

Abstract
The original Rivermead Behavioural Memory Test (RBMT) suggests a cutoff global score of 10 points. However, this limit may be too stringent for older adults attending memory training programs, particularly for those with low education levels. This study aims to provide appropriately adjusted age and education norms for the RBMT. Data from 711 subjects were grouped based on age (65–67, 68–71, 72–75 and 76–83) and education level (primary school, high school and university studies). The data exhibit a clear trend of scores decreasing with age. The diminution in scores does not reach trend levels of significance between neighboring (< 5 years) age intervals, but it is statistically significant at the designated alpha level (p = .05) when younger and older adults are compared over a range of 5 years of difference. 81.86% of our sample has global scores below the suggested cutoff of 10 points. The present study provides a more accurate representation of RBMT global score performance in older adults for specific age and education stratifications.
Keywords: Everyday memory, RBMT, Older adults, Age, Instrumental study
Introduction
The Rivermead Behavioural Memory Test (RBMT) (Wilson et al. 1989) is a tool used to evaluate the functional capacity for independent living and to follow up treatments for everyday memory problems. This instrument predicts cognitive challenges that people face in their everyday lives and makes recommendations aimed at reducing their effects (Parsons et al. 2017). The subtests that form the test correspond to instrumental activities of daily life such as recalling names or places; remembering an appointment or a date; and immediate or delayed recognition of pictures, faces or stories selected from the study by Sunderland et al. (1984) and from the observations of older adults with cognitive decline from the Rivermead Rehabilitation Centre in Oxford. Like traditional tests, this test consists of tasks related to free recall, immediate and delayed memory, verbal and nonverbal tasks and assessments of personal, temporal and spatial orientation. In addition, it includes the evaluation of retrospective and prospective memory. The latter is a type of episodic memory that is not usually included in tests that evaluate mnemic processes (Rendell and Henry 2009). However, different studies suggest that prospective memory is affected by age, and its evaluation allows for discernment between subjects with normal memory and subjects with mild cognitive decline (Matsuzono et al. 2015). The subtests that assess prospective memory in the RBMT are: recall of an appointment, recall of belongings and recall of a message.
The RBMT has high ecological validity, which has been demonstrated in terms of both likelihood (the degree of similarity between the cognitive task involved in the test and the cognitive demand of everyday tasks) (Spooner and Pachana 2006) and veracity (the degree to which existing tests are statistically related to other tests that predict everyday functioning) (Chaytor and Schmitter-Edgecombe 2003). It is easy to understand, use, interpret and apply in a wide variety of contexts, and it has four versions that avoid the effect of repeated administrations. Regarding differential diagnosis, the RBMT has demonstrated usefulness in differentiating, like the traditional tests, subjects with different diagnoses, and in classifying subjects with or without mnemic decline (McAlister and Schmitter-Edgecombe 2016). Concerning the comparison between the RBMT and traditional memory tests, significant correlations are obtained with the Wechsler Memory Scale Revised (WMS-R) (Wechsler 1987), the memory scale of the Luria-Nebraska neuropsychological battery (Golden et al. 1985), the Benton Visual Retention Test (Benton et al. 1986) and the memory subscales of the Cambridge Cognitive Exam (CAMCOG) (García-Martínez and Sánchez-Cánovas 1994; Wilson et al. 1989; Yassuda et al. 2010). In addition, the correlation of the RBMT with the Mini-Mental State Examination (MMSE) (Folstein et al. 1975) suggests that its routine application is useful in cases where cognitive decline is suspected. In addition, it shows sufficient sensitivity and specificity in discerning between normal subjects and those with mild cognitive impairment (MCI) and Alzheimer’s disease (Bolló-Gasol et al. 2014; Yassuda et al. 2010). On the other hand, the correlation between the execution of the subtests and the observations made by therapists addressing memory lapses in older adults reinforces its validity to be used genuinely as a test to identify mnemic deficits in daily life (Alonso and Prieto 2004; Requena et al. 2016; Wilson et al. 1989).
The RBMT has proven psychometric properties, and it combines the scientific rigor of traditional standardized tests with observational techniques. The original validation of the RBMT was initially performed with subjects between 14 and 70 years old and, subsequently, in subjects over the age of 70, including 114 subjects between 70 and 94 years old (mean age = 80.49 ± 5.22 years; mean number of years of schooling = 9.51 ± 1.66) who obtained profile scores of 15.54 ± 5.54 and global scores of 6.57 ± 2.93. The results show that age and level of schooling correlate with the profile total scores of the original RBMT. In addition, studies conducted with the RBMT with older people of different cultures, pathologies and educational levels show mean test scores lower or higher than the original study by Wilson et al. (1989). In contrast, with demographic factors such as sex, no significant differences were found in the RBMT (Strauss et al. 2006; Wilson et al. 1989; Adachi et al. 2013; Huppert and Beardsall 1993; Kazui et al. 2005; Salorio et al. 2004; Wilson et al. 1989; Yassuda et al. 2010). Therefore, it is necessary to obtain normative scores for each population to which the RBMT will be applied and sociodemographic corrections when necessary.
