

Abstract
Background:
Osteoarthritis (OA) is a degenerative disease that not only causes knee pain in older adults, but also has an adverse effect on walking. Therefore, intervention for older patients with OA is important. To investigate the immediate effects of kinesiology taping (KT) on the pain and gait function of the older adults with knee OA.
Methods:
This study enrolled 10 older adults individuals living in the community who were diagnosed with knee OA. All participants were assessed for knee pain, walking ability, and balance before and after application of knee KT. Knee pain was assessed in resting and walking conditions using the visual analog scale. Walking and balance were assessed using a 10-m walking test and a timed up and go test.
Results:
In the present study, KT significantly improved gait and balance with reduction in knee pain during walking than non-KT (P < .05).
Conclusions:
This study demonstrated that knee KT has a positive effect on pain reduction and walking and balance ability of the older adults with OA. Therefore, this study suggests that KT can be used as an intervention to relieve knee pain and aid walking and balance ability in the older adult.
Keywords: gait, kinesiology tape, knee osteoarthritis, older adult, pain
1. Introduction
Knee osteoarthritis (OA) has a high incidence, and the symptoms include joint pain and stiffness, reduced range of motion, and pain that is exacerbated by activities such as climbing stairs, getting up from a chair, and walking for a long time.[1,2] Therefore, appropriate treatment and exercise is important for the older adults with knee OA.
One of the treatments, kinesiology taping (KT), is carried out by applying an adhesive strapping tape to the patella or surrounding soft tissue structures. There have been several methods of taping that have been applied.[3–5] KT alleviates knee pain by improving patellofemoral alignment and relieving the pressure and stress on soft tissues. Because inflammatory soft tissue can become worse when stretched, application of patella taping can provide stability to the knee by reducing the load on the infra-patellar fat pad or pesanserinus.[6,7] Several studies have recently reported the effectiveness of KT in terms of the reduction in the patellofemoral pain and improvement of posture control during functional activities.[8,9]
However, KT can be applied using various designs depending on the researcher, and the effect of each is different.[10] In other words, since the effect of KT depends on the application type, it is important to introduce various application methods to prove the effect. Therefore, the purpose of this study was to investigate the effect of knee KT on the gait of the older adults with OA and to establish the clinical basis of this effect. We hypothesized that KT would aid in knee pain reduction and enhance gait and balance ability than non-KT condition.
2. Methods
2.1. Participants
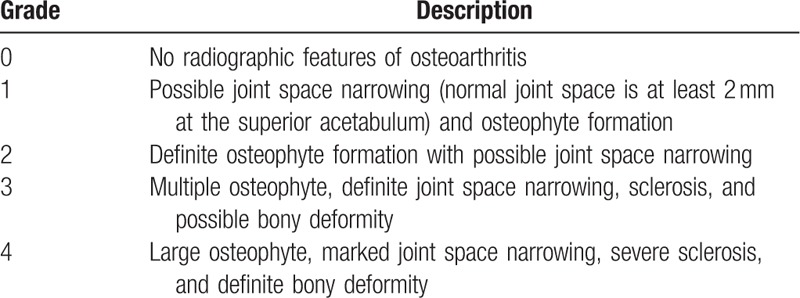
This study was conducted at an elderly welfare facility in South Korea. A total of 10 volunteer subjects with knee OA were recruited for the study. The inclusion criteria were as follows: 60 years old or older, diagnosed with knee OA by radiography, the surgeon then determined the grade of knee OA (1–3) according to the Kellgren and Lawrence (1957) scale[11] (Table 1), independent walking is possible, can carry out activities of daily life independently, and visual analog scale (VAS) score of knee pain >5. The exclusion criteria were as follows: knee swelling, underlying skin disorders, rheumatoid arthritis, previous knee joint surgery, and a planned surgical procedure on the knee joint within the next 6 months. We explained the objective and requirements of our study to all the participants and they voluntarily signed informed consent forms. Ethical approval was obtained from the Seoul Medical Center Institutional Review Board before conducting the experiment (SEOUL 2019-08-014-001).
