

Abstract
In 1996, a Food and Agricultural Organization/World Health Organization expert panel proposed the development of food‐based dietary guidelines (FBDGs) that would be unique and specific to the needs of the populations of different countries. In 1997, a South African FBDG Working Group was initiated to develop a single set of FBDGs aimed at optimal nutrition for all South Africans older than 5 years. Thereafter, additional working groups investigated the development of FBDGs for specific priority groups including HIV/AIDS sufferers, the elderly, pregnant and lactating women and children under 5 years. This resulted in the formation of an expert paediatric FBDG Working Group in 2000, in Cape Town with the task to develop paediatric FBDGs (PFBDGs) for children younger than 5 years. However, it was decided to raise the 5‐year‐age limit to 7 years, which corresponds to one of the recommended dietary allowance (RDA) cut‐offs for both genders and that would cover most pre‐schoolers. Ultimately, three age subcategories were identified for developing specific PFBDGs, i.e. 0–6 months, 6–12 months and 12–84 months. In May 2003, after thorough review of the relevant literature, discussions with various stakeholders and pre‐testing for comprehensibility, a set of preliminary PFBDGs for each of the subcategories was approved by the Working Group to be subjected to consumer testing. The proposed guidelines were considered to be the most appropriate ones for each age group, based on scientific and local evidence, and were evaluated utilizing qualitative methodologies. The results of these data are presented and discussed below. However, further testing is required for the diverse groups in the country.
Keywords: food‐based dietary guidelines, nutrition counselling, pre‐school children, South Africa
The World Declaration and Plan of Action for Nutrition was adopted at the International Conference on Nutrition in Rome in 1992 and includes a number of goals aimed at eliminating or substantially reducing famine and famine‐related deaths, chronic malnutrition, micronutrient deficiencies and diet‐related communicable and non‐communicable diseases. One strategy that was suggested to achieve these goals is the promotion of appropriate diets and lifestyles. In response to this and recognizing the need for more effective nutrition education interventions, the World Health Organization (WHO) (1998) and Food and Agricultural Organization (FAO) of the United Nations convened an international consultation in 1995 to discuss the development of food‐based dietary guidelines (FBDG) 1 as an effective nutrition education tool to promote appropriate diets and lifestyles. Different countries have, since then, begun to adapt their guidelines to make them food‐based.
Development of FBDGs for South Africans (7 years and older)
Like many developing countries, South Africa (SA) has through the years ‘borrowed’ dietary guidelines from other countries like the USA and UK. These borrowed guidelines were not necessarily based on the prevailing nutrition and health status of the South African population, but rather focused on two main areas – undernutrition in low‐income groups, utilizing a three food group approach, or chronic illnesses of lifestyle in affluent (predominantly white) communities, utilizing a five food group approach. The compatibility of these guidelines to the availability, accessibility and/or affordability of foods and/or to the different socio‐economic, cultural and lifestyle needs of the South African communities, was not given due consideration as cited by Love et al. (2001).
In May 1997, the Nutrition Society of South Africa initiated the formation of the SA FBDG Work Group. Members came from a diverse background of experience and training in nutrition, including representation from the National Department of Health (Nutrition Directorate), non‐governmental organizations, academia, agricultural producer organizations, food industry, professional associations and the Medical Research Council (MRC). The mandate of the SA FBDG Work Group was to develop new dietary guidelines that would adequately address the nutrition transition experienced by many South Africans, as well as to optimize nutrition in disadvantaged as well as affluent communities (Love et al. 2001).
To achieve this, the internationally accepted WHO/FAO process for developing FBDGs was adopted (Box 1) (World Health Organization 1998). Accordingly, each guideline was developed to meet the recommended criteria (World Health Organization 1998), namely: affordable, practical, attuned to food availability, culturally sensitive, positive and non‐prescriptive, sustainable and environmentally friendly.
Box 1. WHO/FAO process for development of FBDGs
-
•
Form a representative working group
-
•
Set nutritional objectives based on nutrition‐related diseases, food availability and food intake patterns of the country
-
•
Formulate, through full discussion, a preliminary set of FBDGs that could be useful
-
•
Pilot‐test understanding of FBDGs with consumer groups, and revise as needed
-
•
Compile technical support documents for each FBDG
-
•
Finalize technical support documents, submit to national and international interest groups for comment, and consider changes
-
•
Conclude, adopt, publish and disseminate final report
-
•
Implement FBDGs
-
•
measure impact of FBDGs on eating patterns
FAO, Food and Agricultural Organization; FBDGs, food‐based dietary guidelines; WHO, World Health Organization.