In Spain, the original study was replicated with healthy subjects older than 70 (mean age = 79.2 ± 7.02 years) with the Spanish translation of Mozaz (1991) to categorize the profile scores. However, the study has methodological problems such as the small sample size, the facts that a screening test is not applied in the selection of the sample to differentiate between normal and pathological subjects and that the normative data are obtained from the profile scores but not from the global scores, and how it is not explained how the effect of schooling is controlled in the total profile score of the RBMT. Along the same line, a normative study of the RBMT for a Brazilian sample concluded that education and age significantly determine the profile scores of the RBMT with data similar to the original study (Steibel et al. 2016). Other subsequent studies performed with the Spanish population have been carried out in a clinical setting to assess the usefulness of the RBMT for the diagnosis and follow-up of healthy and MCI conditions in older adults. The profile and global scores obtained in the RBMT make it possible to differentiate between subjects with cognitive deterioration and healthy subjects (of the same age, sex and level of schooling), correctly classifying 98% of the subjects with MCI and 96% of the healthy subjects (Bolló-Gasol et al. 2014). Notice that the profile scores shown by the RBMT make it possible to distinguish healthy subjects from subjects with mild cognitive impairment based on subtests for episodic, prospective, retrospective, visuospatial, orientation and recognition memory. Therefore, until now the normative scores for the RBMT with the healthy older population have been profile scores. In addition, studies that evaluate global scores for older adults establish differential diagnoses between healthy older adults and those with memory disorders (Yassuda et al. 2010)
The current research is part of a wider longitudinal study about the effect of cognitive stimulation programs on the functionality of healthy older adults in León, Spain, and its province. We have observed how memory training programs have proliferated in community contexts outside clinical and research areas, specifically in senior centers. One of the limitations of the program applied in this context is the lack of scientific rigor regarding sample selection, type of design or follow-up evaluation. In this sense, the study aims to provide normative data for the global (or functional) scores of the RBMT, stratified by age and educational level in healthy older adults who attend memory training programs in senior centers of their community.
Method
Participants
The study sample is part of a larger research project whose objective is the longitudinal follow-up of the effect of a memory training program on healthy older adults. The study was approved by the Ethics Committee of the Chair of Aging in All Ages of the University of León in 2016 and was carried out following the deontological standards recognized by the Declaration of Helsinki of 1975 (revised at the 52nd General Assembly in Edinburgh, Scotland, October 2000), the standards of Good Clinical Practice and compliance with Spanish legislation and regulations that regulate clinical research in humans (Royal Decree 223/2004 on regulation of clinical trials).
The study was carried out with people older than 65 living in the community who were recruited in the senior centers of the León and Ponferrada City Councils. The exclusion criteria were: psychiatric and neurological diagnosis, a score in the Barthel of 80 or more points according to the scale of dependence rating (Royal Legislative Decree 504/2007). The following evaluation instruments were administered as inclusion criteria: the Mini Cognitive Examination (MCE) (Lobo et al. 1980; Lobo 1987) with a cutoff point of 28 points to ensure that the population was cognitively healthy (Stephan et al. 2013), the Geriatric Depression Scale (GDS) with a cutoff point of 10 points (Ramos et al. 1993) and the Memory Failure Questionnaire in Everyday Life (MFE) (Baddeley 1990) which includes 28 items about everyday situations and activities.
Procedure
The RBMT (Wilson et al. 1989) consists of 12 subtests which resemble everyday life situations. The test has four versions to evaluate different types of memory: prospective, retrospective, visual, verbal, topographic, associative, recognition and personal spatial and temporal orientation. For this study, we applied the Spanish translation of the Mozaz test (1991), validated with the Wechsler Memory Scale Revised (WMS-R) (Wechsler 1987). The RBMT correction allows us to obtain three different scores: direct, profile and global. While the direct score of each subtest follows the correction guidelines without any modifications, profile and global scores are obtained from direct scores. Direct scores are transformed into dichotomous scores by assigning the value (1) to each correct subtest and (0) to each incorrect one. The total score is the sum of the scores obtained on the different subtests, with the exception of item 6 in which one point involves remembering six ideas of immediate memory from a story and four ideas of delayed memory, and item 9 in which one point is obtained if the subject spontaneously remembers the message in both immediate and delayed memory. The total score in this study is obtained from the sum of all the total scores obtained in the different subtests, and it ranges from 0 to 12 points based on the following items: name, surname, pictures, faces, stories, appointment, immediate route, delayed route, message, orientation, date and personal belongings. The application and correction norms of the RBMT are suitable for older adults; however, the standardized cutoff points show lower scores according to age and level of schooling (Bolló-Gasol et al. 2014).
The MEC-35 (Lobo et al. 1980; Lobo 1987) is the Spanish version of the MMSE (Folstein et al. 1975). This test is broadly used to quantify cognitive decline or cognitive status and its long-term progression. Cognitive status is assessed using tasks including orientation, attention, concentration, language, calculations, constructive praxis and working memory.
The GDS (Yesavage et al. 1983) is a well-known scale used to evaluate the mood of older adults. It consists of 30 items that require dichotomous answers. It has been accepted and validated for geriatric Spanish populations. The sensitivity and specificity of the GDS are about 95% (Ramos et al. 1993).
