Sally Shumaker (Wake Forest University School of Medicine, Winston-Salem, NC).
Footnotes
Disclosure
R.T.C. has received speaker’s fees and honoraria from Novartis; and honoraria for advisory boards and consulting for Novartis, Astra-Zeneca, Pfizer, Novo Nordisk, and Amgen. The other authors have no conflicts to declare.
Supplemental Data
Supplemental figure accompanying this article can be found in the online version at http://dx.doi.org/10.1016/j.cllc.2015.09.004.
References
- 1.Chlebowski RT, Schwartz AG, Wakelee H, et al. Oestrogen plus progestin and lung cancer in postmenopausal women (Women’s Health Initiative trial): a post-hoc analysis of a randomized controlled trial. Lancet 2009; 374:1243–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chlebowski RT, Anderson GL, Manson JE, et al. Lung cancer among post-menopausal women treated with estrogen alone in the Women’s Health Initiative randomized trial. J Natl Cancer Inst 2010; 102:1413–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Schabath MB, Wu X, Vassilopoulou-Sellin R, Spitz MR. Hormone replacement therapy and lung cancer risk: a case-control analysis. Clin Cancer Res 2004; 10: 113–23. [DOI] [PubMed] [Google Scholar]
- 4.Schwartz AG, Wenzlaff AS, Prysak GM, et al. Reproductive factors, hormone use, estrogen receptor expression and risk of non–small cell lung cancer in women. J Clin Oncol 2007; 25:5785–92. [DOI] [PubMed] [Google Scholar]
- 5.Rodriguez C, Spencer Feigelson H, Deka A, et al. Postmenopausal hormone therapy and lung cancer risk in the cancer prevention study II nutrition cohort. Cancer Epidemiol Biomarkers Prev 2008; 17:655–60. [DOI] [PubMed] [Google Scholar]
- 6.Kruezer M, Gerken M, Heinrich J, et al. Hormonal factors and risk of lung cancer among women? Int J Epidemiol 2003; 32:263–71. [DOI] [PubMed] [Google Scholar]
- 7.Baik CS, Strauss GM, Feskanich D. A prospective study of reproductive factors, hormone use, and risk of lung cancer in postmenopausal women. J Clin Oncol 2009; 27, abstract 1501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Taioli E, Wynder EL. Re: Endocinre factors and adenocarcinoma of the lung in women. J Natl Cancer Inst 1994; 86:869–70. [DOI] [PubMed] [Google Scholar]
- 9.Liu Y, Inoue M, Sobue T, et al. Reproductive factors, hormone use and the risk of lung cancer among middle-aged never-smoking Japanese women: a large-scale population-based cohort study. Int J Cancer 2005; 117:662–6. [DOI] [PubMed] [Google Scholar]
- 10.Pesatori AC, Carugno M, Consonni D, et al. Hormone use and risk for lung cancer: a pooled analysis from the International Lung Cancer Consortium (ILCCO). Br J Cancer 2013; 109:1954–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yao Y, Gu X, Zhu J, et al. Hormone replacement therapy in females can decrease the risk of lung cancer: a meta-analysis. PLoS One 2013; 8:e71236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Manson JA, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA 2013; 310:1353–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288:321–33. [DOI] [PubMed] [Google Scholar]
- 14.Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA 2004; 29:1701–12. [DOI] [PubMed] [Google Scholar]
- 15.National Cancer Institute. Surveillance Epidemiology and End Results. Available at: http://www.seer.cancer.gov. Accessed: September 9, 2009.
- 16.Ferrara N, Kerbel RS. Angiogenesis as a therapeutic target. Nature 2005; 438:967–74. [DOI] [PubMed] [Google Scholar]
- 17.Barnabas O, Wang H, Gao XM. Role of estrogen in angiogenesis in cardiovascular diseases. J Geriatr Cardiol 2013; 10:377–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Marquez-Garban DC, Chen HW, Goodglick L, et al. Targeting aromatase and estrogen signaling in human non–small cell lung cancer. Ann N Y Acad Sci 2009; 115:194–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Siegfried JM, Stabile LP. Estrogenic steroid hormones in lung cancer. Semin Oncol 2014; 41:5–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chlebowski RT, Palomares MR, Lillington L, et al. Recent implications of weight loss in lung cancer. Nutrition 1996; 12:S43–7. [DOI] [PubMed] [Google Scholar]
- 21.Bremes RM, Sundstrom S, Aasebo U, et al. , Norweigian Lung Cancer Study Group. The value of prognostic factors in small cell lung cancer: results from a randomized multicenter study with minimum 5 year follow-up. Lung Cancer 2003; 39:303–13. [DOI] [PubMed] [Google Scholar]
- 22.International Early Lung Cancer Action Program Investigators. Women’s susceptibility to tobacco carcinogens and survival after diagnosis of lung cancer. JAMA 2006; 296:180–4. [DOI] [PubMed] [Google Scholar]
- 23.Wakelee HA, Wang W, Schiller JH, et al. , Eastern Cooperative Oncology Group. Survival differences by sex for patients with advanced non–small cell lung cancer on Eastern Cooperative Oncology Group Trial 1594. J Thorac Oncol 2006; 1:441–6. [PubMed] [Google Scholar]
- 24.Ross H, Oldham FB, Bandstra B. Serum-free estradiol (E2) levels are prognostic in men with chemotherapy-naïve advanced non–small cell lung cancer (NSCLC) and performance status (PS). J Clin Oncol 2007; 25:15S, ASCO Ann Proc. [Google Scholar]
- 25.Ganti AK, Sahmoun AE, Panwalker AW, et al. Hormone replacement therapy is associated with decreased survival in women with lung cancer. J Clin Oncol 2006; 24:59–63. [DOI] [PubMed] [Google Scholar]
- 26.Ayeni O, Robinson A. Hormone replacement therapy and outcomes for women with non–small cell lung cancer: can an association be confirmed? Curr Oncol 2009; 16:21–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Huang B, Carloss H, Wyatt SE, et al. Hormone replacement therapy and survival from lung cancer in postmenopausal women in a rural population. Cancer 2009; 115:4167–75. [DOI] [PubMed] [Google Scholar]
- 28.Ettinger B, Friedman GD, Bush T, et al. Reduced mortality associated with long-term postmenopausal estrogen therapy. Obstet Gynecol 1996; 87:6–12. [DOI] [PubMed] [Google Scholar]
- 29.Katcoff H, Wenzlaff AS, Schwartz AG. Survival in women with NSCLC: the role of reproductive history and hormone use. J Thorac Oncol 2014; 9:355–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Clague J, Reynolds P, Henderson KD, et al. Menopausal hormone therapy and lung cancer–specific mortality following diagnosis: the California Teachers study. PLoS One 2014; 9:e103735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Suissa S. Randomized trials built on sand: examples from COPD, hormone therapy, and cancer. Rambam Maimonides Med J 2012; 3:e0014. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.