

ABSTRACT
Women's empowerment has gained attention as critical for child nutrition during the first 1000 days of life. However, the ways in which various women's empowerment measures are applied and the evidence for how they are differentially related to child nutrition is unclear. In this systematic review, therefore, we 1) systematically parse the many ways in which women's empowerment has been quantitatively measured in the context of child nutrition through the use of a theoretically driven application of dimensions and domains of empowerment; 2) summarize evidence for each of the various pathways between women's empowerment and child nutrition, based on dimensions and domains of empowerment; and 3) offer suggestions for future research to better articulate the relationship between women's empowerment and child nutrition. A search of evidence yielded 62 quantitative studies that used 200 unique indicators of women's empowerment, tested in 1316 associations with various child nutrition outcomes. Despite the large number of unique indicators, indicators for time resource allocation and reproductive decisions and indicators for men's engagement in child care and nutrition, all pertinent to child nutrition, were missing. Overall, the findings indicated an inconclusive relationship between women's empowerment and child nutrition: 379 out of 461 (82% weighted) and 217 out of 258 (84% weighted) associations found with stunting and wasting outcomes, respectively, were not significant. The current lack of evidence is likely not due to the absence of an underlying relationship between women's empowerment and child nutrition, but rather limitations in study design. Future research should carefully select women's empowerment indicators in context-specific ways, aggregate them meaningfully, and use a longitudinal study design to conduct pathway and lifecycle analysis in appropriate populations to clarify the relationship between women's empowerment and child nutrition.
Keywords: gender equity, systematic review, nutrition-sensitive, empowerment, infant and young child feeding
Introduction
Women's empowerment, the expansion in women's ability to make strategic life choices (1), is of intrinsic value. As such, efforts to improve the status of women globally are of first-order importance. Additionally, women's empowerment is of instrumental value; it is one means by which societies can improve other important welfare outcomes, e.g., child nutrition, particularly in the first 1000 days of life. Consistent with this argument, the UN's Scaling-Up Nutrition initiative emphasizes the importance of empowering women and girls in national efforts to scale-up nutrition (2). Moreover, nutrition-sensitive interventions aimed at improving the position of women have the potential to be a powerful means of improving child nutrition outcomes (3).
Three peer-reviewed reviews, published in 2015 and 2016, explored aspects of the relationship between quantitative measures of women's empowerment and child nutrition and contributed significantly to knowledge in this arena. Carlson et al. (4) were the first to look at this connection and analyze women's autonomy, one specific dimension of empowerment, and child nutritional status. Cunningham et al. (5) focused on the association between women's empowerment and child nutrition outcomes in South Asia. Pratley (6) provided a more comprehensive summary of the role of women's empowerment on various maternal and child health outcomes, including nutritional status in low- and middle-income countries. All 3 reviews concluded that women's empowerment was generally associated with child nutrition, but they also pointed out difficulties in interpreting results because of the various indicators and categorizations of empowerment. Much has been written on the role of women's empowerment since these reviews appeared.
In this article, we update the state of the evidence and advance prior analyses on this topic in several ways by following several suggestions from the previous reviews to classify the various women's empowerment measures and how they differentially relate to child nutrition (4) and to elucidate how the relationship between women's empowerment and child nutrition differs by regions and age of participants (4–6). Specifically, we had the following 3 objectives: 1) to systematically parse the many ways that women's empowerment has been measured in the context of child nutrition through the use of a theoretically driven application of dimensions and domains of empowerment; 2) to summarize the quantitative evidence for each of the various pathways between women's empowerment and child nutrition, based on dimensions and domains of empowerment; and 3) to offer suggestions for future research to better articulate the relationship between women's empowerment and child nutrition.
Women's Empowerment and Its Indicators
Although many definitions of women's empowerment have been proposed, there is currently no one standardized, operable definition of women's empowerment. However, most of those definitions can be summarized as the process by which a woman achieves agency. Agency is “what a person is free to do and achieve in pursuit of whatever goals or values he or she regards as important” (7). This decision-making sometimes happens through navigating relational and societal dynamics through processes such as negotiation and manipulation (1, 8). The second concept in these definitions is process, which emphasizes a change from one state (gender inequity) to another (gender equity) over time (9). Various works on women's empowerment emphasize women's active involvement in this process and the related psychological change (e.g., gain in self-efficacy) that occurs (1, 9–12).
Categorizing women's empowerment indicators
Such a conceptualization allows for a wide array of operationalization for women's empowerment. This partly explains the difficulty in measuring women's empowerment. To begin to understand the typology of various women's empowerment indicators, Kabeer (1) proposed categorizing indicators of women's empowerment into 3 dimensions along the process of empowerment: resources, agency, and achievements. “Resources,” also called “preconditions” (1) or “opportunity structures” (13), are the material, human, and social resources and institutional environments that would allow one to make a decision (9). Examples of common indicators of women's empowerment that would fall within this dimension include women's education, social capital, and asset ownership. “Agency” captures critical thinking skills and the ability to make independent decisions (14, 15). Typical measures describing this dimension evaluate whether women can make various types of decisions. Lastly, “achievements” are the manifestations of the exercise of agency. Measures of achievements might include increased labor market participation, intolerance of domestic violence, and parental time available for child care. Although this dimension classification might indicate that women's empowerment is a linear process, it is essential to remember it instead happens through a complex interaction among these dimensions and is context specific (1).
Indicators of these 3 dimensions of empowerment can also be found for various domains of a woman's life. Empowerment in one domain does not ensure empowerment in another (1, 7, 9, 11) and therefore empowerment in one domain might be easier to attain than in other domains (9). For example, a woman may not be empowered to make decisions about her reproductive health but may be empowered at the national legal or political level because she has the right to vote (11, 16). Moreover, the importance of each domain of empowerment is context specific (17, 18). Mobility agency, i.e., freedom to visit the market alone, is a standard indicator of agency in South Asia but does not denote empowerment in most settings in many parts of East Africa, where it is expected that women will go to the market (19–25).
Determining the appropriate level of aggregation of a woman's empowerment domain, however, is a challenge. In analyses, researchers need to be sure that their categorization of a domain takes all relevant indicators into account (9, 11, 26, 27), but avoids masking differential contributions of specific indicators of empowerment (28). Various works have proposed categorization of these domains. Ibrahim and Alkire (11) proposed sexuality, marriage, childbearing, and the exercise of reproductive rights; making decisions in the family; participation in labor, land, and financial markets; and engagement with collective action and politics. Malhotra et al. (9) categorized these domains as decision making, sociofamilial, and legal, whereas others (23, 29–31) group them as control of household resources and assets, decision-making capabilities, position in society, and knowledge level, among many others.
Links between women's empowerment and child nutrition
Due to the lack of consensus on how one should categorize the various women's empowerment indicators, we discuss them here based on how they could affect child nutrition. Our understanding of the relationship between women's empowerment and child nutrition (Figure 1) is heavily based on the UNICEF framework for child nutrition (32), especially as modified by Engle et al. in their work on the concepts and measurements of care in nutrition (29), and on the various works on intrahousehold resource allocation (31, 33, 34). Our conceptual framework also emphasizes that women's levels of power can vary over time and across domains, and empowerment in one domain could differentially affect a child's nutrition. Therefore, it is important to consider the stage of life cycle involved in an analysis.
FIGURE 1.

Proposed framework between women’s empowerment and child nutrition based on the UNICEF framework for child nutrition: women’s empowerment impacts whether a household can access resources (A), whether those resources are allocated towards children’s health and nutrition (B), and the amount of dependence in the household (C). Since domains of empowerment are distinct, change over time, and differentially impact child nutrition, it is important to consider stages of life cycle when analyzing this relationship.
The first group of indicators (group A) involve a woman's ability to access resources for her household such as those over a woman's mobility, access to information, or agency over agricultural decisions. Women with higher mobility, for example, might have easier access to various resources for her household, which might be good for child nutrition. A woman's ability to join groups in her village might lead her to participate in a lending and savings group, increasing the availability of cash for her household. Similarly, women having a more equal say in crop decision making is associated with higher levels of technical ability in farming (35) and better household food security (36, 37).
The second group of indicators (group B) involve allocation of household resources for child nutrition. Because most work on the relationship between women's empowerment and child nutrition is focused on this group of indicators, we broke them down into 4 subgroups. The first, and most commonly analyzed, subgroup is material resource allocation (e.g., money, food) (B1). Evidence shows that as women's decision-making power in resource allocation increases, more resources are allocated to child health and nutrition. Cash controlled by women is more likely to be used to purchase food (33, 38) and health care (39, 40) for children of the household than cash controlled by men, and this results in a higher positive influence on household-level calorie availability and health outcomes (41–47). Examples of indicators in this subgroup include women's roles in decision making about household income, food use, and on what to purchase.
Another subgroup concerns women having more say on the allocation of their and other household members’ time (B2). Women having less say about time allocation might lead to unequal task allocation within the household, which can lead to women compromising the amount of time they allot for child care and rest, especially during pregnancy, with detrimental impacts on child nutrition (29, 48). For example, Johnston et al. (49) found that the increased time women spent on agricultural labor might partly explain the lack of evidence of the impact of agriculture on child nutrition. Example indicators of this subgroup include parental time spent on child care or other household chores.
