Abstract
Objective The objective of this paper was to identify safety parameters in the posterior surgical approach of the scapula through a cross-sectional cadaver study.
Methods Thirteen cadaver shoulders with no history of surgery or prior musculoskeletal dysfunction, with mean age, weight, and height of 70.1 years, 61.5 kg, and 1.64 m, respectively, were dissected. The anatomic landmark of the studied pathway (infraglenoid tubercle) and its distance to the axillary and suprascapular nerves were measured.
Results The mean distance between the infraglenoid tubercle (IT) and the axillary nerve (AN) was 23.8 mm, and the mean distance from the IT to the suprascapular nerve (SN) was 33.2 mm.
Conclusion The posterior approach may be considered safe through the interval between the infraspinatus and teres minor. However, caution should be taken during muscle spacing because of the short distance between the fracture site and the location of the SN and AN. These precautions help to avoid major postoperative complications.
Keywords: scapula/anatomy & histology, scapula/surgery, shoulder
Introduction
The incidence of scapula fractures has increased in orthopedic practice and it is usually associated with trauma of great energy, affecting mainly young adults (35–45 years old) victims of car accidents or falls from great heights. 1 2 3 The indications for surgical treatment of glenoid neck fractures are: when they are deviated with a translation greater than one centimeter or when the glenopolar angle is less than 20° (normal 30∘–45∘). 4 The objective of the surgery is to restore the length, alignment, and rotation of the scapula, leading to the improvement of the functional results. 5
Extended scapular approaches provide excellent posterior visualization, useful accessing of the body, spine, and neck of the glenoid. 6 The posterior approach described by Judet, which implies the extensive dissection of the infraspinatus muscle, has been widely used in the treatment of scapular fractures but is being replaced by less invasive variations due to the high morbidity and risk of neurovascular lesions. 5
In the posterior approach, it is important to identify and protect the suprascapular nerve (SN), which emanates from the spinoglenoid notch to innervate the infraspinatus muscle in its fossa (traction on this nerve can cause weakness of the rotator cuff and should be avoided). 6
Despite the variations, the less invasive approaches usually use the interval between the infraspinatus muscle (SN) and the teres minor muscle (axillary nerve—AN) to access the lateral angle of the scapula. With abduction of the shoulder at 60° to 90°, access is facilitated due to the superior detachment of the fibers from the posterior deltoid; however, an excessive abduction can strain the AN and put it at risk during access and bring it closer to the surgical field. 7 8 9 10
The objective of this study is to evaluate the mean distance and proximity of the AN and SN to the infraglenoid tubercle (IT) in order to quantify a safety zone so as to assist the surgeon during surgical access to the scapular neck and body.
Methods
The cadaver study was performed at the Verification of Death Service, from the dissection of a total sample of 13 shoulders from 13 corpses, random laterality, in order to identify the periscapular neurovascular structures (AN and SN) and obtain measurements of their distances to the IT. Only one dissection per corpse was authorized.
The definition of the IT as a bony landmark was determined by its fixed position in relation to the bone structures and by being the topography in which the SN becomes directly visible in the surgical path under discussion.
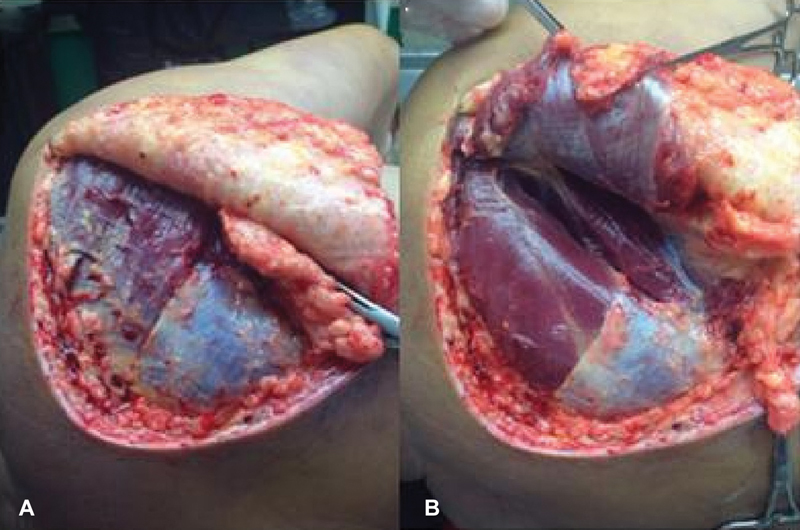
The approach developed was a modified version of Judet's, which proved to be an excellent option for the fixation of scapular fractures, since it provides optimal exposure without injuring the scapular musculature as it does not involve disengagement of its fibers. 5 Each cadaver was positioned in lateral decubitus according to the side to be operated, with the ipsilateral upper limb held initially along the body. An L-shaped incision was made on the skin and subcutaneous tissue, beginning at the lateral border of the acromion to the superomedial angle of the scapula, then curved towards the lower angle, over the medial margin. An exposure plan was developed between the more subcutaneous skin flap and the scapular musculature. For the exposure of the structures, we opted for disinsertion, and for the folding of the posterior portion of the deltoid muscle ( Fig. 1A ). The interval between the infraspinatus and the teres minor muscles was developed so that we could demarcate, with a pin, a fixed and immutable reference point: the inferior tubercle of the glenoid— easily palpable at that location ( Fig. 1B ).
