

Abstract
Objective
Vitamin D deficiency is linked with pain, function, and radiographic progression of knee osteoarthritis (KOA), but the results of studies addressing the association and effect of vitamin D supplementation for pain, function, quality of life, radiographic disease, and progression are inconsistent. The aim of this review is to determine the therapeutic and preventive potential of vitamin D supplementation in KOA.
Method
Eligible pertinent English language studies published in 2000 and thereafter in Medline/PubMed, Scopus, and Google Scholar were selected by using keywords that include “knee osteoarthritis,” “vitamin D supplementation,” “pain,” “structural abnormalities,” “treatment,” and “progression.”
Results
The results of a few studies showed a preventive potential for vitamin D in KOA, but most of the randomized clinical trials that assessed the therapeutic efficacy of vitamin D supplementation in KOA found no clear therapeutic effect, with the exception of one study that found a small but significant effect of vitamin D on pain and knee function. Nonetheless, the results of a few longitudinal studies as well as systematic reviews are promising and thus encourage further studies. Inconsistent results on the effect of vitamin D on KOA may be attributed to factors such as severity of KOA, baseline level of serum vitamin D, duration of treatment, and vitamin D dosages.
Conclusion
Given the multiple skeletal and extraskeletal benefits of vitamin D supplementation in elderly people, the issue of vitamin D supplementation in KOA requires further study to elucidate the dosage and duration of treatment that provides the most effective therapeutic effect.
Introduction
Osteoarthritis (OA) is the most common musculoskeletal disease and an significant cause of disability in the elderly population. It is characterized by skeletal pain, structural damage, and impairment of joint mobility 1, 2. Most of the skeletal joints are affected by OA in the elderly, but the pain linked with knee OA (KOA) is the leading cause of referral to health care centers 1. KOA at both individual and population levels is responsible for a decrease in the permanent loss of life quality. Almost 14 million U.S. populations have symptomatic KOA, and more than half of these people are less than 65 years old 3. This issue emphasizes the need to plan preventive programs to reduce development as well as progression of KOA in the general population.
At present, there is no definitive treatment for KOA, and current therapy aims to relieve pain and modify responsible factors of disease progression and joint destruction 1, 4. However, in the presence of risk factors, structural abnormalities progress and lead to pain and future development of disability in a proportion of patients 1, 5, 6. Thus, the need for novel therapeutic agents that target structural abnormalities in order to slow the progression of KOA has been established 1, 6.
Several factors, such as obesity, age, ethnicity, trauma, and vitamin D deficiency, have been shown to play a role in the development as well as progression of KOA 1, 7. Meanwhile, exploring the role of vitamin D is more important because improving vitamin D deficiency may confer additional benefits in relation to several aspects of the elderly's life, such as osteoporosis, muscle strength, and fall prevention 3, 7. Current data emphasize a possible contributive role for vitamin D deficiency in the ethiopathogenesis of osteoarthritis. Hence, more attention has been given to the administration of vitamin D in order to affect the prevalence rate or to slow progression of KOA 2, 7.
Osteoblastic cells and chondrocytes express vitamin D receptors, and vitamin D plays a role in the regulation of chondrocyte hypertrophy, osteoblastic bone proliferation, and mineralization. Furthermore, activated vitamin D contributes to the production of proteoglycans, osteocalcin, as well as alkaline phosphatase, to maintain cartilage health. Thus, a state of vitamin D deficiency may impose a greater risk of degeneration of knee joint cartilage 8, 9.
Vitamin D deficiency in patients with KOA is linked with pain, increased risk of radiographic OA, worsening of knee pain, impaired life quality, cartilage loss, and worsening and progression of radiographic OA 7, 10, 11, 12, 13, 14, 15. Both vitamin D deficiency and KOA are prevalent in the general population, and both conditions are associated with impaired quality of life, especially in the elderly population 16, 17, 18, 19, 20. In particular, the association of vitamin D with pain sensitization and bone and cartilage metabolism implies that administration of vitamin D supplementation in the treatment of KOA specifically to elderly subjects who are more likely to have vitamin D deficiency is beneficial 21, 22, 23.
So far, the association between vitamin D and knee pain, function, quality of life, and incidence and progression of radiographic KOA has been investigated in many interventional and observational studies, but the results are inconsistent and do not lead to a single conclusion.
Materials and Methods
This narrative review aims to summarize the findings of studies that have examined the association of vitamin D level with pain, function, quality of life, radiographic disease and radiographic progression in patients with KOA, as well as the effect of vitamin D supplementation on pain, function, quality of life, radiographic disease, and radiographic progression. For these purposes English language databases were searched to identify potential studies that have been published in Medline/PubMed, Scopus, and Google Scholar by using keywords such as “vitamin D supplementation,” “knee osteoarthritis,” “treatment,” “radiographic incidence,” “progression,” “worsening,” “pain,” “quality of life,” and “structural abnormalities.” In addition, the references of the selected papers were searched to find eligible studies. A total of 705 records were identified by searching databases, and 23 studies were found to be eligible for this study (Figure 1).
Figure 1.
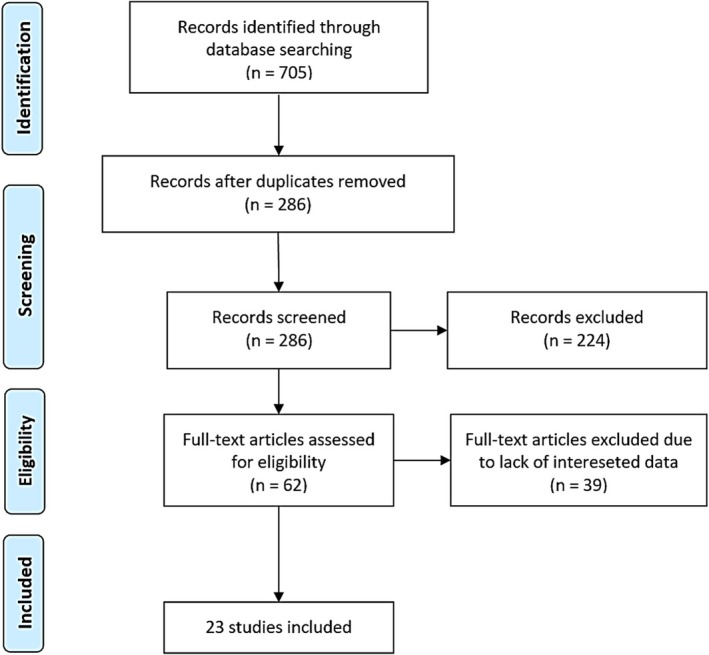
Flow diagram of selection of studies.