During 1998, following an extensive review of the literature on local nutrition‐related public health concerns and food consumption patterns of South Africans, draft sets of guidelines were debated through a wide consultative process (Vorster et al. 2001). During 1999 and 2000, a preliminary set of 11 guidelines were subject to wide‐scale consumer research testing across all spectra within SA [urban and rural areas as well as cultural groups representative of the South African population, namely, black, white, Indian and ‘coloured’ (mixed origin)] (Love et al. 2001). The results of these studies assisted in refining and adapting the dietary guidelines to improve their understanding and application by South African consumers (Love 2001). A final set of FBDGs for healthy South Africans 7 years and older was approved and adopted as national dietary guidelines for SA by the National Department of Health on 9 May 2003 (Written communication, National Department of Health, Nutrition Directorate, Pretoria, South Africa) (Box 2).
Box 2. Food‐based dietary guidelines for healthy South Africans older than 7 years
-
1
Enjoy a variety of foods
-
2
Be active
-
3
Make starchy foods the basis of most meals
-
4
Eat plenty of vegetables and fruits everyday
-
5
Eat dry beans, peas, lentils and soy regularly
-
6
Chicken, fish, milk, meat or eggs could be eaten daily
-
7
Eat fats sparingly
-
8
Use salt sparingly
-
9
Drink lots of clean, safe water
-
10
If you drink alcohol, drink sensibly
-
11
Use food and drinks containing sugar sparingly and not between meals
Development of food‐based dietary guidelines for South Africans (younger than 7 years)
Early in 2000, the SA FBDG Work Group (Vorster et al. 2001) initiated the formation of additional Work Groups to develop FBDGs for specific priority groups including people with HIV and AIDS, the elderly, pregnant and lactating women, and infants and young children. The decision to develop separate FBDGs for infants and young children was based on the unique nutritional needs of children with regard to growth and development, and the diet‐related public health issues specific to South African children. As a result, a paediatric FBDG (PFBDG) Work Group was initiated to develop FBDGs for infants and young children (with an initial age cut‐off of younger than 5 years). A representative (in terms of culture and paediatric experience) intersectoral PFBDG Work Group 2 was convened in late 2000, and was independently approved as being satisfactorily inclusive by an expert from the WHO (Dr. P. Pietinen).
The PFBDG Work Group followed the recommended WHO/FAO process as used for the development of the ‘adult’ guidelines (Box 1) (World Health Organization 1998), with the PFBDG messages being directed to the child carer, rather than the child him/herself. The process followed is represented diagrammatically in Fig. 1.
Figure 1.
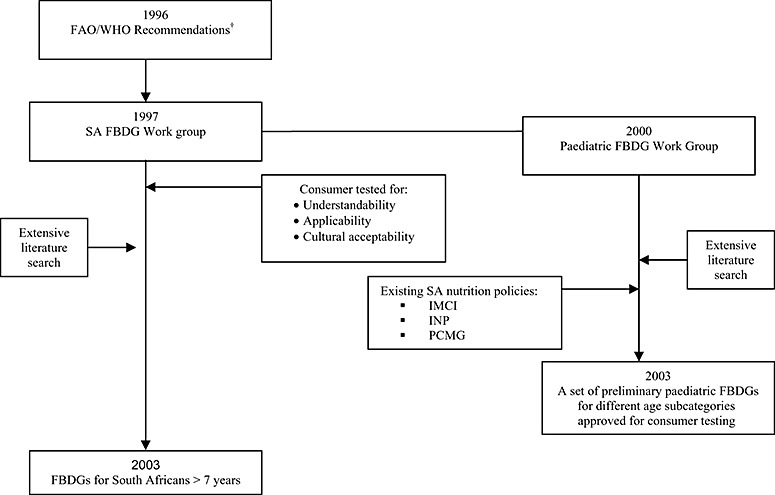
The process of developing paediatric food‐based dietary guidelines (PFBDG) for different age sub‐categories in South Africa (SA). FAO, Food and Agricultural Organization; IMCI, Integrated Management of Childhood Illnesses; INP, the Integrated Nutritional Programme; PCMG, Paediatric Case Management Guidelines; WHO, World Health Organization. †Source: World Health Organization (1998).