The next subgroup of indicators pertains to women's decision making about child care and child health (B3). The assumption is that women empowered to make decisions on this topic are better positioned to ensure prevention and treatment of their children's illnesses, which would be enacted through their decisions about material (B1) and time (B2) resource allocation. The interpretations of these indicators are less straightforward because scoring high in them could instead be due to assignment of child care as solely women's responsibilities in the community rather than an increase in women's control of resources to address their children's illnesses. Indicators in this subgroup include questions on who decides whether a child is breastfed or what to do when a child is sick.
The last subgroup of resource allocation indicators (B4) are about whether women can determine the activities (i.e., exercise, rest, socialization, health care) and material resources (i.e., good-quality food) that are optimal for their own health and nutrition status. Maternal nutritional status across the life course is crucial for child nutritional status at birth and reduces the risk of fetal and infant mortality, intrauterine growth retardation, low birth weight and premature birth, poor brain development, and risk of infection (50, 51). Postpartum, women's physical health also influences the ability to provide food and care for children (29). Maternal mental health is crucial for proper child feeding, hygiene, and health-seeking behaviors (52). For example, maternal depression has been shown to be associated with breastfeeding duration (53), child illness (52), impaired growth, slowed cognitive development, and child psychosocial health (54).
The last group of indicators (group C) are related to reproductive decisions. An increase in women's decision-making power in this topic is associated with increased contraceptive use (24, 55–58), which helps decrease high-risk pregnancies, i.e., those occurring among adolescents or due to insufficient birth intervals; both of which are associated with poor birth outcomes (59–64). High parity can also influence child nutrition through various mechanisms such as insufficient maternal nutrient stores for pregnancy, suboptimal breastfeeding related to subsequent pregnancy, and household resource competition (65).
There are three important ideas to keep in mind when considering these pathways. First is that all of these pathways rely on the assumption that there are sufficient available resources in the community (to be accessed, for indicator group A) and household (to be allocated, for indicator group B) in the first place (66). Secondly, most of these pathways also rely on the assumption that women make decisions that are optimal for child nutrition. This is where ensuring appropriate nutrition knowledge fits into this pathway. Currently, the evidence seems to indicate that women, when given the opportunity, make better decisions than men about the care and nutrition of children. We suggest this is due to the assignment of child care as a woman's task in many communities in the world. Lastly, it is important to note that all the pathways described above can also operate by engaging other individuals (e.g., husbands) within households in child care activities (67–71). For example, increasing available healthy foods for children in the household can be achieved by increasing women's ability to decide which food to buy or by men buying healthy foods. Similarly, improving the quality of child care can be achieved by men engaging in activities traditionally assigned to women, such as child care and household chores.
Methods
Search
The keywords “women,” “power,” “child,” “nutrition,” and their synonyms (Supplemental Table 1) were searched in PubMed, EconLit, SocIndex, CAB Abstracts, GenderWatch, POPLINE, Sociological Abstracts, and Web of Science. Searches were conducted twice: initially in August 2016 and an update in September 2017. All studies were downloaded into Mendeley, a reference management software. Duplicate references were eliminated. To ensure breadth, references of the included studies were hand searched and screened for inclusion.
Screening
A multistep screening process was conducted (Figure 2). Titles and abstracts of search results were screened by 5 reviewers (PG, SO, E Umuhire for the 2016 search results; C Benzaken, E Umuhire, A Beck for the 2017 search results). At the beginning of each round of screening, 10% of articles were screened by ≥2 reviewers. The team discussed and reconciled any discrepancies in the selection of documents before continuing with the screening process. A similar process was conducted for the screening of full texts.
FIGURE 2.
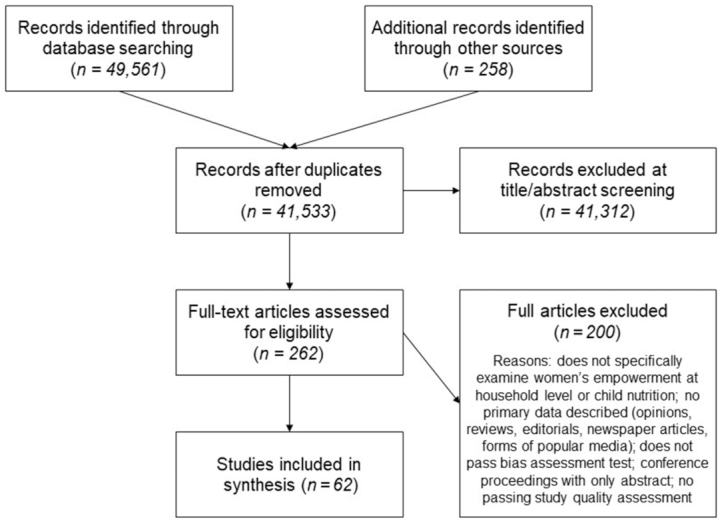
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of studies reviewed in this systematic review of the relationship between women's empowerment and child nutrition outcomes.
Eligibility criteria
Studies were excluded if they did not include women's empowerment as an exposure indicator of interest and child nutrition as the outcome indicator of interest. Studies that only looked at women's education, women's employment, and gender of household head were not included because they might affect child nutrition through various pathways other than decision making within a household. Child nutrition outcomes included various child anthropometry and infant and young child feeding indicators.
Both peer-reviewed and gray literature were included. Specifically, the following formats were included: journal articles, research studies, evaluations, dissertations, reports, and working papers. Conference proceedings without the full paper published online were excluded, as were opinions, reviews, editorials, newspaper articles, forms of popular media, and any other articles not presenting original research. We also excluded articles that only looked at women's empowerment measures at the national level such as the number of women in parliament or those that did not include quantitative analysis between women's empowerment and child nutrition. No restrictions were made regarding the language of publications, publication dates, study setting, or sample size.
Risk-of-bias assessment and quality appraisal
We performed 2 levels of risk-of-bias assessment and quality appraisal (see Supplemental Table 2). To assess the risk of bias, we used National Heart, Lung, and Blood Institute's study quality assessment tools for observational cohort and cross-sectional studies (72). Study quality was assessed by reviewers (MVS, SO, or C Benzaken) with the use of the form, and 20% of the documents were subjected to independent quality control by a second reviewer. Disagreements were resolved by discussion and, if necessary, by arbitration involving a third reviewer. Studies ranked “poor” were then excluded from the review. To further narrow down selection criteria among observational studies, a Childcare and Early Education Research Connections (CCEERC) quality score for quantitative observational studies was also assigned to each study (73). The CCEERC score ranges from −11 to 11; following CCEERC guidelines, all studies that scored 0 or a negative score on the scale were excluded from further review.
Analysis
Using a standardized table in Microsoft Excel, 3 reviewers (MVS, SO, J Risman) extracted and aggregated data on population characteristics (sample size, children's age, residence), study characteristics (study design, data source, study field of authors), control variables, and definitions of women's empowerment. For each association between women's empowerment and child nutrition, 2 reviewers (MVS, JR) recorded the indicator for women's empowerment, the indicator for child nutrition, effect size, and statistical significance. These associations were categorized as statistically significantly positive, statistically significantly negative, or statistically nonsignificant, where significance was defined at P < 0.05. Within each study, these associations were weighted based on the total number of associations presented. A greater number of associations presented in a study resulted in each individual association having a smaller weight. This is because the number of associations presented varied widely from one study to another.
The empowerment indicators were then categorized to the appropriate dimensions and groups. Indicators encompassing multiple domains were marked “multiple.” An example of one such indicator was the popular Women's Empowerment in Agriculture Index (28) which includes indicators on accessing resources for household (group membership, production decision) and material (income use decision), and time resource allocation (time use) in various dimensions. Another set of indicators that encompassed multiple domains contained questions regarding attitude towards domestic violence, as these tend to cover various situations. A question about whether a husband is justified in beating his wife if their child is sick falls under the child care subgroup of resource allocation (B3), whereas the same question for if she goes somewhere without asking is under the accessing resources group of indicators (A).
Child nutrition outcomes were defined as measures of child growth. They were reported as categorical variables (whether the child is stunted, wasted, or underweight) or continuous (height-for-age z score, weight-for-height z-score, and weight-for-age z score). Although we also extracted data on underweight children, interpretation of this nutritional status indicator was not clear, and therefore we only included these results in the Supplemental Material.
We also extracted data on 2 important proximate determinants of child nutritional status: child's diet and child's illness. For child's diet, we included infant and young child feeding indicators as defined by UNICEF (74). Breastfeeding behaviors included early initiation of breastfeeding, exclusive breastfeeding up to 6 mo of age, and duration of any breastfeeding. Complementary feeding behaviors included measures of dietary diversity, meal frequency, and the combination of the 2 as a measure for a minimally adequate diet. For indicators of child illness, we included any measures of child illness, child vaccination, and if the child received treatment when ill.