Results
Normal bone and cartilage metabolism requires an optimal level of serum 25‐hydroxyvitamin D3 (serum 25(OH)D), which, in active form, exerts anabolic and catabolic actions on bone and cartilage tissues. Therefore, low intake of vitamin D or a vitamin D deficiency state might impair osteoblastic activity, bone metabolism, as well as cartilage turnover and thus result in progression or exacerbation of OA 9. Several studies have shown an association between low serum vitamin D and osteoarthritis severity, pain, radiographic progression and impaired quality of life. Hence, the therapeutic influence of supplemental vitamin D has been investigated in many interventional studies.
Vitamin D level and association with pain, function, quality of life, radiographic disease and radiographic progression.
A systematic review and meta‐analysis of 81 observational studies with 50 834 participants found significantly lower serum 25(OH)D in patients with pain conditions like arthritis, muscle pain, and chronic widespread pain as compared with the control group 24. Another meta‐analysis of 12 studies revealed an association between hypovitaminosis D, particularly serum 25(OH)D levels less than 8‐10 ng/ml, and chronic widespread pain 25. In one large cross‐sectional study, patients with serum 25(OH)D levels of 15 ng/ml or less had greater risk of pain, including widespread pain, as compared with those patients with serum 25(OH)D levels that were greater than 15 ng/ml 26. Low serum vitamin D is related to OA and OA‐related pain, particularly when the hand and hip are involved 27.
The results of a large longitudinal, population‐based cohort study of patients with KOA indicated an association between baseline serum 25(OH)D less than 25 nmol/L and incident knee pain or worsening of knee pain over 5 years of follow‐up 28. Nonetheless, in the Hertfordshire Cohort Study, the association between low serum 25(OH)D and pain was weak 15, and in two small cross‐sectional studies, there was no association between vitamin D deficiency and pain in KOA. However both studies failed to compare serum 25(OH)D level in patients with a control group, and more than 90% of the study population in both studies had a vitamin D deficiency 29, 30. Several observational studies have related vitamin D deficiency to the development and progression of radiographic osteoarthritis and impaired quality of life 7, 12, 13, 14, 17, 18, 23, 31, 32, 33 (Table 1).
Table 1.
Studies on the association between vitamin D and outcomes of patients with knee osteoarthritis
| Reference | Study Type and Population | Results |
|---|---|---|
| Wu et al 50 | A systematic review and meta‐analysis of 81 observational studies with 50 834 participants | Compared with control group, mean serum 25(OH)D level was significantly lower in patients with arthritis, muscle pain, and chronic widespread pain. |
| Lane et al 10 | Longitudinal study including 237 patients with low serum 25(OH)D | Over 8 years, low serum 25(OH)D was associated with increased risk of incident hip OA. |
| Lastlett et al 28 | Longitudinal population‐based cohort study, 769 randomly selected patients with KOA aged 62(50‐80) years, serum 25(OH)D <25 nmol/ml | Over 5 years, moderate vitamin D deficiency predicted incident worsening of KOA. |
| Felson et al 48 | Longitudinal study, 715 patients with KOA, mean age, 53.1 ± 8.7, mean serum 25(OH)D <29 ng/ml | Over 9 years, no association was found between baseline serum 25(OH)D and worsening of radiographic KOA. |
| Chaganti et al 12 | Longitudinal study of elderly men with hip OA | Over 4‐6 years, subjects with serum 25(OH)D <30 ng/ml had increased risk of prevalent hip OA as compared with those that had levels >30 ng/ml. |
| Zhang et al 11 | Longitudinal study, 418 patients with KOA, aged 61.2 ± 9.1 years | Over 24‐48 months, serum 25(OH)D <15 nmol/L was associated with increased risk of KOA by OR = 2.3(95% CI, 1.1‐4.5). |
| Zheng et al 22 | Longitudinal clinical trial, 340 people, mean age 62.3 years with symptomatic KOA | Over 24 months, individuals with consistent serum 25(OH)D >50 nmol/L had a lower loss of tibial cartilage volume, less increase in effusion‐synovitis volume, and lower loss of WOMAC index of physical function as compared with the consistently <50 nmol/L group |
| Cao et al 45 | Systematic review and meta‐ analysis of patients with KOA | An association was found between vitamin D deficiency and cartilage loss and joint space narrowing. |
| Ding et al 42 | Longitudinal study of 880 randomly selected KOA, mean age 61.7 ± 7 years serum 25(OH)D < 50 nmol/L | Over 2.9 years, a positive association was found between baseline serum 25(OH)D and medial cartilage volume only in women. |
| McAlindon et al 40 | Prospective observational study of 556 patients with KOA, aged 70.3 ± 4.5 years, baseline serum 25(OH)D, 29.6 ng/ml | Over 10 years, low serum 25(OH)D was associated with increased risk of progressive KOA. |
| Bergink 43 | Prospective population‐based cohort study, 1248 patients of Rotterdam study, mean vitamin D intake and serum 25(OH)D was 64 IU/d and 66 nmol/L respectively. | Over 6.5 years, an association was found between vitamin D intake and risk of progression of radiographic KOA. |
| Bassiouni et al 41 | Longitudinal study of patients with KOA | Over 12 months, deterioration of medial femorotibial OA was significantly greater in subjects with serum 25(OH)D 10 ng/ml vs >10 ng/ml. |
| Bergink et al 44 | Meta‐analysis of six cross‐sectional studies | Decreasing serum vitamin D was associated with increased risk of joint KOA space narrowing and progression radiographic KOA |
| Jagannath et al 49 | Longitudinal study of 396 subjects aged 64.8 ± 2.7 years | Over 10.3 years, baseline serum 25(OH)D was not associated with progression of KOA in older men and women. |
Abbreviation: KOA, knee osteoarthritis; serum 25(OH)D = serum 25‐hydroxyvitamin D3; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Low levels of serum vitamin D are also a determinant for the development of major health‐related conditions, and in older persons it represents an independent risk factor for falls 19, 34. Some clinical features, such as muscle pain and weakness, difficulties in gait and climbing stairs, and generalized loss of muscular mass, active daily living disability (ADL), particularly in elderly people, are associated with vitamin D deficiency 35. This issue has been investigated in a number of observational studies. In a large study of community‐dwelling adults aged 77 to 100 years old, serum 25(OH)D at less than 30 ng/ml was associated with poorer physical performance and more prevalent mobility and ADL disability. In this study, baseline vitamin D deficiency was a predictor of incident disability over 3 years of follow‐up 36. A similar association of vitamin D and quality of life has been shown in participants of the fifth Korean National Health and Nutrition Examination Survey (KNHANES V) aged 50 or older. In this study, serum 25(OH)D less than 10 ng/ml was significantly associated with poor health‐related quality of life 37. Furthermore, poor knee function, locomotor dysfunctions, and decline in physical performance are associated with vitamin D deficiency 19, 20, 38, 39.