The PFBDG Work Group also made a subsequent recommendation to the SA FBDG Work Group that the cut‐off age for the healthy adult guidelines should be raised to 7 years from the initial 5 years. This recommendation was motivated as the older age would cover most South African pre‐school children for which the school‐going age was raised to 7 years in 2004.
A further recommendation was made by the PFBDG Work Group to subcategorise the 0–7‐year age group into three age categories for the paediatric guidelines; younger than 6 months, 6–12 months and 1–7 years to better reflect the identified public health issues as well as specialized needs and stages of development of these three age subcategories. Birth to 2 years of age is considered the critical period for optimal growth, health and behavioural development (Dewey 2001). It is difficult to reverse any damage that may result from nutritional deficiencies during this period, and this can have serious effects on the child's life. As the WHO prescribes exclusive breastfeeding for babies aged younger than 6 months of age (Dewey 2001), it was recommended that this be the first age subcategory for the PFBDGs. Although the WHO guidelines very clearly indicate that breastfeeding may continue beyond 2 years, it was decided to make the second age category to younger than a year and not 2 years as it is also recommended that ‘by 12 months most children can eat the same types of foods as consumed by the rest of the family’ (Dewey 2001) and fits in with the WHO dietary reference values. 3 It was a heavily debated issue and it was decided to address the continuation of breastfeeding in supportive documentation of the 6–12‐month age group, enabling guidelines for 1–7 years to focus on family meals.
According to the literature (Steyn et al. 1993; The South African Vitamin A Consultative Group et al. 1994; Cameron 1997; Delport et al. 1997; Labadarios, 2001), the main public health issues identified for South African children younger than 2 years include early cessation of breastfeeding, early weaning, stunting, micronutrient deficiencies (vitamin A, iron), adverse outcomes associated with TB and HIV, poor immunization coverage, allergies/intolerances, dental caries, infrequent feeding, poor hygiene practices, diarrhoeal and parasitic infections and insufficient care/nurturing. For those older than 2 years, additional micronutrient deficiencies become apparent (i.e. calcium, iodine, vitamin B2, zinc and folate), inadequate growth, as well as other infections such as malaria, upper/lower respiratory tract infections and cholera.
PFBDG: identification of key concepts
As the WHO prescribes exclusive breastfeeding for babies aged 0–6 months of age (Dewey 2001), it was essential that this message be addressed. Other key concepts regarding feeding identified for the group of younger than 6 months were methods of feeding (cup versus bottle), and the use of breast milk substitutes.
Children between the ages of 6 and 12 months pose a unique challenge to nutrition educators as this is the age marked by the gradual introduction of complementary foods while the child is still being breastfed. This is also the age where gross motor skills develop and self‐feeding becomes possible. Other key concepts identified and discussed were excessive intakes of fruit juice and milk, early introduction of cow's milk, food allergies and intolerances, the introduction and use of a cup as opposed to a bottle for fluids, small stomach size (and thus small frequent meals) and nutrient densities of foods. As indicated previously, once a wide range of solids have been successfully introduced, the next step is to try and encourage children older than 12 months to partake in usual family meals, thereby providing a stepping stone to the ‘adult’ guidelines to be followed from age 7 years.
As indicated above, the public health issues identified in South African children are not all necessarily food‐based. For total health and well‐being, it was therefore decided that other aspects such as nurturing and caring for children, oral hygiene and clinic attendance for growth monitoring and immunizations were essential as key concepts across all three age categories.
PFBDG: preliminary messages
Key concepts identified for each age subcategory were discussed during a consultative workshop session that included members of the PFBDG Work Group as well as external partners from Maternal and Child Health, Primary Health Care and Oral Health, who had not been involved in the conceptualisation thus far. During this workshop, preliminary messages per age subcategory were brainstormed based on the evidence gathered and key concepts previously identified. To illustrate, suggested breastfeeding messages for the younger than 6‐month age subcategory included, ‘Breastfed is best fed’; ‘Feed your baby breast milk only for the first 6 months’; ‘Exclusively breastfeed your baby’; ‘Feed your baby only breast milk for the first 6 months’. Other relevant issues that were debated included: to whom the messages should be aimed; the ever‐increasing and important underlying problem of unknown HIV status of mothers and their infants (discussed in greater detail in the final article of this supplement); contravention of the code for marketing of breast milk substitutes if mentioning alternative feeding; as well as taking the relevant political and social factors specific to the South African context into consideration.
