

Abstract
Agricultural strategies such as dairy intensification have potential to improve human nutrition through increased household food security. Increasing dairy productivity could also adversely affect infant and young child feeding (IYCF) practices because of increased maternal stress, demands on maternal time, and beliefs about the timing and appropriate types of complementary foods. Yet, few studies have looked rigorously at how interventions can affect young children (0–60 months). The study explores, within the context of rural dairy farming in Kenya, the relationship between level of household dairy production and selected IYCF practices using a mixed‐methods approach. Six focus group discussions with women involved in dairy farming investigated their attitudes towards breastfeeding, introduction of complementary foods and child diets. Ninety‐two households involved in three levels of dairy production with at least one child 0–60 months participated in a household survey. Quantitative results indicated that women from higher dairy producing households were more likely to introduce cow's milk to infants before they reached 6 months than women from households not producing any dairy. Themes from the focus group discussions demonstrated that women were familiar with exclusive breastfeeding recommendations, but indicated a preference for mixed feeding of infants. Evidence from this study can inform nutrition education programmes targeted to farmers participating in dairy interventions in rural, low‐income settings to minimise potential harm to the nutritional status of children.
Keywords: low‐income countries, infant and child nutrition, complementary feeding, breastfeeding
Introduction
One expected outcome of agricultural intensification strategies targeted towards the rural poor is that the increased food production will improve nutrition through improved household food security. How food production, food consumption and human nutrition are linked in agricultural have been described using five pathways as part of a generally accepted framework (World Bank, Agriculture and Rural Development Department 2007). With increased food production and income, agricultural strategies could directly improve nutrition through increased consumption of the food produced or indirectly through the purchase of other foods or expenditures on health care. Other pathways to improved nutrition through agriculture focus on empowering female household members to have more equitable decision‐making power over resources, given their positive role in household food security and health outcomes (Quisumbing et al. 1995; World Bank, Agriculture and Rural Development Department 2007).
Dairy intensification describes a particular agricultural strategy designed to help smallholder farmers out of poverty by increasing their access to resources to create a more productive and profitable dairy farm. Typically, dairy intensification combines multiple innovations, including but not limited to investment in higher‐yielding cows and improved cattle management, feeding systems and feeding production. In the case of smallholder dairying in sub‐Saharan Africa, women traditionally have held an important role in the collection, processing and sale of cow's milk as well as the care and feeding of animals (Curry 1996; Mullins et al. 1996; Tangka et al. 2000). Agricultural strategies that modify these smallholder systems are likely to lead to changes in female farmers' workload, control of income and intra‐household decision‐making power, which may have effects on the nutritional status of infants and young children in the households (Niemeijer et al. 1988; Huss‐Ashmore 1996; Tangka et al. 2000).
Undernutrition contributes to at least 35% of deaths in children less than 5 years of age globally (World Health Organization 2010). Animal source foods (ASF), such as cow's milk, contain several key micronutrients and high‐quality protein, which promote growth in children. Available income, preferences, decision making and intra‐household distribution of ASF may limit young children from consuming recommended amounts of ASF. Dairy interventions are one such agricultural strategy that is expected to address these deficiencies through increasing production and consumption of cow's milk, yet who in the household consumes the milk is an important factor in determining positive nutritional outcomes of the intervention. Even though cow's milk is considered to be an energy‐dense, high‐quality protein, the nutritional benefits do not necessarily apply to infants. Breast milk alone provides the nutrients needed for infants up to 6 months (Dewey 2003). The introduction of other foods, including cow's milk, in the child's first 6 months of life, is considered a suboptimal feeding practice. Suboptimal feeding practices in a child's first 2 years of life can increase the risks of morbidity, mortality, and poor growth and development (Black et al. 2008).
Studies of dairy strategies and dairy farming households have shown varying effects on household consumption and nutrition, but have provided little evidence on the effects on young children in these households. In two studies in Kenya, households that produced more dairy or owned cows did not necessarily have higher milk intakes than comparison households (Leegwater et al. 1991; Nicholson et al. 2003, 2004). Of these studies, the one that collected child anthropometric data and adjusted for child, household head and household characteristics found that the ownership of cows may have some positive association with child growth, like reducing the prevalence of stunting, but no association with wasting (Nicholson et al. 2003). The Leegwater et al. (1991) study reported that households participating in a dairy programme had greater daily energy intakes and household dietary diversity than control households, yet the study did not assess or adjust for potential confounding. In a separate study in Ethiopia, households that owned improved breeds of dairy cows had greater daily energy intakes and significantly higher intakes of protein, fat, carbohydrates, vitamin A and iron (Ahmed et al. 2000). Importantly, neither of the studies collected dietary data from children in the households. One study looked specifically at the diets of pre‐school children (1–4 years old) in India and reported that children living in the highest dairy‐producing households had higher energy and protein intakes, yet results did not appear to have been assessed or adjusted for potential confounding (Begum 1994). Results from the literature are inconclusive on whether dairy production is strongly associated with improved household diets, and even more so, without child‐level dietary data and adjustment for confounding, it is difficult to ascertain the effects on child nutrition.
As development programme implementers seek ways to improve child nutrition through agricultural interventions, evidence on the intra‐household nutritional effects of dairy interventions is needed to inform programme design. Our mixed‐methods study explores the influence of intensified dairy production on child nutrition by comparing young children (0–60 months) who lived in households not currently producing dairy (n = 30) to those in two other groups of households with higher levels of dairy production (n = 31, n = 31). We examined the association between level of household dairy production and five IYCF practices: (1) currently breastfeeding; (2) exclusive breastfeeding; (3) age of introduction of water; (4) age of introduction of cow's milk; and (5) age‐appropriate dietary diversity. Furthermore, qualitative data clarified the attitudes and beliefs of women involved in dairy farming towards age‐appropriate diets, breastfeeding and introduction of complementary foods.
Key messages
Dairy intensification is used as an agricultural strategy to address rural poverty, empower women and improve household nutrition, yet evidence is limited on the effects of dairy intensification on infant and young child feeding (IYCF) practices.
A study in rural Kenya compared children from households not producing dairy to those from households with higher levels of production to explore the effects on child nutrition.
Results indicate that higher levels of dairy production may adversely affect optimal IYCF practices, namely exclusive breastfeeding and age of introduction of cow's milk.
Dairy development programmes should consider incorporating nutrition education as an avenue to reinforce IYCF messages and promote nutrition.