In community‐dwelling elderly women and men, vitamin D deficiency is associated with worse coordination and weaker strength, lower walking time, lower upper limb strength, and weaker aerobic capacity 39. A large cross‐sectional and longitudinal design (3‐year follow‐up) study of 1234 men and women over 65 years old found that serum 25(OH)D levels lower than 10 ng/ml and 10‐20 ng/ml are predictors of future development of decline in physical performance 20.
The results of studies on the association between vitamin D and radiographic abnormalities are conflicting (Table 1). This is because the study population, baseline serum 25(OH)D, and the outcomes were different across studies. Association between low serum vitamin D with increased risk of KOA progression has been observed in four longitudinal studies. The risk of progression as well as deterioration of medial femorotibial OA were greater in subjects with lower serum 25(OH)D levels than individuals with higher levels of serum 25(OH)D 11, 22, 40, 41.
In one longitudinal study, changes in medial and lateral tibial cartilage volume assessed by magnetic resonance imaging (MRI) were positively associated with changes in serum vitamin D over 2.9 years of follow‐up 42. In the population of the Rotterdam study, low intake of vitamin D was associated with increased risk of radiographic KOA, particularly in subjects with low baseline bone mineral density. In this study, progression of radiographic OA occurred in 5.1% of the participants in the highest tertile versus 12.6% in the lowest tertile 43.
The results of three systematic reviews and meta‐analyses revealed an association between low serum 25(OH)D and progression of radiographic KOA 7, 44, 45. Nevertheless, two cohort studies found no association between low serum vitamin D and development of incident knee or hip OA over a follow‐up period of more than 10 years 27, 46. Moreover, two longitudinal studies of patients with vitamin D deficiency (serum 25(OH)D less than 20 ng/ml) and another cross‐sectional study of men and women aged 18‐74 years, found no significant differences in radiographic hand OA and the risk of joint space narrowing or cartilage loss in KOA, or KOA progression between subjects with and without vitamin D deficiency 47, 48, 49.
Vitamin D supplementation on pain, function, quality of life, radiographic disease and radiographic progression.
KOA itself is a disabling condition, and the presence of vitamin D deficiency in KOA aggravates the disability and impairs physical performance and quality of life 50, 51. Furthermore, low serum vitamin D is related to pain sensitization and severity of pain, and both conditions have important contributions to the development or severity of clinical symptoms in patients with KOA 52. Prevalence of vitamin D deficiency in elderly people, particularly in those with KOA, is high and poses a greater risk of developing muscle weakness, physical dysfunction, and impaired quality of life 18, 19, 31, 35, 53. In one study, supplementation of vitamin D, with a daily dosage of 800‐1000 IU, exerted a consistent beneficial effect on muscle strength, gait, and balance in the elderly 54. A quantitative meta‐analysis of 19 published randomized control trials (RCTs) revealed that vitamin D supplementation was associated with greater reduction in pain score as compared with the placebo group 50. These observations suggest the importance of maintaining serum vitamin D levels in elderly people at a sufficient state. An adequate level of serum vitamin D is expected to improve muscle strength, reduce knee pain, and reinforce physical performance 23, 33, 55. The results of studies in relation to vitamin D supplementation and KOA are summarized in Table 2.
Table 2.