Table 1.
Kellgren-Lawrence classification system.
2.2. Study procedure
This study was conducted using a one-group, pre and post design. KT (BB Tape, WETAPE Inc., Pyeongtaek, Korea) was applied by one experienced physical therapist on both knees. All participants were assessed in 2 conditions (KT and non-KT) and the order was randomized using a coin toss.
The application method of KT is as follows. KT is applied from below the patella to the lateral area of the quadriceps muscle with an approximate 10% to 15% stretch (Fig. 1A). KT is applied from below the patella to the medial area of the quadriceps muscle with an approximate 10% to 15% stretch (Fig. 1B). KT is applied from below the patella to the distal femur with an approximate 10% to 15% stretch in both upward directions (Fig. 1C). KT is applied from above the patella to the proximal tibia with an approximate 10% to 15% stretch in both downward directions (Fig. 1D).[12] Each testing session consisted the following actions: application (or not) of KT from below the patella to the quadriceps and proximal tibia, assessment of walking ability, dynamic balance ability, and pain severity.
Figure 1.

Application of kinesiology taping.
2.3. Outcome measurements
This study utilized the visual analogue scale (VAS) to assess knee pain during resting and walking phases in 2 conditions (KT and non-KT). Knee pain during the resting state was assessed in the standing position before walking, and pain during gait was assessed immediately after walking. VAS is a scale for assessing pain, ranging from 1 to 10 points (0 points with no pain at all, 10 points with maximum pain). The minimal clinically important difference (MCID) of VAS was reported as 1.2 regardless of the degree of pain.[13]
Walking ability was assessed using a 10-m walking test (10MWT). The 10MWT is a measure of one's walking ability with an intra-rater and inter-rater reliability correlation coefficient of r = 0.95 to 0.96.[14] The 10MWT measured the time required for the participant to walk 10 m on a course that was a total distance of 14 m. Tape, at 2 and 12 m, indicated the start and end of the 10-m walking distance. The first and last 2 m of the course were used for acceleration and deceleration and were not timed. Participants were asked to stand at the 2-m tape line ahead of the 10-m line and then walk at a comfortable pace to the 12-m tape line beyond the 10-m line. The MCID of 10MWT was estimated as 0.05 m/s in older adults.[15]
Dynamic balance ability was assessed using a timed up and go test (TUG). TUG is a simple test that can quickly measure mobility and balance with an intra-rater and inter-rater reliability correlation coefficient of r = 0.98 to 0.99.[16] TUG measured the time that the subject took to rise from a 46-cm height armchair, walk 3 m, turn around as fast as possible in the direction of the affected side, walk back to the chair, and sit down. Participants were also asked to rise from the chair with a “start” command, walk along the floor line marked 3-m long, turn around on the affected side, and walk back to the chair at a regular speed and sit down. The MCID of TUG for a range of measure in patients with knee OA was estimated as 1.10 seconds.[17]
2.4. Data analysis
We compared differences in the mean values for KT gait and non-KT gait in participants using a Wilcoxon singed rank test. We used the SPSS software (ver. 18.0 for Windows; SPSS, Chicago, IL). Statistical significance was set at P < .05.
3. Results
3.1. General characteristics of the patient
A total of 10 participants participated in the study, and there was no dropout. Therefore, data from these 10 patients were analyzed. The general characteristics of the subjects are shown in Table 2. The flowchart of the study is shown in Fig. 2.
Table 2.
Demographic characteristics of the subjects.
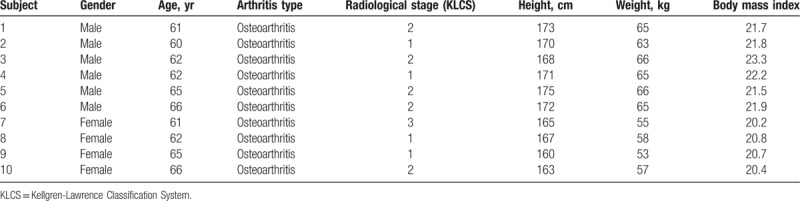
Figure 2.