Materials and methods
Participants
This paper presents findings from a mixed‐methods study conducted in three villages in Rift Valley Province, Kenya, where the East Africa Dairy Development project (EADD) was operating. The first‐phase goal of EADD was to move 1 million people in East Africa living on small 1–5‐acre farms out of poverty by increasing their access to agricultural innovations and services that would increase the production, profitability and marketability of their milk. The EADD model in Kenya was built around the establishment of hubs, which served as a one‐stop shop for dairy farmers to deliver and sell their milk and access agro‐vet services and credit. Reducing poverty and increasing food security were stated goals in the first phase of the project, but improving child nutrition was not. Our study was embedded in a larger research project, which was intended to inform efforts and future research of EADD's knowledge partner, the International Livestock Research Institute (ILRI), in the design of livestock interventions for smallholder households, like EADD, in order to maximise nutrition and food security benefits and minimise negative trade‐offs. The larger project was conducted in villages purposively selected based on the presence of EADD activities. The study area is inhabited predominantly by the Kalenjin tribe, with the main system of agriculture being mixed crop/livestock and subsistence farming. Details of this larger research project are described elsewhere (Shreenath et al. 2011).
Data collection and processing
Data collection occurred in June–July 2010 and consisted of separate focus group discussions with male farmers, female farmers and mothers of young children representing varying levels of dairy production. Findings from the focus groups informed development of the household survey (Fig. 1). For comparison, we designated, a priori, three dairy intensification groups based on current levels of dairy production. Using the household's average, daily milk production of the highest‐yielding cow in the herd in the past month, study participants were categorised as (1) no milk production (no milk); (2) milk production less than 6 litres per day (medium); and (3) milk production 6 or more litres per day (high).
Figure 1.
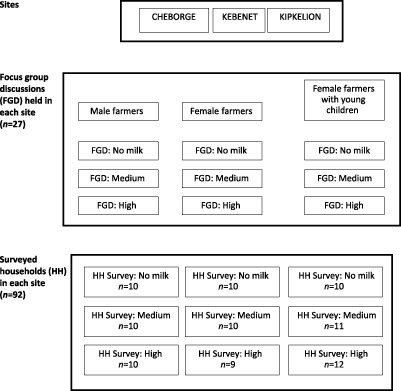
Data collection methods used in the larger research study, by site.
Focus group discussions
Focus group discussions were conducted in each site to explore community attitudes and experiences related to dairy production (sales and inputs); household income and investments; dietary habits; infant and young child feeding and care practices; zoonotic disease in animals and humans; and household decision making. Community gatekeepers, EADD staff and EADD interns recruited participants for the focus group discussions based on residence in or around the study sites, self‐identification as farmers and self‐reported current level of dairy production.
In the larger research project, 27 focus group discussions were conducted with an average of 12 people in each group, for a total participation of about 324 people. Focus groups were held separately for male farmers, female farmers and female farmers with young children. Each of these groups was further subdivided into three subgroups based on our defined levels of dairy production. Although efforts were made to group farmers by level of production, there was some variation by site. At one site, not enough women with young children were present to create three focus groups and in another site, two different focus groups were created for male farmers in the high production group. Two Kenyan university professors and a Kenyan PhD candidate with training and experience in qualitative research facilitated the focus group discussions in the language participants preferred, which was typically Kiswahili, Kalenjin, English or some combination of the three. Discussions lasted about 3.5 h, on average, and were audio recorded when participants gave permission (22 of 27 focus group discussions). At the end of the discussion, the groups convened to share what was discussed and facilitators answered participants' questions about human and animal health and nutrition. The researchers provided a small stipend (KES150; approximately USD1.75) to each participant to cover travel costs and a light snack.
Household survey
The basic sampling units for the household survey were households with young children (0–60 months) residing in the three study sites. As this was a pilot study, no sample size calculations were made. Rather, the aim was to survey 30 households in each site, with 10 households from each level of dairy production. Using OziExplorer, GPS mapping software, the team randomly generated 15 GPS points within a 5‐km radius from the EADD site hub in each village. The team used GPS devices to locate households at or near the GPS coordinates. Once the household was located, the team determined if the household met the eligibility criteria. Eligible households had at least one young child (0–60 months) and fit into one of the dairy production levels as previously defined. If the household was not eligible or the quota had been met for the specific production level, the household member was asked to identify other nearby households who met the selection criteria, and the team proceeded to those households. Due to time constraints, the team went to the next nearest household if no one was home at the household nearest the GPS coordinates. In two sites, the 15 GPS points were exhausted before the production level quota was met, so the team randomly generated five additional GPS points and followed this procedure until sample size had been reached. Ninety‐four households were surveyed across the three study sites. We excluded two questionnaires because (1) the respondent did not meet the selection criteria and (2) the respondent was unable to answer the majority of questions concerning the index child, leaving a sample size of 92.
A trained interviewer administered a structured household questionnaire with two parts. Part A, directed to the head of household, covered questions about household socio‐demographics; household income and investments; dairy production, sales and inputs; decision making; and syndromic surveillance of zoonotic disease in animals as well as humans. Part B, directed to the primary caretaker of the index child (the youngest child in the household), included questions about household dairy consumption with a focus on the index child; dietary diversity and food security; time allocation of the primary caregiver; decision making; and household health‐seeking behaviour and practices. If the head of household was not home and the primary caretaker of the index child could answer questions related to household income and farm activities and inputs, she completed both parts.
Data management and analysis
Infant and young child feeding practices
We selected five IYCF practices, defined below, as outcomes for the present study because they align with current, age‐specific feeding recommendations for young children (World Health Organization 2010). Following the recommendations is not only important for child growth and development, but evidence from observational studies suggests that suboptimal infant and young children feeding practices can increase the risk of morbidity and mortality in young children (Black et al. 2008). All the practices were coded as dichotomous (yes/no in a specified time frame) based on responses from the primary caretaker concerning the index child.
Currently breastfeeding was determined by an affirmative response to the question ‘Are you still breastfeeding?’
Breastfeeding was considered to be exclusive breastfeeding if the primary caretaker indicated that she did not begin giving any liquids or foods other than breast milk to the child before 6 months.
Early introduction of water was estimated by the response to a question regarding the age the child was first given water. If the response was prior to 6 months, the variable was coded as yes.
Early introduction of cow's milk was estimated separately by the response to a question about the age the child was first given cow's milk. Just as with water, if the response was prior to 6 months, the variable was coded as yes.
Age‐appropriate dietary diversity was estimated by a 24‐h recall of foods from a 13‐item list consumed by the child described in more detail in the next paragraph based on standard methodologies (Swindale & Bilinksy 2006) according to current WHO child feeding recommendations (World Health Organization 2010).
Individual dietary diversity
The individual dietary diversity score (IDDS) for the index children was calculated based on the number of different food groups consumed in the previous 24 h out of seven food groups: (1) grains; (2) dairy; (3) vitamin A‐rich fruits and vegetables; (4) other fruits and vegetables; (5) flesh foods; (6) eggs; and (7) legumes and nuts (Swindale & Bilinksy 2006). The IDDS typically includes an eighth food group – foods prepared with fat – which was excluded from our study. The IDDS can be used as a proxy measure for the nutritional quality of an individual's diet, food access and food consumption (Swindale & Bilinksy 2006; Food and Agricultural Organization 2008). The IDDS cannot be used to assess the quantity of food consumed, and a one‐time administration of the questionnaire does not capture seasonal variation in diets (Food and Agricultural Organization 2008). Age‐appropriate dietary diversity indicated that children older than 6 months consumed 4 or more food groups in the past 24 h. The child's ASF consumption score was based on the sum of two food groups ‘flesh’ and ‘eggs’ and excluded ‘dairy’ given the study population's relatively high consumption of dairy products.