Studies on the effect of supplemental vitamin D on the outcomes of patients with knee osteoarthritis
| Reference | Type of Study, Characteristics of the Study Population | Vitamin D Dosage and Duration of Treatment | Outcome Measures | Results |
|---|---|---|---|---|
| Jin et al 58 | RCT, 413 symptomatic KOA aged 50‐79 years, baseline serum 25(OH)D, 12.5‐60 nmol/L | 50 000 IU cholecalciferol monthly for 24 months vs placebo | Changes in knee pain by WOMAC, and tibial cartilage volume loss assessed by MRI | Vitamin D supplementation did not result in significant changes in pain and cartilage volume. |
| Arden et al 60 | RCT, 417 patients with KOA, aged >50 years, mean baseline 25(OH)D 20.7 ± 8.9 ng/ml | 800 IU daily for 3 years | Radiological progression of KOA in the medial joint, and changes in WOMAC pain | Vitamin D did not show a significant decrease in the rate of joint space narrowing. |
| McAlindon et al 59 | RCT, 146 symptomatic KOA, aged 61.8 ± 7.7 years, mean baseline 25(OH)D 22.7 ± 11.4 ng/ml | 2000 IU daily with dose escalation to elevate serum 25(OH)D >36 ng/ml | Change in pain and cartilage volume loss assessed by MRI from baseline | Vitamin D did not reduce knee pain or cartilage loss vs placebo. |
| Sanghi et al 56 | RCT, 107 KOA, mean baseline serum 25(OH)D <50 nmol/L, aged 53 ± 7.4 ng/ml (52 vitamin D, 51 in placebo group) | 60 000 IU daily for 10 days and 60 000 IU monthly for 12 months | Changes in knee pain and function | Small but statistically significant clinical benefits on pain and function in vitamin D group. |
| Diao et al 63 | Systematic review of previous studies consisting of 570 patients with KOA and 560 controls | Not mentioned | Pain and cartilage volume changes | Vitamin D had a statistically significant but small to moderate effect on pain in KOA but no effect on tibial cartilage volume. |
| Wang et al 65 | RCT, 413 symptomatic KOA, aged 63.7 ± 7 years, baseline serum 25(OH)D, 12.5‐60 nmol/L | 50 000 IU cholecalciferol monthly vs placebo for 24 months | Effect on synovitis, joint effusion | Vitamin D retarded effusion synovitis, suggesting an anti‐inflammatory effect. |
| Gao et al 62 | Meta‐analysis of four RCTs between 2013 and 2016 consisting of 1136 patients | Ranged from 800 IU daily to 60 000 IU weekly | Changes in WOMAC pain, function and stiffness, tibial cartilage volume | The serum 25(OH)D increased by 17.58 μg/L in vitamin D group vs 5.7 nmol/L reduction g/L in placebo group. Improvement in WOMAC pain, stiffness but not in tibial cartilage volume loss. |
| Perry et al 66 | RCT, 24 patients with symptomatic KOA and 26 control. Baseline serum 25(OH)D in patients 26.6 ± 8.5 and in control 25.3 ± 8.7 ng/ml | 800 IU daily cholecalciferol vs placebo for 2 years | Changes in synovial tissue volume and also subchondral bone marrow lesion assessed by MRI | No significant difference in MRI findings. Serum 25(OH)D increased by 5.2 ng/ml in vitamin D group and decreased by 2.5 ng/ml in placebo. |
| Heidari et al 23 | Longitudinal study of 67 patients with symptomatic KOA, aged 50 ± 6.6, baseline serum 25(OH)D <20 ng/ml | 50 000 IU cholecalciferol weekly for 2 months | Knee pain, quadriceps muscle strength | Significant decrease in pain and significant improvement in quadricep muscle strength. |
| Manoy et al 67 | Longitudinal study, 175 patients with KOA, aged 64.5 ± 0.5 5 years, baseline 25(OH)D <30 ng/ml (41% <20 ng/ml); no control group | 40 000 IU ergocalciferol for 3 months | Pain, grip strength, quality of life, physical performance | Significant improvement in pain, grip strength, quality of life, and physical performance. |
| Alsubiaee et al 68 | Longitudinal study of 53 patients with KOA, aged 45 ± 4.5 years, baseline serum 25(OH)D <75 nmol/L | Cholecalciferol 45 000 IU weekly for 3 months followed by 45 000 IU every 2 weeks for 2 years | Pain, joint function | No effect on joint pain and function compared with baseline. |
Abbreviation: KOA, knee osteoarthritis; MRI, magnetic resonance imaging; RCT, randomized placebo‐controlled clinical trial; serum 25(OH)D, serum 25‐hydroxyvitamin D3; WOMAC, Western Ontario McMaster Universities Arthritis.
In a short longitudinal study of 67 patients with vitamin D deficiency and symptomatic KOA, vitamin D supplementation at a weekly dosage of 50 000 IU for 2 months increased serum vitamin D to sufficient levels and significantly improved knee pain and quadricep muscle strength. Lack of a control group and a small sample size are limitations of this study 23.
Four RCTs have assessed the effect of vitamin D supplementation in KOA. Sanghi et al in a randomized placebo‐controlled clinical trial of patients with vitamin D deficiency and KOA found significant improvement in knee pain and function with a high‐dose cholecalciferol supplementation at 60 000 IU daily for 10 days and 60 000 IU monthly for 12 months. The level of serum 25(OH)D increased from baseline by 45.7 nmol/L in the vitamin D group versus 2.12 nmol/L in the placebo group 56. Small sample size and short duration of treatment are limitations of this study. Nonetheless, the effect of vitamin D on pain was estimated to be larger than the effect of nonsteroidal anti‐inflammatory drugs and close to the effect of intra‐articular corticosteroid on KOA pain 57.
Jin et al, in another study of patients with KOA and low serum vitamin D (serum 25(OH)D less than 60 nmol/L), found no significant effect of 50 000 IU cholecalciferol monthly for 2 years on pain, cartilage volume loss, and progression of structural abnormalities as assessed by MRI. Compared with a later study, the mean age of patients in this study was higher (63.5 ± 6.9 vs 53.2 ± 9.6 years), and the serum level in 21% of the vitamin D–treated group did not reach a sufficient level. Nonetheless, in post hoc analysis, a significant improvement of knee pain was detected in the vitamin D group. Furthermore, the magnitude of improvement in total Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score and WOMAC function in the vitamin D group was greater, and progression of bone marrow lesions (BMLs) in this group was significantly lower than it was in the placebo group 58. Two RCTs that compared the effect of a low daily dose of supplemental vitamin D with placebo found no beneficial effect of vitamin D in KOA 59, 60. In a study by McAlindon et al, 2000 IU cholecalciferol daily for 2 years with dose escalation to elevate serum levels to more than 36 ng/ml had no effect on pain or cartilage volume loss as compared with the placebo group. In this study, only 61.3% of the patients in the vitamin D group achieved the target level of 36 ng/ml, and the patients of the treatment group had more severe disease regarding WOMAC pain scores, WOMAC function, and femoral cartilage volume at baseline. In addition, 51% of patients in the vitamin D group had advanced KOA with Kellgren and Lawrence grades of 3 and 4 and in whom structural abnormalities are less expected to be reversible. Nevertheless, in subset analysis, the effect of vitamin D on WOMAC pain was significantly larger in patients who were vitamin D deficient at baseline 59. Similarly, in another 3‐year randomized double‐blind, placebo‐controlled trial of 474 symptomatic patients with KOA by Arden et al, supplementation of cholecalciferol with a daily dose of 800 IU had no significant effect on the rate of joint space narrowing assessed by X‐ray, knee pain, function, or stiffness, even in vitamin D–deficient participants. The serum 25(OH)D level increased by 10 μg/L in 1 year, and the serum 25(OH)D level increased from 20.7 ± 8.9 μg/L at baseline to 30.4 ± 7 μg /L at the end point. At 12 months, 46% of the vitamin D–supplemented group vs 14% of the placebo group achieved sufficient levels of serum vitamin D 60. Application of radiography is a limitation of this study because the sensitivity of radiography is lower than that of MRI 61.
