

Abstract
The study objective was to understand the role of traditional Awajún foods in dietary quality and the potential impacts on growth of Awajún infants and young children 0–23 months of age. Research took place in April and May of 2004, along the Cenepa River in six Awajún communities. Anthropometry estimated nutritional status for 32 infants (0–23 months). Repeat dietary recalls and infant feeding histories were completed with 32 mothers. Adequacy of the complementary foods was compared with World Health Organization guidelines. Anthropometry indicated a high prevalence of stunting (39.4% of infants and young children), with nutritional status declining with age. Half of the Awajún mothers practised exclusive breastfeeding. Dietary recalls and infant food histories suggested that many of the infants were getting adequate nutrition from complementary foods and breastfeeding; however, there was variation in breastfeeding and complementary feeding practices among the mothers. Complementary feeding for young children 12–23 months generally met nutrient recommendations, but mean intakes for iron, zinc, calcium and vitamin A were inadequate in infants 6–11 months. Traditional foods provided 85% of energy and were more nutrient dense than market foods. Appropriate infant and complementary feeding was found among some women; however, given the range of feeding practices and introduction of market foods, health promotion targeting infant and young child feeding is warranted.
Keywords: breastfeeding, infant and young child feeding, complementary feeding, Amazon, traditional food, Indigenous Peoples
Introduction
Indigenous Peoples have survived thousands of years with traditional diets high in biodiversity and which meet nutrient needs for a continuous population. As such, traditional diets of Indigenous People must be regularly accessible and acceptable, and often protective of the local ecosystem (FAO/WHO 2002). Traditional foods for an indigenous population can be defined as all acceptable foods provided by the natural resources of a particular cultural group (Kuhnlein & Receveur 1996). Exclusive breastfeeding until 6 months of age (meaning only breast milk) is promoted as the optimal nutrition and immune protection for this period. At 6 months of age, introduction of nutrient‐dense complementary foods should begin, with continued breastfeeding until at least 2 years of age (PAHO/WHO 2004). Complementary feeding interventions can improve child growth when well targeted with culturally appropriate messages (Dewey & Adu‐Afarwuah 2008). Breast milk is an essential traditional food available and accessible to all cultures around the world, and thus is part of a traditional food system; breastfeeding is also affordable, environmentally friendly and culturally appropriate in addition to providing nutrition and immune protection (Léon‐Carva et al. 2002).
Key messages
-
•
Exclusive breastfeeding for 6 months needs to be promoted in Rio Cenepa Awajún communities.
-
•
Given the decline in nutritional status documented here in the first 2 years of life, there is a need for targeted nutrition interventions for the Awajún to promote nutrient‐dense complementary foods, taking advantage of healthy local foods.
-
•
Traditional local foods, especially breast milk and animal source foods, need to be promoted, as market foods and commercial milks in their colorful packaging, but with fewer nutritional advantages, are increasingly available in the community.
-
•
Health promotion with traditional foods need to include policies that protect access and availability of healthy, culturally appropriate animal and plant foods; these policies need to include land protection for use by the Awajún.
The Amazon basin spans five countries and is home to many groups of Indigenous Peoples. While some studies have reported on the nutritional status and health of Indigenous Peoples in the Amazon, very little is known about infant feeding practices. The Awajún are the largest group of Indigenous Peoples in the Peruvian Amazon (SICNA 1999) who practise a subsistence lifestyle along the tributaries of the upper Marañon River (Berlin & Markell 1977). The rates of stunting [height‐for‐age Z‐score (HAZ) < −2] among children 3–5 years of age were found to be 49%, and severe stunting (HAZ < −3) was 26% (Roche et al. 2007a). When chronic malnutrition (as measured by the percentage of children under 5 years of age with HAZ less than −2) is greater than 20%, intervention is required and when above 40%, it becomes a critical public health concern (World Bank 2006). In a subsequent larger study in the Amazonas district, the prevalence of chronic malnutrition for children under 3 years was found to be 33.4%, and above 65% had anaemia, with the Cenepa showing higher levels (Huamán‐Espino & Valladares 2006).
Although wide variation was evident in our earlier report, the average diet of the 3–5‐year‐olds of this Awajún population showed overall adequacy, with low rates of wasting and underweight in this age group (Roche et al. 2007a). To understand the high prevalence of stunting among the Awajún children, it was essential to describe the breastfeeding and complementary feeding practices of infants and children under 2 years of age, with special consideration for the role of traditional foods.