Household food consumption
A food consumption score (FCS) was constructed from the data collected on the number of times individual food items were consumed in the household in the prior 7 days following the methodology recommended by the World Food Programme (WFP) (World Food Programme, Vulnerability Analysis and Mapping Branch 2008). The FCS is a method used by the WFP to describe food consumption patterns and assess household food security. The score was created by grouping the individual food items into seven food groups and summing the consumption frequencies within each group: (1) main staples (maize, maize flour, millet and other cereals); (2) pulses; (3) vegetables; (4) fruit; (5) meat and fish; (6) milk; and (7) oil. The FCS methodology includes two additional food groups – sugar and condiments – which were not included in our questionnaire. An ASF consumption score was based on the household's score for the ‘meat and fish’ food group, excluding the ‘milk’ food group given the context of the study population's relatively high consumption of dairy.
Household demographics and socio‐economic status
The following demographic and socio‐economic characteristics of the household head were included: age, gender, ethnicity, completed years of schooling and self‐reported literacy (whether or not respondent was literate in English or Kiswahili). A dichotomous variable was created to indicate whether or not the household head's primary work was in agriculture. A household asset score was created by summing the number of items owned from a list of six household items – cooker/gas stove, radio, television, mobile phone, motorcycle and bicycle. An agricultural asset score was created by summing the number of items owned from a list of six agricultural tools – hoe, spade, plough, sprayer pump, cart and water pump. The characteristics of the primary caretaker we included were age, completed years of schooling and whether or not the primary caretaker's primary work was in agriculture. Characteristics of the index child included the child's age and sex. Additional characteristics collected included survey site, number of household members, number of children under 16 years old living in the household, and type of and distance to primary water source.
The primary exposure variable of interest was level of dairy production, a three‐level ordinal variable, based on the respondent's total daily amount of milk produced by the best cow in the herd, as described previously.
Quantitative data analysis
Quantitative data cleaning and analyses were performed with SAS software (version 9.1; SAS Institute, Inc., Cary, NC, USA). The data set was checked for any missing and implausible values; observations with missing and implausible values were excluded from analysis. One implausible value for the timing of cessation of breastfeeding was excluded from analysis of cessation of breastfeeding (12‐month‐old child whose cessation of breastfeeding was reported as >12 months).
As a first step, we performed univariate analyses to describe the socio‐demographic, agricultural and dietary characteristics of the households, overall and across levels of dairy production and site. Means and SD were reported for continuous variables and frequency distributions for categorical variables. Differences between the level of production groups and between sites were compared using analysis of variance for continuous variables and Mantel–Haenszel chi‐square test for categorical variables. We considered P‐values <0.05 to be indicative of significance. Bivariate analysis was used to evaluate the association between the independent variable (level of dairy production) and the five outcomes of interest: currently breastfeeding, exclusive breastfeeding, early introduction of water, early introduction of cow's milk and age‐appropriate dietary diversity.
Multiple logistic regression was used to estimate the odds of each outcome by the household's level of dairy production, unadjusted and adjusted for the following covariates in each of the five models: site, age of primary caretaker, years of education of primary caretaker, age of child, sex of child, total number of household members, household assets score, acres of farm land owned and the household FCS. These covariates were selected because of their previously demonstrated significance to IYCF practices and relationship to the research question. These covariates were all continuous, except study site, which had three levels (Cheborge, Kebenet and Kipkelion); sex of the child (dichotomous); and acres of farm land owned (dichotomised by >2 and ≤2 acres). Collinearity was assessed by fitting a multivariate regression model for each feeding outcome and checking the variance inflation factor (VIF) for the variables in the model. Collinearity was not considered an issue as no VIF exceeded 10. Associations are presented as adjusted odds ratios and 95% confidence limits.
Preparation and analysis of qualitative data
Our qualitative analysis focused on research questions related to community attitudes of women towards IYCF practices. Although 27 focus group discussions were held in the large research study, our analysis focused on a subset of transcripts, specifically six groups with female farmers, both with and without young children, representing the three levels of dairy production. Because the themes discussed across groups varied little, we are confident that saturation was reached. Kenyan research assistants transcribed verbatim (except for identifiers) the digital recordings of the focus group discussions, and then translated the transcripts into English. A member of the study team (C.H.) with experience in qualitative research, fluent in Kiswahili and English, checked the accuracy of the transcriptions and English translations. A single coder (A.J.W.), trained in qualitative methods, read and analysed the transcripts using thematic analysis to label sections using codes developed inductively from the data and deductively from the research questions and focus group discussion guides in order to identify reoccurring themes. Using MAXQDA 10 to aid in the coding and analytical process (VERBI Software, Marburg, Germany), data on a particular theme could then be easily retrieved by code to draw conclusions. Our key findings are presented textually with quotes.
Ethical review
Ethical approval was obtained from the Institutional Review Board of Emory University. ILRI and the Government of Kenya have a standing agreement regarding human subjects' protections. Local community leaders were informed about the aim and procedures of the study. All study participants gave their verbal consent to participate after the study objectives, the intended use of the results, and confidentiality were explained to them.
Results
Findings from the household survey
Demographics
Of the 92 households surveyed, 12 had a child 0–5 months (13%), 12 had a child 6–11 months (13%), 25 had a child 12–23 months (27%) and 43 had a child 24–60 months. Households were socio‐demographically similar across levels of production in terms of characteristics of the household head, primary caretaker and child (Table 1). High dairy production households owned a greater number of household and agricultural assets and had larger farms than lower dairy production groups. In terms of the nutritional context of the households, the mean FCS for households was significantly higher in higher dairy producing households (P = 0.0007; Table 2). Conversely, the diets of children 6–60 months did not differ by level of dairy production (Table 2).
Table 1.