Meta‐analysis of the four abovementioned RCTs by Gao et al, which consisted of a total of 1136 patients, revealed that serum 25(OH)D increased by 17.58 nmol/L in the vitamin D group and decreased by 5.7 nmol/L in the placebo group. Pooled results showed that vitamin D supplementation at more than 2000 IU daily was associated with a significant improvement in stiffness and WOMAC pain but not in WOMAC function and progression of tibial cartilage volume loss 62. Another meta‐analysis of the same studies by Diao et al reached the same conclusion 63. Nonetheless, the results of a systematic review of RCTs that consists of 1189 participants aged 45 years and older did not support vitamin D supplementation in KOA 64.
In a clinical trial of vitamin D–deficient KOA with knee joint effusion‐synovitis, vitamin D supplementation retarded the progression of synovitis 65. In another RCT of 60 patients with symptomatic KOA (25 taking 800 IU cholecalciferol daily and 26 taking placebo for 2 years), the MRI findings showed no significant differences in synovial tissue volume and subchondral BMLs between the study groups. Small sample size, low vitamin D dosage, and short duration of treatment are major limitations of this study. In this study, only a small proportion of the participants had vitamin D deficiency 66.
Manoy et al, in a longitudinal study of patients with vitamin D deficiency or insufficient patients with symptomatic KOA, administered 40 000 IU ergocalciferol weekly for 6 months. At endpoint, the serum 25(OH)D level increased to sufficient levels (greater than 30 ng/ml) and resulted in a significant improvement of the muscle strength, Visual Analogue Scale (VAS) pain score, physical performance, and the quality of life, but pain on physical activity assessed by WOMAC did not improve 67. However, lack of a control group and short period of treatment are limitations of this study. The results of a small uncontrolled study of patients with symptomatic KOA demonstrated that vitamin D supplementation at 45 000 IU weekly for three months, followed by 45,000 IU every 2 weeks for 1 year, had no effect on knee pain and function in patients with baseline serum 25(OH)D at 75 nmol/L or less. In this study, only 58 out of 100 participants completed the study 68.
Discussion
It should be noted that OA is a chronic condition and that osteoarticular changes occur several years after exposure to risk factors. Therefore, recovery of these structural changes requires long‐term treatment. Thus, short‐term clinical trials are not expected to be associated with a detectable improvement in structural abnormalities by using radiography or MRI. On the other hand, lack of a correlation between clinical symptoms and structural changes in KOA makes it difficult to show structural recovery in subjects with clinical improvement.
The mechanism by which vitamin D deficiency may contribute to the development or worsening of KOA symptoms is unclear, but it can be explained by the effect of vitamin D on inflammatory response, muscle strength, and pain sensitization 23, 33, 63, 65, 69, 70.
In conclusion, existing data suggest a beneficial effect of high‐dose vitamin D supplementation on pain, muscle strength, and quality of life in KOA, without a radiographic or MRI‐detectable improvement on structural changes. However, regarding a positive association of vitamin D deficiency with worsening and progression of radiographic KOA, maintaining serum 25(OH)D at sufficient levels by vitamin D supplementation might be beneficial in KOA. There are several potential explanations to clarify conflicting results across diverse clinical trials. Factors such as baseline serum 25(OH)D level, vitamin D dosages, duration of treatment, severity of KOA, and varying outcome measures across diverse studies all may differently affect the results. Structural changes in patients with advanced KOA are less responsive to treatment as compared with patients with mild disease. Furthermore, structural improvement requires prolonged periods of treatment, and its detection needs a sensitive tool because the size of recovery is not large enough to be detected by conventional radiography or even MRI. On the other hand, prevalence and distribution of the associated factors of knee pain and KOA progression—such as age, sex, vitamin D deficiency, muscle weakness, severity of inflammatory process, and obesity—vary across studies. The influence of any of these factors can undermine the therapeutic effect of vitamin D supplementation.
Currently, the type of structural lesion or clinical features that are susceptible to vitamin D treatment are not known to be considered for treatment outcome. However, structural abnormalities that are associated with vitamin D deficiency are expected to have a greater chance of reversing. Furthermore, changes in abnormalities, such as BMLs, cartilage defects, cartilage volume, synovitis/effusion, and muscle strength, which are more responsive to treatment, can be considered as outcome measures.
Long‐term longitudinal studies with periodic measurement of serum 25(OH)D along with clinical examination and imaging studies can provide opportunities to determine the causal relationship between serum vitamin D and KOA.
Efficacy of vitamin D supplementation on symptoms and structural abnormalities in KOA requires further RCTs. Selection of patients with early KOA is preferable because abnormalities at earlier stages of KOA are likely more reversible and possibly more responsive to treatment.
Several biologic markers pertaining to cartilage metabolism have been recognized. These parameters might be more sensitive to changes in response to treatment and can be considered for evaluation of treatment response in future studies.
Author Contributions
All authors contributed to preparation of manuscript, revision, as well as review of final revised paper.
Study conception and design
Heidari, Babaei.
Acquisition of data
Heidari, Babaei.
Analysis of data
Heidari, Babaei.
Acknowledgments
The authors thank Mohammad Zamani (Student Research Committee, School of Medicine, Babol University of Medical Sciences) for his help in preparing the flow diagram.
No potential conflicts of interest relevant to this article were reported.