Materials and methods
Study communities
The study took place in the communities of Cocoaushi, Mamayaque, Nuevo Tutino, Tuutin, Pagki and Nuevo Kanam, along the lower Cenepa River area in the Amazonas district of Peru, South America, with populations ranging from 60 to 638 people per community (SICNA 1999). The study was conducted during April and May 2004, known by the Awajún as the season of heavy rains and scarce fishing. Traditional food lists were established through key informant interviews and community focus groups. These food lists were the first step in developing a food composition table for local Awajún foods to be used in calculating dietary intakes. All mothers with children 0–2 years of age were invited to participate in the infant dietary intake and food history component of the study. In the majority of cases, there was one mother per household. When a mother had two or more children between 0–2 years, one child was randomly selected. Approximately 80% of invited women participated. Lack of time, scepticism of the study and the need for caring of family members were given as reasons for non‐participation. A limitation to the study was the non‐random convenience sample; however, according to local health promoters, there appeared to be no participation bias and the final sample was determined to be a good representation of the communities (M. Roche, unpublished observations).
Anthropometry
Length was assessed in the infants and young children using a recumbent height board (WHO 1995). Weight was measured to a precision of 0.1 kg with a digital standing scale with the mother holding the child and then weighing the mother and subtracting the weight of the mother. Age was reported by the mother and confirmed with the health card and/or community records of births when available. In order to understand nutritional status throughout infancy, statistical comparisons of the length for age Z‐scores were calculated for age groups 0–5 months, 6–11 months and 12–23 months. Using SPSS 15.0 for Windows (SPSS 2006), a one‐way analysis of variance (ANOVA) was used to compare mean nutritional status of the age groups defined above. A quantile‐quantile (Q‐Q) plot to test for normality was performed. Anthro 2005 was used to calculate and analyse anthropometry using the World Health Organization (WHO) growth curves (WHO 2006).
Dietary recalls
Methodology for obtaining dietary data was reported earlier (2007a, 2007b). Essentially, standardized 24‐hour dietary recalls on two non‐consecutive days, with a separation of 3–4 days were obtained from all mothers for 32 infants and young children (aged 0–23 months) (Basiotis et al. 1987). Mothers provided information on whether the food was obtained through family production, purchase or donation. To estimate portion sizes, mothers showed their cups, plates and an infant pinig (clay feeding bowl with spout made especially for an infant) as references for quantifying food consumption. Community members were asked to show specific local food items to help establish reference weights for local foods. These were weighed with a food balance scale with a precision of 1 g. Community focus groups helped establish local portion sizes specifically for infants and young children as well as the usual preparation methods. Mothers reported the consumption by infants and young children, including frequency of breastfeeding. To enhance recall ability for mothers and children, times of daily activities such as going to the chacra (fields) were used as prompts to help define which foods were given to the infant as part of a multiple pass method. Dietary recall data were reviewed and entered with food codes corresponding to the Instituto de Investigacion Nutricional (IIN) food composition table of Peruvian foods (IIN 2004). Food composition analysis was done by the IIN for suri and eep, and these foods were added to the IIN Peruvian food composition database. Since several Amazon foods were missing food composition data in the database, five foods were estimated using the US Department of Agriculture (USDA) food tables (USDA 2004), and composition for four foods was substituted for foods with unknown nutrient data by using similar foods. Analysis of additional Awajún foods would be beneficial to fully understand the nutritional potential of the food system. The number of feeding episodes per day (in addition to breast milk) was calculated based on the average of the two recall days for each child. The mean energy and nutrient densities of the complementary foods were calculated using the available food composition data and estimated grams consumed based on the average of the two dietary recall days. Energy density (kcal g−1) and nutrient densities (amount of nutrient per 100 kcal) were compared with the recommendations for complementary foods considering average breast milk intake (Brown et al. 1998; Dewey & Brown 2003). The mean number of feeding episodes for Awajún infants was compared with age‐appropriate recommendations based on mean energy density established from the dietary recalls (Dewey & Brown 2003). Total energy and nutrient intakes were compared with recommended intakes of Food and Agriculture Organization/WHO (FAO/WHO 2002) and Dewey & Brown (2003).