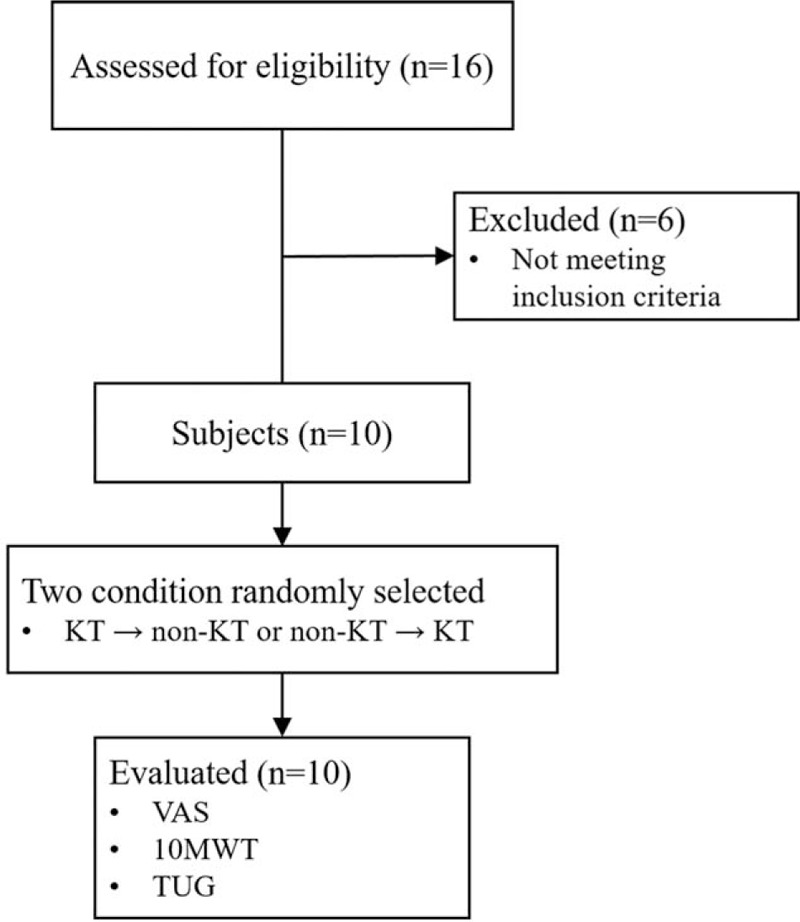
Flow chart of the study.
3.2. Pain evaluation
With respect to the evaluation of pain, the KT condition showed a significant decrease in the VAS score during gait as compared with the non-KT condition (6.40 ± 0.51 vs 5.40 ± 0.69, change: 1.00 ± 0.66, P = .008). On the other hand, there was no significant difference between the 2 conditions during resting (4.20 ± 0.63 vs 4.00 ± 0.47, change: 0.20 ± 0.42, P = .157) (Fig. 3, Table 3).
Figure 3.
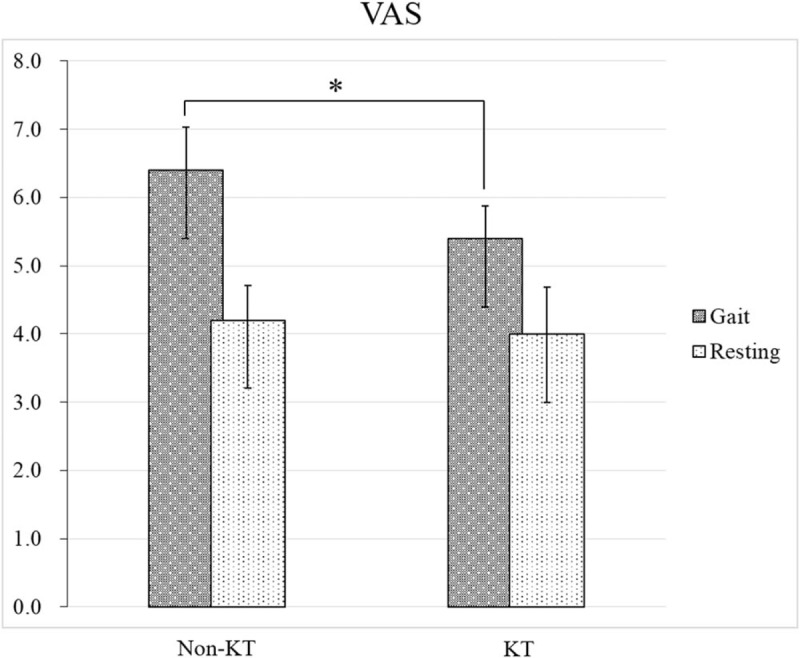
Knee pain evaluation. VAS = visual analog scale.
