

Abstract
Introduction
In the USA, nearly one in three people will experience herpes zoster (HZ) in their lifetime. Underserved communities may be at even higher risk due to several factors, including access to healthcare, education, and co-morbid conditions. The purpose of this study was to investigate current knowledge, attitudes, beliefs and practices (KABP) relative to HZ and HZ vaccines in a large urban city.
Methods
A cross-sectional KABP survey was conducted via in-person interview among 381 participants aged ≥ 50 years in Detroit, MI, USA, from June to August 2018. Survey results were stratified into two groups [< 60 and ≥ 60 years of age (YO)] for comparison.
Results
Of the 381 participants, 373 reported their age (110 < 60 YO and 263 ≥ 60 YO). Overall, the majority of participants reported having heard of HZ and HZ vaccines. In addition, receiving a recommendation from a healthcare provider (37.5%) followed by gaining a better understanding of HZ vaccine (36.7%) and of HZ (29.9%) were leading factors that influenced participants’ willingness to receive the vaccine. Of note, 65.5% of participants < 60 YO reported the belief that HZ is preventable versus only 53.2% in those ≥ 60 YO (p = 0.001).
Conclusion
Our findings underscore the need to educate patients in underserved communities about HZ as well as new HZ vaccine recommendations to improve vaccination rates and reduce the incidence of HZ and its associated sequelae.
Electronic supplementary material
The online version of this article (10.1007/s40121-019-00269-2) contains supplementary material, which is available to authorized users.
Keywords: Herpes zoster, Shingles, Survey, Vaccination
Introduction
Herpes zoster (HZ), or shingles, results from reactivation of the varicella-zoster virus. It is estimated that one out of every three people in the USA will develop HZ during their lifetime, and 13% of people ≥ 60 years of age will develop post-herpetic neuralgia (PHN), which can significantly reduce quality of life [1]. Despite the recognized burden of HZ and PHN, HZ vaccination rates in the US remain low. Whites have significantly higher HZ vaccination rates (37.7%) compared with Asians (21.9%), Hispanics (21.4%) and African Americans (15.7%) [2]. Additional factors such as education, household income and existing relationship with a healthcare provider have been independently associated with HZ vaccination [3]. Such disparities in HZ immunization rates may reflect the interrelationship of health and socioeconomic disparities between these racial/ethnic groups found across the US [4].
In October 2017, the US Food and Drug Administration approved a new recombinant zoster vaccine, Shingrix® (GlaxoSmithKline, Rixensart, Belgium). Evidence shows the efficacy of Shingrix® against HZ at 97%, a substantial improvement from 51% displayed by the live zoster vaccine, Zostavax® (Merck & Co., Inc., Whitehouse Station, NJ, USA), the only HZ vaccine available in the US prior the approval of Shingrix® [5, 6]. Increasing patient uptake of this new and more effective vaccine has potential to significantly reduce HZ disease burden. Thus, it is important to gauge patient understanding of HZ and HZ vaccines, particularly in disadvantaged populations that suffer from health disparities. In this report, we assess knowledge, attitudes, beliefs and practices (KABP) among people residing in a large urban American city with a high proportion of medically underserved individuals and families to identify potential opportunities to improve HZ awareness and vaccine uptake.
Methods
Study Overview
A KABP survey was developed, and convenience sampling was conducted at four different locations (two large retail stores located in the city’s suburban neighborhoods and two community centers located in combined commercial/residential districts) in Detroit, MI, USA. This city was chosen because it houses the institution conducting the study and is demographically characteristic of an underserved area with significant healthcare disparities. According to the US Health Resources & Services Administration, Detroit is a federally designated health professional shortage area for primary care, and nearly every square mile of the city is designated as a medically underserved area [7]. The city’s population is just over 670,000 residents, 79.1% of whom are Black or African American, 9.9% White and 7.6% Hispanic or Latinx [8]. In addition, the median household income in Detroit in 2017 was $27,838, and 37.9% of its residents live in poverty [8].