Infant food history
To gain an understanding of infant feeding practices, we included questions on the following: initiation of breastfeeding, exclusive breastfeeding, use of other non‐human milks, introduction of complementary foods and continued breastfeeding. Each mother was asked to respond to these questions in an infant food history questionnaire in addition to the dietary 24‐hour recalls. Focus groups and key informant interviews were conducted with young women as well as elders from the six communities to define which key foods should be included in the infant food history. Those selected were cassava (Manihot esculenta), suri (a larva of the order Coleopterus found in decomposing palm trunks), banana, eep (green leafy vegetables), fish, squash, egg, fruit, chicken, animal organs, fried food, aguaje (Mauritian palm fruit; Mauritia flexuosa), chapo (banana and water combination) and palm heart. During the focus groups and key informant interviews, the preparation methods for infant and young child complementary foods were described. Mothers were asked at what age they introduced the food, or if the child had not yet been given the food, at what age the mother planned to introduce the food, as well as the intended frequency.
Ethics
This study followed the principles of participatory health research of the planning and management framework specific to Indigenous Peoples (Sims & Kuhnlein 2003). Informed consent was obtained on three levels; (1) an umbrella written research agreement with the Organización de Desarrollo de las Comunidades Fronterizas del Cenepa (ODECOFROC); (2) informed written consent and research agreement with the four communities and two annexes; and (3) individual oral parental consent with a community witness and interpreter for all subjects. Ethics approval was given by the Faculty of Agricultural and Environmental Sciences Committee on Human Research Ethics Review Board at McGill University and the Ethics Committee of the IIN in Lima, Peru.
Results
Food in a typical day in the life of a young Awajún child
For a child of 1 year of age, he or she would wake up early in the morning with her mother at around 5 a.m. and breastfeed. She would spend the morning in the kitchen with her siblings as mom starts the three‐log wood fire. Mom would give her a small pinig of masato (premasticated cassava beverage). About an hour later, mom would give her a piece of boiled cassava. Once the fire had cooled, her mom would roast peeled bananas directly on the coals. She would eat the banana and then be wrapped in the shawl on her mother's back to begin the 1.5‐hour journey to the family chacra (gardening plot). She would spend most of her day in the chacra with her mother, who would give her a raw banana, a suri (larvae) picked from a rotting palm tree, seasonal fruits such as papaya and orange. She would also breastfeed on demand throughout the day. She and her mother would return home at the end of the day so mom could prepare a dinner with boiled cassava as well as a patarashka, which is made by wrapping ingredients in banana leaves such as leafy greens, mushrooms and small fish from the stream. The child would be given a small portion of the meal as well as warm chapo (banana and water thick beverage). After dinner, the child would be breastfed before going to sleep.
Anthropometry of infants
A total of 32 infants and young children under 2 years of age were included in the study. The mean anthropometric Z‐scores per age group are shown in Fig. 1. For infants and young children, the HAZ ranged from −4.34 to 1.65, with mean ± standard deviation HAZ at −1.71 ± 1.41 for all infants and young children. Overall, 39.4% of the infants and young children were stunted (HAZ < −2). Stunting increased with age; the one‐way ANOVA, comparing the mean HAZ for infants and young children, showed a significant difference among the three age groups (F = 8.46, P = 0.001) and the HAZ was significantly negatively correlated with age in months (r = −0.62 P < 0.001) (Table 1). The mean weight‐for‐age Z‐score (WAZ) was −0.57 ± 1.46 for infants and young children 0–23 months of age. The prevalence of underweight was lower than stunting; 12.5% of the children were underweight (WAZ < −2). WAZ was also significantly negatively correlated with age in months (r = −0.50, P = 0.003). There was a slight difference in the age groups (F = 3.23, P = 0.05). The mean weight‐for‐height Z‐score (WHZ) was 0.50 ± 1.49 for all children. Differences of WHZ by age were not detected with this limited small sample size (r = −0.32 P = 0.08) (Fig. 1). Given the small sample size, it is also possible that other real differences were missed.
Figure 1.
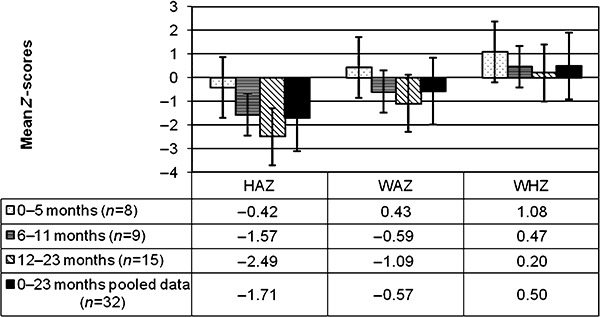
Anthropometry of Awajún children 0–23 months of age as measured by height‐for‐age Z‐score (HAZ*), weight‐for‐age Z‐score (WAZ*) and weight‐for‐height Z‐score (WHZ*) (n = 32) *New World Health Organization growth standards were used to calculate anthropometry (WHO 2006).