Characteristics of surveyed households, by level of dairy production (n = 92)
| No milk | Medium | High | |
|---|---|---|---|
| Households | |||
| Sample size | 30 | 31 | 31 |
| Household size (mean ± SD) | 5.3 ± 2.1 | 6.3 ± 2.2 | 6.3 ± 1.9 |
| Number of children, under age 16 (mean ± SD) | 2.9 ± 1.7 | 3.3 ± 1.7 | 3.6 ± 1.5 |
| Household assets score, out of 6 (mean ± SD)* | 1.9 ± 1.4 | 2.0 ± 0.9 | 2.6 ± 1.0 |
| Area of land owned, in acres (mean ± SD)* | 1.2 ± 1.6 | 3.1 ± 3.3 | 5.5 ± 9.6 |
| Agricultural assets score, out of 4 (mean ± SD)* | 1.4 ± 0.7 | 2.1 ± 1.1 | 2.4 ± 0.9 |
| Primary water source | |||
| Rivers/streams (%, n) | 66.7 (20) | 61.3 (19) | 51.6 (16) |
| Unprotected dug well/springs (%, n) | 16.5 (5) | 25.8 (8) | 6.5 (2) |
| Protected dug well (%, n) | 3.3 (1) | 6.5 (2) | 12.9 (4) |
| Piped into homestead (%, n) | 0 (0) | 3.2 (1) | 16.1 (5) |
| Other sources (%, n) | 13.3 (4) | 3.2 (1) | 12.9 (4) |
| Household head | |||
| Age (mean ± SD) | 40.8 ± 13.8 | 40.0 ± 11.0 | 41.5 ± 10.5 |
| Female (%, n) | 13.3 (4) | 12.9 (4) | 3.2 (1) |
| Ethnicity* | |||
| Kalenjin (%, n) | 73.3 (22) | 96.8 (30) | 100 (31) |
| Kisii (%, n) | 10 (3) | 3.2 (1) | 0 |
| Luhya (%, n) | 3.3 (1) | 0 (0) | 0 |
| Kikuyu (%, n) | 13.3 (4) | 0 (0) | 0 |
| Years of education (mean ± SD) | 9.4 ± 4.4 | 9.7 ± 4.8 | 10.8 ± 4.4 |
| Primary activity is not agriculture (%, n) | 35.7 (10) | 41.9 (13) | 32.3 (10) |
| Literate (%, n) | 83.3 (25) | 87.1 (27) | 90.3 (28) |
| Primary caretaker | |||
| Age (mean ± SD) | 28.8 ± 10.1 | 33.4 ± 10.1 | 32.0 ± 7.3 |
| Years of education (mean ± SD) | 7.7 ± 2.8 | 8.4 ± 3.6 | 9.7 ± 4.5 |
| Index child | |||
| Age, in months (mean ± SD) | 20.1 ± 15.5 | 20.1 ± 13.2 | 26.7 ± 17.5 |
| Male children (%, n) | 46.7 (14) | 38.7 (12) | 54.8 (17) |
*Analysis of variance for continuous variables and chi‐square test for categorical variables, P < 0.05.
Table 2.
Dietary characteristics for households and index children, by level of milk production ‡
| No Milk | Medium | High | |
|---|---|---|---|
| Household | |||
| Sample size | 30 | 31 | 31 |
| Food consumption score (mean ± SD) † | 32.8 ± 6.7 | 36.9 ± 4.8 | 38.1 ± 4.5 |
| ASF score, excluding milk (mean ± SD) † | 1.7 ± 0.85 | 2.7 ± 2.3 | 3.5 ± 2.2 |
| Milk consumption, in litres (median, IQR) § | – | 1 (1.5, 2.5) | 5 (3.0, 6.0) |
| Food insecure in past 12 months (%, n) | 33.3 (10) | 32.3 (10) | 19.4 (6) |
| Adults went without milk in past 30 days (%, n) † | 43.3 (13) | 22.6 (7) | 3.2 (1) |
| Child went without milk in past 30 days (%, n) † | 30.0 (9) | 9.7 (3) | 0 (0) |
| Index child* | |||
| Sample size | 25 | 28 | 27 |
| Dietary diversity score (mean ± SD) | 5.0 ± 1.2 | 4.7 ± 1.2 | 5.6 ± 0.9 |
| ASF score, excluding milk (mean ± SD) | 0.4 ± 0.6 | 0.3 ± 0.5 | 0.4 ± 0.6 |
| ASF was consumed, excluding milk (%, n) | 32.0 (8) | 32.1 (9) | 37.0 (10) |
ASF, animal source foods; IQR, interquartile range. *Index child in this case, youngest child in the household 6–60 months old. †Analysis of variance for continuous variables and chi‐square test for categorical variables, P < 0.05. ‡Individual dietary diversity for the index child was based on a recall of foods consumed by index children at least 6 months of age in the previous 24 h from a 13‐item list, administered to the primary caretaker of the child. The list of food items were grouped into seven food groups for analysis: (1) grains; (2) dairy; (3) vitamin A‐rich fruits and vegetables; (4) other fruits and vegetables; (5) flesh foods; (6) eggs; and (7) legumes and nuts. The dietary diversity score was calculated based on the number of different food groups consumed out of seven. §Household milk consumption data was only collected from medium and high milk‐producing households, n = 62.
IYCF practices
Of children 0–11 months, 100% were still breastfeeding. Among children <6 months, 58% were reported to be exclusively breastfeeding (Table 3). Only 18% of children 6–11 months had been exclusively breastfed through their first 6 months of age. Overall, data on the median age of introduction of non‐breast milk substances indicated that mothers were giving their child water at a median age of 3 months, followed by cow's milk and porridge at a median age of 4 months, and then mashed or semi‐solid foods at a median age of 6 months. Data on the median age of introduction of non‐breast milk substances indicated that cow's milk was introduced earliest among those in the high dairy group (3.5 months) and latest in the no milk group (6 months). Eighty per cent of children 6–60 months had age‐appropriate dietary diversity (Table 3).
Table 3.
IYCF practices, by child's age and by level of milk production
| No milk | Medium | High | |
|---|---|---|---|
| Currently breastfeeding (%, n) | |||
| Children 0–11 months (n = 24) | 100 (11) | 100 (7) | 100 (6) |
| Children 12–23 months (n = 25) | 20 (5) | 32 (8) | 20 (5) |
| EBF for first 6 months (%, n) | |||
| Children 0–6 months, currently EBF (n = 12) | 60 (3) | 66.7 (2) | 50 (2) |
| Children 6–11 months (n = 11) | 40 (2) | 0 (0) | 0 (0) |
| Children 12–23 months (n = 24) | 28.6 (2) | 10 (1) | 20 (2) |
| Median age of introduction of select complementary foods, in months (median, IQR) | |||
| Water (n = 77) | 4 (1, 6) | 3 (1, 7) | 2 (1, 6) |
| Cow's milk (n = 80) | 6 (2, 6) | 4 (3, 6) | 3.5 (2, 6) |
| Porridge (n = 81) | 6 (2, 6) | 3.5 (2, 6) | 4 (3, 6) |
| Mashed or semi‐solid foods (n = 76) | 7 (6, 9) | 6 (6, 8) | 6 (5, 8) |
| Age‐appropriate dietary diversity* (%, n) | |||
| Children 6–60 months, (n = 80) | 84 (21) | 68 (19) | 89 (24) |
IYCF, infant and young child feeding practices; EBF, exclusively breastfed; IQR, interquartile range. *Age‐appropriate dietary diversity indicates that children older than 6 months consumed 4 or more food groups in the past 24 h.
Associations of dairy production and IYCF practices
Increasing levels of dairy production was negatively associated with breastfeeding (exclusive) in univariate analysis and these associations remained significant when adjusted for other factors (Table 4). There was a significant association between high dairy production and the age of introduction of water. Infants from high dairy production households had a 12‐fold greater odds of receiving cow's milk early compared to the no milk production group. Level of dairy production and age‐appropriate dietary diversity were not associated in univariate or multivariate analyses.