The MFE (Sunderland et al. 1984) includes 28 items that mimic everyday situations and actions. The subjective evaluation of memory was carried out using the Memory Failures of Everyday (MFE) questionnaire by Sunderland et al. (1984), which includes 28 items that mimic everyday situations and activities. Scores are presented on a three-point scale (0 = never, rarely; 1 = occasionally, sometimes; 2 = frequently, often). In the Spanish version, the coefficient α calculated was 0.83 Lobo 1987. Other authors have obtained similar results with different samples (Montejo et al. 2006; Garamendi et al. 2010). We used the Spanish language version that appears in Baddeley’s work (1990) because it is the most widely utilized in Spanish language research studies, social contexts and clinical practices (Montejo et al. 2011; Requena et al. 2009).
Statistical analyses
Descriptive statistical tests were performed in order to provide the demographic characteristics of the sample and a description of the performance in the test. The normative data of age and education level of the RBMT were obtained by stratifying the sample into four age groups (65–67, 68–71, 72–75 and 76–83) in order to balance the number of subjects in each group. They were subsequently classified into three education groups (primary, secondary and university) (see Table 1). To present the descriptive data by groups and analyze the effect of the factors of age groups, educational level and sex, a two-factor ANOVA was applied. The effect size was studied using the η2 statistic. Finally, the normative data of the RBMT were analyzed by age and education. The post hoc comparisons of the groups were carried out using the Tukey test. The percentage distribution of individuals who were below the normal cutoff point (X < 10) was 81.86%.
Table 1.
Age- and education-adjusted normative data for the RBMT and the MEC
| N | RBMT Mean ± SD | MEC Mean ± SD | |
|---|---|---|---|
| Age range | |||
| From 65 to 67 | 187 | 7.91 ± 2.12 | 29.52 ± 0.87 |
| From 68 to 71 | 187 | 7.35 ± 2.24 | 29.39 ± 0.91 |
| From 72 to 75 | 169 | 6.76 ± 2.35 | 29.24 ± 0.98 |
| From 76 to 83 | 168 | 6.91 ± 2.17 | 29.23 ± 1.12 |
| Education | |||
| Primary | 480 | 7.04 ± 2.29 | 29.30 ± 1.03 |
| Secondary | 136 | 7.96 ± 2.25 | 29.46 ± 0.96 |
| University | 95 | 7.30 ± 1.87 | 29.42 ± 6.12 |
Results
The study involved 711 subjects after excluding 68 volunteers who either did not meet any of the criteria for the study or rejected participating in it. The following are the characteristics of the study group: demographic: 617 women and 94 men aged between 65 and 83 years (mean = 71.76 years, standard deviation (SD): 5.05); educational level: 95 subjects with a university degree, 136 with studies equivalent to high school and 480 with primary studies; and marital status: 350 married, 290 widowed, 62 single and 9 divorced. The mean MCE score was 29.34 (± .97), GDS was 9.07 (± 4.89), and MFE was 18.71 (± 9.66).
The analyses show that age has a significant effect on the scores (F (1.6) = 7.947, p = .001); however, the size of the effect is only significant between the extreme age groups (η2 = 0.51 or η2 = 0.46), while the neighboring age groups show a very low effect size (η2 = 0.25 or η2 = − 0.06). These data should also be related to studies suggesting that there is an inflection point in the cognitive decline of healthy subjects (Livingston et al. 2017). Educational level also shows significant differences (F (1.6) = 6.362, p = .002), but in this case the differences are identified between the level of primary and secondary studies but not between the levels of extreme studies. The effect size between the scores in the RBMT and the level of studies confirms these same results (η2 = − 0.40, between the level of nearby studies and η2 = − 0.11, level of extreme studies) (see Table 2).
Table 2.
Multiple comparisons by age and education for the RBMT
| (I) Age ranges | (J) Age range | Mean comparison (I–J) | Standard error | p | Effect size |
|---|---|---|---|---|---|
| Age range | |||||
| From 65 to 67 | From 68 to 71 | .56 | .22 | .067 | 0.25 |
| From 72 to 75 | 1.15 | .23 | .001* | 0.51 | |
| From 76 to 83 | .99 | .23 | .001* | 0.46 | |
| From 68 to 71 | From 65 to 67 | − .56 | .22 | .067 | − 0.25 |
| From 72 to 75 | .58 | .23 | .058 | 0.25 | |
| From 76 to 83 | .43 | .23 | .247 | 0.19 | |
| From 72 to 75 | From 65 to 67 | − 1.15 | .23 | .001* | − 0.51 |
| From 68 to 71 | − .58 | .23 | .058 | − 0.25 | |
| From 76 to 83 | − .15 | .24 | .920 | − 0.06 | |
| From 76 to 83 | From 65 to 67 | − .99 | .23 | .001* | − 0.46 |
| From 68 to 71 | − .43 | .23 | .247 | − 0.19 | |
| From 72 to 75 | .15 | .24 | .920 | 0.06 | |
| Education | |||||
| Primary | Secondary | − .91 | .21 | .001* | − 0.40 |
| University | − .25 | .24 | .553 | − 0.11 | |
| Secondary | Primary | .91 | .21 | .001* | 0.40 |
| University | .65 | .29 | .067 | 0.31 | |
| University | Primary | .25 | .24 | .553 | 0.11 |
| Secondary | − .65 | .29 | .067 | − 0.31 | |
*Indicates the significance of p-value .001
Table 3 shows the means by age and education level, respectively, corresponding to the scores of the 12 items that make up the score of the global test of the RBMT. Figure 1 shows the means of these scores in descending order where it can be observed that the lowest scores are related to prospective memory.