Messages included in existing nutrition or nutrition‐related local policy documentation was also taken into consideration to ensure standardization of the nutrition message to the consumer. Policy documents that were referred to (discussed in greater detail in the article that deals with nutrition intervention at primary health care (PHC) facilities by Hendricks et al.), were the Integrated Management of Childhood Illnesses, the Integrated Nutritional Programme and Paediatric Case Management Guidelines.
Overall, 14 preliminary messages were suggested for the younger than 6‐month group, 11 for the 6–12‐month group and 15 for the 1–7‐year group. This set of suggested PFBDGs was then subjected to screening to determine which messages would be more appropriate for further consumer testing to prevent overlapping with similar messages. Screening was conducted among mothers/carers (n = 31) of children in the target age range who were conveniently sampled from a clinic in a low socio‐economic area. Mothers/carers were individually interviewed and asked to explain what each message meant to them in their own words. Each mother/carer was given a randomly assigned number of possible messages for the age group that her child represented. This screening was the first phase of screening the messages to be consumer‐tested.
Simultaneously, this set of PFBDGs was also surveyed among 21 randomly selected South African dietitians. Content validity of the messages was investigated using a self‐administered questionnaire, which first explained the process of the PFBDGs and then asked for opinions on all of the possible messages. The questionnaire included an open‐ended section with suggestions for alternative messages and phrasing.
Findings of the screening and self‐administered questionnaires were discussed by the PFBDG Work Group and a preliminary set of PFBDGs was produced for each age subcategory (Box 3. Preliminary PFBDGs: younger than 6 months, Box 4. Preliminary PFBDGs: 6–12 months, Box 5. Preliminary PFBDGs: 1–7 years).
Box 3. Preliminary PFBDGs: younger than 6 months
-
1
Enjoy time with your baby
-
2
Breastfeeding is best for your baby for the first 6 months
-
3
Clean your baby's mouth regularly
-
4
Take your baby to the clinic every month
PFBDGs, paediatric food‐based dietary guidelines.
Box 4. Preliminary PFBDGs: 6–12 months
-
1
Enjoy time with your baby
-
2
From 6 months start giving your baby small amounts of solid foods
-
3
Increase your baby's meals to five times a day
-
4
Keep on breastfeeding your baby
-
5
Offer your baby clean safe water regularly
-
6
Teach your baby to drink from a cup
-
7
Take your baby to the clinic every month
PFBDGs, paediatric food‐based dietary guidelines.
Box 5. Preliminary PFBDGs: 1–7 years
-
1
Encourage children to eat a variety of foods
-
2
Feed children 5 small meals a day
-
3
Make starchy foods the basis of a child's main meals
-
4
Children need plenty of vegetables and fruit every day
-
5
Children need to drink milk every day
-
6
Children can eat chicken, fish, meat, eggs, beans, soya or peanut butter every day
-
7
If children have sweet treats or drinks, offer small amounts with meals
-
8
Offer children clean, safe water regularly
-
9
Take children to the clinic every 3 months
-
10
Encourage children to play and be active every day
PFBDGs, paediatric food‐based dietary guidelines.
At this point, it is important to once again point out that the guidelines were meant to meet the FAO/WHO criteria of being affordable, practical, attuned to food availability, culturally sensitive, positive and non‐prescriptive, sustainable and environmentally friendly (World Health Organization 1998). Guidelines cannot be longwinded and need to be clear, short, precise and stand‐alone messages – it is the supportive documentation that provides the additional information and further explanations. It is imperative though that these guidelines do not differ completely to international guidelines. If then a comparison is made with the WHO guiding principles for complementary feeding of the breastfed and non‐breastfed child under 2 years of age (Dewey 2001), it is clear that if not addressed by the suggested guideline, the information is meant to be covered by the supportive documentation for that specific guideline as indicated in Table 1.
Table 1.