Table 1.
Age of introduction or intention to introduce complementary foods and frequency of consumption (n = 20–31)
| Food | n | Age range of introduction (months) | Mean age ± standard deviation food introduced (months) | Frequency of consumption (no. of infants fed food) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Daily | 1/week | 1/month | 1/season (3 months) | 1/year | Not sure | ||||
| Cassava | 30 | 3–12 | 6.5 ± 2.3 | 24 | 6 | – | – | – | – |
| Suri | 29 | 3–24 | 12.1 ± 6.3 | – | 3 | 17 | 3 | – | 6 |
| Banana | 31 | 2–24 | 8.4 ± 5.8 | 16 | 12 | 3 | – | – | – |
| Fish | 29 | 4–24 | 8.3 ± 4.3 | 1 | 15 | 10 | 1 | – | 2 |
| Eep (leafy greens) | 29 | 5–24 | 11.9 ± 5.3 | 2 | 14 | 7 | 1 | – | 5 |
| Squash | 20 | 6–48 | 14.6 ± 10.3 | 6 | 4 | 6 | 1 | – | 3 |
| Egg | 29 | 3–24 | 8.2 ± 4.4 | 3 | 15 | 8 | 1 | – | 2 |
| Seasonal fruits | 30 | 4–12 | 9.3 ± 2.8 | 14 | 6 | 5 | – | – | 5 |
| Chicken | 30 | 4–24 | 9.3 ± 3.9 | – | 5 | 20 | 1 | – | 4 |
| Pork | 28 | 5–36 | 16.5 ± 9.3 | 4 | 3 | 11 | 2 | – | 8 |
| Liver or organs | 30 | 2–24 | 9.9 ± 6.1 | – | 5 | 19 | 1 | – | 5 |
| Fried food item | 20 | 4–24 | 13.8 ± 6.4 | – | 4 | 8 | 2 | – | 6 |
| Aguaje (Mauritian palm fruit) | 30 | 4–24 | 11.0 ± 5.4 | 13 | 7 | 3 | 1 | – | 6 |
| Palm heart | 30 | 3–24 | 8.4 ± 4.5 | 1 | 13 | 10 | 1 | – | 5 |
| Chapo (banana and water thick beverage) | 29 | 2–12 | 6.7 ± 2.9 | 18 | 6 | 2 | – | – | 3 |
Dietary intakes
Early initiation and exclusive breastfeeding
According to the infant food history questionnaire, all Awajún mothers breastfed their infants and children and almost three quarters of mothers reported giving colostrum to their infant (74%). However, from the infant food histories as well as the dietary recalls, it was evident that exclusive breastfeeding to 6 months was not always practised. Among the Awajún mothers, 52% reported exclusive breastfeeding for 6 months, or intention to do so (two mothers with infants <6 months) in the infant food history questionnaire. Exclusive breastfeeding was not the practice or intended practice for 48% of the women who had already introduced foods or were planning to introduce foods before their infant was 6 months of age (two mothers with infants <6 months). Results from the infant food history questionnaire reported complementary foods such as banana and chapo were introduced as early as 2 months. Repeat dietary recall analyses found that five of the eight infants (63%) less than 6 months of age were exclusively breastfeeding at the time of the interview. Two of the infants under 6 months of age who received complementary foods, received only breast milk on one day of the recall and breast milk plus additional foods on the other dietary recall. There were two infants 8 months of age that received only breast milk. There was also one infant of 8 months of age who received complementary foods on one of the recall days and only breast milk on the other. One infant 9 months of age consumed breast milk only for both days of the dietary recall.
Continued breastfeeding
Only 12.6% of mothers had stopped or had intentions of stopping breastfeeding before 1 year of age; 51.6% had breastfed or intended to continue breastfeeding beyond 1 year of age, while 22.6% said they had or would breastfeed until the child reached 2 years of age. There were 6.5% and 3.2% of mothers who reported intentions to breastfeed their children to 3 and 4 years of age, respectively.
Non‐human milk consumption
Canned evaporated milk was being given to 39% of the infants from 3 to 23 months of age. Infants that received this non‐human milk began receiving it between the age of 3 and 21 months of age, with 25% of those who received the milk starting before 6 months of age. On average, infants started consuming the evaporated milk at 8 months. Canned evaporated milk was donated to families through the government ‘Glass of Milk’ program and was intended for infants and children >6 months.