Table 3.
Means for every item for the RBMT global test stratified by age and education
| Age range | Education level | ||||||
|---|---|---|---|---|---|---|---|
| From 65 to 67 | From 68 to 71 | From 72 to 75 | From 76 to 83 | Primary | Secondary | University | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Date | .64 ± .47 | .50 ± .50 | .48 ± .50 | .48 ± .50 | .51 ± .50 | .61 ± .48 | .52 ± .50 |
| Message | .59 ± .49 | .49 ± .50 | .46 ± .50 | .47 ± .50 | .48 ± .50 | .60 ± .49 | .50±.50 |
| Story | .57 ± .49 | .47 ± .50 | .50 ± .50 | .48 ± .50 | .49 ± .50 | .63 ± .48 | .43 ± .49 |
| Name | .67 ± .46 | .68 ± .46 | .62 ± .48 | .64 ± .47 | .62 ± .48 | .75 ± .43 | .69 ± .46 |
| Orientation | .63 ± .48 | .56 ± .49 | .47 ± .50 | .49 ± .50 | .51 ± .50 | .58 ± .49 | .61 ± .49 |
| Surname | .70 ± .45 | .68 ± .46 | .65 ± .47 | .68 ± .46 | .66 ± .47 | .67 ± .46 | .76 ± .42 |
| Pictures | .78 ± .41 | .73 ± .44 | .79 ± .40 | .75 ± .43 | .77 ± .41 | .74 ± .43 | .77 ± .41 |
| Faces | .77 ± .42 | .80 ± .39 | .66 ± .47 | .67 ± .47 | .73 ± .44 | .78 ± .41 | .66 ± .47 |
| Immediate route | .81 ± .38 | .77 ± .41 | .72 ± .44 | .70 ± .45 | .74 ± .43 | .77 ± .41 | .77 ± .41 |
| Delayed route | .71 ± .45 | .69 ± .46 | .55 ± .49 | .65 ± .47 | .64 ± .48 | .72 ± .44 | .64 ± .48 |
| Appointment | .40 ± .49 | .40 ± .49 | .37 ± .48 | .42 ± .49 | .39 ± .48 | .42 ± .49 | .40 ± .49 |
| Object | .58 ± .49 | .53 ± .50 | .42 ± .49 | .42 ± .49 | .45 ± .49 | .63 ± .48 | .50 ± .50 |
Fig. 1.
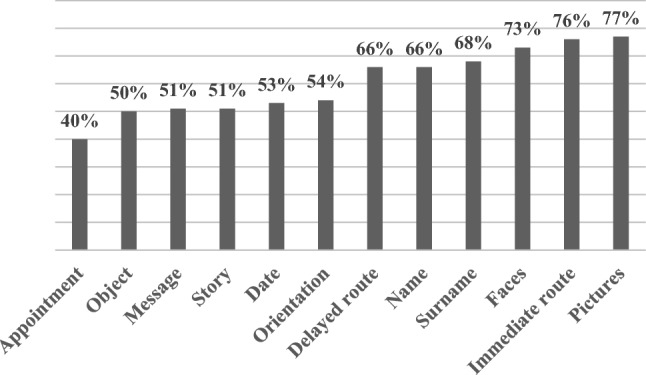
Items ranged by the number of correct responses for the RBMT
As shown in Fig. 2, in general, the performance of the study sample in the RBMT shows a distribution that is quite similar to a normal curve. Only some subjects are at the moderate level (three points) or at the normal level (12 points). Most subjects are identified in scores between six and eight points indicating a weak memory level according to the original cutoff point. In particular, the overall score of the RBMT was 7.26 (SD = 2.26), which is approximately three points lower than the cutoff point suggested by Wilson et al. (1989).
Fig. 2.