Comparison of the preliminary PFBDG and the WHO guiding principles
| PFBDG < 6 months | PFBDG 6–12 months | PFBDG 1–7 years | WHO guiding principles |
|---|---|---|---|
| 1. Enjoy time with your baby | 1. Enjoy time with your baby | 3. Responsive feeding | |
| 2. Breastfeeding is best for your baby for the first 6 months | 4. Keep breastfeeding your baby | 1. Duration of exclusive breastfeeding and age of introduction of complementary foods (6 months)/ 2. Maintenance of breastfeeding (2 years)/ 10. Feeding during and after illness | |
| 6. Teach your baby to drink from a cup | |||
| 2. From 6 months start giving your baby small amounts of solid foods | 1. Duration of exclusive breastfeeding and age of introduction of complementary foods (6 months)/ 6. Food consistency/9. Use of vitamin‐mineral supplements or fortified products for infant and mother | ||
| 3. Increase your baby's meals to five times a day | 2. Feed children five small meals a day | 5. Amount of complementary food needed/7. Meal frequency and energy density | |
| 1. Encourage children to enjoy a variety of foods | 4. Safe preparation and storage of complementary foods/ 8. Nutrient content of complementary foods/ 10. Feeding during and after illness | ||
| 3. Clean your baby's mouth regularly | 5. Offer your baby clean, safe water regularly | 8. Offer children clean, safe water regularly | |
| 4. Take your baby to the clinic every month | 7. Take your baby to the clinic every month | 6. Take children to the clinic every 3 months | |
| 7. Encourage children to be active every day | |||
| 3. Make starchy foods the basis of a child's main meals | |||
| 4. Children need plenty of vegetables and fruits every day | 8. Nutrient content of complementary foods | ||
| 5. Children need to drink milk every day | 2. Maintenance of breastfeeding (2 years) | ||
| 9. Children can eat chicken, fish, meat, eggs, beans, soya or peanut butter every day | 8. Nutrient content of complementary foods | ||
| 10. If children have sweet treats or drinks, offer small amounts with meals | 8. Nutrient content of complementary foods |
PFBDG, paediatric food‐based dietary guideline; WHO, World Health Organization.
PFBDG: consumer research testing
As cited by Love et al. (2001) although dietary guidelines can be a powerful nutrition education tool, available evidence suggests that they are commonly misunderstood and applied inappropriately by the public. Consumer testing is therefore recommended to ensure that the public is aware of, understands, and can implement the dietary guidelines. The FAO/WHO expert panel recommends testing to be performed among the general public by using focus group discussions of 6–8 individuals as a means of gathering qualitative data. A sufficient range and number of groups should be consulted to yield a fair representation of the study population (World Health Organization 1998).
Consumer testing of the preliminary PFBDGs therefore aimed to target women from different language groups, including a cross‐section of socio‐economic backgrounds within South African society. Thereby, women with children younger than 7 years of age from diverse language and culture groups in the country and from various socio‐economic backgrounds were to be purposively represented. Qualitative research methodology was planned utilizing focus group discussions to determine comprehension of and the ability to practically apply the PFBDGs. This would facilitate the gaining of insight into beliefs, thoughts, attitudes, motives and behaviours of participants with children in each of the three age subcategories (Katzenellenbogen et al. 1997; World Health Organization 1998). Focus group discussions were to be held with as many diverse groups as possible in terms of language, culture, socio‐economic status (SES) and age of child but in homogenous groups for each discussion (6–10 mothers per group). Refreshments were offered to the mothers during the 60–90‐min discussions (tea and biscuits), but no further compensation was provided. Data collection was to be to the point of data saturation. A discussion guide was to be followed by the facilitator and an observer was to be present to transcribe the discussion taking place in the home language of the group. All discussions were to be recorded, preferably via video recordings to enable further transcription for analysis purposes as well as triangulation of the data. Informed consent had to be obtained from each participant as well as permission for recording of the sessions. Analysis of the data was to be performed by collating the transcribed data from observer notes and videotapes and grouping into themes.
This qualitative research protocol was initially offered to both senior undergraduate and postgraduate students studying at the three universities involved in the PFBDG Work Group (University of the Western Cape, University of Cape Town and Stellenbosch University) with financial support from the MRC. All nine universities involved in dietetic training in SA have subsequently been invited to partake in this research opportunity.