Table 3.
Pain evaluation of 2 conditions.

3.3. Gait and balance evaluation
In the evaluation of gait ability, the KT condition showed a statistically significant decrease in the 10MWT score when compared with the non-KT condition (10.46 ± 0.82 vs 9.13 ± 0.96, change: 1.32 ± 0.40, P = .005). In terms of balance ability, the KT condition showed a statistically significant decrease in the TUG score as compared with the non-KT condition (11.69 ± 1.23 vs 10.24 ± 1.01, change: 1.44 ± 0.72, P = .005) (Fig. 4, Table 4).
Figure 4.
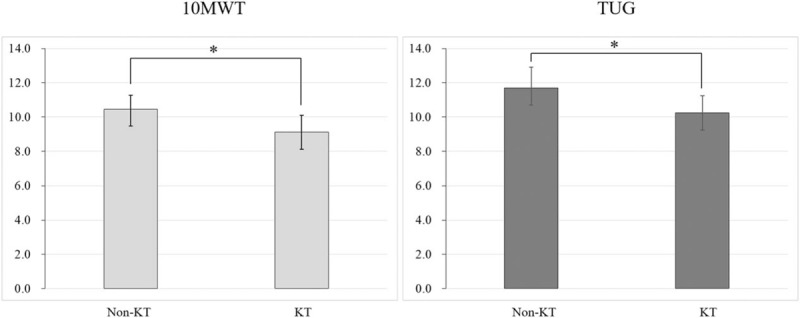
Gait and balance evaluation, 10MWT = 10-m walking test, TUG = timed up and go test.
Table 4.
Gait and balance evaluation of 2 conditions.

3.4. Side effect according to KT
In this study, no side effects owing to KT were reported specifically. However, 2 of the 10 patients reported discomfort after removing KT.
4. Discussion
This study investigated the effect of KT on the pain and gait function in the older adults with knee OA. Knee pain was measured using VAS during resting and gait conditions. The results of this study show that the use of KT is effective in decreasing knee pain in older adults with knee OA during walking. Previous studies have reported that KT has an immediate effect in relieving knee pain in knee OA patients.[18–20] In particular, these patients experience more pain during walking than in the resting condition; this is called movement-evoked pain.[13] The reduction of movement-evoked pain with KT can be explained by the following reasons. Elasticity of the tape and its application under tension leads to a mobilization of the skin during movement and improves blood and lymph circulation.[20,21] Decrease in pain with the application of the KT is likely due to the stimulation of low-threshold cutaneous mechanoreceptors, located in the joints, muscles, tendons, and skin.[12,22] Stimulation of these mechanoreceptors activates large diameter fibers (e.g., A-beta fibers), which reduces pain transduction along the small nociceptive fibers, namely the C and A-delta fibers, via activation of inhibitory interneurons.[23,24] This mechanism is believed to directly influence pain perception.
This study also investigated the effect of KT on walking. As a result, KT showed a significant influence on the gait function (e.g., gait speed, balance) of the older adults with knee OA, suggesting that KT had a positive effect on gait function. Knee OA, is one of the main causes of pain among the older adults while walking. Because knee OA causes knee pain and discomfort, it causes instability and fear during gait. In this study, we evaluated the reduction in pain using VAS, which showed a significant decrease in knee pain during gait. This means that the patients walked with less knee pain, fear, or discomfort as compared with that in the non-KT condition. Therefore, this may have had a positive effect on gait speed or stability.