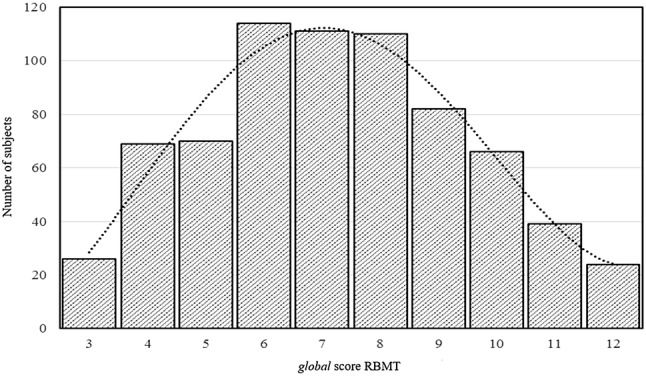
RBMT global score distribution for the whole sample
Discussion
The objective of this study was to provide normative data for the global score of the RBMT, stratified by age and educational level in healthy older adults. In particular, we intended to optimize the usefulness of the RBMT as a tool for evaluating memory training programs in community contexts. The data show that 81.86% of the participants were below the normal cutoff point of the original test. The highest scores were obtained by younger subjects (between 65 and 67 years old), and significant differences among age groups were manifested in age intervals of at least 5 years, but not in shorter temporal periods. These results confirm hypotheses and conclusions of other studies highlighting that memory capacity in older people with normal aging decreases with age (Alonso and Prieto 2004; Reijnders et al. 2013). Regarding the level of education, we found that there were significant differences between subjects with a secondary level of schooling and subjects with a low level of schooling, but not between these subjects and the ones with a higher education level. These results are consistent with the sample used by Wilson et al. (1989). This probably reflects the fact that, unlike the classic tests that are composed of abstract and decontextualized exercises, the RBMT ecological measure consists of exercises that simulate tasks of daily life (e.g., remembering faces, stories or dates). These kinds of tasks favor the performance of subjects with less schooling because they focus on what older people do with their memory capacities instead of focusing on how memory works and on providing data about the factors underlying the scores obtained (Rodríguez-Bailón et al. 2015; Parsons et al. 2017)
When comparing our results with previous studies carried out with the RBMT, we verified a tendency of these studies to show normative data with a profile score but not with a global score for a larger population (Alonso and Prieto 2004; Steibel et al. 2016). The profile scores of the RBMT are obtained from the sum of the scores of all the tasks valued between 0 and 2 points (two points indicate normal performance; one point indicates intermediate performance; and zero points indicate error on the task), while the global scores are obtained by evaluating each task as 1/0 (success/error). That is, in the application of the RBMT with a profile score, the evaluator is allowed to help the subject by providing clues. However, in the application of the test with a global score, no help is given to the subject. Therefore, the global scores but not the profile scores indicate the actual functional level of the subject with regard to the different types of memory (retrospective, prospective, immediate or long term, recognition and free) that are evaluated by the RBMT (Wilson et al. 1989). Profile scores have the diagnostic purpose of classifying between healthy subjects and those with memory impairments. For example, the study conducted by Alonso and Prieto 2004 with a Spanish sample classified between older adults with good versus deteriorating health by using the data profile score. The results showed that an increase in age is related to a decrease of up to three points in the profile scores of the extreme age groups (70–75 years and 80 years). Along this same line, a study conducted with a Brazilian sample (Steibel et al. 2016) used the RBMT test to classify everyday memory levels in healthy older adults; it showed a negative correlation between the profile scores in the RBMT and the age of the subjects, which ranged from 69 to 80 years. There was a difference of up to four points in the scores of these test subjects. Therefore, both studies showed a trend similar to the global scores obtained in our study. That is, clear differences in scores between extreme ages are established, and differences between neighboring ages are attenuated (see Table 3).
On the order hand, regarding previous studies carried out with the global score of the RBMT with the Spanish population, the research carried out by Bolló-Gasol et al. (2014) was aimed at assessing the usefulness of this score as a diagnosis and follow-up of subjects with cognitive impairments who progress to dementia. This study included a control group of 30 healthy subjects who obtained a global score of 7 (± 1.83) points compared to 5.91 (± 2.51) points obtained by subjects with cognitive impairments. This score is higher than that obtained in our study (6.76 ± 2.35) and is also higher than that obtained from the English population (6.57 ± 2.93) with which the original study of the RBMT was carried out. One possible explanation would be in the difference of age means of the samples in both studies. While in the study of Bolló-Gasol et al. (2014) the mean age of the participants was 72.9 ± 6.18, in our study the overall score in the RBMT corresponds to the age interval 72–75 and the mean age of the original sample was 80.49 ± 5.25. Note that in the revised RBMT studies there is a decrease in the score of older adults (Strauss et al. 2006). On the other hand, the global score of the RBMT among our subjects with a primary level of schooling was 7.04 points, similar to that obtained in the study conducted by Bolló-Gasol et al. (2014) 7 ± 1.83 in a population with a mean of 6 years of schooling. However, none of these values coincide with the values of the RBMT scores of the original study (Wilson et al. 1989). Therefore, the need for stratified norms that include age and education is emphasized.
Consequently, the results of the studies that used both profile and global scores suggest that a lower threshold is required to classify the memory levels of the healthy senior population, especially among the oldest adults. Even with the correction of the cutoff point being adjusted to the study sample (7.26), 54.8% of the participants in our research study obtained scores below this cutoff point. Therefore, we propose to use the normative data presented in Tables 1 and 3, which provide the means and standard deviations of the RBMT global scores stratified by age and educational level. Note that, while cutoff points are useful for quickly determining whether a subject may require a more in-depth assessment, normative points corrected for age and education provide a more refined estimation of cognitive performance, and they can help to reduce misclassification during the screening phase (Kopecek et al. 2017). It often happens that older people with different levels of education but similar functionality have different scores, which emphasizes the importance of taking into account age and education in the performance of memory tasks (Malek-Ahmadi et al. 2015). The results of our study constitute a clear example of the same functionality, and different ages, educational levels and memory performances. On the other hand, the lowest means of the subtests are related to prospective memory (see Fig. 2), a result that agrees with previous studies carried out with traditional memory tests (Libon et al. 2011; Martín et al. 2013) or with the RBMT (Kazui et al. 2005; Yassuda et al. 2010). This type of memory assesses the cognitive capacity to remember the performance of actions that will be performed in the future such as remembering to take medication or run errands (Costa et al. 2011; Niedzwienska et al. 2016). The subtest of remembering an appointment shows the lowest score despite hearing a warning signal. However, the signal has a low association with what the subject must remember (the appointment). In addition, the task that the subject is performing at the moment the signal sounds does not offer any clue about the memory demand of the subtest (Huppert and Beardsall 1993; Man et al. 2016; Mogle et al. 2017).