Participants were recruited via flyers and/or approached in person by study personnel, and verbal agreement to participate in the survey was obtained. All participants received a study information sheet. Upon verbal consent and confirmation that their age was ≥ 50 years by study personnel (participants asked: “are you 50 years or older?” and this question was included in the demographic section of the survey), study personnel then performed a face-to-face interview using a paper-based survey instrument. After completing the survey, participants received HZ-based educational handouts and a $10.00 gift card to a local retailer. People who had never heard of shingles were excluded from this study. The Wayne State University Institutional Review Board reviewed and approved this study (reference no. 043918B3X). This study conformed with the Helsinki Declaration of 1964, as revised in 2013, concerning human and animal rights, and Springer’s policy concerning informed consent has been followed.
Survey Instrument
The survey is available in the supplementary material and consisted of 42 multiple-choice items. It consisted of five sections: demographic, knowledge (20 items), attitudes (11 items), beliefs and influence of practice toward HZ vaccines (11 items). HZ was referred to as ‘shingles’ in the survey. Participants were instructed to completely answer each item based on their current knowledge.
Data Collection and Statistical Analysis
Sample size estimation assumed a statistical power of 0.8 and a confidence level of 95% (alpha = 0.05). Assuming a target population of 209,409 aged ≥ 50 years in Detroit, and an overall response rate of at least 80%, we estimated a required sample size of 350 individuals. Surveys were administered by trained key personnel from June to August 2018. Answers from paper-based surveys were transcribed into the Research Electronic Data Capture (REDCap) tool (est. 2004 Vanderbilt University, Nashville, TN) and analyzed using SPSS (ver. 24) statistical analysis software (2016; IBM Corp. Armonk, NY). Univariate (chi-square or Fisher’s exact test) analyses were used to describe patterns of KABPs among participants. A p value < 0.05 was considered significant.
Results
Participant Demographics
Three hundred eighty-one participants completed the survey, and of these 373 provided information on age. Sixty-five percent (n = 241) of participants were female, and 90.3% (n = 344) were Black or African American. Participants were stratified into two groups [age < 60 or ≥ 60 years old (YO); Fig. 1]. This age cutoff was chosen to allow for better understanding of zoster knowledge, behaviors and practices among those at lower or greater risk for HZ [1].
Fig. 1.
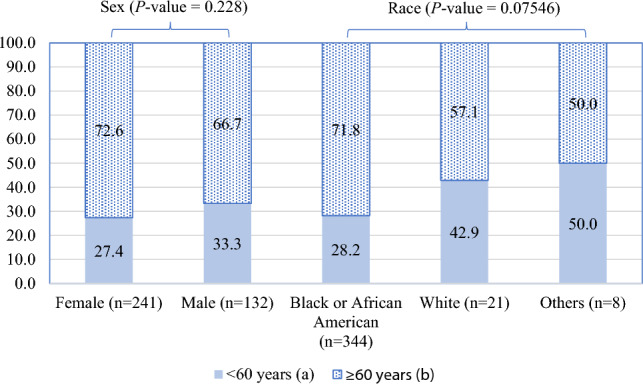
Demographic characteristics of participants (%) by age group. aMean (standard deviation): 54.4 (3.1) years. Range 50–59 years. bMean (standard deviation): 68.3 (6.6) years. Range 60–92 years
Knowledge of HZ and HZ Vaccines
When asked “do you think that shingles is common in the US,” the majority of both groups (< 60 YO and ≥ 60 YO) chose “yes” (69.1% and 68.5%). The majority also reported knowing at least one person who had HZ in the past (68.2% and 68.4%); 13.3% of participants ≥ 60 YO had reported experiencing HZ personally compared with only 8.2% of participants < 60 YO. The majority of both groups knew that HZ is a nerve/skin disease (96.4% and 93.1%), and that adults aged ≥ 50 years had a higher risk of HZ (69.1% and 66.9%) than those < 50 years. Participants of both age groups selected post-herpetic neuralgia (PHN) as the most common complication of HZ (40.4% and 44.4%) followed by rash (39.7% and 33.2%). Participants of both age groups knew that HZ can be recurrent (61.8% and 58.6%) and that HZ is not transmitted person to person (49.1% and 56.3%).