Another reason is that KT supports the knee joint to provide stability and helps activate the associated muscles and improves the range of motion. KT is hypothesized to facilitate a small, immediate increase in muscle strength by producing a concentric pull on the fascia, which may stimulate increased muscle concentration.[25] In this study, KT was designed to increase the stability of the joint by reinforcing the lateral and medial collateral ligaments around the femoral patella of the knee joint. It is presumed that this supports the stability of the joint and positively influences mobility parameters such as strength and range of motion. Previous studies have reported that KT not only increases the stability of joints and soft tissues, but also has a temporary effect in increasing muscle activation or strength and range of motion,[4,24] which supports the results of this study.
This study had several limitations. First, it is difficult to generalize the results of this study, because the sample size was small. Second, this study only confirmed the immediate effect of KT on pain and gait function; thus, determining the long-term effect is not possible for pain and gait function and sustained effects on changes or benefits such as swelling, joint movement, and muscle activation. Third, this study evaluated the pain and gait ability during KT and non-KT conditions only; thus, the possibility of placebo effect cannot be ruled out.
5. Conclusion
This study confirmed that KT reduces the knee pain during walking in among the older adults with knee OA and is a useful method for improving walking ability. Therefore, we recommend KT as an option applicable to the older adult with knee OA.
Author contributions
Conceptualization: Jung-Hoon Lee.
Formal analysis: Na-Kyoung Hwang.
Funding acquisition: Young-Jin Jung, Gihyoun Lee.
Investigation: Sang-Hoon Lee, Jung-Hoon Lee.
Methodology: Ji-Su Park, Jung-Hoon Lee.
Project administration: Young-Jin Jung, Gihyoun Lee.
Supervision: Young-Jin Jung, Gihyoun Lee.
Writing – original draft: Na-Kyoung Hwang.
Writing – review & editing: Ji-Su Park, Taehyung Yoon, Sang-Hoon Lee.
Footnotes
Abbreviations: 10MWT = 10-m walking test, KT = kinesiology taping, OA = osteoarthritis, TUG = timed up and go test, VAS = visual analog scale.
How to cite this article: Park JS, Yoon T, Lee SH, Na-Kyung H, Jung-Hoon L, Jung YJ, Lee G. Immediate effects of kinesiology tape on the pain and gait function in older adults with knee osteoarthritis. Medicine. 2019;98:45(e17880).
Y-JJ and GL are co-corresponding authors and contributed equally to this work with GL, and Y-JJ.
This work was supported by Dongseo University, “Dongseo Cluster Project” Research Fund of 2019 (DSU-2019002).
The authors have no conflicts of interest to disclose.