One of the strengths of the current study is that despite the greater number of female participants than male, the sample accurately resembles the gender ratio of older adults who usually go to senior centers to participate in memory training programs (Gross and Rebok 2011; Montejo 2003; McAvinue et al. 2013). On the other hand, different studies suggesting normative data for older adults using the RBMT have been carried out with an equally greater proportion of women than men (Araujo et al. 2010). In addition, no significant differences have been found regarding the sex variable and the RBMT scores (Adachi et al. 2013; Strauss et al. 2006; Wilson et al. 1989; Yassuda et al. 2010).
Taken together, our results emphasize the need for accurate normative data of the RBMT that should be applied by professionals who carry out memory training programs in community contexts. The use of demographically adjusted RBMT scores as well as the normative data of each subtest provides professionals with a more accurate estimate of the type of exercises that subjects participating in these types of programs need to train for. The weaknesses of the study appear when it comes to the generalization of its results, as the sample is representative of the population of older adults attending senior centers, and the number of male participants is low. However, the fact that even the group with the highest level of education presents scores below the normative level emphasizes the need for corrected education standards of these normative data. In future research, it is recommended that investigators determine whether the classification of these data (proposed as normative) corresponds to specific clinical diagnoses.
Footnotes
Responsible editor: Matthias Kliegel.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
C. Requena, Phone: +34 987 293143, Email: c.requena@unileon.es
P. Alvarez-Merino, Phone: +34 987 293143, Email: palvm@unileon.es
G. W. Rebok, Phone: +1 410-955-8550, Email: grebok1@jhu.edu
References
- Adachi H, Shinagawa S, Komori K, Toyota Y, Mori T, Matsumoto T, Sonobe N, Kashibayashi T, Ishikawa T, Fukuhara R, Ikeda M. Comparison of the utility of everyday memory test and the Alzheimer’s disease assessment scale-cognitive part for evaluation of mild cognitive impairment and very mild Alzheimer’s disease. Psychiatry Clin Neurosci. 2013;67(3):148–153. doi: 10.1111/pcn.12034. [DOI] [PubMed] [Google Scholar]
- Alonso M, Prieto P. Validación de la versión en español del test conductual de memoria de rivermead (RBMT) para población mayor de 70 años. Psicothema. 2004;16(2):325–328. [Google Scholar]
- Araujo FG, Ruiz DAD, Alemán MAA. Programa de entrenamiento cognitivo en adultos mayores. Rev Mex de Med Física y Rehabil. 2010;22(1):26–31. [Google Scholar]
- Baddeley A. Su memoria, cómo conocerla y dominarla. Madrid: Debate; 1990. pp. 22–23. [Google Scholar]
- Benton A, de la Cruz M, Pando A. TRVB: test de retención visual de Benton: manual. Madrid: Tea; 1986. [Google Scholar]
- Bolló-Gasol S, Piñol-Ripoll G, Cejudo-Bolivar JC, Llorente-Vizcaino A, Peraita-Adrados H. Ecological assessment of mild cognitive impairment and Alzheimer disease using the Rivermead Behavioural Memory Test. Neurología (English Edition) 2014;29(6):339–345. doi: 10.1016/j.nrleng.2013.07.001. [DOI] [PubMed] [Google Scholar]
- Chaytor N, Schmitter-Edgecombe M. The ecological validity of neuropsychological tests: a review of the literature on everyday cognitive skills. Neuropsychol Rev. 2003;13(4):181–197. doi: 10.1023/B:NERV.0000009483.91468.fb. [DOI] [PubMed] [Google Scholar]
- Costa A, Caltagirone C, Carlesimo G. Prospective memory impairment in mild cognitive impairment: an analytical review. Neuropsychol Rev. 2011;21(4):390–404. doi: 10.1007/s11065-011-9172-z. [DOI] [PubMed] [Google Scholar]
- Folstein M, Folstein S, McHugh P. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Garamendi F, Delgado DA, Amaya MA. Programa de entrenamiento cognitivo en adultos mayores (A cognitive training program in elderly adults) Revista Mexicana de Medicina Física y Rehabilitación. 2010;22:26–31. [Google Scholar]
- García Martínez J, Sánchez Cánovas J. Adaptación del cuestionario de fallos de memoria en la vida cotidiana (MFE) Boletín de Psicología. 1994;43:89–107. [Google Scholar]
- Golden C, Purisch A, Hammeke T. Luria-Nebraska neuropsychological battery: forms I and II. Los Ángeles: Western Psychological Services; 1985. [Google Scholar]
- Gross AL, Rebok GW. Memory training and strategy use in older adults: results from the ACTIVE study. Psychol Aging. 2011;26(3):503. doi: 10.1037/a0022687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huppert F, Beardsall L. Prospective memory impairment as an early indicator of dementia. J Clin Exp Neuropsychol. 1993;15(5):805–821. doi: 10.1080/01688639308402597. [DOI] [PubMed] [Google Scholar]