Most participants of both groups (< 60 YO and ≥ 60 YO) had heard of the HZ vaccine (Fig. 2). The most common information source for hearing about the HZ vaccine was television or internet advertisements (36.0% and 37.2%) followed by their doctor (25.2% and 31.4%) and their pharmacist (9.7% and 14.2%). Interestingly, a significantly higher proportion of respondents < 60 YO (62.7%) felt that the HZ vaccine was associated with side effects versus those ≥ 60 YO (39.2%; p < 0.001), and 35% (29.1% in < 60 YO and 36.9% in ≥ 60 YO) of overall participants did not know that the HZ vaccine was associated with any side effects.
Fig. 2.

Knowledge of herpes zoster vaccines
Attitudes and Beliefs Toward HZ and HZ Vaccines
Most participants of both groups believed that HZ can be treated (92.7% and 93.9%). Of those, 67.6% of participants < 60 YO thought treatments were safe and effective compared with 71.3% of participants ≥ 60 YO. Over half of participants of both groups thought HZ is curable (60.0% and 63.1%). However, only 53.2% of participants ≥ 60 YO thought HZ is preventable compared with 65.5% of participants < 60 YO (p = 0.001). About 18% of both groups thought that it was very unlikely that they could experience shingles while only 12% thought they were very likely to get shingles, now or in the future. Most participants thought that the pain associated with HZ is serious (67.3% and 60.5%).
In questions related to vaccine safety and efficacy, > 50% of participants of both groups believed that HZ vaccines were safe and effective. Additional survey data related to attitudes and beliefs are shown in Fig. 3.
Fig. 3.

Attitudes and beliefs regarding shingles and shingles vaccines
Practices Toward HZ and HZ Vaccines
Only 19.1% of participants < 60 YO indicated that they received a recommendation for a shingles vaccine from their healthcare provider versus 43.3% of participants ≥ 60 YO (p = 0.000) (Table 1). Willingness to receive the shingles vaccine was reported among 46.4% of participants < 60 YO compared with 50.2% in participants ≥ 60 YO (p = 0.750). In addition, a high proportion of participants in both the younger and older age groups expressed a willingness to seek more information from a healthcare provider about the shingles vaccine (84.5% in < 60 YO vs. 87.1% in ≥ 60 YO).
Table 1.
Practices toward herpes zoster and herpes zoster vaccines
| Characteristic | N | Age (years) | P value | |
|---|---|---|---|---|
| < 60 n (%) |
≥ 60 n (%) |
|||
| Did your doctor/pharmacist or other healthcare provider ever recommend you to be vaccinated with the shingles vaccine? | ||||
| Yes | 135 | 21 (19.1) | 114 (43.3) | 0.000 |
| No | 238 | 89 (80.9) | 149 (56.7) | |
| All other things being equal, if you are offered a shingles vaccine that is 97.2% protective and requires two doses gives 2 months apart (vaccine #1) or a shingles vaccine that is 51.3% protective and requires one dose (vaccine #2), which vaccine would you choose? | ||||
| Vaccine #1 | 313 | 97 (88.2) | 216 (82.1) | 0.200 |
| Vaccine #2 | 52 | 10 (9.1) | 42 (16.0) | |
| Others | 8 | 3 (2.7) | 5 (1.9) | |
We asked both age groups whether they would be willing to receive the vaccine based on a recommendation from three different healthcare professionals: a doctor, a nurse and a pharmacist; 71.8% of participants < 60 YO and 73.0% of those ≥ 60 YO stated they would based on a doctor’s recommendation followed by recommendation from a nurse (53.6% and 54.0%) and, lastly, a recommendation from a pharmacist (48.2% and 45.6%), respectively. No significant differences were found in willingness to take healthcare provider recommendations when comparing the two age groups.
When given the choice between “vaccine #1 (97.2% protective, requiring two doses 2 months apart) vs. vaccine #2 (51.3% protective, requiring one dose),” 88.2% of respondents < 60 YO selected vaccine #1 compared with 82.1% of respondents ≥ 60 YO (p = 0.200).