References
- 1. Heidari B. Knee osteoarthritis diagnosis, treatment and associated factors of progression: part II. Caspian J Intern Med 2011;2:249–55. [PMC free article] [PubMed] [Google Scholar]
- 2. Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol 2018;30:160–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Abbott JH, Usiskin IM, Wilson R, Hansen P, Losina E. The quality‐of‐life burden of knee osteoarthritis in New Zealand adults: a model‐based evaluation. PloS One 2017;12:e0185676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ding C, Jones G, Wluka AE, Cicuttini F. What can we learn about osteoarthritis by studying a healthy person against a person with early onset of disease? Curr Opin Rheumatol 2010;22:520–7. [DOI] [PubMed] [Google Scholar]
- 5. Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med 2006;354:841–8. [DOI] [PubMed] [Google Scholar]
- 6. Yoo JJ, Kim DH, Kim HA. Risk factors for progression of radiographic knee osteoarthritis in elderly community residents in Korea. BMC Musculoskelet Disord 2018;19:80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Vaishya R, Vijay V, Lama P, Agarwal A. Does vitamin D deficiency influence the incidence and progression of knee osteoarthritis? ‐ A literature review. J Clin Orthop Trauma 2019;10:9–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Mabey T, Honsawek S. Role of vitamin D in osteoarthritis: molecular, cellular, and clinical perspectives. Int J Endocrinol 2015;2015:383918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Garfinkel RJ, Dilisio MF, Agrawal DK. Vitamin D and its effects on articular cartilage and osteoarthritis. Orthop J Sports Med 2017;5:2325967117711376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Lane NE, Gore LR, Cummings SR, Hochberg MC, Scott JC, Williams EN, et al, and the Osteoporotic Fractures Research Group . Serum vitamin D levels and incident changes of radiographic hip osteoarthritis: a longitudinal study. Arthritis Rheum 1999;42:854–60. [DOI] [PubMed] [Google Scholar]
- 11. Zhang FF, Driban JB, Lo GH, Price LL, Booth S, Eaton CB, et al. Vitamin D deficiency is associated with progression of knee osteoarthritis. J Nutr 2014;144:2002–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Chaganti RK, Parimi N, Cawthon P, Dam TL, Nevitt MC, Lane NE. Association of 25‐hydroxyvitamin D with prevalent osteoarthritis of the hip in elderly men: the osteoporotic fractures in men study. Arthritis Rheum 2010;62:511–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Heidari B, Hajian‐Tilaki K, Babaei M. Determinants of pain in patients with symptomatic knee osteoarthritis. Caspian J Intern Med 2016;7:153–61. [PMC free article] [PubMed] [Google Scholar]
- 14. Heidari B, Heidari P, Tilaki KH. Relationship between unexplained arthralgia and vitamin D deficiency: a case control study. Acta Med Iran 2014;52:400–5. [PubMed] [Google Scholar]
- 15. Muraki S, Dennison E, Jameson K, Boucher BJ, Akune T, Yoshimura N, et al. Association of vitamin D status with knee pain and radiographic knee osteoarthritis. Osteoarthritis Cartilage 2011;19:1301–6. [DOI] [PubMed] [Google Scholar]
- 16. Heidari B, Heidari P, Tilaki KH. High prevalence of vitamin d deficiency in women presenting to rheumatology clinic in north of Iran: an inverse relation with age. J Women's Health Care 2013;2:123. [Google Scholar]
- 17. Felson DT, Naimark A, Anderson J, Kazis L, Castelli W, Meenan RF, and the Framingham Osteoarthritis Study . The prevalence of knee osteoarthritis in the elderly. Arthritis Rheum 1987;30:914–8. [DOI] [PubMed] [Google Scholar]
- 18. Jansen JA, Haddad FS. High prevalence of vitamin D deficiency in elderly patients with advanced osteoarthritis scheduled for total knee replacement associated with poorer preoperative functional state. Ann R Coll Surg Engl 2013;95:569–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Levinger P, Begg R, Sanders KM, Nagano H, Downie C, Petersen A, et al. The effect of vitamin D status on pain, lower limb strength and knee function during balance recovery in people with knee osteoarthritis: an exploratory study. Arch Osteoporos 2017;12:83. [DOI] [PubMed] [Google Scholar]
- 20. Zamboni M, Zoico E, Tosoni P, Zivelonghi A, Bortolani A, Maggi S, et al. Relation between vitamin D, physical performance, and disability in elderly persons. J Gerontol A Biol Sci Med Sci 2002;57:M7–11. [DOI] [PubMed] [Google Scholar]
- 21. Gloth FM III, Greenough WB III. Vitamin D deficiency as a contributor to multiple forms of chronic pain. Mayo Clin Proc 2004;79:696 699; author reply 699. [DOI] [PubMed] [Google Scholar]
- 22. Zheng S, Jin X, Cicuttini F, Wang X, Zhu Z, Wluka A, et al. Maintaining vitamin D sufficiency is associated with improved structural and symptomatic outcomes in knee osteoarthritis. Am J Med 2017;130:1211–8. [DOI] [PubMed] [Google Scholar]
- 23. Heidari B, Javadian Y, Babaei M, Yousef‐Ghahari B. Restorative effect of vitamin D deficiency on knee pain and quadriceps in knee osteoarthritis. Acta Med Iran 2015;53:466–70. [PubMed] [Google Scholar]
- 24. Wu Z, Malihi Z, Stewart AW, Lawes CM, Scragg R. The association between vitamin D concentration and pain: a systematic review and meta‐analysis. Public Health Nutr 2018;21:2022–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Hsiao MY, Hung CY, Chang KV, Han DS, Wang TG. Is serum.hypovitaminosis D associated with chronic widespread pain including fibromyalgia? A meta‐analysis of observational studies. Pain Physician 2015;18:E877–87. [PubMed] [Google Scholar]