Complementary foods
According to the infant feeding history questionnaire, the first foods most commonly introduced were cassava and chapo (Table 1). The complementary foods generally introduced next would be banana, palm heart, fish and egg. However, there was a wide range in the age of introducing each complementary food (Table 1). In terms of frequency of consumption, cassava, banana, chapo, aguaje and seasonal fruits were most commonly given to infants daily. Animal source foods including fish and egg were most commonly given once a week or less frequently. Leafy greens (eep) were generally given once a week. Complementary foods given less frequently included chicken, pork, liver or other organs, suri (larvae), and squash (Table 1).
Feeding episodes and frequency
A feeding episode was defined as an instance when the infant or child was fed food other than breast milk or alternative milks. Culturally, there was no differentiation between a snack and a meal. The three children under 6 months of age who received food were fed once a day in addition to breast milk. Infants 6–8 months of age (n = 4) had an average of 1.3 ± 1.9 feeding episodes per day. For infants 9–11 months of age (n = 4), the average number of feeding episodes per day was 1.9 ± 1.6. For children 12–23 (n = 15) months of age, the average number of feeding episodes per day was 7.4 ± 2.1.
Energy and nutrient intakes
Energy intake from complementary foods
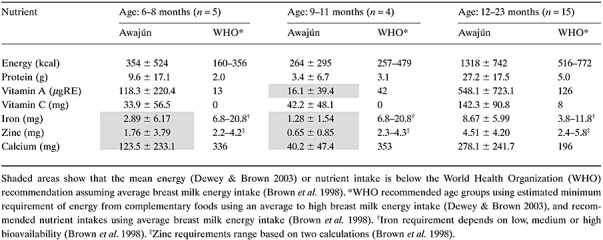
Infants 6–8 months of age and 9–11 months of age met the recommended daily intakes for energy. Mean total energy intake was above the recommendation for 6–8‐month‐olds and just below for infants 9–11 months of age (Table 2). The infants from 12–23 months, on average, consumed appropriate amounts of energy.
Table 2.
Estimated energy and nutrient intake from complementary foods for Awajún infants and young children in comparison with WHO recommendations (n = 24) (mean ± standard deviation)
Energy density of complementary foods
The mean energy density of complementary foods was 1.1 ± 0.2 kcal g−1 for infants 6–8 months of age (n = 3), 1.4 ± 0.3 kcal g−1 for infants 9–11 months of age (n = 3) and 1.3 ± 0.5 kcal/g for children 12–23 months of age (n = 15). These energy densities met the recommended values for each age group considering average breast milk intake and mean number of complementary feeding episodes reported, with the exception of the youngest age group (Dewey & Brown 2003). In this case, the energy density corresponds to between one and two feeding episodes (actual mean is 1.3 times) and would readily meet the recommendations if there were a ‘high’ breast milk intake.
Nutrient intake from complementary foods
Mean intakes by infants 6–11 months of age met recommended intakes of complementary foods for protein and vitamin C, and for vitamin A only for the infants 6–8 months (Table 2) (Brown et al. 1998). Mean intakes for infants 6–8 months did not meet the recommended intakes for iron, zinc, and calcium. For the 9–11 months age group, they were also below the recommended intakes for iron, zinc and calcium as well as vitamin A. Mean intakes by infants 12–23 months of age met recommended intakes for protein, vitamin A, vitamin C, zinc, iron and calcium (Table 3) (Brown et al. 1998).
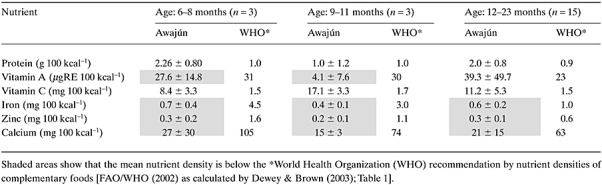
Table 3.
Estimated nutrient densities from complementary foods for Awajún infants and young children in comparison with WHO recommendation (n = 24) (mean ± standard deviation)
Nutrient density of complementary foods
Mean nutrient densities for complementary foods consumed by infants from 6–11 months of age met recommended densities for protein and vitamin C (Table 3). However, lower nutrient density than desired was found for vitamin A, calcium, iron and zinc. Mean nutrient densities consumed by children 12–23 months were above the recommended densities for protein, vitamin A and vitamin C, while the densities for iron, zinc and calcium were below recommendations (Table 3).
Traditional food in comparison with market food
Table 4 shows the relative energy and nutrient contributions of traditional food and market food to the diet of infants and young children in this Awajún population. The contribution of breast milk is not included in the traditional foods here, and commercial milks are excluded from the market foods. For infants and young children 6–23 months of age, traditional food provided most of the complementary food energy (86.9%) and proportionally more protein, vitamin A, vitamin C, zinc and calcium than the market foods.