Table 4.
Factors associated with level of dairy production and select IYCF practices
| Variable | Currently breastfed | EBF to 6 months | Water before 6 months | Cow's milk before 6 months | Age‐appropriate DD |
|---|---|---|---|---|---|
| Adjusted OR (95% Wald CL) | Adjusted OR (95% Wald CL) | Adjusted OR (95% Wald CL) | Adjusted OR (95% Wald CL) | Adjusted OR (95% Wald CL) | |
| Production level | |||||
| No milk (REF) | 1 | 1 | 1 | 1 | 1 |
| Medium | 0.01 (<0.001, 0.9) | 0.05 (0.01, 0.3)* | 3.6 (0.9, 15.0) | 3.0 (0.8, 11.1) | 0.2 (0.02, 1.2) |
| High | 0.04 (<0.001, 2.4) | 0.03 (0.003, 0.3)* | 5.8 (1.2, 29.0)* | 12.2 (2.3, 65.0)* | 0.3 (0.04, 3.4) |
| Site | |||||
| Cheborge (REF) | 1 | 1 | 1 | 1 | 1 |
| Kebenet | 1.4 (0.1, 27.0) | 0.1 (0.02, 0.9)* | 6.1 (1.5, 25.0)* | 0.9 (0.2, 3.4) | 0.7 (0.1, 4.1) |
| Kipkelion | 4.1 (0.2, 86.9) | 1.5 (0.4, 5.7) | 1.3 (0.4, 4.6) | 1.0 (0.3, 3.7) | 1.5 (0.2, 11.0) |
| Household size | 0.7 (0.4, 1.4) | 1.1 (0.7, 1.5) | 1.0 (0.8, 1.4) | 1.2 (0.9, 1.6) | 1.1 (0.7, 1.7) |
| Household asset score | 0.6 (0.3, 1.5) | 1.5 (0.8, 2.8) | 0.6 (0.3, 1.0) | 0.8 (0.5, 1.4) | 1.8 (0.8, 4.3) |
| FCS | 1.1 (0.9, 1.3) | 1.0 (0.9, 1.1) | 1.0 (1.0, 1.1) † | 1.0 (0.9, 1.1) | 1.1 (1.0, 1.3) † |
| Size of farm owned | |||||
| ≤2 acres (REF) | 1 | 1 | 1 | 1 | 1 |
| >2 acres | 0.6 (0.1, 5.7) | 9.1 (1.8, 46.6)* | 0.4 (0.1, 1.4) | 0.2 (0.04, 0.6)* | 4.8 (0.8, 29.4) |
| Index child | |||||
| Gender | |||||
| Male (REF) | 1 | 1 | 1 | 1 | 1 |
| Female | 5.8 (0.5, 71.5) | 1.0 (0.3, 3.7) | 1.2 (0.4, 3.5) | 4.1 (1.4, 12.6)* | 2.2 (0.5, 10.0) |
| Age, in months | 0.6 (0.4, 0.8)* | 1.0 (1.0, 1.0) † | 1.0 (1.0, 1.1) † | 1.0 (1.0, 1.1) † | 1.0 (1.0, 1.1) † |
| Primary Caretaker | |||||
| Age, in years | 1.3 (1.0, 1.7) † | 1.0 (0.9, 1.1) | 1.0 (0.9, 1.0) | 1.0 (1.0, 1.1) | 0.9 (0.8, 1.0) |
| Years of education | 0.8 (0.5, 1.1) | 1.1 (0.9, 1.4) | 0.9 (0.8, 1.1) | 1.0 (0.9, 1.2) | 0.9 (0.8, 1.2) |
CL, confidence limit; DD, dietary diversity; EBF, exclusively breastfed; FCS, food consumption score; OR, odds ratio. Logistic regression, adjusted for site, age of primary caretaker, years of education of primary caretaker, age of child, sex of child, total number of household members, household assets score, acres of farm land owned and the household food consumption score. An asterisk (*) indicates that the 95% CL does not contain 1. †95% CL included 1 after rounding, therefore, it was not considered significant.
Findings from the focus group discussions
Two key themes were identified in the analysis of the focus group discussions with female farmers and women with young children: (1) the important role of cow's milk in the diet of people of all ages but especially children and (2) the belief that cow's milk was a viable substitute to breast milk, especially if breast milk was perceived to be insufficient.
Important role of dairy in the diet
The description of typical diets of adults and children in these communities made it clear that fresh cow's milk was viewed as part of an ideal household diet across all levels of production. Fresh milk was added to tea, fermented into a drink called mursik, and the cream of the milk was added to vegetables. When cow's milk was available, it was commonly added to porridge, or uji, and fed to children under 2 years old. Many farmers in the medium and high production groups reported children and adults consuming fresh milk with or after meals. In the no milk production group, the importance of fresh milk consumption was frequently prefaced with statements about its relationship to the household's ability to afford milk. A woman with young children from the no milk production group explained, ‘You buy milk and put in to tea; if some of it remains it goes into the baby's uji.’ Indeed, milk was so important to the household diet, that a female farmer with young children from the medium production group explained how sometimes if later in the day she realised she needed more milk for family consumption and she had sold it all to the cooperative that morning, she would return to the cooperative to purchase milk, at a higher price than what she had sold it (24 ksh vs 18 ksh). The perceived health benefits of cow's milk likely explain why women believed it was important that young children consume milk. Some of the benefits they cited included physical growth, cognitive ability and a pleasant physical appearance. A woman from the high production group described how the lack of milk would result in negative health outcomes, ‘Without milk they won't be healthy. Their hair would get brown, the kids wouldn't get full and their legs would be like this [indicating bowed legs].’
Across production groups, women explained how they used their decision‐making power to ensure there was fresh cow's milk for the youngest children. Whether the households had plenty of milk or only a little, children's consumption was prioritised. When asked about the amount of milk used at lunchtime, a woman with young children from the high production group explained, ‘It will depend if the milk is there. If [the milk] is not there, you only give to [the] kids.’ A women with young children from the medium production group said, ‘I cook tea with some of the morning milk, but what remains is for my children. Since I have many children, I divide it and use it the whole day.’ Typically, the morning milking produced more cow's milk than the evening and it seemed common for households to keep the milk from the evening milking for household consumption, particularly for children. When that was not the case, a woman with young children from the high production group explained what she did instead, ‘If the evening milk is not enough you retain some of the morning milk for the young children.’
Reasons for mixed feeding
As seen from the household survey, mixed feeding of young infants is commonplace, with cow's milk, uji and water being the most common supplemental foods. The majority of women in the focus group discussions reported being taught to exclusively breastfeed their infants up to 6 months, but when probed, many acknowledged that they practice mixed feeding, giving breast milk plus water, cow's milk or uji. When probed, many women indicated they started giving their infants cow's milk or uji, some as early as 1 or 2 months. ‘From one month to 6 months, we prefer for them to either breastfeed or drink maize flour porridge [uji],’ said a woman with young children from the no milk production group. It is important to note that it was not uncommon for cow's milk to be added to the child's uji, so the distinction between the introductions of the two may not always be clear.