Fig. 1.
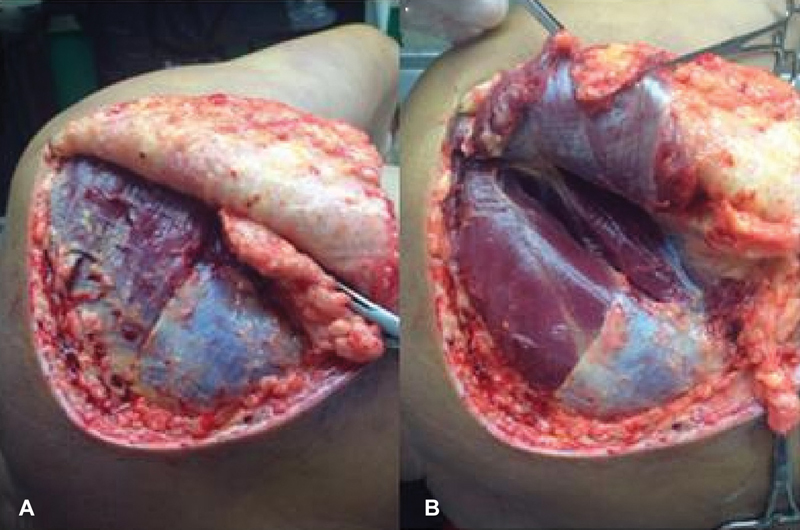
L-shaped incision on the medial border of the scapula and subcutaneous flap exposing the musculature (A); folding of the posterior portion of the deltoid muscle and divulsion of the interval between infraspinatus and teres major muscle (B).
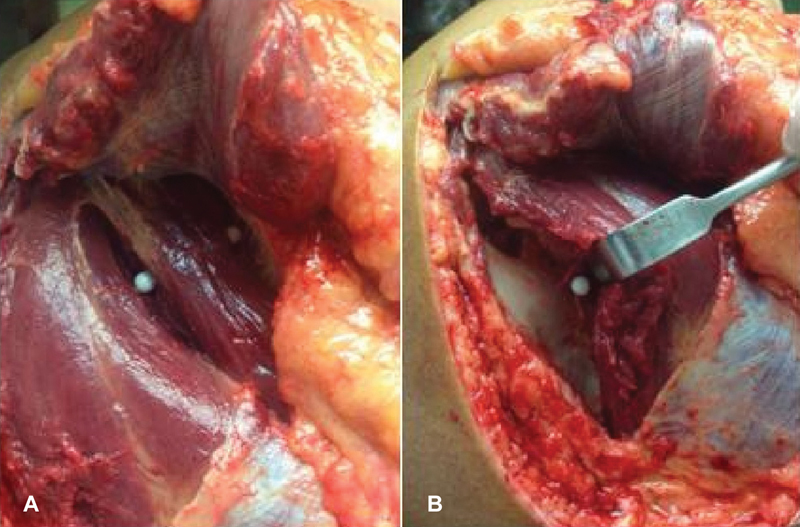
Through careful dissection of the anterior region of the infraspinatus and teres minor muscles, their respective nerves were identified: suprascapular and axillary branch, and then demarcated with pins at the point of their penetration into the belly of each muscle ( Fig. 2A e 2B ).
Fig. 2.
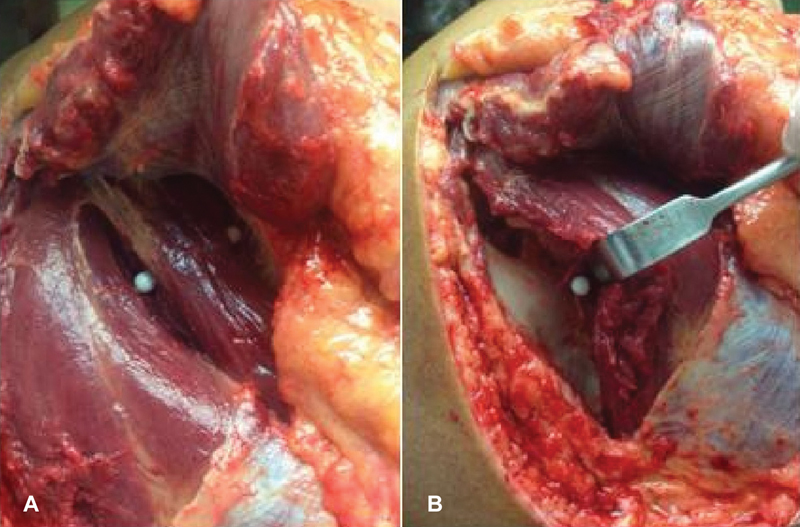
Pin marking on the infraglenoid tubercle in the intermuscular spacing and on the most distal portion of the axillary nerve branch to the teres minor muscle (A); marking the suprascapular nerve over its most distal dissected portion (B).