Limited consumer testing of the preliminary PFBDGs has, thus far, been conducted using the proposed protocol outlined above, but has been among mothers with children within all three subcategories. Each study has made use of videotaped focus group discussions according to predetermined discussion guides to determine the comprehensibility of the preliminary guidelines for each of the age groups as well as the practical applicability and cultural acceptability. Unfortunately, all testing thus far has been in only one of the nine provinces of SA, the Western Cape Province. The guidelines for babies younger than 6 months were tested in urban and non‐urban areas in the Western Cape by a group of three undergraduate BSc Dietetic IV students under the guidance of study leaders at Stellenbosch University (SU). The guidelines for the 6–12 months group were tested in the urban and rural areas of Oudtshoorn and the guidelines for 1–7 years, in the City of Cape Town. Both of the latter studies were conducted in fulfilment of a Master of Nutrition degree at SU under the supervision of study leaders from SU and the MRC.
Although these results are preliminary and not representative at this stage, the authors felt it was important to share the experience gained thus far. Results from each of the studies will be submitted for publication in due course. Generally, the focus groups were convened according to settlement type, SES and ethnicity to reflect the Western Cape population, using purposive sampling. Focus groups were conducted in the home language of the participants. English‐ and Afrikaans‐speaking focus groups were conducted in all age groups, whereas Xhosa groups were only used in the two groups younger than a year. Few volunteers were found in the Xhosa‐speaking groups though, indicating under‐representation of this group, which is a major limitation for finalization of the guidelines. Consumer testing has to date been conducted on 229 consumers (89 mothers with children younger than 6 months, 64 with children aged 6–12 months and 76 between 1 and 7 years). Preliminary results from these first three studies are provided to enable those wanting to consumer‐test guidelines, some insight regarding the data collected to date. Results indicate the perceptions of the mothers and the recommendations from the investigators from each study to the PFBDG Work Group, who will only be able to finalize the guidelines once representative consumer‐testing has been completed.
PFBDG for infants younger than 6 months
Results for the younger than 6 months preliminary PFBDGs were that, in general, mothers understood them and could reportedly implement them.
Guideline 1: breastfeeding is best for your baby during the first 6 months
Constraints like having to go back to work, being tired and not having enough milk were indicated regarding implementing the first guideline. As found in other studies in SA, disturbingly, the term ‘exclusive’ is not understood by the consumer. It was also reported that it was not clear whether other foods could also be included at this stage; therefore, suggestions were made to include ‘only’ to this breastfeeding guideline: ‘Breastfeeding is the only feed your baby needs for the first 6 months’. The investigators also recommended that a guideline should be included regarding demand breastfeeding.
Guideline 2: clean your baby's mouth regularly
Generally, the guideline seemed to be completely misunderstood and it was suggested that it be reworded to indicate overall hygiene or left out completely.
Guideline 3: take your baby to the clinic every month
Mothers seemed to understand this guideline, but indicated frustration with long waiting times and transport although realising the importance of the message. Regular visits and reasons for visits were suggested to be included in the supportive documentation.
Guideline 4: enjoy time with your baby
This guideline was well‐accepted and understood by all. Interestingly, the role of the father was discussed and suggested for inclusion into the supportive documentation.
PFBDG for infants 6–12 months
Results from the 6–12‐month group found that although perceived as important by the majority of respondents, some of the preliminary guidelines were not well‐understood without explanation.
Guideline 1: enjoy time with your baby
The reason most often mentioned for not being able to comply with this guideline was tiredness and lack of leisure time preventing participants from enjoying time with their babies.
Guideline 2: from 6 months start giving your baby small amounts of solid foods
Unaffordability and unavailability of complementary foods were indicated to be the most important hindrances to compliance with this guideline. However, cereal added to milk in feeding bottles at an early age was considered by some not to be ‘real’ solid food and some participants admitted to starting with this as early as 2–3 months. Another custom among some people in rural areas to give ‘meelbol’ 4 to infants was reported. Although a number of participants were uncertain about the meaning of ‘a small amount’, most agreed that it would be that quantity that a child would eat without being forced. Although cereals, fruit and vegetables, being good sources of energy and some nutrients, especially if enriched, were correctly perceived as suitable first foods for infants of 6–12 months old, it is a cause for concern that complementary foods such as chicken, meat and egg yolk, rich in protein, iron and zinc, were seldom mentioned and should therefore be emphasized in the supportive documentation.
Guideline 3: gradually increase your baby's meals to five times a day
Participants experienced the most problems interpreting this guideline, with more than half of participants indicating that a baby should not eat more than three times per day. A lack of knowledge and absence from home during the day were perceived as the main obstacles to compliance with this guideline. Three meals were generally considered to be the norm, although most agreed that they would give their child mid‐morning or mid‐afternoon snacks of bread or fruit. These were not considered to be ‘proper’ meals. In two of the rural discussion groups, participants also admitted that they were unsure of the meaning of ‘gradually’. Alternatives for this guideline were suggested.