Regarding vaccine cost, 31.4% of participants reported willingness to receive the vaccine only if it were provided free of charge. Thirty-six percent of participants were willing to pay up to $24.99 USD, and 18.7% were willing to pay $25.00 to 50.00 USD. One-hundred forty-three (37.5%) participants reported that a recommendation by a healthcare provider was the most important factor that would change their decision to receive the vaccine followed by gaining a better understanding of the vaccine (36.7%), gaining a better understanding of the disease (29.9%), reduced cost of the vaccine (11.8%) and “other” factor(s) (3.7%).
Discussion
In a representative sample of medically underserved and socioeconomically challenged participants, knowledge, attitudes, beliefs and practices regarding HZ and HZ vaccines were highly variable. These findings are consistent with existing studies, including those in characteristically different populations [9–11].
Our results demonstrate that provider recommendations play a vital role in promoting HZ vaccination by positively influencing willingness to receive the vaccine. This concept has been displayed in a similar study by Teeter et al., which found that among 681 participants, there was over a fivefold increase in likelihood of vaccination if they received a recommendation from a healthcare provider [12]. It should be noted however that the majority of participants in this study were white and unvaccinated. Our study provides a unique perspective, as it is the only survey on HZ and HZ vaccines, to our knowledge, that was conducted in an underserved, urban environment with a socioeconomically challenged population.
Despite the importance of provider recommendations, only 36.1% of survey respondents reported receiving a recommendation for the shingles vaccine from their healthcare provider, representing a significant missed opportunity to more frequently and effectively educate eligible patients [13]. Furthermore, despite a lower recommendation acceptance rate compared with doctors and nurses, pharmacists’ ability to provide vaccinations and their increased accessibility compared with other healthcare providers represent another opportunity for patient education. Efforts that provide training to pharmacists in vaccine communication with patients and caregivers may help reduce missed vaccination opportunities at the pharmacy level.
In the US and other countries, the high cost of the HZ vaccine is a well-established barrier to vaccination [14]. However, results of our study revealed that reducing the cost of the HZ vaccine was only the fourth most important factor that would change participants’ decision to receive the vaccine, when given the choice of the following factors: recommendation by a healthcare provider, gaining a better understanding of the HZ vaccine, gaining a better understanding of HZ, reduced cost of the vaccine and ‘other.’ These data suggest that vaccine cost is not the sole reason for the inability to receive HZ vaccination among patients in medically underserved communities. Other reasons for not receiving HZ vaccination include important factors such as having adequate insurance coverage and access to transportation.
The efficacy of existing vaccines against HZ and the number of doses required were found to be other important factors in willingness to receive vaccinations. Given efficacy rates and dose series requirements of the two HZ vaccines currently utilized, the vast majority of participants stated they would choose the option with a higher efficacy rate, even if it required two doses instead of just one. This shows that providing patients basic evidentiary information on vaccines can be a major tool to overcome the barrier of multiple-dose requirements, even in the medically underserved.
A few limitations apply to our study. First, our survey was investigator-created and non-validated. Survey responses were self-reported and are thus susceptible to recall bias. In addition, although the survey was conducted in a medically underserved demographic, we were unable to verify the educational background and/or socioeconomic status of each participant, as this information was not collected. Lastly, because this survey was conducted in a primarily African American population, the results may be less representative of other populations with a predominance of other racial/ethnic groups.
Conclusion
Our findings contribute to understanding the KABPs regarding HZ and HZ vaccines in a sample of primarily African American persons in a medically underserved, socioeconomically challenged community. Our study suggests that lack of vaccine recommendations from healthcare providers may be a significant factor influencing low HZ vaccination rates in these communities. It is crucial to educate patients about HZ and its complications, as well as basic information regarding HZ vaccines, to improve vaccination rates and reduce the incidence of HZ. Future research should focus on continued identification of barriers to vaccination through KABP assessment in diverse populations and training all types of HCPs to improve the delivery and increase the frequency of recommendations for HZ vaccination to their patients.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgements
The authors would like to thank key personnel Adalah Yahia, Katherine Chuong, Mariam Hijazi, Mary Whitney, Maryam Al-Jazrawi, Mohamad Akil, Nesreen Altairy, Rana Aoun and Riham Mansour for their assistance with survey administration. The authors would also like to thank all survey respondents for participating in this study.