Measurements were made using a universal caliper between the defined static reference point— the IT—and the pins placed at the most distal points of each nerve. The distances were determined in millimeters: IT to SN and IT to AN.
In addition to the specific data of the measurements, the data of the corpses studied were collected: gender, age, weight, height.
Exclusion criteria: specimens showing signs of injury or previous shoulder surgeries or previous diseases of the shoulder girdle.
Results
The parameters were evaluated in 13 shoulders of 13 fresh cadavers. Among these, eight were male and five were female. The mean age was 70.1 years old (from 48–98).
The mean weight of the studied corpses was 61.5 kg, while the mean height was 1.64 m, ranging from 1.52 to 1.75 m. The mean distance from the IT to the AN was 23.8 mm, ranging from 17 to 28 mm, and the standard deviation (SD) was 7.6 mm. The mean distance from the IT to the SN was 33.2 mm, ranging from 17 to 43 mm. The SD was 23.8 mm, ranging from 17 to 32 mm.
Discussion
With the increased incidence of scapular fractures due to high energy trauma, it is natural that there is also an increase in the severity of these fractures and, thus, the probability of surgical treatment.
Barbieri et al 11 reported good results in 106 patients with conservatively treated scapula fractures and suggest that surgical cases are the minority because this is, among other causes, a difficult approach and with risks of muscular injuries.
Even with the development of new access techniques, as seen in the works of Jerosch et al, 8 Wirth et al, 9 and Pizanis et al, 12 who reported a low incidence of complications, the surgical approach of the scapula may jeopardize some neurovascular structures, such as the AN and the SN, with injuries occurring in up to 2 to 3% of cases in the postoperative period. Excessive traction of these nerves by detachment of tissues during access may cause weakening of the rotator cuff. 6
Jerosch et al developed a posterior subdeltoid access and revealed a mean distance of 21.98 mm up to the AN but they did not establish in their work the reference points used. 8
Longo et al 13 cited a 6% rate of SN injury during surgeries for shoulder instability and noted that the course of this nerve is altered in cases of rupture of the rotator cuff. During their study, the distance between the posterior border of the glenoid and the SN was measured in the spinoglenoid notch with mean values of 12 mm in internal rotation and 19 mm in external rotation of the shoulder.
Wirth et al 9 studied posterior access through division of the deltoid muscle and advised caution (during dissection) with the SN, which may be located about 15 mm medial to the edge of the posterior glenoid. Ball et al, 14 in a study of the anatomy of the posterior branch of the AN have described that the branch to the teres minor muscle arises immediately at the inferior border of the glenoid next to the origin of the long head of the triceps and measures about 11 to 25 mm (mean of 18 mm) until it enters the muscle.
We considered that, in the Ball study, the origin of the branch of the AN for the teres minor muscle is the same of the parameter we used for the measurement, which is the IT. Thus, in comparison to our study, we reached slightly higher values with a mean of 23.8 mm for the distance between the IT and the AN.
Shaffer et al, 15 during electroneuromyographic assessment of the SN during posterior access with horizontal division of the infraspinatus muscle, obtained a mean value of 22.5 mm distance between the posterior border of the glenoid to the nearest branch that crossed that muscular division. This measurement has the parameters very close to those of our study referring to the same nerve, but presents values considerably lower than those found in ours, whose mean value was 33.2 mm for the distance between the IT to the SN, probably due to the difference in bone parameter and muscle division had been randomized in the Shaffer study.
It is important to emphasize that in our study the mean age of the patients was 70.1 years and the mean weight of 60.5 kg. This reflects the profile of the elderly specimens studied at a Verification of Death Service, with hypotrophic muscle characteristics expected for the studied age group, and their possible influence on the distances between established parameters. We assume that in younger and more active individuals, the values may be relatively higher due to a greater muscular trophism. However, due to the small number of specimens studied, we are unable to prove such an assertion.