- Kazui H, Matsuda A, Hirono N, Mori E, Miyoshi N, Ogino A, et al. Everyday memory impairment of patients with mild cognitive impairment. Dement Geriatr Cognit Disord. 2005;19:331–337. doi: 10.1159/000084559. [DOI] [PubMed] [Google Scholar]
- Kopecek M, Stepankova H, Lukavsky J, Ripova D, Nikolai T, Bezdicek O. Montreal cognitive assessment (MoCA): normative data for old and very old Czech adults. Appl Neuropsychol Adult. 2017;24(1):23–29. doi: 10.1080/23279095.2015.1065261. [DOI] [PubMed] [Google Scholar]
- Libon D, Bondi M, Price C, Lamar M, Eppig J, Wambach M, et al. Verbal serial list learning in mild cognitive impairment: a profile analysis of interference, forgetting and errors. J Int Neuropsychol Soc. 2011;17(5):905–914. doi: 10.1017/S1355617711000944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Livingston G, Sommerlad A, Orgeta V, Costafreda S, Huntley J, Ames D, Ballard C, Banerjee S, Burns A, Cohen-Mansfield J, Cooper C, Fox N, Gitlin L, Howard R, Kales H, Larson E, Ritchie K, Rockwood K, Sampson E, Samus Q, Schneider L, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care. Lancet. 2017;390:10113. doi: 10.1016/S0140-6736(17)31363-6. [DOI] [PubMed] [Google Scholar]
- Lobo A. “Screening” de trastornos psíquicos en la práctica médica. Zaragoza: Secretariado de Publicaciones, Universidad de Zaragoza; 1987. [Google Scholar]
- Lobo A, Escobar V, Ezquerra J, Seva Díaz A. “El Mini-Examen Cognoscitivo” (Un test sencillo, práctico, para detectar alteraciones intelectuales en pacientes psiquiátricos) [The “Mini-Examen Cognoscitiuo”: a simple and practical test to detect intellectual dysfunctions in psychiatric patients] Revista de Psiquiatría y Psicología Médica. 1980;14(5):39–57. [Google Scholar]
- Malek-Ahmadi M, Powell J, Belden C, O’Connor K, Evans L, Coon D, Nieri W. Age-and education-adjusted normative data for the montreal cognitive assessment (MoCA) in older adults age 70–99. Aging Neuropsychol Cognit. 2015;22(6):755–761. doi: 10.1080/13825585.2015.1041449. [DOI] [PubMed] [Google Scholar]
- Man D, Ganesan B, Yip C, Lee C, Tsang S, Pan Y, Janice Y, Shum D. Validation of the virtual-reality prospective memory test (Hong Kong Chinese version) for individuals with first-episode schizophrenia. Neuropsychol Rehabil. 2016;13:1–14. doi: 10.1080/09602011.2016.1251949. [DOI] [PubMed] [Google Scholar]
- Martín M, Sasson Y, Crivelli L, Gerschovich E, Campos J, Calcagno M, et al. Relevancia del efecto de posición serial en el diagnostic diferencial entre el deterioro cognitivo leve, la demencia de tipo Alzheimer y el envejecimiento normal. Neurología. 2013;28:219–225. doi: 10.1016/j.nrl.2012.04.013. [DOI] [PubMed] [Google Scholar]
- Matsuzono K, Yamashita T, Ohta Y, Hishikawa N, Sato K, Kono S, Deguchi K, Nakano Y, Abe K. Clinical benefits for older Alzheimer’s disease patients: Okayama Late Dementia Study (OLDS) J Alzheimer’s Dis. 2015;46(3):687–693. doi: 10.3233/JAD-150175. [DOI] [PubMed] [Google Scholar]
- McAlister C, Schmitter-Edgecombe M. Cross-sectional and longitudinal analyses of everyday memory lapses in older adults. Aging Neuropsychol Cognit. 2016;23(5):591–608. doi: 10.1080/13825585.2015.1132669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAvinue LP, Golemme M, Castorina M, Tatti E, Pigni FM, Salomone S, Robertson IH. An evaluation of a working memory training scheme in older adults. Front Aging Neurosci. 2013;5:20. doi: 10.3389/fnagi.2013.00020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mogle J, Muñoz E, Hill N, Smyth J, Sliwinski M. Daily memory lapses in adults: characterization and influence on affect. J Gerontol Ser B Psychol Sci Soc Sci. 2017;1:2. doi: 10.1093/geronb/gbx012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montejo P. Programa de entrenamiento de memoria para mayores con alteraciones de memoria: resultados y predictores. Rev española de Geriatría y Gerontol. 2003;38(6):316–326. doi: 10.1016/S0211-139X(03)74908-7. [DOI] [Google Scholar]
- Montejo P, Montenegro M, Reinoso AI, De Andrés E, Claver MD. Programa de memoria: método UMAM. Madrid: Díaz de Santos; 2006. [Google Scholar]
- Montejo P, Montenegro M, Fernández MA, Maestu F. Subjective memory complaints in the elderly: prevalence and influence of temporal orientation, depression and quality of life in a population-based study in the city of Madrid. Aging Ment Health. 2011;15(1):85–96. doi: 10.1080/13607863.2010.501062. [DOI] [PubMed] [Google Scholar]
- Mozaz T. Test conductual de memoria de Rivermead. Madrid: TEA; 1991. [Google Scholar]