Table 4.
Relative % energy and nutrient contributions of traditional foods and market foods for Awajún infants and young children aged 0–23 months (breast milk and breast milk substitutes excluded) (n = 24)
| Energy (%) | Protein (%) | Vitamin A (%) | Vitamin C (%) | Iron (%) | Zinc (%) | Calcium (%) | |
|---|---|---|---|---|---|---|---|
| Traditional food | 86.9 | 99.2 | 99.9 | 99.7 | 86.2 | 89.8 | 92.0 |
| Market food | 13.1 | 0.8 | 0.1 | 0.3 | 13.8 | 11.2 | 8.0 |
Discussion
For almost 30 years, there has been little mention of the Awajún in the nutrition literature; to the best of our knowledge, this is the first study to describe the infant and young child feeding practices of the Awajún (Berlin & Markell 1977; Huamán‐Espino & Valladares 2006). Breastfeeding and appropriate complementary feeding are essential to ensure healthy growth of infants and young children (Léon‐Carva et al. 2002). Although this study is limited to a small non‐random sample of women and children and caution must be taken in interpreting the results; we found considerable variation in infant feeding practices among Awajún women despite very similar subsistence lifestyle. Appropriate practices and key nutrient‐dense local foods need to be highlighted and promoted in the Cenepa region to maximize the potential growth and development of all Awajún children.
Although the sample sizes for this study were small, analysis of the nutritional status of children would suggest that the Awajún in the Cenepa area are generally born at a healthy size in terms of length for age. The nutritional status continually declines starting from the first few months of life. This pattern is consistent with the progression of malnutrition seen throughout Latin America (Shrimpton et al. 2001).
Stunting is a result of an inadequate diet and/or repeat infections. Although this study cannot suggest a direct cause for the decline in nutritional status with age, exclusive breastfeeding for the first 6 months of life would offer a child both nutritional adequacy and protection against infections (Léon‐Carva et al. 2002). As only 52% of the mothers exclusively breastfed, the promotion of exclusive breastfeeding may be an opportunity to improve the health and growth of the Awajún children. As there were many women in the community who gave colostrum, exclusively breastfed for the first 6 months of life and continued breastfeeding for 2 years, these positive practices are culturally acceptable to the Awajún. A few children were given nutrient‐dense local foods including animal products, starting at 6 months of age; most were given mainly staple foods such as banana as young as 2 months, while others were not given animal products such as chicken meat or organs until almost 2 years of age. Earlier research also suggested that animal source foods were consumed infrequently at the household level (Huamán‐Espino & Valladares 2006). Nutrition interventions are most effective when targeted at children early in the first 2 years of life and specifically from the first few months to prevent the observed growth faltering that starts before 6 months of age and continues to 2 years of age (Martorell et al. 1994; Shrimpton et al. 2001). Community‐level growth‐monitoring and promotion programs were not in place, yet it could help the Awajún mothers recognize early growth faltering and offer targeted nutrition counselling.
The infant feeding histories showed 52% mothers exclusively breastfed, while the dietary recalls gave a higher prevalence of 63%, indicating that foods and liquids other than breast milk may not be given every day. Exclusive breastfeeding until 6 months and continued breastfeeding until 2 years need to be addressed. The late introduction of foods to complement breast milk for infants from 6 months is of concern. In the age group 6–11 months, some infants were given complementary foods only on some days. This feeding practice was only captured by doing repeat 24‐hour recalls and would have been missed by the infant food history. The infant food history provided useful information into the age range at which complementary foods were introduced. Nutrient‐dense foods including eggs, suri, chicken and leafy greens should be promoted for children 6–12 months of age as these were generally introduced very late.
Young children 12–23 months of age seemed to be meeting the recommended needs and nutrient densities for complementary foods better than the younger age groups (6–11 months) as they are given more and a wider variety of foods. Although the appropriate nutrient densities were lower than desired for iron, zinc and calcium, the Awajún may have compensated for this with energy intakes above the recommended values in this older age group, thus having mean adequate total intakes for these nutrients (Table 3). This study was limited to the lean (rains and scarce fishing) season, and improved nutrient densities might be expected from the 24‐hour recalls in other months, whereas the infant food histories included foods available in all seasons. Animal source foods are especially known to be important in childhood nutrition (Kuhnlein & Receveur 2007) as they are rich, bioavailable sources of several nutrients. The Awajún traditional food system offers nutrient‐dense complementary foods that can be promoted; for example, suri is a source of animal protein, iron and zinc (Roche et al. 2007b), fish and eggs are also available and acceptable foods for infants and young children and aguaje (M. flexuosa) is rich in vitamin A. Both the suri and aguaje were available during the lean season.