Furthermore, we present the minimum, maximum, mean, and median of the various associations found. This is to indicate a sense of the magnitude of these relationships and is not meant to be interpreted as the result of a meta-analysis because the absence of uniformity in empowerment indicators make meta-analyses impossible. Finally, we conducted these analyses stratified by age group of participating children (<2 y old compared with <5 y old), region of participants (South Asia compared with sub-Saharan Africa), whether a study controlled for pathway variables, data source (primary compared with secondary), and whether a study was a published journal article (compared with gray literature).
Results
Search results
The initial search yielded 41,533 studies; these were pared down to 262 studies after title and abstract screening. After full-text review, 62 studies were deemed eligible (75–136), 26 of which had not been included in the 3 previous reviews on this topic.
Study characteristics
Notable characteristics of the 62 studies included in this review are summarized in Table 1; detailed characteristics of each study are available as a supplement (Supplemental Table 3). We found many similarities between the included studies. Firstly, all studies were cross-sectional, with 3 studies collecting repeated cross-sectional data. Although no restrictions were made for languages, all 62 studies selected were in English. Two-thirds (68%) of studies were secondary analyses of available data sets, with 27% based on data from Demographic Health Surveys from various countries and 18% based on the Indian National Family and Health Survey. Most papers presented data from South Asia (56%) or sub-Saharan Africa (42%). Few studies included data for children aged <2 y (23%). Half (50%) of the studies controlled for what could be considered as a pathway variable between women's empowerment and child nutrition. For example, when looking at the relationship between women's decision making and height-for-age z score, Abate et al. (75) controlled for whether a child was receiving optimal feeding. Multiple studies controlled for maternal health (90, 94, 117).
TABLE 1.
Characteristics of studies that met inclusion criteria for assessment of the relationship between women's empowerment and child nutrition (n = 62 studies)1
| No. of studies | |
|---|---|
| Region | |
| South Asia | 35 |
| Sub-Saharan Africa | 26 |
| Latin America and the Caribbean | 9 |
| Middle East and North Africa | 2 |
| East Asia and Pacific | 2 |
| Residence | |
| Rural | 26 |
| Urban | 2 |
| Both | 34 |
| Maximum age of child, y | |
| 2 | 14 |
| >2 | 45 |
| Unclear | 3 |
| Study design | |
| Cross-sectional | 59 |
| Repeated cross-sectional | 3 |
| Data source | |
| Demographic and Health Surveys | 17 |
| Indian National Family Health Survey | 11 |
| Other secondary data sources | 14 |
| Baseline survey of interventions | 5 |
| Primary data collection | 16 |
| Year of publication | |
| 1996–1998 | 3 |
| 1999–2002 | 2 |
| 2003–2006 | 8 |
| 2007–2010 | 17 |
| 2011–2013 | 16 |
| 2014–2017 | 16 |
| Publication type | |
| Journal article | 50 |
| Gray literature | 12 |
| Controlling for pathway variables | 31 |
Regions were classified according to World Bank criteria (137). Some studies may have multiple sources.
Dimensions and domains of women's empowerment indicators
Across the 62 studies of women's empowerment, 200 unique indicators of empowerment were identified (Table 2; Supplemental Table 4). There was no predominantly used indicator—the most commonly used one was only used in 7 studies. This high number of unique indicators, however, tended to occupy similar dimensions and domains. Most indicators identified were categorized under the dimensions of resources and agency and were about accessing resources (A) and material resource allocation (B1). On the other hand, only 5 studies used indicators for the time-resource allocation (B2) and only 3 studies looked at the empowerment in reproduction (C). Similarly, only 14 studies used indicators capturing the achievement dimension of women's empowerment.
TABLE 2.
Types of indicators of women's empowerment found in the studies reviewed
| Dimension of empowerment | ||||
|---|---|---|---|---|
| Group of indicators | Resources | Agency | Achievements | Multiple |
| (A) Accessing resources for households | Group membership (79, 93, 95, 107, 109, 135); Leadership in groups (93, 131, 135) | Mobility decision (79, 104, 110, 119, 124, 125); Decision to stay visit family/friends (83, 97, 117, 124); Credit decision making (93, 107, 135); Agriculture decision (93, 108, 109, 135) | If women receive social support (92, 95); Women's mobility (122, 123, 125); Access to credit (127); Access to media (78, 87) | Index on mobility (88) |
| (B1) Allocating resources within household, material allocation | Women's share of income (98, 131); Difference in income with spouse (82); Women's asset ownership (77, 80, 93, 98, 107, 108, 118, 135) | Food allocation decision making (83, 85, 114, 118, 122–124); Money allocation decision making (75, 78, 81, 93, 94, 97, 109, 117–119, 124–126, 135) | Mother can spend money as needed (79, 127) | Index on money allocation power (92) |
| (B2) Allocating resources within household, time allocation | — | — | Women's time use (93, 109, 135); Male involvement in household work (79) | Father's involvement in child care index (75) |
| (B3) Allocating resources within household, child care | — | Child care decision (83, 111, 119, 125) | — | — |
| (B4) Allocating resources within household, parent care | — | Decision on own health care (83, 90, 90, 94, 97, 101, 102, 117, 118, 124, 126); Mobility to accessing own health care (94, 100) | Feeling empowered (79, 103, 127); Life satisfaction (107) | — |
| (C) Reproduction decisions | Domestic violence attitude, sexual (104) | Family planning decision (75); Decision on when to have sex (81) | Experience of sexual domestic violence (128) | — |
| (Multiple) | Education difference (82, 88, 104); Domestic violence attitude score (81, 82, 88, 92, 119, 124, 125, 128); Age difference (82, 88) | Multiple decisions (75, 79, 80, 82, 84, 87–89, 91, 92, 99, 102, 106, 110, 112, 115, 116, 125, 132–134, 136) | Experience of domestic violence (82, 120–123, 125, 128) | Women's empowerment in Agriculture Index (93, 107–109, 135); Controlling behaviors (102, 121); Any domestic violence experience (102); Maternal capabilities index (103); Other (79, 85, 96, 105, 113, 122, 122) |
Relationships between women's empowerment and child nutrition
We identified 1316 associations between women's empowerment indicators and the various child nutrition measures. Of those, 227 (36% weighted) reported associations were statistically significant and positive. Although this is more than the 34 negative associations observed (2% weighted), the majority (1055 associations, 62% weighted) were not statistically significant, which indicates an overall limited evidence base for the impact of women's empowerment on various child nutrition outcomes.
Women's empowerment and child nutritional status
Women's empowerment and stunting
We identified 461 associations from 39 studies, and of those, 70 associations (20% weighted) were positively statistically significant, whereas 12 associations (3% weighted) were negatively significant (Supplemental Figure 1A, Supplemental Table 5). This proportion is observed across most dimensions and indicator groups for which there are enough studies, such as domains of accessing resources (A), material resource allocation (B1), and aggregate indexes (“multiple”). Few studies looked at indicators of time resource allocation (B2) and child care (B3).
The effect sizes for these associations were also small. Out of 307 associations with height-for-age z score, 186 (36% weighted) were between −0.10 and 0.10 SDs. Out of 146 associations with stunting, 76 (60% weighted) had an OR between 0.9 and 1.11. Stratified analysis (Supplemental Figure 2) revealed that positive associations were more likely to be found in studies that used primary data than in those that used secondary data sources and in studies that did not control for pathway variables. We also found that very few studies for this relationship were available for children aged <2 y.
Women's empowerment and wasting
We also examined the 258 associations from 22 studies examining the relationship between women's empowerment and wasting outcomes as an indicator of acute malnutrition. Of those associations, only 34 (33% weighted) were positively statistically significant, and 7 (2% weighted) were negatively significant (Supplemental Figure 1B, Supplemental Table 6). Overall, there were fewer indicators tested against this outcome, with most studies only looking at indicators of material allocation domain and indicators for multiple domains. The high proportion of significant relationships with this outcome was between indicators encompassing multiple dimensions and domains, and it is driven by 3 studies that only report 1–3 relationships and therefore were weighted more (91, 96, 105). Most of the effect sizes were also small: 135 out of 201 effects (41% weighted) on weight-for-height z score were between −0.10 and 0.10 SD, and 15 out of 24 effects on wasting had ORs of between 0.9 and 1.11. We also saw from the stratified analysis (Supplemental Figure 3) that very few studies looking at this outcome were performed in South Asia. Results from underweight outcome can be found in Supplemental Table 7.
Women's empowerment and proximate determinants
Infant and young child feeding
Few studies investigated the relationship between women's empowerment and infant and young child feeding practices. We found 7 studies that examined breastfeeding outcomes (Supplemental Figure 1C, Supplemental Table 8), and most of the associations tested are with indicators from resource dimensions. From these studies, 46 associations were tested, with only 5 (13% weighted) found to be positively significant and another 5 (10% weighted) to be negatively significant. The average effect size of women's empowerment on the duration of breastfeeding was less than half a day, and the geometric average OR of the effect of various women's empowerment measures on exclusive breastfeeding was 0.99.