Guideline 4: keep on breastfeeding your baby
Applicability of the guideline on prolonged breastfeeding seemed the most problematic and a number of reasons were offered for inability to comply with continuation of breastfeeding. Milk that was perceived as ‘being too little’ or ‘has dried up’ was cited as the most common constraint, while being employed, being too tired, not having enough time, the infant preferring a bottle and being instructed by a general practitioner not to breastfeed were, respectively, cited by some participants as constraints.
Guideline 5: offer your baby clean safe water regularly
The only reason offered for not being able to apply the water guideline was uncertainty about the safety of water in the area. Most participants thought that only boiled, cooled water was safe for an infant, while a few thought that water from a tap was also safe. Part of the discussion regarding this guideline, included the concept of fluoride as water fluoridisation could play a major role in oral health and would be included in the supportive documentation. ‘Fluoride’ was a concept found to be almost unknown among participants. In two of the groups, it was suggested that the guideline could be made more understandable by changing the wording to ‘Give your baby clean, boiled and cooled drinking water several times a day’.
Guideline 6: teach your baby to drink from a cup
The perceived messiness of teaching a small child to drink from a cup was the only constraint mentioned for this guideline.
Guideline 7: take your baby to the clinic every month
Fear of criticism was the major reported deterrent for participants from attending the clinic.
PFBDG for infants 1–7 years
In the older than a year group, the mothers seemed to understand the proposed PFBDGs as intended, but the rationale behind the guidelines was not always known.
Guideline 1: encourage children to eat a variety of foods
The guideline was well‐accepted and understood.
Guideline 2: feed children five small meals a day
Problems similar to the 6–12‐month group discussions regarding frequency of meals were found where mothers reported that children ‘graze’ throughout the day, generally in the form of three meals and two snacks. Again it seemed that the wording was more problematic than the message itself and mothers would like to see the guideline modified.
Guideline 3: make starchy foods the basis of a child's main meals
All mothers understood what the term ‘starchy foods’ meant and they understood the reason for eating such foods. The more educated mothers, however, disagreed with the wording of the guideline, saying that the term is old‐fashioned and that ‘carbohydrates’ and the term Glycemic Index should be used instead. Suggestions for alternate, more understandable wording of the guideline were given.
Guideline 4: children need plenty of vegetables and fruit every day
All mothers indicated that this guideline is important, yet they would like to have portions specified. Mothers reported that as long as children get either fruit or vegetables during the day, there is no need for them to get both. Affordability in the lower SES was mentioned as a constraint to this guideline.
Guideline 5: children need to drink milk every day
The dairy guideline resulted in uncertainty among the mothers regarding the advantages and disadvantages of milk intake. The role of misinformation regarding especially allergies should be addressed.
Guideline 6: children can eat chicken, fish, meat, eggs, beans, soya or peanut butter every day
Mothers agreed that protein is an important component of the diet. They thought the guideline to be a sound one because it uses the word ‘can’ instead of ‘must’ and protein sources are listed in the guideline. Minor alterations to the wording were suggested. All mothers give their children protein foods, with soya being the least used.
Guideline 7: if children have sweet treats or drinks, offer small amounts with meals
The responses to this guideline were mostly negative. Mothers felt that the word ‘with’ implies that sweet treats and drinks should form a part of every meal, and that the word ‘after’ would be better. Most of the mothers do give their children some sweet treats or drinks to prevent their children from overindulging at parties. Mothers did feel that moderation is important, and that a fruit or yoghurt can be offered as something sweet. Alternate wording was offered and mention was made of the fact that sweets should not be allowed at playgroup/crèche/pre‐primary school and that carbonated drinks companies should not be allowed to sell their products at playgroup/crèche/pre‐primary schools.
Guideline 8: offer children clean, safe water regularly
This was well understood.
Guideline 9: take children to the clinic every 3 months
The same constraints to clinic attendance were mentioned in this group as for the 6–12 months group.
Guideline 10: encourage children to play and be active every day
The guideline was well‐accepted and understood.