The mothers in the focus group discussions provided several reasons for introducing non‐breast milk substances, especially cow's milk, prior to 6 months. Some mothers seemed to think breast milk was inadequate for the child and so the child needed additional foods. One mother from the medium production group said, ‘If you don't have enough milk, it is wise to give him uji … That's why we do it.’ When asked about what else should be given to the child if the breast milk was insufficient, women in several of the groups said to give the children cow's milk or add cow's milk to uji. One woman in the medium production level group explained there was an exception, ‘But if you have sufficient milk … you cannot introduce them before 6 months.’
Some of the reasons provided in the group discussions for having insufficient breast milk included not eating enough foods or not enough healthy foods, working too hard or illness. A woman with young children in the no milk production group explained, ‘Sometimes you as a mother don't feed well, so even when you breastfeed no milk comes out.’ A woman with young children from the high production group said, ‘If the work is more, we are saying breast milk is not enough for the kid because of a lot of work.’ In particular, the mother's work appeared to influence breastfeeding practices. Women working in casual labour are paid by the amount of work accomplished (i.e. weight of tea leaves picked), so any interruption during their work day could mean less money earned. During a discussion about duration of exclusive breastfeeding, a woman from the no milk production group said, ‘But you know, we who do casual labour sometimes start to give them porridge early.’ On the other hand, women explained how some of their responsibilities did not impede their breastfeeding practices. A woman with young children from the medium production group explained, ‘You know, when you are grazing [cattle], you just sit and watch, so the child will just breastfeed.’ Another woman with young children from the no milk production group explained how she managed breastfeeding while working on the farm: ‘If he or she cries while you are tilling, you stop first and breastfeed.’
Unfortunately, the data collected do not provide insights beyond these reasons as to why women practised mixed feeding for infants less than 6 months. Some of the data suggest that the type of work women were involved with influenced their IYCF practices, sometimes facilitating breastfeeding on demand, although the transcripts do not distinguish whether or not the mothers were talking about children less than 6 months of age, or older. Other women explained how their workload diminished break milk production, so they felt that introducing other liquids and foods was necessary. Less frequently mentioned reasons provided in the focus group discussions for early cessation of breastfeeding included child illness and related loss of appetite, maternal illness necessitating medication with instruction not to breastfeed, and return to studies or work.
Discussion
We used data from a mixed‐methods study in three communities in Rift Valley Province, Kenya, to explore the relationship between a household's level of dairy production and IYCF practices. Overall, a low proportion of children in this study were exclusively breastfed through their first 6 months of life, and mothers expressed a preference for mixed feeding. Our results indicated that engaging in higher levels of dairy production was associated with significantly lower odds that children would be exclusively breastfed to 6 months. In particular, mothers from households in high levels of dairy production were more likely to introduce water and cow's milk into their child's diet at an earlier age than mothers from households in medium or no dairy production households. Our findings support the hypothesis that higher levels of dairy production may adversely affect optimal IYCF practices, namely exclusive breastfeeding and introduction of water and cow's milk, but do not affect other child feeding practices such as currently breastfeeding or dietary diversity.
In spite of the knowledge that exclusive breastfeeding was important, mothers expressed a preference for mixed feeding with uji and cow's milk, corroborating recent studies in Kenya showing that exclusive breastfeeding practices are not in line with WHO recommendations, and like the mothers in our study, there appears to be a preference for mixed feeding (Gewa et al. 2011; Kimani‐Murage et al. 2011). The preference for mixed feeding young infants is concerning, as physiologically, an infant's gastrointestinal, renal, and neurophysiological systems are not mature enough to process foods or liquids other than breast milk before 6 months. Further starchy foods, like uji, as well as cow's milk, can cause diarrhoea and contribute to iron deficiency (Akre 1989; Dewey 2003). Our qualitative findings suggest that to some extent, intensifying work loads of mothers and food insecurity may lead mothers to perceive that their milk is insufficient to meet the needs of their infants. Previous studies in this region have also observed an association between food insecurity and mother's perceived capacity to produce sufficient breast milk (Gewa et al. 2011; Kimani‐Murage et al. 2011; Nor et al. 2011; Webb Girard et al. 2012a).
As smallholder farmers intensify their dairy systems, the intensified systems will require more labour and in this population, women are likely to absorb the additional workload until the household can afford to hire additional labourers (Mullins et al. 1996). If women perceive a direct relationship between the type of work and breast milk sufficiency, women may believe their ability to exclusively breastfeed will be compromised as workload increases. Demands for labour may also increase the time mothers leave the care and feeding of their infant to other caregivers, a theme that needs further exploration. All of this illustrates the importance of contextual understanding of gender roles in dairy systems in order to design programmes that will limit any negative effects dairy intensification may have on maternal and child nutrition.
An unexpected finding in this study was the lack of a relationship between level of dairy production and children's dietary diversity, even though we observed a positive relationship between level of dairy production and household food consumption patterns. It is likely that no relationship was observed among children because overall, most of the children older than 6 months in this sample (80%) had met the recommended minimum for dietary diversity. This estimate contrasts sharply with the Kenyan DHS in which 55.9% of children 6–23 months in Rift Valley Province met the minimum dietary diversity requirements (Kenya National Bureau of Statistics & ICF Macro 2010). A study in neighbouring Western Kenya, which used a 7‐day recall period and counted food items, instead of food groups found that 45% of pre‐school children had very low dietary diversity and 30.6% of children had not consumed dairy in the previous 7 days (Ekesa et al. 2008). Differences may be explained by the use of different data collection tools, but the availability and preference for milk in our study population, as well as the preferential allocation to children highlighted in the focus groups, appears to be a contributing factor to improved dietary quality for young children regardless of level of dairy production. This finding is positive given what is known about the importance of ASF consumption, particularly milk, and child health (Allen 1993; Grillenberger et al. 2003; Neumann et al. 2003; Dror & Allen 2011).
Although we did not compare households involved in a dairy intervention to households not involved, our results could be used to make hypotheses about the potential household effects of dairy interventions. Dairy interventions are often promoted as a strategy for dietary diversification, so the lack of an association in this study between children's dietary diversity and level of dairy production is notable. Although dietary diversity is only one measure of nutrition, our results are consistent with assessments that have found the evidence of effectiveness of livestock interventions to be insufficient or variable for improving infant and child nutrition unless improving nutrition is an explicitly stated goal or includes nutrition education(Bhutta et al. 2008; Masset et al. 2012).