Ten included studies looked at complementary feeding outcomes (Supplemental Figure 1D, Supplemental Table 9). From the 163 associations tested, 25 (32% weighted) were positively significant, and 8 (5% weighted) were negatively significant. For both outcomes, studies tended to use indicators that would encompass multiple domains or multiple dimensions. The average effect size of women's empowerment on dietary diversity score was 0.04 food groups, whereas the average effect size on meal frequency was only 0.01 times/d.
Health inputs
We found 3 studies looking at the relationship of various women's empowerment measures with various illnesses in children (Supplemental Figure 1E, Supplemental Table 10) and 14 studies on the relationship with health care use (Supplemental Figure 1F, Supplemental Table 11), including vaccination, antenatal class attendance, and health care access when a child is sick. There were 18 out of 26 (67% weighted) and 25 out of 48 (62% weighted) positive statistically significant relationships between empowerment measures and illness and health care use, respectively. The average ORs of the effect of various women's empowerment measures on various measures on illness and various health care use measures were 1.44 and 1.13, respectively.
Discussion
In this paper, we reviewed 62 studies of the relationship between women's empowerment and nutrition. We found that the women's empowerment indicators used in these studies were inconsistent and limited in scope (Table 2), and that the strength of the relationship between women's empowerment and child nutrition was often overstated. Below, we elaborate on each of these.
Objective 1: parse and critically review indicators
We found 2 seemingly contradictory problems with indicators currently used in studies examining the relationship between women's empowerment and child nutrition. On the one hand, we found a huge variation (200 unique indicators), which made comparing multiple studies difficult, a problem identified by previous reviews (7–9). This variation was due to the variety in aggregation and operationalization of women's empowerment indicators. For example, some studies that include indicators of the agency dimension of empowerment include joint decision making (75, 78, 83, 85, 88, 94, 97, 101, 117, 126, 128, 133, 134), whereas others only count women making a final decision as a sign of empowerment (91, 114, 118). Another example is the variety of questions asked within an indicator. When looking at the material resource allocation domain, indicators irregularly included women's financial decision making for any of the following: large purchases, food purchases, daily purchases, medicine, clothes, toiletries, and so on.
On the other hand, we found that the current literature is still lacking studies that use indicators in dimensions and domains relevant to child nutrition, such as indicators on time resource allocation and reproduction, indicators of the achievement dimension, and indicators for men's engagement in child care and nutrition (Supplemental Figure 1). Cunningham et al. (5) also noticed the lack of workload and time resource allocation indicators. A possible explanation for the absence of these indicators is that 68% of the included studies were a secondary analysis of Demographic Health Surveys and Indian National Family and Health Survey datasets, which do not contain these indicators. Our current evidence for the relationship between women's empowerment and child nutrition is highly reliant on indicators available in those 2 datasets. A further explanation of the lack of indicators on men's engagement in child care and nutrition is possibly due to assumptions that men may not support women's empowerment (69–71) or care about children's well-being (138). In support of this, a review of gender-integrated women's empowerment programs found that relatively few programs that include men and boys go beyond the pilot stage or last beyond a short-term time frame (139).
We also found that many indicators aggregate multiple dimensions and domains of empowerment. This aggregation can be problematic when some parts of the indicator is significantly related to the nutrition outcome, and others are not. This introduced a measurement error that biases the estimate of the relationship between women's empowerment and child nutrition towards zero.
Objective 2: summarize evidence
There was underwhelming evidence of a positive association between women's empowerment and child nutritional status. For stunting (Supplemental Figure 1A) and wasting (Supplemental Figure 1B), the vast majority of the associations tested were not statistically significant, and overall, the average effect sizes were small. Unfortunately, this lack of statistically significant relationships with nutritional outcomes was consistent throughout the various dimensions and groups of indicators. This finding was true even when we stratified the studies (Supplemental Figures 2 and 3) according to age group of participating children (<2 y old compared with <5 y old), region of participants (South Asia compared with sub-Saharan Africa), whether a study controls for pathway variables, data source (primary compared with secondary), or whether a study was a published journal article (compared with gray literature).
To understand the lack of clear association between any dimension and domains of women's empowerment to child nutrition status, we examined the relationship between women's empowerment and proximate determinants of child nutritional status: infant and young child feeding practices, child illness, and health care use. We found similarly inconclusive evidence of relationships between women's empowerment measures and infant and young child feeding (see Supplemental Figure 1C for breastfeeding and Supplemental Figure 1D for complementary feeding). On the other hand, significant positive associations were more likely to be reported for illness (33 out of 36 associations, 78% weighted) and health care use (11 out of 20 associations, 62% weighted). It is critical, however, to remember that associations between women's empowerment and illness were only found in 3 studies and any strong claim between women's empowerment and child illness are pending further evidence.
Objective 3: suggestions for further research
There are 2 possible explanations for the weak evidence between women's empowerment and child nutrition. One is that there is no underlying relationship between women's empowerment and child nutrition. The other is that this lack of evidence is due to methodologic weaknesses. Before we discount the role of women's empowerment as unimportant for child nutrition, we argue that we should first improve the quality of evidence on the relationship. To do that, like Richardson (17), we encourage researchers to design studies that allow for full integration of theories of women's empowerment and a clear indication of the specific pathways between women's empowerment and child nutrition being tested. Specifically:
Reconsider choice of study design
All studies reviewed were observational and cross-sectional. Furthermore, very few studies used any statistical manipulation such as instrumental variables or matching that would help with establishing stronger counterfactuals. We therefore agree with a recommendation by Carlson and Pratley (4, 140) and suggest more rigorous longitudinal study design or even a randomized-intervention approach to testing the effects of improved gender equity. This would allow for a causal inference because it would eliminate the possible endogeneity that empowered women are simply different from nonempowered women.
Assess across the life cycle
Longitudinal study designs would also allow for analysis of how empowerment across the life cycle might differentially affect child nutrition (Figure 1). Different domains of empowerment might be essential at various points in the life course. For example, agency in reproductive decisions (i.e., choices of contraception and when to get pregnant) would play a role in a mother's readiness for pregnancy and therefore might affect stunting outcomes upon birth, but we would not expect agency in reproduction decisions to affect a 2-y-old's diet.
This is especially important because a large proportion of the studies we found test women's current empowerment and whether their child is stunted. Stunting is an indicator of chronic malnutrition; it might be affected by women's decision-making power as to whether she wants to be pregnant in the first place, her workload during pregnancy and breastfeeding, her child's diet over the years, and so on. Because a woman's level of empowerment can vary over time, her current empowerment level might not reflect those indicators. This mismatch between the timing of empowerment and child nutrition indicators is even more pronounced in studies looking at children aged >2 y, which was the case in 32 out of 39 studies on women's empowerment and stunting.
Define pathways tested
We found that few studies in our reviews articulated and tested the pathway between women's empowerment and child nutrition. Consequently, we found that many of the studies control for pathway variables between women's empowerment and child nutrition in their regression, e.g., care practice score, infant and young child feeding practices, or health care access. Controlling for pathway variables might explain the null associations found in the literature. A more helpful and interesting analysis would be to examine the relationship between women's empowerment and these pathway variables or to even conduct mediation analyses of these pathway variables. We are aware of qualitative studies that describe how these pathways affect child nutrition (141–143); however, we found very few quantitative studies doing so.
Consider pathways when choosing empowerment indicators
Precise identification of proposed pathways and contextual knowledge between women's empowerment and nutrition can also guide a better choice of indicators for these studies. Our finding that positive associations are more likely to be found from studies that use primary data sources rather than secondary data sources (Supplemental Figures 2 and 3) suggest the importance of careful selection of indicators. In general, we need more studies that use indicators capturing time resource allocation (B2) and reproductive decisions (C), indicators of the achievement dimension, and indicators for men's engagement in child care and nutrition. In contrast, we do not need more studies about how child nutrition might be affected by empowerment based on indicators that do not have a clear pathway of the impact towards child nutrition, e.g., age at first marriage or political group membership. Similarly, explicitly describing pathways tested would prevent researchers from making use of indicators that aggregate various pathways towards child nutrition, as discussed earlier.
Examples of pathways that should be tested can be found in Figure 1. Empowerment in accessing resources (A), for example, should have an impact on household resources such as food security and access to health services to even have a chance of having an impact on child nutrition. More research should also be done on empowerment in reproductive decisions (C), women's readiness for pregnancy, and child nutritional status at birth. There is also a need for more studies on the role of mother's physical and mental health on the relationship between various resource allocation indicators (B) and child care practices, and eventually child nutrition. Empowerment in mother's time allocation, women's time use after giving birth, and rate of exclusive breastfeeding is another research opportunity, as is the relationship between empowerment in reproductive decisions, birth spacing, and duration of breastfeeding.
Investigate interaction with household wealth
Another inquiry worthy of analysis is how women's empowerment would interact with household wealth. It is easy to see how, in extremely wealthy households, where food is abundant, women's ability to make a decision might not be correlated with child nutrition because household resource allocation is not a contested issue. On the other hand, in a household with very few resources, a change in a woman's decision-making power in material resource (e.g., money, food) allocation would likely have no effect on improved infant and young child feeding practices and child nutrition outcomes (144).