In conclusion, recommendations from all three studies completed at this time indicate that further testing is required in other languages and cultural groups around SA so as to capture its diversity. Furthermore, the supportive documentation should include extensive and appropriate information as identified by the consumers as well as incorporating the WHO guiding principles for complementary feeding of the breastfed and non‐breastfed child under 2 years of age (Dewey 2001) (Table 1).
PFBDG: the way forward
In a parallel process to finalize the PFBDGs in as timely a manner as possible, the PFBDG Work Group is producing the evidence‐based technical support documentation for the PFBDGs. Once the consumer testing of the PFBDGs is complete, i.e. further testing in other languages and cultures, a final draft of the guideline and supportive documentation will be submitted together with the technical support documents to the National Department of Health for approval and adoption as national dietary guidelines for South Africans younger than 7 years.
Dissemination of these guidelines through the development of consumer materials and media awareness campaigns will also have to be conducted, including training of health professionals to ensure that standardized messages are provided to the consumer.
Acknowledgements
The dedication, hard work and support of all members of the PFBDG Working Group as well as the undergraduate and postgraduate students who were and will be involved in consumer testing the draft PFBDGs is acknowledged.
Footnotes
Qualitative statements that express dietary goals in terms of foods, not nutrients. They are evidence‐based, simple and practical (action‐oriented). They are intended for the consumer and in some countries, form the basis of nutrition policies and programmes.
The intersectoral Working Group comprised individuals from the three local Universities (Departments of Dietetics, Dentistry and Child and Adolescent Health), Red Cross War Memorial Children's Hospital, the food and private sector hospital industries, the South African Medical Research Council, the Nutrition Directorate at provincial and regional level, as well as the chairperson of the SA FBDG Work Group.
The WHO dietary references values use the following age cut‐offs: 0–6 months, 6–12 months, 1–3 years, 3–5 years and 5–7 years.
Bread flour is baked in the oven to slightly brown it and is afterwards mixed with water to give as porridge or with more water as an alternative to milk.
References
- Cameron N. (1997) Comments on: growth, feeding practices and infections in black infants. South African Medical Journal 87, 1024–1025. [PubMed] [Google Scholar]
- Delport S.D., Becker P.J. & Bergh A. (1997) Growth, feeding practices and infections in black infants. South African Medical Journal 87, 57–61. [PubMed] [Google Scholar]
- Dewey K. (2001) Guiding Principles for Complementary Feeding of the Breastfed Child. WHO, Pan American Health Organization: Geneva. [Google Scholar]
- Katzenellenbogen J.M., Joubert G. & Abdool Karim S.S. (eds) (1997) Section D: common approaches in epidemiology In: Epidemiology – A Manual for South Africa, pp 176–181. Oxford University Press Southern Africa: Cape Town. [Google Scholar]
- Labadarios D. (ed.), Steyn N., Maunder E., MacIntyre U., Swart R., Gericke G. et al. (2001) The National Food Consumption Survey (NFCS)‐children aged 1–9 years, South Africa, 1999. South African Journal of Clinical Nutrition 14, 62–75. [Google Scholar]
- Love P. (2001) South African food‐based dietary guidelines. South African Journal of Clinical Nutrition 14, 42–43. [Google Scholar]
- Love P., Maunder E., Green M., Ross F., Smale‐Lovely J., Charlton K. (2001) South African food‐based dietary guidelines: testing of the preliminary guidelines among women in KwaZulu Natal and the Western Cape. South African Journal of Clinical Nutrition 14, 9–19. [Google Scholar]
- Steyn N.P., Badenhorst C.J., Nel J.H. & Ladzani R. (1993) Breastfeeding and weaning practices of Pedi mothers and the dietary intakes of their pre‐school children. South African Journal of Food Science and Nutrition 5, 10–13. [Google Scholar]
- The South African Vitamin A Consultative Group (SAVACG ) (1995) Children Aged 6–71 Months in South Africa, 1994: Their Anthropometric, Vitamin A, Iron and Immunisation Coverage Status. SAVACG, Isando. [PubMed] [Google Scholar]
- Vorster H.H., Love P. & Brown C. (2001) Development of food‐based dietary guidelines for South Africa: the process. South African Journal of Clinical Nutrition 14(Suppl.), S3–S6. [Google Scholar]
- World Health Organization (1998) Preparation and use of food‐based dietary guidelines In: Report of a joint FAO/WHO Consultation, Technical Report Series 880, pp 27–44. WHO: Geneva. [PubMed] [Google Scholar]