To our knowledge, this study is one of the first to test the relationship between the level of dairy production and IYCF practices. The collection of child‐level data provides important information about how dairy intensification could influence the nutrition of young members of dairy households. Unlike other studies looking specifically at dairy cow ownership and production, our study adjusted for other factors related to dairy production in the examination of the association between level of dairy production and IYCF practices. To our knowledge, there is little qualitative research on the relationship between dairy production and IYCF practices. The qualitative portion of this study provided insights into intra‐household food allocation, food preferences for different age groups and barriers to optimal IYCF practices.
Our study had some limitations, some of which are explained by the fact that the large research project was not designed to answer specific questions about IYCF practices. First was the small sample size, particularly for infants and children under 2 years old, which contributed to the large confidence limits around some of the point estimates in the models. Furthermore, we are aware that some recall bias of events occurring during the child's first 6 months was introduced given that nearly half of the children in our sample were older than 2 years old. A larger sample of infants would allow us to draw more conclusions about IYCF practice variations across age groups. Secondly, the survey lacked questions for some important feeding practices, such as the use of pre‐lactal feeds, bottle feeding and feeding frequency. The lack of these data precluded the development and multivariate modelling of a feeding practice index, the findings of which could have compared with other studies (Armar‐Klemesu et al. 2000; Arimond & Ruel 2002; Moursi et al. 2009). Thirdly, due to time and logistical constraints, we did not use a standard 24‐h recall method for capturing food consumption of the child and the household overall. Finally, this was a small study conducted in a particular area of Kenya where dairying is common and dairy is an integral part of the local diet, so results may not be generalisable beyond the study population. Nonetheless, we believe the findings may have implications for other dairy interventions.
Recent reviews suggest that agricultural interventions that include a nutritional education component can strengthen the intervention's ability to improve child nutrition (Berti et al. 2004; Leroy & Frongillo 2007; Randolph et al. 2007; Webb Girard et al. 2012b). Education in this context should focus on striking a balance between promoting milk as a good source of nutrition for young children and emphasising the potential adverse health consequences of introducing milk and other foods and liquids to infants before 6 months of age. Given the important role of dairy in the traditional diet, education should be culturally appropriate and sensitive to cultural beliefs regarding the importance of dairy for children. In order to promote optimal breastfeeding practices, exclusive breastfeeding messages should be tailored with information regarding the infant's inability to digest cow's milk and emphasise the additional benefits of breast milk for promoting infant immunity and protection from diarrhoea. Strategies should focus on encouraging breastfeeding mothers to consume more milk themselves, emphasising how this directly benefits the mother and the infant, more so than giving milk to infants. There are a variety of options for delivering these messages. Some have proposed that female agricultural extension workers could be mobilised to advise women on dairy farming and serve as links to other child nutrition and health services (United States Agency for International Development's Infant and Young Child Nutrition Project 2011). Indeed, community‐based delivery of messages is considered an effective strategy to promote exclusive breastfeeding (Tylleskar et al. 2011).
In conclusion, our study suggests that agricultural strategies, like dairy intensification, may have mixed effects on households. Unintended negative effects on infants are possible, as suggested in this study, if child feeding practices are modified in accordance with increased availability of cow's milk or if intensified dairy production increases the demands on women's time and workload. Agricultural strategies such as dairy intensification may provide a strategic venue for reinforcing IYCF messages on exclusive breastfeeding and support female farmers within the context of the programme to ensure benefits for young child nutrition.
Source of funding
Fieldwork was supported by a grant from the Global Health Institute at Emory University, Atlanta, USA, and the International Livestock Research Institute, Nairobi, Kenya.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Contributions
AWG, KMY, UR and CN designed the study; AWG, KMY, UR and CN supervised the fieldwork; AJW analysed the data, wrote the manuscript and had primary responsibility for the final content. All authors read and approved the final manuscript. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of Emory University, the International Livestock Research Institute, or the International Food Policy Research Institute.
Acknowledgements
We are grateful to the International Livestock Research Institute field team for all their hard work and commitment during fieldwork in Kenya and to the transcription team who transcribed and translated the qualitative data. We thank Thomas Randolph, Jemimah Njuki, Isabelle Baltenweck, Delia Grace and Peter Little for their thoughtful inputs on study design and Craig Hadley for inputs on study design and assistance with quality assurance of translation of the transcripts. Finally, we thank all the Kenyan farmers who contributed their time to participate in this project.
References
- Ahmed M., Jabbar M. & Ehui S. (2000) Household‐level economic and nutritional impacts of market oriented dairy production in the Ethiopian highlands. Food and Nutrition Bulletin 21, 460–465. [Google Scholar]
- Akre J. (1989) Physiological development of the infant and its implications for complementary feeding. Bulletin of the World Health Organization 67 (Suppl.), 55–67. [PMC free article] [PubMed] [Google Scholar]
- Allen L.H. (1993) The nutrition CRSP: what is marginal malnutrition, and does it affect human function? Nutrition Reviews 51, 255–267. [DOI] [PubMed] [Google Scholar]
- Arimond M. & Ruel M.T. (2002) Summary Indicators for Infant and Child Feeding Practices: An Example from the Ethiopia Demographic and Health Survey 2000 . Food and Nutrition Technical Assistance Project, Academy for Educational Development: Washington, D.C.
- Armar‐Klemesu M., Ruel M.T., Maxwell D.G., Levin C.E. & Morris S.S. (2000) Poor maternal schooling is the main constraint to good child care practices in Accra. Journal of Nutrition 130, 1597–1607. [DOI] [PubMed] [Google Scholar]
- Begum J.M. (1994) The impact of dairy development on protein and calorie intake of pre‐school children. Indian Journal of Medical Sciences 48, 61–64. [PubMed] [Google Scholar]
- Berti P.R., Krasevec J. & FitzGerald S. (2004) A review of the effectiveness of agriculture interventions in improving nutrition outcomes. Public Health Nutrition 7, 599–609. [DOI] [PubMed] [Google Scholar]
- Bhutta Z.A., Ahmed T., Black R.E., Cousens S., Dewey K., Giugliani E. et al (2008) What works? Interventions for maternal and child undernutrition and survival. Lancet 371, 417–440. [DOI] [PubMed] [Google Scholar]
- Black R.E., Allen L.H., Bhutta Z.A., Caulfield L.E., de Onis M., Ezzati M. et al (2008) Maternal and child undernutrition: global and regional exposures and health consequences. Lancet 371, 243–260. [DOI] [PubMed] [Google Scholar]
- Curry J. (1996) Gender and livestock in African production systems: an introduction. Human Ecology 24, 149–160. [Google Scholar]
- Dewey K. (2003) Guiding Principles for Complementary Feeding of the Breastfed Child. Pan American Health Organization and World Health Organization: Washington, DC. [Google Scholar]
- Dror D.K. & Allen L.H. (2011) The importance of milk and other animal‐source foods for children in low‐income countries. Food and Nutrition Bulletin 32, 227–243. [DOI] [PubMed] [Google Scholar]
- Ekesa B.N., Walingo M.K. & Abukutsa‐Onyano M.O. (2008) Influence of agricultural biodiversity on dietary diversity of preschool children in Matungu Division, Western Kenya. African Journal of Food Agriculture, Nutrition, and Development 8, 390–404. [Google Scholar]
- Food and Agricultural Organization (2008) Guidelines for measuring household and individual dietary diversity, version 4 . Food and Agricultural Organization: Rome.