Improve operationalization of empowerment indicators
Because debates about women's empowerment indicators are still ongoing, studies comparing various operationalizations of a specific indicator on its strength of association with child nutrition might be a helpful contribution to the literature. For example, to help contribute data to the debate on whether to include joint decision making when measuring income-allocation decision making, researchers could report on both ways to operationalize the indicator and compare how the two operationalizations relate to child's diet.
Increase the types of population studied
Only 14 out of 62 studies included data from outside South Asia and sub-Saharan Africa. Because the importance of various dimensions and domains of women's empowerment vary by region, more studies looking at this relationship in regions such as East Asia and the Pacific, the Middle East and North Africa, and Latin America and the Caribbean are needed. Studies in sub-Saharan Africa are also needed to address the current gap in dimensions and domains, e.g., child care and reproductive domains.
Limitations
Given that the concept of women's empowerment encompasses such a broad set of indicators, it is probable that we missed studies analyzing domains and dimensions of women's empowerment if the studies did not frame the topic as women's empowerment. Examples include studies on maternal social support and education in the context of maternal capabilities and knowledge. We tried to minimize this by hand-searching bibliographies of selected articles to minimize omission of relevant articles. Similarly, our discussion of pathways is also hindered by our keyword search. Our focus on nutritional status might prevent us from finding discussions between women's empowerment and other important pathways such as food security or access to health services. However, this does not negate our finding that papers analyzing the relationship between women's empowerment and child nutrition did not include discussion of these pathways. Another limitation of this study is our focus on quantitative studies. Qualitative data would help us to understand the various pathways in which women's empowerment would affect child nutrition because this relationship is so highly contextual. However, this was outside the scope of the current article.
Conclusions
The impact of women's empowerment on child nutrition is a burgeoning field with plenty of analytic opportunities and a worthwhile end goal of informing interventions. So far, the evidence has been limited and inconclusive: 379 out of 461 (82% weighted) and 217 out of 258 (84% weighted) associations between women's empowerment and stunting and wasting outcomes, respectively, were not significant. Before we discount the role of women's empowerment as unimportant for child nutrition, we invite the research community to focus on studying the pathways between women's empowerment and child nutrition by explicitly declaring which pathways between women's empowerment and child nutrition they are testing, carefully selecting the appropriate women's empowerment indicators and aggregating them meaningfully, and collecting primary longitudinal data that will allow pathway analysis to take into account the population's life cycle. We also invite the research community to conduct this research on populations outside South Asia and sub-Saharan Africa.
Supplementary Material
Acknowledgments
We thank the research assistants who helped with article screening, data extraction, and bias assessment for this review: Casey Benzaken, Amelia Beck, and Emilie Umuhire from Northwestern University, and Julie Risman from Cornell University. We also thank the Young Research Group for their support. The authors’ responsibilities were as follows—MVS: conceived the research idea, designed the research protocol, oversaw article screening and intervened as necessary, extracted data, analyzed data, conducted bias assessment, and wrote the manuscript; SLY: conceived the research idea, advised on the research protocol, interpreted the data, and critically revised the manuscript; PG and SO: conducted literature searches, screened articles, and extracted data; RBK and JH: provided critical advice on research protocol, interpreted the data, and revised the manuscripts; and all authors: read and approved the final manuscript.
Notes
MVS was partly supported by the Collaborative Crop Research Program of the McKnight Foundation. SLY was supported by the National Institutes of Health (K01 MH098902).
Author disclosures: MVS, RBK, JH, PG, SO, and SLY, no conflicts of interest.
Supplemental Tables 1–11 and Supplemental Figures 1–3 are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/advances/.
References
- 1. Kabeer N. Resources, agency, achievements: reflections on the measurement of women's empowerment. Dev Change. 1999;30:435–64. [Google Scholar]
- 2. Scaling Up Nutrition. In practice brief #6: empowering women and girls to improve nutrition: building a sisterhood of success. [Internet] 2016. Available from:http://docs.scalingupnutrition.org/wp-content/uploads/2016/05/IN-PRACTICE-BRIEF-6-EMPOWERING-WOMEN-AND-GIRLS-TO-IMPROVE-NUTITION-BUILDING-A-SISTERHOOD-OF-SUCCESS.pdf. [Google Scholar]
- 3. Ruel MT, Alderman H. Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition?. Lancet. 2013;382:536–51. [DOI] [PubMed] [Google Scholar]
- 4. Carlson GJ, Kordas K, Murray-Kolb LE. Associations between women's autonomy and child nutritional status: a review of the literature. Matern Child Nutr. 2015;11:452–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Cunningham K, Ruel M, Ferguson E, Uauy R. Women's empowerment and child nutritional status in South Asia: a synthesis of the literature. Matern Child Nutr. 2015;11:1–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Pratley P. Associations between quantitative measures of women's empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Soc Sci Med. 2016;169:119–31. [DOI] [PubMed] [Google Scholar]
- 7. Sen A. Well-being, agency and freedom: the Dewey Lectures 1984. J Philos. 1985;82, 4:169–221. [Google Scholar]
- 8. Cornwall A, Edwards J. Introduction: negotiating empowerment. IDS Bull. 2010;41:1–9. [Google Scholar]
- 9. Malhotra A, Schuler SR. Women's empowerment as a variable in international development. Meas Empower Cross-Discip Perspect. 2005;1:71–88. [Google Scholar]
- 10. Alsop R, Bertelsen MF, Holland J. Empowerment in practice: from analysis to implementation. World Bank; 2006. [Google Scholar]
- 11. Ibrahim S, Alkire S. Agency and empowerment: a proposal for internationally comparable indicators. Oxf Dev Stud. 2007;35:379–403. [Google Scholar]
- 12. Cornwall A, Anyidoho NA. Introduction: women's empowerment: contentions and contestations. Development. 2010;53:144–9. [Google Scholar]
- 13. Alsop R, Heinsohn N. Measuring empowerment in practice: structuring analysis and framing indicators. World Bank; 2005. [Google Scholar]
- 14. Kim SS, Ali D, Kennedy A, Tesfaye R, Tadesse AW, Abrha TH, Rawat R, Menon P. Assessing implementation fidelity of a community-based infant and young child feeding intervention in Ethiopia identifies delivery challenges that limit reach to communities: a mixed-method process evaluation study. BMC Public Health. 2015;15:316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Mosedale S. Assessing women's empowerment: towards a conceptual framework. J Int Dev. 2005;17:243–57. [Google Scholar]
- 16. Samman E, Santos M. Agency and empowerment: a review of concepts, indicators and empirical evidence. [Internet] Oxford Poverty and Human Development Initiative; 2009 [cited 2018 May 15]. Available from:http://www.ophi.org.uk/wp-content/uploads/OPHI-RP-10a.pdf, Accessed Dec 15, 2018. [Google Scholar]
- 17. Richardson RA. Measuring women's empowerment: a critical review of current practices and recommendations for researchers. Soc Indic Res. 2018;137:539–57. [Google Scholar]
- 18. Ghuman SJ, Lee HJ, Smith HL. Measurement of women's autonomy according to women and their husbands: results from five Asian countries. Soc Sci Res. 2006;35:1–28. [Google Scholar]
- 19. Ahmed AU, Quisumbing AR, Nasreen M, Hoddinott JF, Bryan E. Comparing food and cash transfers to the ultra poor in Bangladesh. Washington (DC): International Food Policy Research Institute; 2009. [Google Scholar]
- 20. Al Riyami A, Afifi M, Mabry RM. Women's autonomy, education and employment in Oman and their influence on contraceptive use. Reprod Health Matters. 2004;12:144–54. [DOI] [PubMed] [Google Scholar]
- 21. Chakrabarti S, Biswas CS. An exploratory analysis of women's empowerment in India: a structural equation modelling approach. J Dev Stud. 2012;48:164–80. [Google Scholar]
- 22. Hadley C, Brewis A, Pike I. Does less autonomy erode women's health? Yes. No. Maybe.Am J Hum Biol. 2010;22:103–10. [DOI] [PubMed] [Google Scholar]