Conclusion
The surgical approach for the treatment of glenoid neck fractures is considered safe through the interval between the infraspinatus and teres minor muscles; however, much attention and caution should be exercised during muscle spacing due to the short distance between the fracture site and the location of the SN and AN, thus avoiding major postoperative complications.
Conflitos de Interesse Os autores declaram não haver conflitos de interesse.
Trabalho desenvolvido no Grupo de Ombro e Cotovelo, Hospital do Servidor Público Estadual de São Paulo, São Paulo, SP, Brasil. Publicado Originalmente por Elsevier Editora Ltda.
Study developed at the Group of Shoulder and Elbow, Hospital do Servidor Público Estadual de São Paulo, São Paulo, SP, Brazil. Published Originally by Elsevier Editora Ltda.
Referências
- 1.Ada J R, Miller M E. Scapular fractures. Analysis of 113 cases. Clin Orthop Relat Res. 1991;(269):174–180. [PubMed] [Google Scholar]
- 2.McGahan J P, Rab G T, Dublin A. Fractures of the scapula. J Trauma. 1980;20(10):880–883. doi: 10.1097/00005373-198010000-00011. [DOI] [PubMed] [Google Scholar]
- 3.Thompson D A, Flynn T C, Miller P W, Fischer R P. The significance of scapular fractures. J Trauma. 1985;25(10):974–977. doi: 10.1097/00005373-198510000-00008. [DOI] [PubMed] [Google Scholar]
- 4.Geel C W. New York: Thieme: Stuttgart; 2000. Scapula and clavicle; pp. 261–2. [Google Scholar]
- 5.Jones C B, Cornelius J P, Sietsema D L, Ringler J R, Endres T J. Modified Judet approach and minifragment fixation of scapular body and glenoid neck fractures. J Orthop Trauma. 2009;23(08):558–564. doi: 10.1097/BOT.0b013e3181a18216. [DOI] [PubMed] [Google Scholar]
- 6.Cole P A, Dubin J R, Freeman G.Operative techniques in the management of scapular fractures Orthop Clin North Am 20134403331–343., viii [DOI] [PubMed] [Google Scholar]
- 7.Salassa T E, Hill B W, Cole P A. Quantitative comparison of exposure for the posterior Judet approach to the scapula with and without deltoid takedown. J Shoulder Elbow Surg. 2014;23(11):1747–1752. doi: 10.1016/j.jse.2014.02.025. [DOI] [PubMed] [Google Scholar]
- 8.Jerosch J, Greig M, Peuker E T, Filler T J. The posterior subdeltoid approach: a modified access to the posterior glenohumeral joint. J Shoulder Elbow Surg. 2001;10(03):265–268. doi: 10.1067/mse.2001.112885. [DOI] [PubMed] [Google Scholar]
- 9.Wirth M A, Butters K P, Rockwood C A., Jr The posterior deltoid-splitting approach to the shoulder. Clin Orthop Relat Res. 1993;(296):92–98. [PubMed] [Google Scholar]
- 10.van Noort A, van Loon C J, Rijnberg W J. Limited posterior approach for internal fixation of a glenoid fracture. Arch Orthop Trauma Surg. 2004;124(02):140–144. doi: 10.1007/s00402-003-0604-y. [DOI] [PubMed] [Google Scholar]
- 11.Barbieri C H, Mazzer N, Mendonça F H, Damasceno L HF. Fraturas da escápula. Rev Bras Ortop. 2001;36(07):245–254. [Google Scholar]
- 12.Pizanis A, Tosounidis G, Braun C, Pohlemann T, Wirbel R J. The posterior two-portal approach for reconstruction of scapula fractures: results of 39 patients. Injury. 2013;44(11):1630–1635. doi: 10.1016/j.injury.2013.07.020. [DOI] [PubMed] [Google Scholar]
- 13.Longo U G, Forriol F, Loppini M et al. The safe zone for avoiding suprascapular nerve injury in bone block procedures for shoulder instability. A cadaveric study. Knee Surg Sports Traumatol Arthrosc. 2015;23(05):1506–1510. doi: 10.1007/s00167-014-2900-1. [DOI] [PubMed] [Google Scholar]
- 14.Ball C M, Steger T, Galatz L M, Yamaguchi K. The posterior branch of the axillary nerve: an anatomic study. J Bone Joint Surg Am. 2003;85(08):1497–1501. doi: 10.2106/00004623-200308000-00010. [DOI] [PubMed] [Google Scholar]
- 15.Shaffer B S, Conway J, Jobe F W, Kvitne R S, Tibone J E. Infraspinatus muscle-splitting incision in posterior shoulder surgery. An anatomic and electromyographic study. Am J Sports Med. 1994;22(01):113–120. doi: 10.1177/036354659402200118. [DOI] [PubMed] [Google Scholar]