- 26. Veronese N, Maggi S, Noale M, De Rui, Bolzetta F, Zambon S, et al. Serum 25‐hydroxyvitamin D and osteoarthritis in older people: the Progetto Veneto Anziani Study. Rejuvenation Res 2015;18:543–53. [DOI] [PubMed] [Google Scholar]
- 27. McBeth J, Pye SR, O'Neill TW, Macfarlane GJ, Tajar A, Bartfai G, et al, and EMAS Group . Musculoskeletal pain is associated with very low levels of vitamin D in men: results from the European Male Ageing Study. Ann Rheum Dis 2010;69:1448–52. [DOI] [PubMed] [Google Scholar]
- 28. Lastlett LL, Quinn S, Burgess JR, Parameswaran V, Winzenberg TM, Jones G, et al. Moderate vitamin D deficiency is associated with changes in knee and hip pain in older adults: a 5‐year longitudinal study. Ann Rheum Dis 2014;73:697–703. [DOI] [PubMed] [Google Scholar]
- 29. Cakar M, Ayanoglu S, Cabuk H, Seyran M, Dedeoglu SS, Gurbuz H. Association between vitamin D concentrations and knee pain in patients with osteoarthritis. PeerJ 2018;6:e4670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Al‐Jarallah KF, Shehab D, Al‐Awadhi A, Nahar I, Haider MZ, Moussa MA. Are 25(OH)D levels related to the severity of knee osteoarthritis and function? Med Princ Pract 2012;21:74–8. [DOI] [PubMed] [Google Scholar]
- 31. Babaei M, Esmaeili Jadidi M, Heidari B, Gholinia H. Vitamin D deficiency is associated with tibial bone pain and tenderness. A possible contributive role. Int J Rheum Dis 2018;21:788–95. [DOI] [PubMed] [Google Scholar]
- 32. Heidari B, Heidari P, Hajian‐Tilaki K. Association between serum vitamin D deficiency and knee osteoarthritis. Int Orthop 2011;35:1627–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Javadian Y, Adabi M, Heidari B, Babaei M, Firouzjahi A, Ghahhari BY, et al. Quadriceps muscle strength correlates with serum vitamin d and knee pain in knee osteoarthritis. Clin J Pain 2017;33:67–70. [DOI] [PubMed] [Google Scholar]
- 34. Cesari M, Incalzi RA, Zamboni V, Pahor M. Vitamin D hormone: a multitude of actions potentially influencing the physical function decline in older persons. Geriatr Gerontol Int 2011;11:133–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Kojima G, Tamai A, Masaki K, Gatchell G, Epure J, China C, et al. Prevalence of vitamin D deficiency and association with functional status in newly admitted male veteran nursing home residents. J Am Geriatr Soc 2013;61:1953–7. [DOI] [PubMed] [Google Scholar]
- 36. Houston DK, Tooze JA, Davis CC, Chaves PH, Hirsch CH, Robbins JA, et al. Serum 25‐Hydroxy D and physical function in old adults: The cardiovascular health study all stars. J Am Geriatr Soc 2011;59:1793–801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Kim HJ, Lee JY, Kim TJ, Lee JW. Association between serum vitamin D status and health‐related quality of life (HRQOL) in an older Korean population with radiographic knee osteoarthritis: data from the Korean National Health and Nutrition Examination survey (2010‐2011). Health Qual Life Outcomes 2015;13:48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Martino G, Catalano A, Bellone F, Langher V, Lasco C, Penna A, et al. Quality of life in postmenopausal women: which role for vitamin D? Mediterranean J Clin Psychol 2018;6:1–14. [Google Scholar]
- 39. Toffanello ED, Perissinotto E, Sergi G, Zambon S, Musacchio E, Maggi S, et al. Vitamin D and physical performance in elderly subjects: the Pro.V.A study. PLoS One 2012;7:e34950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. McAlindon TE, Felson DT, Zhang Y, Hannan MT, Alidabadi P, Weissman B, et al. Relation of dietary intake and serum levels of vitamin D to progression of osteoarthritis of the knee among participants in the Framingham Study. Ann Intern Med 1996;125:353–9. [DOI] [PubMed] [Google Scholar]
- 41. Bassiouni H, Aly H, Zaky K, Abaza N, Bardin T. Probing the relation between vitamin D deficiency and progression of medial femoro‐tibial osteoarthitis of the knee. Curr Rheumatol Rev 2017;13:65–71. [DOI] [PubMed] [Google Scholar]
- 42. Ding C, Cicuttini F, Parameswaran V, Burgess J, Quinn S, Jones G. Serum levels of vitamin D, sunlight exposure, and knee cartilage loss in older adults: the Tasmanian older adult cohort study. Arthritis Rheum 2009;60:1381–9. [DOI] [PubMed] [Google Scholar]
- 43. Bergink AP, Uitterlinden AG, Van Leeuwen JP, Buurman CJ, Hofman A, Verhaar JA, et al. Vitamin D status, bone mineral density, and the development of radiographic osteoarthritis of the knee: the Rotterdam Study. J Clin Rheumatol 2009;15:230–7. [DOI] [PubMed] [Google Scholar]
- 44. Bergink AP, Zillikens MC, Van Leeuwen JP, Hofman A, Uitterlinden AG, van Meurs JB. 25‐Hydroxyvitamin D and osteoarthritis: a meta‐analysis including new data. Semin Arthritis Rheum 2016;45:539–46. [DOI] [PubMed] [Google Scholar]
- 45. Cao Y, Winzenberg T, Nguo K, Lin J, Jones G, Ding C. Association between serum levels of 25‐hydroxyvitamin D and osteoarthritis: a systematic review. Rheumatology (Oxford) 2013;52:1323–34. [DOI] [PubMed] [Google Scholar]
- 46. Konstari S, Kaila‐Kangas L, Jääskeläinen T, Heliövaara M, Rissanen H, Marniemi J, et al. Serum 25‐hydroxyvitamin D and the risk of knee and hip osteoarthritis leading to hospitalization: a cohort study of 5274 Finns. Rheumatology (Oxford) 2014;53:1778–82. [DOI] [PubMed] [Google Scholar]
- 47. Kalichman L, Kobyliansky E. Association between circulatory levels of vitamin D and radiographic hand osteoarthritis. Rheumatol Int 2012;32:253–7. [DOI] [PubMed] [Google Scholar]