- 23. Jejeebhoy SJ. Women's autonomy in rural India: its dimensions, determinants, and the influence of context. na; 2000. [Google Scholar]
- 24. Morgan S, Niraula SR. Gender inequality and fertility in two Nepali villages. Popul Dev Rev. 1995;21:541–61. [Google Scholar]
- 25. Schuler SR, Islam F, Rottach E. Women's empowerment revisited: a case study from Bangladesh. Dev Pract. 2010;20:840–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Agarwala R, Lynch SM. Refining the measurement of women's autonomy: an international application of a multi-dimensional construct. Soc Forces. 2006;84:2077–98. [Google Scholar]
- 27. Mason KO. The status of women: conceptual and methodological issues in demographic studies. Sociol Forum. 1986;1:284–300. [Google Scholar]
- 28. Alkire S, Meinzen Dick R, Peterman A, Quisumbing AR, Seymour G, Vaz A. The women’s empowerment in agriculture index. [Internet]. Oxford: Oxford Poverty & Human Development Initiative, 2013[cited 2017 May 31]. Available from: http://www.ophi.org.uk/wp-content/uploads/ophi-wp-58.pdf?cda6c1. [Google Scholar]
- 29. Engle PL, Menon P, Haddad L. Care and nutrition: concepts and measurement. World Dev. 1999;27:1309–37. [Google Scholar]
- 30. McGuire J, Popkin B. Beating the zero sum game: women and nutrition in the Third World. Part 2. Food Nutr Bull. 1990;12:3–11. [Google Scholar]
- 31. Bhagowalia P, Menon P, Quisumbing AR, Soundararajan V. Unpacking the links between women's empowerment and child nutrition: evidence using nationally representative data from Bangladesh, Agricultural and Applied Economics Association (AAEA) 2010 Annual Meeting [Internet]. 2010[cited 2015 Jan 26]. Available from: https://ageconsearch.umn.edu/record/61273. [Google Scholar]
- 32. Causes and most vulnerable to undernutrition—UNICEF Conceptual Framework [Internet]. [cited 24 April, 2016]. Available from: http://www.unicef.org/nutrition/training/2.5/4.html. [Google Scholar]
- 33. Quisumbing AR, Maluccio JA. Resources at marriage and intrahousehold allocation: evidence from Bangladesh, Ethiopia, Indonesia, and South Africa. Oxf Bull Econ Stat. 2003;65:283–327. [Google Scholar]
- 34. Hoddinott J, Haddad L. Does female income share influence household expenditures? Evidence from Côte d'Ivoire. Oxf Bull Econ Stat. 1995;57:77–96. [Google Scholar]
- 35. Seymour G. Women's empowerment in agriculture: implications for technical efficiency in rural Bangladesh. Agric Econ. 2016;48:513–22. [Google Scholar]
- 36. Sharaunga S, Mudhara M, Bogale A. Effects of ‘women empowerment’ on household food security in rural KwaZulu-Natal province. Dev Policy Rev. 2016;34:223–52. [Google Scholar]
- 37. Tsiboe F, Zereyesus YA, Popp JS, Osei E. The effect of women's empowerment in agriculture on household nutrition and food poverty in Northern Ghana. Soc Indic Res. 2018;138(1):89–108. [Google Scholar]
- 38. Porter M. Effects of microcredit and other loans on female empowerment in Bangladesh: the borrower's gender influences intra-household resource allocation. Agric Econ. 2016;47(2):235–45. [Google Scholar]
- 39. United Nations Children's Fund, Liverpool School of Tropical Medicine. Gender influences on child survival, health and nutrition: a narrative review. New York and Liverpool: UNICEF; 2011. [Google Scholar]
- 40. Babu SC, Thirumaran S, Mohanam TC. Agricultural productivity, seasonality and gender bias in rural nutrition: empirical evidence from South India. Soc Sci Med. 1993;37:1313–9. [DOI] [PubMed] [Google Scholar]
- 41. Von Braun J, De Haen H, Blanken J. Commercialization of agriculture under population pressure: effects on production, consumption, and nutrition in Rwanda. Int Food Policy Res Inst. 1991; Report No.: 85. [Google Scholar]
- 42. Handa S. Expenditure behavior and children's welfare: an analysis of female headed households in Jamaica. J Dev Econ. 1996;50:165–87. [DOI] [PubMed] [Google Scholar]
- 43. Schultz TP. Testing the neoclassical model of family labor supply and fertility. J Hum Resour. 1990;25(4):599–634. [Google Scholar]
- 44. Doan RM, Bisharat L. Female autonomy and child nutritional status: the extended-family residential unit in Amman, Jordan. Soc Sci Med. 1990;31:783–9. [DOI] [PubMed] [Google Scholar]
- 45. Castle SE. Child fostering and children's nutritional outcomes in rural Mali: the role of female status in directing child transfers. Soc Sci Med. 1995;40:679–93. [DOI] [PubMed] [Google Scholar]
- 46. Engle PL. Maternal work and child-care strategies in peri-urban Guatemala: nutritional effects. Child Dev. 1991;62:954–65. [DOI] [PubMed] [Google Scholar]
- 47. Garcia M. Impact of female sources of income on food demand among rural households in the Philippines Vol. 30. [Internet].1991; [cited 2015 Oct 23]. Available from: http://krishikosh.egranth.ac.in/handle/1/2055733. [Google Scholar]
- 48. Blackden M, Wodon Q. Gender, time use, and poverty: introduction. [Internet] MPRA paper; 2006; [cited 2015 May 19]. Available from: http://mpra.ub.uni-muenchen.de/11080/. [Google Scholar]
- 49. Johnston D, Stevano S, Malapit HJ, Hull E, Kadiyala S. Review: time use as an explanation for the agri-nutrition disconnect: evidence from rural areas in low- and middle-income countries. Food Policy. 2018;76:8–18. [Google Scholar]
- 50. Nnam NM. Improving maternal nutrition for better pregnancy outcomes. Proc Nutr Soc. 2015;74:454–9. [DOI] [PubMed] [Google Scholar]
- 51. Wrottesley SV, Lamper C, Pisa PT. Review of the importance of nutrition during the first 1000 days: maternal nutritional status and its associations with fetal growth and birth, neonatal and infant outcomes among African women. J Dev Orig Health Dis. 2016;7:144–62. [DOI] [PubMed] [Google Scholar]
- 52. Nguyen PH, Saha KK, Ali D, Menon P, Manohar S, Mai LT, Rawat R, Ruel MT. Maternal mental health is associated with child undernutrition and illness in Bangladesh, Vietnam and Ethiopia. Public Health Nutr. 2014;17:1318–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Dias CC, Figueiredo B. Breastfeeding and depression: a systematic review of the literature. J Affect Disord. 2015;171:142–54. [DOI] [PubMed] [Google Scholar]
- 54. Bennett L. The role of women in income production and intra-household allocation of resources as a determinant of child nutrition and health. Food Nutr Bull. 1988;10:16–26. [Google Scholar]
- 55. Balk D. Individual and community aspects of women's status and fertility in rural Bangladesh. Popul Stud. 1994;48:21–45. [Google Scholar]
- 56. Upadhyay UD, Hindin MJ. Do higher status and more autonomous women have longer birth intervals? Results from Cebu, Philippines. Soc Sci Med. 2005;60:2641–55. [DOI] [PubMed] [Google Scholar]
- 57. DeRose LF, Ezeh AC. Decision-making patterns and contraceptive use: evidence from Uganda. Popul Res Policy Rev. 2009;29:423–39. [Google Scholar]
- 58. Abada T, Tengkorang ET. Women's autonomy and unintended pregnancies in the Philippines. J Biosoc Sci. 2012;44:703–18. [DOI] [PubMed] [Google Scholar]
- 59. Goisis A, Remes H, Barclay K, Martikainen P, Myrskylä M. Advanced maternal age and the risk of low birth weight and preterm delivery: a within-family analysis using Finnish population registers. Am J Epidemiol. 2017;186:1219–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Hoque ME. Advanced maternal age and outcomes of pregnancy: a retrospective study from South Africa. Biomed Res. 2012;23:(2):. [Google Scholar]
- 61. Haldre K, Rahu K, Karro H, Rahu M. Is a poor pregnancy outcome related to young maternal age? A study of teenagers in Estonia during the period of major socio-economic changes (from 1992 to 2002). Eur J Obstet Gynecol Reprod Biol. 2007;131:45–51. [DOI] [PubMed] [Google Scholar]
- 62. Paranjothy S, Broughton H, Adappa R, Fone D. Teenage pregnancy: who suffers?. Arch Dis Child. 2009;94:239–45. [DOI] [PubMed] [Google Scholar]
- 63. Conde-Agudelo A. Maternal morbidity and mortality associated with interpregnancy interval: cross sectional study. BMJ. 2000;321:1255–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: evidence from the demographic and health surveys. Int J Gynecol Obstet. 2005;89:S7–24. [DOI] [PubMed] [Google Scholar]
- 65. Conde‐Agudelo A, Rosas‐Bermudez A, Castaño F, Norton MH. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms. Stud Fam Plann. 2012;43:93–114. [DOI] [PubMed] [Google Scholar]
- 66. UNICEF. Tracking progress on child and maternal nutrition: a survival and development priority. [Internet] UNICEF; 2013; [cited 2013 July 17]. Available from: http://www.unicef.org/publications/index_51656.html#. [Google Scholar]
- 67. Njuki J, Sanginga PC. Women, livestock ownership and markets: bridging the gender gap in eastern and southern Africa. Routledge; 2013. [Google Scholar]