References
- [1].McDonough CM, Jette AM. The contribution of osteoarthritis to functional limitations and disability. Clin Geriatr Med 2010;26:387–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Arnold CM, Faulkner RA. The effect of aquatic exercise and education on lowering fall risk in older adults with hip osteoarthritis. J Aging Phys Act 2010;18:245–60. [DOI] [PubMed] [Google Scholar]
- [3].Anandkumar S, Sudarshan S, Nagpal P. Efficacy of kinesio taping on isokinetic quadriceps torque in knee osteoarthritis: a double blinded randomized controlled study. Physiother Theory Pract 2014;30:375–83. [DOI] [PubMed] [Google Scholar]
- [4].Warden SJ, Hinman RS, Watson MA, Jr, et al. Patellar taping and bracing for the treatment of chronic knee pain: a systematic review and meta-analysis. Arthritis Rheum 2008;59:73–83. [DOI] [PubMed] [Google Scholar]
- [5].Serra MV, Vieira ER, Brunt D, et al. Kinesio taping effects on knee extension force among soccer players. Braz J Phys Ther 2015;19:152–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Hinman RS, Crossley KM, McConnell J, et al. Efficacy of knee tape in the management of osteoarthritis of the knee: blinded randomised controlled trial. BMJ 2003;327:135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Krustev E, Reid A, McDougall JJ. Tapping into the endocannabinoid system to ameliorate acute inflammatory flares and associated pain in mouse knee joints. Arthritis Res Ther 2014;16:437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Campolo M, Babu J, Dmochowska K, et al. A comparison of two taping techniques (kinesio and mcconnell) and their effect on anterior knee pain during functional activities. Int J Sports Phys Ther 2013;8:105–10. [PMC free article] [PubMed] [Google Scholar]
- [9].Crossley KM, Marino GP, Macilquham MD, et al. Can patellar tape reduce the patellar malalignment and pain associated with patellofemoral osteoarthritis? Arthritis Rheum 2009;61:1719–25. [DOI] [PubMed] [Google Scholar]
- [10].Alexander CM, McMullan M, Harrison PJ. What is the effect of taping along or across a muscle on motoneurone excitability? A study using triceps surae. Man Ther 2008;13:57–62. [DOI] [PubMed] [Google Scholar]
- [11].Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis 1957;16:494–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Lee JH, Choi SW. Balance Taping: Clinical Application of Elastic Therapeutic Tape for Musculoskeletal Disorders. WE TAPE, Paju; 2016. [Google Scholar]
- [13].Kelly AM. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J 2001;18:205–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Van Loo MA, Moseley AM, Bosman JM, et al. Test-re-test reliability of walking speed, step length and step width measurement after traumatic brain injury: a pilot study. Brain Inj 2004;18:1041–8. [DOI] [PubMed] [Google Scholar]
- [15].Rehab measures [homepage on the Internet]. Chicago: Rehabilitation Measures Database web site. Available at: http://www.rehabmeasures.org/Lists/RehabMeasures/PrintView.aspx?ID=901 Accessed August 15, 2019. [Google Scholar]
- [16].Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142–8. [DOI] [PubMed] [Google Scholar]
- [17].Alghadir A, Anwer S, Brismee JM. The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1-3 knee osteoarthritis. BMC Musculoskelet Disord 2015;16:174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Cho HY, Kim EH, Kim J, et al. Kinesio taping improves pain, range of motion, and proprioception in older patients with knee osteoarthritis: a randomized controlled trial. Am J Phys Med Rehabil 2015;94:192–200. [DOI] [PubMed] [Google Scholar]
- [19].Lu Z, Li X, Chen R, et al. Kinesio taping improves pain and function in patients with knee osteoarthritis: a meta-analysis of randomized controlled trials. Int J Surg 2018;59:27–35. [DOI] [PubMed] [Google Scholar]
- [20].Rahlf AL, Braumann KM, Zech A. Kinesio taping improves perceptions of pain and function of patients with knee osteoarthritis. A randomized, controlled trial. J Sport Rehabil 2019;28:481–7. [DOI] [PubMed] [Google Scholar]
- [21].Kase K, Wallis J, Kase T. Clinical Therapeutic Applications of the Kinesio Taping Methods. 4th edTokyo: Kinesio Taping Association; 2003. [Google Scholar]
- [22].Konishi Y. Tactile stimulation with kinesiology tape alleviates muscle weakness attributable to attenuation of Ia afferents. J Sci Med Sport 2013;16:45–8. [DOI] [PubMed] [Google Scholar]
- [23].Bravi R, Quarta E, Cohen EJ, et al. A little elastic for a better performance: kinesiotaping of the motor effector modulates neural mechanisms for rhythmic movements. Front Syst Neurosci 2014;25:181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Martini FH. Fundamentals of Anatomy and Physiology. 4th ed.United States of America: Prentice Hall; 2004. [Google Scholar]
- [25].Kaya Mutlu E, Mustafaoglu R, Birinci T, et al. Does kinesio taping of the knee improve pain and functionality in patients with knee osteoarthritis? A randomized controlled clinical trial. Am J Phys Med Rehabil 2017;96:25–33. [DOI] [PubMed] [Google Scholar]