The energy densities of the diets were similar for all age groups; however, mothers fed children 12–23 months of age much more frequently than the younger children. Although breast milk consumption was not quantified in this study, infant food histories, dietary recalls, focus groups and observation suggested the Awajún infants received a high amount of energy from breast milk. Targeted interventions to improve frequency and nutrient density of feeding starting at 6 months of age would be appropriate. Interventions in rural Bangladesh have shown positive results in increasing frequency of feeding and density of complementary foods in infants and young children (Kimmons et al. 2004). As Awajún infants and young children spend most of the day with their mothers either around the house or in the chacra (family plot for cultivation up to 2 hours canoe ride and walk away from the house), feeding frequency will depend on having easily accessible foods in the chacra in addition to foods that could be prepared at home.
Promoting the benefits of breastfeeding and nutrient‐dense local complementary foods will be important, as availability and access to market foods including commercial milks increase for the Awajún. In 2004, less than 1% of the foods the Awajún consumed were purchased or donated by the government. Children 3–5 years of age had a diet consisting of 18% of energy from donated food, and mothers' diets were 6.5% donated food (Roche et al. 2007a); yet in the analyses here, 39% of the infants were consuming donated canned evaporated milk. If the government provides donated foods, a nutrient‐dense fortified complementary food with explicit written labelling in Awajún and Spanish might be more appropriate and beneficial. As the communities of the Rio Cenepa have river access only, market foods arrive by merchant boats that travel up the river from community to community. Many market foods, including evaporated milk, arrive in colourful packaging and often include posters or advertising for the shops selling these items (M. Roche, unpublished observations). Should milk substitutes be marketed in these communities without promotion of breastfeeding as a best practice, there could be negative health, economic and environmental consequences for the Awajún. Community‐level or government legislation could protect the Awajún from influential or potentially misleading marketing of unhealthy foods. Awajún elders also feared that further decline in traditional food consumption could result from decrease in access to land for traditional hunting, fishing and cultivation.
Given the chronic malnutrition and growth retardation occurring in the infants and children during the first 2 years of life observed in this small sample of Awajún children and reported by others (Huamán‐Espino & Valladares 2006), there is a need for targeted nutrition interventions to improve infant and young child feeding. There is considerable variation in infant feeding practices among Awajún women, and more attention should be given to promote and strengthen appropriate practices. In addition to the promotion of optimum breastfeeding practices, there is a need to highlight the use of key nutrient‐dense traditional complementary foods for infants beginning at 6 months of age, and finding ways to make these acceptable. After these results were shared with the participating communities, nutrition promotion and food security small‐scale interventions were initiated to improve nutrition for Awajún children in the Cenepa area.
Health promotion of traditional foods for Indigenous Peoples goes beyond the knowledge, attitudes and practice framework; it must also include advocacy for the protection of the rights of Indigenous Peoples to the land that offers them a healthy diet, and informed decisions in the market foods introduced.
Source of funding
We recognize the funding contribution of the Canadian Institutes for Health Research, Institute of Aboriginal Peoples Health and Institute of Population and Public Health.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Acknowledgements
We sincerely thank Sandra Vidal, Melissa Abad and Miluska Carrasco for their work in data collection. We also thank Alvaro, Ruben and Francisco (Pancho) Kantuash Saan for their efforts in translation. ODECOFROC and the dedicated women's group were essential throughout the research, for which we are grateful. We would like to thank Margot Marin of the IIN for her assistance in data management. We extend our appreciation to the Awajún communities of lower Cenepa, especially the women and children who participated in this study.