- 48. Felson DT, Niu J, Clancy M, Aliabadi P, Sack B, Guermazi A, et al. Low levels of vitamin D and worsening of knee osteoarthritis: results of two longitudinal studies. Arthritis Rheum 2007;56:129–36. [DOI] [PubMed] [Google Scholar]
- 49. Jagannath D, Edwards MH, Parsons C, Litwic A, Cooper C, Dennison E. Serum vitamin D does not influence rate of progression of knee osteoarthritis over 10 years: results from the Hertfordshire Cohort Study. Rheumatology 2014;53 Suppl 1:i129. [Google Scholar]
- 50. Wu Z, Malihi Z, Stewart AW, Lawes CM, Scragg R. Effect of vitamin D supplementation on pain: a systematic review and meta‐analysis. Pain Physician 2016;19:415–27. [PubMed] [Google Scholar]
- 51. Kenny AM, Biskup B, Robbins B, Marcella G, Burleson JA. Effects of vitamin D supplementation on strength, physical function, and health perception in older, community‐dwelling men. J Am Geriatr Soc 2003;51:1762–7. [DOI] [PubMed] [Google Scholar]
- 52. Glover TL, Horgas AL, Fillinbim RB, Goodin BR. Vitamin D status and pain sensitization in knee osteoarthritis: a critical review of the literature. Pain Manag 2015;5:447–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Sheikhzadeh M, Lotfi I, Mossavi A, Heidari B, Monadi M, Bakhshi E, Influence of supplemental vitamin D on intensity of benign paroxysmal positional vertigo: A longitudinal study. Caspian J Intern Med 2016;7:93–98. [PMC free article] [PubMed] [Google Scholar]
- 54. Muir SW, Montero‐Odasso M. Effect of vitamin D supplementation on muscle strength, gait and balance in older adults: a systematic review and meta‐analysis. J Am Geriatr Soc 2011;59:2291–300. [DOI] [PubMed] [Google Scholar]
- 55. Bunout D, Barrera G, Leiva L, Gattas V, de la Maza MP, Avendaño M, et al. Effects of vitamin D supplementation and exercise training on physical performance in Chilean vitamin D deficient elderly subjects. Exp Gerontol 2006;41:746–52. [DOI] [PubMed] [Google Scholar]
- 56. Sanghi D, Mishra A, Sharma AC, Singh A, Natu SM, Agarwal S, et al. Does vitamin D improve osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Relat Res 2013;471:3556–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Felson DT. CORR Insights: does vitamin D improve osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Relat Res 2013;471:3563–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Jin X, Jones G, Cicuttini F, Wluka A, Zhu Z, Han W, et al. Effect of vitamin D supplementation on tibial cartilage volume and knee pain among patients with symptomatic knee osteoarthritis: a randomized clinical trial. JAMA 2016;315:1005–13. [DOI] [PubMed] [Google Scholar]
- 59. McAlindon T, LaValley M, Schneider E, Nuite M, Lee JY, Price LL, et al. Effect of vitamin D supplementation on progression of knee pain and cartilage volume loss in patients with symptomatic osteoarthritis: a randomized controlled trial. JAMA 2013;309:155–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Arden NK, Cro S, Sheard S, Doré CJ, Bara A, Tebbs SA, et al. The effect of vitamin D supplementation on knee osteoarthritis, the VIDEO study: a randomised controlled trial. Osteoarthritis Cartilage 2016;24:1858–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Amin S, LaValley MP, Guermazi A, Grigoryan M, Hunter DJ, Clancy M, et al. The relationship between cartilage loss on magnetic resonance imaging and radiographic progression in men and women with knee osteoarthritis. Arthritis Rheum 2005;52:3152–9. [DOI] [PubMed] [Google Scholar]
- 62. Gao XR, Chen YS, Deng W. The effect of vitamin D supplementation on knee osteoarthritis: a meta‐analysis of randomized controlled trials. Int J Surg 2017;46:14–20. [DOI] [PubMed] [Google Scholar]
- 63. Diao N, Yang B, Yu F. Effect of vitamin D supplementation on knee osteoarthritis: a systematic review and meta‐analysis of randomized clinical trials. Clin Biochem 2017;50:1312–6. [DOI] [PubMed] [Google Scholar]
- 64. Hussein S, Singh A, Akhtar M, Najmi AK. Vitamin D supplementation for the management of knee osteoarthritis: a systematic review of randomized controlled trials. Rheumatol Int 2017;37:1489–98. [DOI] [PubMed] [Google Scholar]
- 65. Wang X, Cicuttini F, Jin X, Wluka AE, Han W, Zhu Z, et al. Knee effusion‐synovitis volume measurement and effects of vitamin D supplementation in patients with knee osteoarthritis. Osteoarthritis and Cartilage 2017;25:1304–12. [DOI] [PubMed] [Google Scholar]
- 66. Perry TA, Parkes MJ, Hodgson R, Felson DT, O'Neill TW, Arden NK. Effect of vitamin D supplementation on synovial tissue volume and subchondral bone marrow lesion volume in symptomatic knee osteoarthritis. BMC Musculoskelet Disord 2019;20:76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Manoy P, Yuktanandana P, Tanavalee A, Anomasiri W, Ngarmukos S, Tanpowpong T, et al. Vitamin D supplementation improves quality of life and physical performance in osteoarthritis patients. Nutrients 2017;9:799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Alsubiaee KM, Alkhathlan KT, Omair A, Alenezi FM. The effects of vitamin D supplementation in patients with knee osteoarthritis: uncontrolled open label clinical trial. J Arthritis 2016;5:222. [Google Scholar]
- 69. Stockton KA, Mengersen K, Paratz JD, Kandiah D, Bennell KL. Effect of vitamin D supplementation on muscle strength: a systematic review and meta‐analysis. Osteoporos Int 2011;22:85971. [DOI] [PubMed] [Google Scholar]
- 70. Halfon M, Phan O, Teta D. Vitamin D: a review on its effects on muscle strength, the risk of fall, and frailty. BioMed Research Int 2015;2015:953241. [DOI] [PMC free article] [PubMed] [Google Scholar]