- 68. Doggett E, Goodridge G, Mosely E, Shattuck D, Wilcher R. Gender integration framework: how to integrate gender in every aspect of our work. [Internet]. Durham (NC): FHI360, 2012[cited 2015 Nov 3]. Available from: http://www.fhi360.org/sites/default/files/media/documents/FHI%20360_Gender%20Integration%20Framework_3.8%20%2528no%20photos%2529.pdf. [Google Scholar]
- 69. Chant SH. Gender, generation and poverty: exploring the feminisation of poverty in africa, Asia and Latin America. Edward Elgar; 2007. [Google Scholar]
- 70. Hwang T, Miruka M. Engaging men and boys in food and nutrition security: the hidden half of gender equality programming. [Internet]. 2014; [cited 2015 Nov 3]. Available from: https://www.spring-nutrition.org/events/engaging-men-and-boys-food-and-nutrition-security-hidden-half-gender-equality-programming. [Google Scholar]
- 71. Barker G, Schulte J. Engaging men as allies in women's economic empowerment: strategies and recommendations for CARE country offices. [Internet] Oslo: CARE; 2010[cited 2015 Nov 2]. Available from: http://pathways.care2share.wikispaces.net/file/view/Engaging+Men+in+econ+WE_Report+on+CARE.doc/312576840/Engaging+Men+in+econ+WE_Report+on+CARE.doc. [Google Scholar]
- 72. National Heart, Lung, and Blood Institute (NHLBI). Study quality assessment tools [Internet]. [cited 2018 May 9]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. [Google Scholar]
- 73. Quantitative Research Assessment Tool [Internet]. [cited 2018 Aug 20]. Available from: https://www.researchconnections.org/childcare/datamethods/downloads/quantitativeresearch.pdf. [Google Scholar]
- 74. WHO. Indicators for assessing infant and young child feeding practices [Internet]. WHO; 2008[cited 2016 Oct 26]. Available from: http://www.who.int/water_sanitation_health/monitoring/oms_brochure_core_questionsfinal24608.pdf. [Google Scholar]
- 75. Abate KH, Belachew T. Women's autonomy and men's involvement in child care and feeding as predictors of infant and young child anthropometric indices in coffee farming households of Jimma Zone, South West of Ethiopia. PLoS One. 2017;12:e0172885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Ackerson LK, Subramanian SV. Domestic violence and chronic malnutrition among women and children in India. Am J Epidemiol. 2008;167:1188–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Agarwal S, Srivastava A. Social determinants of children's health in urban areas in India. J Health Care Poor Underserved. 2009;20:68–89. [DOI] [PubMed] [Google Scholar]
- 78. Aguayo VM, Nair R, Badgaiyan N, Krishna V. Determinants of stunting and poor linear growth in children under 2 years of age in India: an in-depth analysis of Maharashtra's comprehensive nutrition survey. Matern Child Nutr. 2016;12:121–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Alaofè H, Zhu M, Burney J, Naylor R, Douglas T. Association between women's empowerment and maternal and child nutrition in Kalalé district of northern Benin. Food Nutr Bull. 2017;38:302–18. [DOI] [PubMed] [Google Scholar]
- 80. Allendorf K. Do women's land rights promote empowerment and child health in Nepal?. World Dev. 2007;35:1975–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Amugsi DA, Mittelmark MB, Lartey A, Matanda DJ, Urke HB. Influence of childcare practices on nutritional status of Ghanaian children: a regression analysis of the Ghana Demographic and Health Surveys. BMJ Open. 2014;4:e005340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Antai D. Gender inequities, relationship power, and childhood immunization uptake in Nigeria: a population-based cross-sectional study. Int J Infect Dis. 2012;16:e136–45. [DOI] [PubMed] [Google Scholar]
- 83. Barrios PL. Relationship between household structure, maternal autonomy and undernutrition in Brazilian children. Rutgers, The State University of New Jersey, New Brunswick. [thesis]; 2012. [Google Scholar]
- 84. Becker S, Fonseca-Becker F, Schenck-Yglesias C. Husbands’ and wives’ reports of women's decision-making power in Western Guatemala and their effects on preventive health behaviors. Soc Sci Med. 2006;62:2313–26. [DOI] [PubMed] [Google Scholar]
- 85. Begin F, Habicht J-P, Frongillo Jr EA, Delisle H. The deterioration in children's nutritional status in rural Chad: the effect of mothers’ influence on feeding. Am J Public Health. 1997;87:1356–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Begin F, Frongillo EA, Delisle H. Caregiver behaviors and resources influence child height-for-age in rural Chad. J Nutr. 1999;129:680–6. [DOI] [PubMed] [Google Scholar]
- 87. Begum S, Sen B. Maternal health, child well-being and chronic poverty: does women's agency matter?. Bangladesh Dev Stud. 2009;69–93. [Google Scholar]
- 88. Bhagowalia P, Menon P, Quisumbing AR, Soundararajan V. What dimensions of women's empowerment matter most for child nutrition?[Internet]. Washington (DC): IFPRI; 2012 [cited 2015 Jan 26]. [Google Scholar]
- 89. Bose S. The effect of women's status and community on the gender differential in children's nutrition in India. J Biosoc Sci. 2011;43:513–33. [DOI] [PubMed] [Google Scholar]
- 90. Brennan L, McDonald J, Shlomowitz R. Infant feeding practices and chronic child malnutrition in the Indian states of Karnataka and Uttar Pradesh. Econ Hum Biol. 2004;2:139–58. [DOI] [PubMed] [Google Scholar]
- 91. Brunson EK, Shell-Duncan B, Steele M. Women's autonomy and its relationship to children's nutrition among the Rendille of northern Kenya. Am J Hum Biol. 2009;21:55–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Cliffer IR. Women's empowerment and infant and young child feeding in Bangladesh [thesis]. [Internet]. Emory University; 2013; [cited 2015 Jan 20]. Available from: http://catalog.ihsn.org/index.php/citations/21342. [Google Scholar]
- 93. Cunningham K, Ploubidis GB, Menon P, Ruel M, Kadiyala S, Uauy R, Ferguson E. Women's empowerment in agriculture and child nutritional status in rural Nepal. Public Health Nutr. 2015;18:3134–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Dancer D, Rammohan A. Maternal autonomy and child nutrition: evidence from rural Nepal. Indian Growth Dev Rev. 2009;2:18–38. [Google Scholar]
- 95. De Silva MJ, Harpham T. Maternal social capital and child nutritional status in four developing countries. Health Place. 2007;13:341–55. [DOI] [PubMed] [Google Scholar]
- 96. Debnath A, Bhattacharjee N. Understanding malnutrition of tribal children in India: the role of women's empowerment. Ecol Food Nutr. 2016;55:508–27. [DOI] [PubMed] [Google Scholar]
- 97. Desai S, Johnson K. Women's decision making and child health: familial and social hierarchies, in A focus on gender: collected papers on gender using DHS data. 2005;55–68. [Google Scholar]
- 98. Fafchamps M, Kebede B, Quisumbing AR. Intrahousehold welfare in rural Ethiopia. Oxf Bull Econ Stat. 2009;71:567–99. [Google Scholar]
- 99. Franckel A, Lalou R. Health seeking behaviour for childhood malaria: household dynamics in rural Senegal. J Biosoc Sci. 2009;41:1. [DOI] [PubMed] [Google Scholar]
- 100. Grabowski R, Self S. Mother's autonomy: impact on the quality of children's healthcare in India. Appl Econ. 2013;45:1903–13. [Google Scholar]
- 101. Haile ZT, Chertok IRA, Teweldeberhan AK. Determinants of utilization of sufficient tetanus toxoid immunization during pregnancy: evidence from the Kenya Demographic and Health Survey, 2008–2009. J Community Health. 2013;38:492–9. [DOI] [PubMed] [Google Scholar]
- 102. Heaton TB, Forste R. Domestic violence, couple interaction and children's health in Latin America. J Fam Violence. 2008;23:183–93. [Google Scholar]
- 103. Ickes SB, Wu M, Mandel MP, Roberts AC. Associations between social support, psychological well-being, decision making, empowerment, infant and young child feeding, and nutritional status in Ugandan children ages 0 to 24 months. Matern Child Nutr. 2018;14(e12483):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Imai KS, Annim SK, Kulkarni VS, Gaiha R. Women's empowerment and prevalence of stunted and underweight children in rural India. World Dev. 2014;62:88–105. [Google Scholar]
- 105. Lépine A, Strobl E. The effect of women's bargaining power on child nutrition in rural Senegal. World Dev. 2013;45:17–30. [Google Scholar]
- 106. Maffioli D, Sacco P, Gabrielli G. Women's position in the family and child nutritional status in several Asian and African Countries. XXVI IUSP International Population Conference; Marrakech; 2009. [Google Scholar]
- 107. Malapit HJL, Sraboni E, Quisumbing AR, Akhter A. Gender empowerment gaps in agriculture and children's well-being in Bangladesh[Internet]. Report no. 2688064.Rochester (NY): Social Science Research Network; 2015 [cited 2019 Jan 30]. Available from: http://papers.ssrn.com/abstract = 2688064. [Google Scholar]
- 108. Malapit HJL, Quisumbing AR. What dimensions of women's empowerment in agriculture matter for nutrition in Ghana?. Food Policy. 2015;52:54–63. [Google Scholar]