References
- Basiotis P.B., Welsh S.O., Cronin F.J., Kelsay J.L. & Mertz W. (1987) Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. Journal of Nutrition 117, 1638–1641. [DOI] [PubMed] [Google Scholar]
- Berlin E.A. & Markell E.K. (1977) An assessment of the nutritional and health status of an Aguaruna Jívaro community, Amazonas, Peru. Ecology of Food and Nutrition 6, 69–81. [Google Scholar]
- Brown K.H., Dewey K.G. & Allen L.H. (1998) Complementary Feeding of Young Children in Developing Countries: A Review of Current Scientific Knowledge. World Health Organization: Geneva. [Google Scholar]
- Dewey K.G. & Adu‐Afarwuah S. (2008) Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Maternal and Child Nutrition 4, 24–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dewey K.G. & Brown K.H. (2003) Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food and Nutrition Bulletin 24, 15–28. [DOI] [PubMed] [Google Scholar]
- FAO/WHO (Food and Agriculture Organization/World Health Organization) (2002) Human Vitamin and Mineral Requirements: Report of a Joint FAO/WHO Expert Consultation Bangkok, Thailand. Food and Nutrition Division, FAO: Rome. [Google Scholar]
- Huamán‐Espino L. & Valladares C. (2006) Estado Nutricional y Características del Consumo Alimentario de la Población Aguaruna. Revista Peruana de Medicina Experimental y Salud Publica 23, 12–21. [Google Scholar]
- IIN (Instituto de Investigación Nutricional) (2004) Tabla de Composición de Alimentos. IIN: Lima. [Google Scholar]
- Kimmons J.E., Dewey K.G., Haque E., Chakraborty J., Osendarp S.J.M. & Brown K.H. (2004) Behavior‐change trials to assess the feasibility of improving complementary feeding practices and micronutrient intake of infants in rural Bangladesh. Food and Nutrition Bulletin 25, 228–238. [DOI] [PubMed] [Google Scholar]
- Kuhnlein H.V. & Receveur O. (1996) Dietary change and traditional food systems of Indigenous Peoples. Annual Review of Nutrition 16, 417–442. [DOI] [PubMed] [Google Scholar]
- Kuhnlein H.V. & Receveur O. (2007) Local cultural animal food contributes high levels of nutrients for Arctic Canadian indigenous adults and children. Journal of Nutrition 137, 1110–1114. [DOI] [PubMed] [Google Scholar]
- Léon‐Carva N., Lutter C., Ross J. & Martin L. (2002) Quantifying the Benefits of Breastfeeding: A Summary of the Evidence. PAHO (Pan American Health Organization): Washington, DC. [Google Scholar]
- Martorell R., Kettel Khan L. & Schroeder D.G. (1994) Reversibility of stunting: epidemiological findings in children from developing countries. European Journal of Clinical Nutrition 48, S45–S57. [PubMed] [Google Scholar]
- PAHO/WHO (Pan American Health Organization/World Health Organization) (2004) Guiding Principles for Complementary Feeding of the Breastfed Child. Division of Health Promotion and Protection, PAHO/WHO: Washington, DC. [Google Scholar]
- Roche M.L., Creed‐Kanashiro H.M., Tuesta I. & Kuhnlein H.V. (2007a) Traditional food system provides dietary quality for the Awajún in the Peruvian Amazon. Ecology of Food and Nutrition 46, 377–399. [DOI] [PubMed] [Google Scholar]
- Roche M.L., Creed‐Kanashiro H.M., Tuesta I. & Kuhnlein H.V. (2007b) Traditional food diversity predicts dietary quality for the Awajún in the Peruvian Amazon. Public Health Nutrition 11, 457–465. [DOI] [PubMed] [Google Scholar]
- Shrimpton R., Victora C.G., de Onis M., Costa Lima R., Blössner M. & Clugston G. (2001) Worldwide timing of growth faltering: implications for nutritional interventions. Pediatrics 107, e75. [DOI] [PubMed] [Google Scholar]
- SICNA (Sistema de Información sobre Comunidades Nativas Tituladas del Perú) (1999) Datos de Población de la Cuenca del Cenepa Provincia Condorcanqui. Departamento Amazonas. Instituto del Bien Común: Lima. [Google Scholar]
- Sims J. & Kuhnlein H.V. (2003) Indigenous Peoples & Participatory Health Research. Planning and Management. Preparing Research Agreements. World Health Organization: Geneva. [Google Scholar]
- SPSS (2006) SPSS for Windows Version 15.0. SPSS, Inc.: Chicago. [Google Scholar]
- USDA (United States Department of Agriculture) (2004) Agricultural Research Service Nutrient Data Laboratory Home Page. Available at: http://www.nal.usda.gov/fnic/foodcomp/search/ (accessed October 2005).
- WHO (World Health Organization) (1995) Physical Status: The Use and Interpretation of Anthropometry. World Health Organization: Geneva. [PubMed] [Google Scholar]
- WHO (World Health Organization) (2006) WHO Anthro 2005, Beta Version Feb 17th, 2006: Software for Assessing Growth and Development of the World's Children. World Health Organization: Geneva. [Google Scholar]
- World Bank (2006) Repositioning Nutrition as Central to Development: A Strategy for Large‐Scale Action. The World Bank: Washington, DC. [Google Scholar]