Funding
This work was supported by the Wayne State University Department of Pharmacy Practice Research & Development fund. No Rapid Service Fee was received by the journal for the publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Nour A. Baalbaki, Joseph P. Fava, Melanie Ng, Ezinwanne Okorafor, Asad Nawaz, Wesley Chiu, Abdulbaset Salim, Raymond Cha and Paul E. Kilgore have nothing to disclose. Paul E. Kilgore is an Editorial Board Member for the journal.
Compliance with Ethics Guidelines
The Wayne State University Institutional Review Board reviewed and approved this study (reference number: 043918B3X). This study conformed with the Helsinki Declaration of 1964, as revised in 2013, concerning human and animal rights, and Springer’s policy concerning informed consent has been followed.
Data Availability
The datasets generated during and/or analyzed during the current study are available in the Mendeley repository [http://dx.doi.org/10.17632/sykkm7rx4m.1].
Footnotes
Enhanced Digital Features
To view enhanced digital features for this article go to 10.6084/m9.figshare.9901172.
References
- 1.Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP) Morb Mortal Weekly Rep. 2008;57:1–30. [PubMed] [Google Scholar]
- 2.Saguil A, Kane S, Mercado M, et al. Herpes zoster and postherpetic neuralgia: prevention and management. Am Fam Physician. 2017;96(10):656–663. [PubMed] [Google Scholar]
- 3.Lu PJ, O’Halloran A, Williams WW, et al. National and state-specific shingles vaccination among adults aged >/=60 years. Am J Prev Med. 2017;52(3):362–372. doi: 10.1016/j.amepre.2016.08.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Williams DR, Mohammed SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med. 2009;32(1):20–47. doi: 10.1007/s10865-008-9185-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shingrix (Zoster Vaccine Recombinant, Adjuvanted). GlaxoSmithKline Biologicals, Rixensart, Belgium; 2017. https://gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Shingrix/pdf/SHINGRIX.PDF. Accessed 27 Sept 2019.
- 6.Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271–2284. doi: 10.1056/nejmoa051016. [DOI] [PubMed] [Google Scholar]
- 7.Map Tool: data.HRSA.gov. https://data.hrsa.gov/hdw/tools/MapTool.aspx. Accessed 19 Sept 2019.
- 8.QuickFacts: Detroit city, Michigan. United States Census Bureau. https://www.census.gov/quickfacts/detroitcitymichigan. Accessed 6 Dec 2018.
- 9.Paek E, Johnson R. Public awareness and knowledge of herpes zoster: results of a global survey. Gerontology. 2010;56(1):20–31. doi: 10.1159/000240046. [DOI] [PubMed] [Google Scholar]
- 10.Valente N, Lupi S, Stefanati A, et al. Evaluation of the acceptability of a vaccine against herpes zoster in the over 50 years old: an Italian observational study. BMJ open. 2016;6(10):e011539. doi: 10.1136/bmjopen-2016-011539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Joon Lee T, Hayes S, Cummings DM, et al. Herpes zoster knowledge, prevalence, and vaccination rate by race. J Am Board Fam Med. 2013;26(1):45–51. doi: 10.3122/jabfm.2013.01.120154. [DOI] [PubMed] [Google Scholar]
- 12.Teeter BS, Garza KB, Stevenson TL, et al. Factors associated with herpes zoster vaccination status and acceptance of vaccine recommendation in community pharmacies. Vaccine. 2014;32(43):5749–5754. doi: 10.1016/j.vaccine.2014.08.040. [DOI] [PubMed] [Google Scholar]
- 13.Nowalk MP, Zimmerman RK, Cleary SM, et al. Missed opportunities to vaccinate older adults in primary care. J Am Board Fam Pract. 2005;18(1):20–27. doi: 10.3122/jabfm.18.1.20. [DOI] [PubMed] [Google Scholar]
- 14.Hurley LP, Lindley MC, Harpaz R, et al. Barriers to the use of herpes zoster vaccine. Ann Intern Med. 2010;152(9):555–560. doi: 10.7326/0003-4819-152-9-201005040-00005. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available in the Mendeley repository [http://dx.doi.org/10.17632/sykkm7rx4m.1].