- 109. Malapit HJL, Kadiyala S, Quisumbing AR, Cunningham K, Tyagi P. Women's empowerment mitigates the negative effects of low production diversity on maternal and child nutrition in Nepal. J Dev Stud. 2015;51:1097–123. [Google Scholar]
- 110. Malhotra C, Malhotra R, Ostbye T, Subramanian SV. Maternal autonomy and child health care utilization in India: results from the National Family Health Survey. Asia Pac J Public Health. 2014;26:401–13. [DOI] [PubMed] [Google Scholar]
- 111. Mashal T, Takano T, Nakamura K, Kizuki M, Hemat S, Watanabe M, Seino K. Factors associated with the health and nutritional status of children under 5 years of age in Afghanistan: family behaviour related to women and past experience of war-related hardships. BMC Public Health. 2008;8:301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Merchant SS, Udipi SA. Positive and negative deviance in growth of urban slum children in Bombay. Food Nutr Bull. 1997;18:(4):1–14. [Google Scholar]
- 113. Na M, Jennings L, Talegawkar SA, Ahmed S. Association between women's empowerment and infant and child feeding practices in sub-Saharan Africa: an analysis of Demographic and Health Surveys. Public Health Nutr. 2015;18:17:3155–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Patel A, Leonard W, Reyes-García V, McDade T, Huanca T, Tanner S, Vadez V. Parental preference, bargaining power, and child nutritional status: evidence from the Bolivian Amazon. Tsimane' Amazonian Panel Study Working Papers. 2007, No. 31. [Google Scholar]; Evanston: (IL): Department of Anthropology, Northwestern University. [Google Scholar]
- 115. Radebe BZ, Brady P, Siziya S, Todd H. Maternal risk factors for childhood malnutrition in the Mazowe District of Zimbabwe. Cent Afr J Med. 1996;42:240–4. [PubMed] [Google Scholar]
- 116. Rahman MM, Saima U, Goni MA. Impact of maternal household decision-making autonomy on child nutritional status in Bangladesh. Asia-Pac J Public Health Asia-Pac Acad Consort Public Health. 2015;27:509–20. [DOI] [PubMed] [Google Scholar]
- 117. Rajaram R, Perkins JM, Joe W, Subramanian SV. Individual and community levels of maternal autonomy and child undernutrition in India. Int J Public Health. 2017;62:327–35. [DOI] [PubMed] [Google Scholar]
- 118. Ross-Suits HM. Maternal autonomy as a protective factor in child nutritional outcome in Tanzania[Internet]. [Thesis Paper 99] Georgia State University; 2010. Available from: https://scholarworks.gsu.edu/iph_theses/99/. [Google Scholar]
- 119. Roushdy R. Intrahousehold resource allocation in Egypt: does women's empowerment lead to greater investments in children?. [Internet].Economic Research Forum; 2004; [cited 2017 Mar]. Available from: https://www.researchgate.net/profile/Mohamed_Marouani/publication/5081272_The_Impact_of_the_Multifiber_Agreement_Phaseout_on_Unemployment_in_Tunisia_A_Prospective_Dynamic_Analysis/links/09e4150b359a615d5d000000.pdf#page = 306. [Google Scholar]
- 120. Sabarwal S, McCormick MC, Silverman JG, Subramanian SV. Association between maternal intimate partner violence victimization and childhood immunization in India. J Trop Pediatr. 2012;58:107–13. [DOI] [PubMed] [Google Scholar]
- 121. Salazar M, Högberg U, Valladares E, Persson L-Å. Intimate partner violence and early child growth: a community-based cohort study in Nicaragua. BMC Pediatr. 2012;12:82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Sethuraman K, Lansdown R, Sullivan K. Women's empowerment and domestic violence: the role of sociocultural determinants in maternal and child undernutrition in tribal and rural communities in South India. Food Nutr Bull. 2006;27:128–43. [DOI] [PubMed] [Google Scholar]
- 123. Sethuraman K. The role of women's empowerment and domestic violence in child growth and undernutrition in a tribal and rural community in south India. [research paper]. [Internet].Helsinki: UNU-WIDER: 2008 [cited 2015 Aug 28], Available from: https://www.wider.unu.edu/sites/default/files/rp2008-15.pdf. [Google Scholar]
- 124. Shroff M, Griffiths P, Adair L, Suchindran C, Bentley M. Maternal autonomy is inversely related to child stunting in Andhra Pradesh, India. Matern Child Nutr. 2009;5:64–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Shroff MR, Griffiths PL, Suchindran C, Nagalla B, Vazir S, Bentley ME. Does maternal autonomy influence feeding practices and infant growth in rural India?. Soc Sci Med. 2011;73:447–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Siddhanta A, Chattopadhyay A. Role of women's empowerment in determining child stunting in eastern India and Bangladesh. Soc Sci Spectr. 2017;3:38–51. [Google Scholar]
- 127. Simon D, Adams AM, Madhavan S. Women's social power, child nutrition and poverty in Mali. J Biosoc Sci. 2002;34:193–213. [DOI] [PubMed] [Google Scholar]
- 128. Sipsma H, Callands TA, Bradley E, Harris B, Johnson B, Hansen NB. Healthcare utilisation and empowerment among women in Liberia. J Epidemiol Community Health. 2013;67:953–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Smith LC, Ramakrishnan U, Ndiaye A, Haddad L, Martorell R. The importance of women's status for child nutrition in developing countries [Internet]. International Food Policy Research Institute; 2003; [cited 2015 Aug 27]. Available from: https://core.ac.uk/download/pdf/6289649.pdf. [Google Scholar]
- 130. Tariku A, Alemu K, Gizaw Z, Muchie KF, Derso T, Abebe SM, Yitayal M, Fekadu A, Ayele TA, Alemayehu GA. Mothers’ education and ANC visit improved exclusive breastfeeding in Dabat Health and Demographic Surveillance System Site, northwest Ethiopia. PLoS One. 2017;12:e0179056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. Trapp EM. How social factors and maternal empowerment affect sex-equality and child well-being in Bangladesh, [doctoral thesis submitted to University of Colorado Department of Sociology]2006. [Google Scholar]
- 132. Ueyama M. Effects of women's agriculture on child health in rural Malawi: “Food Security Effect” and “Bargaining Effect”. [Internet]. Japan Society for the Promotion of Science. Hitotsubashi University. 2006[cited 2017 Dec 12]. Available from: http://www.csae.ox.ac.uk/conferences/2006-EOI-RPI/papers/csae/Ueyama.pdf. [Google Scholar]
- 133. Wado YD, Afework MF, Hindin MJ. Childhood vaccination in rural southwestern Ethiopia: the nexus with demographic factors and women's autonomy. Pan Afr Med J. 2014;17(Suppl 1):9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Woldemicael G, Tenkorang EY. Women's autonomy and maternal health-seeking behavior in Ethiopia. Matern Child Health J. 2010;14:988–98. [DOI] [PubMed] [Google Scholar]
- 135. Zereyesus YA, Amanor-Boadu V, Ross KL, Shanoyan A. Does women's empowerment in agriculture matter for children's health status? Insights from borthern Ghana. Soc Indic Res. 2017;132:1265–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Ziaei S, Contreras M, Zelaya Blandon E, Persson L-A, Hjern A, Ekstrom E-C. Women's autonomy and social support and their associations with infant and young child feeding and nutritional status: community-based survey in rural Nicaragua. Public Health Nutr. 2015;18:1979–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137. World Bank. Country data [Internet]. [cited 2019 Apr 27]. Available from: https://data.worldbank.org/country. [Google Scholar]
- 138. Ganle JK, Dery I. ‘‘What men don't know can hurt women's health’’: a qualitative study of the barriers to and opportunities for men's involvement in maternal healthcare in Ghana. Reprod Health. 2015;12:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Barker GT, Ricardo C, Nascimento M. Engaging men and boys in changing gender-based inequity in health: evidence from programme intevrentions[Internet]. Geneva: World Health Organizatio;2007; [cited 2015 Dec 1]. Available from: http://www.who.int/iris/handle/10665/43679. [Google Scholar]
- 140. Pratley P. Associations between quantitative measures of women's empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Soc Sci Med. 2016;169:119–31. [DOI] [PubMed] [Google Scholar]
- 141. Lemke S, Benade AJA. Black South African households, gender relations and food and nutrition security. South Afr J Clin Nutr. 2000;13:106. [Google Scholar]
- 142. Humphries S, Classen L, Jiménez J, Sierra F, Gallardo O, Gómez M. Opening cracks for the transgression of social boundaries: an evaluation of the gender impacts of farmer research teams in Honduras. World Dev. 2012;40:2078–95. [Google Scholar]
- 143. Bezner Kerr R, Chilanga E, Nyantakyi-Frimpong H, Luginaah I, Lupafya E. Integrated agriculture programs to address malnutrition in northern Malawi. BMC Public Health. 2016;16:1197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. O'Laughlin B. A bigger piece of a very small pie: intrahousehold resource allocation and poverty reduction in Africa. Dev Change. 2007;38:21–44. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.