- Niedźwieńska A, Rendell P, Barzykowski K, Leszczyńska A. Virtual week: validity and psychometric properties of a Polish adaptation. Rev Eur de Psychol Appl Eur Rev Appl Psychol. 2016;66(2):79–84. doi: 10.1016/j.erap.2016.02.003. [DOI] [Google Scholar]
- Parsons T, Carlew A, Magtoto J, Stonecipher K. The potential of function-led virtual environments for ecologically valid measures of executive function in experimental and clinical neuropsychology. Neuropsychol Rehabil. 2017;27(5):777–807. doi: 10.1080/09602011.2015.1109524. [DOI] [PubMed] [Google Scholar]
- Ramos J, Montejo M, Lafuente R, Ponce de León C, Moreno A. Validación de tres procedimientos para diagnosticar depresión en ancianos. Rev Espanõla de Geriatr y Gerontol. 1993;28(5):275–279. [Google Scholar]
- Real Decreto 223/2004, de 6 de febrero, por el que se regulan los ensayos clínicos con medicamentos. BOE número 33, 07/02/2004
- Real Decreto 504/2007, de 20 de abril, por el que se aprueba el baremo de valoración de la situación de dependencia establecido por la Ley 39/2006, de 14 de diciembre, de promoción de la autonomía personal y atención a las personas en situación de dependencia. BOE número 96, 21/04/2007
- Reijnders J, van Heugten C, van Boxtel M. Cognitive interventions in healthy older adults and people with mild cognitive impairment: a systematic review. Ageing Res Rev. 2013;12:263–275. doi: 10.1016/j.arr.2012.07.003. [DOI] [PubMed] [Google Scholar]
- Rendell PG, Henry JD. A review of virtual week for prospective memory assessment: clinical implications. Brain Impair. 2009;10(1):14–22. doi: 10.1375/brim.10.1.14. [DOI] [Google Scholar]
- Requena C, López-Fernández V, Ortiz-Alonso T. Satisfacción con la vida en relación con la funcionalidad de las personas mayores activas. Actas Española de Psiquiatr. 2009;37(2):61–67. [Google Scholar]
- Requena C, Turrero A, Ortiz T. Six-year training improves everyday memory in healthy older people. Randomized controlled trial. Front Aging Neurosci. 2016;8:135. doi: 10.3389/fnagi.2016.00135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodríguez-Bailón M, Montoro-Membila N, Garcia-Morán T, Arnedo-Montoro ML, Funes Molina MJ. Preliminary cognitive scale of basic and instrumental activities of daily living for dementia and mild cognitive impairment. J Clin Exp Neuropsychol. 2015;37(4):339–353. doi: 10.1080/13803395.2015.1013022. [DOI] [PubMed] [Google Scholar]
- Salorio P, Barcia D, Fortea I, Moya F, Hernández A (2004) Detección precoz del deterioro cognitivo mediante el RBMT y el Test del Reloj
- Spooner DM, Pachana NA. Ecological validity in neuropsychological assessment: a case for greater consideration in research with neurologically intact populations. Arch Clin Neuropsychol. 2006;21(4):327–337. doi: 10.1016/j.acn.2006.04.004. [DOI] [PubMed] [Google Scholar]
- Steibel NM, Olchik MR, Yassuda MS, Finger G, Gomes I. Influence of age and education on the Rivermead Behavioral Memory Test (RBMT) among healthy elderly. Dement Neuropsychol. 2016;10(1):26–30. doi: 10.1590/s1980-57642016dn10100005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephan B, Minett T, Pagett E, Siervo M, Brayne C, McKeith I. Diagnosing Mild Cognitive Impairment (MCI) in clinical trials: a systematic review. BMJ Open. 2013;3:e001909. doi: 10.1136/bmjopen-2012-001909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauss E, Sherman EM, Spreen O. A compendium of neuropsychological tests: administration, norms, and commentary. Washington: American Chemical Society; 2006. [Google Scholar]
- Sunderland A, Harris J, Gleave J. Memory failures in everyday life following severe head injury. J Clin Exp Neuropsychol. 1984;6(2):127–142. doi: 10.1080/01688638408401204. [DOI] [PubMed] [Google Scholar]
- Wechsler D. WMS-R: Wechsler memory scale–revised: manual. San Antonio: Psychological Corporation; 1987. [Google Scholar]
- Wilson B, Cockburn J, Baddeley A, Hiorns R. The development and validation of a test battery for detecting and monitoring everyday memory problems. J Clin Exp Neuropsychol. 1989;11(6):855–870. doi: 10.1080/01688638908400940. [DOI] [PubMed] [Google Scholar]
- Yassuda M, Flaks M, Viola L, Speggiorin-Pereira F, Memória C, Villela-Nunes P, Forlenza O. Psychometric characteristics of the Rivermead Behavioural Memory Test (RBMT) as an early detection instrument for dementia and mild cognitive impairment in Brazil. Int Psychogeriatr. 2010;22(6):1003–1011. doi: 10.1017/S1041610210001055. [DOI] [PubMed] [Google Scholar]
- Yesavage J, Brink T, Rose T, Lum O, Huang V, Adey M, Leirer V. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1983;17(1):37–49. doi: 10.1016/0022-3956(82)90033-4. [DOI] [PubMed] [Google Scholar]