- Gewa C.A., Oguttu M. & Savaglio L. (2011) Determinants of early child‐feeding practices among HIV‐infected and noninfected mothers in rural Kenya. Journal of Human Lactation 27, 239–249. [DOI] [PubMed] [Google Scholar]
- Grillenberger M., Neumann C.G., Murphy S.P., Bwibo N.O., Van't Veer P., Hautvast J.G. et al (2003) Food supplements have a positive impact on weight gain and the addition of animal source foods increases lean body mass of Kenyan schoolchildren. Journal of Nutrition 133 (Suppl 2), 3957S–3964S. [DOI] [PubMed] [Google Scholar]
- Huss‐Ashmore R. (1996) Livestock, nutrition, and intrahousehold resource control in Uasin Gishu district, Kenya. Human Ecology 24, 191–213. [Google Scholar]
- Kenya National Bureau of Statistics & ICF Macro (2010) Kenya Demographic and Health Survey, 2008–2009. Kenya National Bureau of Statistics and ICF Macro: Calverton, MD. [Google Scholar]
- Kimani‐Murage E.W., Madise N.J., Fotso J.C., Kyobutungi C., Mutua M.K., Gitau T.M. et al (2011) Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health 11, 396–406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leegwater P., Ngolo J. & Hoorweg J. (1991) Dairy Development and Nutrition . Food and Nutrition Planning Unit, Ministry of Planning and National Development African Studies Center: Nairobi.
- Leroy J.L. & Frongillo E.A. (2007) Can interventions to promote animal production ameliorate undernutrition? Journal of Nutrition 137, 2311–2316. [DOI] [PubMed] [Google Scholar]
- Masset E., Haddad L., Cornelius A. & Isaza‐Castro J. (2012) Effectiveness of agricultural interventions that aim to improve nutritional status of children: systematic review. British Medical Journal 344, d8222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moursi M.M., Treche S., Martin‐Prevel Y., Maire B. & Delpeuch F. (2009) Association of a summary index of child feeding with diet quality and growth of 6–23 months children in urban Madagascar. European Journal of Clinical Nutrition 63, 718–724. [DOI] [PubMed] [Google Scholar]
- Mullins G., Wahome L., Tsangari P. & Maarse L. (1996) Impacts of intensive dairy production on smallholder farm women in coastal Kenya. Human Ecology 24, 231–253. [Google Scholar]
- Neumann C.G., Bwibo N.O., Murphy S.P., Sigman M., Whaley S., Allen L.H. et al (2003) Animal source foods improve dietary quality, micronutrient status, growth and cognitive function in Kenyan school children: background, study design and baseline findings. Journal of Nutrition 133 (Suppl. 2), 3941S–3949S. [DOI] [PubMed] [Google Scholar]
- Nicholson C.F., Mwangi L., Staal S.J. & Thornton P.K. (2003) Dairy Cow Ownership and Child Nutritional Status in Kenya . Annual Meeting: Montreal, Quebec, Canada on July 27, 2003. Agricultural and Applied Economics Association. Montreal, Quebec.
- Nicholson C.F., Thornton P.K. & Muinga R.W. (2004) Household‐level impacts of dairy cow ownership in Coastal Kenya. Journal of Agricultural Economics 55, 175–195. [Google Scholar]
- Niemeijer R., Geuns M., Kliest T., Ogonda V. & Hoorweg J. (1988) Nutrition in agricultural development: the case of irrigated rice cultivation in West Kenya. Ecology of Food and Nutrition 22, 65–81. [Google Scholar]
- Nor B., Ahlberg B.M., Doherty T., Zembe Y., Jackson D. & Ekstrom E.C. (2011) Mother's perceptions and experiences of infant feeding within a community‐based peer counselling intervention in South Africa. Maternal and Child Nutrition 8, 448–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quisumbing A.R., Brown L.R., Feldstein H.S., Haddad L. & Pena C. (1995) Women: The Key to Food Security . International Food Policy Research Institute: Washington, DC.
- Randolph T.F., Schelling E., Grace D., Nicholson C.F., Leroy J.L., Cole D.C. et al (2007) Invited review: role of livestock in human nutrition and health for poverty reduction in developing countries. Journal of Animal Science 85, 2788–2800. [DOI] [PubMed] [Google Scholar]
- Shreenath S., Watkins A.J., Wyatt A.J., Yearous‐Algozin A., Ramakrishnan U., Webb Girard A. et al (2011) Exploratory Assessment of the Relationship between Dairy Intensification, Gender and Child Nutrition among Smallholder Farmers in Buret and Kipkelion Districts, Kenya . International Livestock Research Institute: Nairobi.
- Swindale A. & Bilinksy P. (2006) Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide (v. 2) . Food and Nutrition Technical Assistance Project and Academy for Educational Development: Washington, DC.
- Tangka F.K., Jabbar M.A. & Shapiro B.I. (2000) Gender Roles and Child Nutrition in Livestock Production Systems in Developing Countries: A Critical Review. International Livestock Research Institute: Nairobi. [Google Scholar]
- Tylleskar T., Jackson D., Meda N., Engebretsen I.M.S., Chopra M., Diallo A.H. et al (2011) Exclusive breastfeeding promotion by peer counsellors in sub‐Saharan Africa (PROMISE‐EBF): a cluster‐randomised trial. Lancet 378, 420–427. [DOI] [PubMed] [Google Scholar]
- United States Agency for International Development's Infant and Young Child Nutrition Project (2011) Nutrition and Food Security Impacts of Agricultural Projects – A Review of Experience . United States Agency for International Development: Washington, DC.
- Webb Girard A., Cherobon A., Mbugua S., Kamau‐Mbuthia E., Amin A. & Sellen D.W. (2012a) Food insecurity is associated with attitudes towards exclusive breastfeeding among women in urban Kenya. Maternal and Child Nutrition 8, 199–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webb Girard A., Self J.L., McAuliffe C. & Olude O. (2012b) The effects of household food production strategies on the health and nutrition outcomes of women and young children: a systematic review. Paediatric and Perinatal Epidemiology 26, 205–222. [DOI] [PubMed] [Google Scholar]
- World Bank, Agriculture and Rural Development Department (2007) From Agriculture to Nutrition – Pathways, Synergies, and Outcomes . World Bank: Washington, DC.
- World Food Programme, Vulnerability Analysis and Mapping Branch (2008) Food Consumption Analysis – Calculation and use of the Food Consumption Score in Food Security Analysis . World Food Programme: Rome.
- World Health Organization (2010) Indicators for Assessing Infant and Young Child Feeding Practices Part 2: Measurement . World Health Organization: Geneva.