

Abstract
Australia has high initiation rates of breastfeeding, but the challenges of establishing and maintaining breastfeeding in the first few months of infant life result in many women changing to artificial formula feeding. This paper reports on the impact of a new strategy to improve breastfeeding duration rates in the first 8 weeks post‐partum. The Earlybird Program (EBP) combines the professional expertise of child and family health (C&FH) nurses with the expertise of the participating mothers to support each other in establishing breastfeeding in the first 8 weeks. This retrospective study compared the breastfeeding patterns of first‐time mothers who attended the EBP, with the breastfeeding patterns of mothers who accessed individual appointments with the nurses in a 12‐month period, and examined the predictors of continued breastfeeding at 8 weeks. The total sample comprised 193 infant records. Women who selected the EBP were more likely to be employed and less likely to be categorized as non‐English speaking background. These women also had more visits to the C&FH service. Logistic regression was used to determine the factors associated with breastfeeding cessation at 8 weeks post‐natal. After adjusting for variables, only exclusive breastfeeding at first visit and attending the EBP were significant predictors of continuing to breastfeed at 8 weeks. Facilitation skills that recognize the expertise of participating women were considered an important aspect of the programme.
Keywords: breastfeeding, child and family health nurses, parent groups, facilitation
Introduction
Breastfeeding is considered the optimum method of infant feeding for the first 6 months of life, conferring significant health benefits to both the mother and the baby. The Australian government recommends exclusive breastfeeding to 6 months of age (NHMRC 2003). Australian studies demonstrate that between 80% and 90% of women will initiate breastfeeding, yet there continues to be a rapid decline in breastfeeding rates during the first 6 to 8 weeks following birth (Lowe 1993; Scott et al. 1999; Donath & Amir 2000), and breastfeeding rates at 3 and 6 months are well below the government targets set for the year 2000 and beyond (Nutbeam et al. 1993). Furthermore, recent Australian and international research has demonstrated that there are increasing levels of distress among women related to breastfeeding in the early post‐birth period (Hoddinott & Pill 1999; Murphy 1999; Schmied & Lupton 2001; Nystrom & Ohrling 2004).
Internationally, government and institutional policies have been implemented to increase initiation and duration of breastfeeding. Australia, for example, is a signatory to the World Health Organization (WHO) code on the marketing of breastmilk substitutes. National and state policies support the implementation of the WHO and UNICEF Baby Friendly Hospital Initiative, focusing on the promotion and support of breastfeeding. In the later 1990s, the Australian government allocated 2 million dollars to a National Breastfeeding Strategy that aimed to raise community awareness and increase professional knowledge and skills to support breastfeeding.
A Cochrane systematic review by Sikorski and colleagues in 2001, and updated in 2003, examined the effect of enhanced breastfeeding support. The review incorporated 13 randomized control trials across seven countries, and found that professional support provided to women in the early post‐natal period has a positive effect on breastfeeding duration to 8 weeks (Sikorski et al. 2003).
Furthermore, a systematic review and meta‐analysis conducted by Guise et al. (2003) for the US Preventative Services Task Force found that both education and support interventions provided post‐natally increased breastfeeding duration up to 6 months of age. Educational interventions providing structured content around the benefits of breastfeeding appeared to have the greatest single effect when compared with interventions increasing support to mothers.
In populations where breastfeeding initiation is high, it may be that supportive interventions have a greater effect on increasing breastfeeding duration. In their recent review, Sikorski et al. (2003) suggest that there is a limited understanding of the elements of successful support in breastfeeding interventions.
Peer support groups, such as La Leche League (LLL), National Childbirth Trust and Australian Breastfeeding Association (ABA), have been providing support for breastfeeding women since the late 1950s and early 1960s. Research demonstrates that peer support can be effective and important in sustaining breastfeeding (Kisten et al. 1994; Locklin 1995; Shaw & Kaczorowski 1999; Dykes 2003). Generally, this support involves the training of peers (mothers who have breastfed), either to provide one‐to‐one peer counselling or to facilitate group support, in a similar tradition to LLL and ABA (Dykes 2003). This form of peer support usually occurs face to face, but has been demonstrated to be effective through telephone counselling (Dennis et al. 2002).
In this paper, we describe an approach that professionals [child and family health (C&FH) nurses] facilitate peer support in the first 8 weeks post‐partum in order to increase women’s confidence in parenting, to increase breastfeeding duration rates and to support mother–infant attachment. The model of peer support recognizes the existing (without additional education or training) knowledge and experience of the participants, their capacity to learn from and support each other, and the importance of building self‐confidence in decision making.
The paper presents the findings of a retrospective study comparing the breastfeeding patterns of first‐time mothers who attended this support group, known as the ‘Earlybird Program’ (EBP), with the breastfeeding patterns of mothers who accessed individual appointments with the nurses at the study site in a 12‐month period. It examines the predictors of continued breastfeeding at 8 weeks post‐natal.
The child and family health service
In Australia, C&FH nurses 1 are, together with general practitioners (known in some countries as family physicians), the primary group of health professionals who provide care for mothers and infants after their discharge from maternity services. Similar to the health visitor in the United Kingdom, these nurses provide a universal and preventative service to families with children under the age of 5 years. Families attend more frequently in the first few months of an infant’s life, although health and development screenings are offered at 1–4 weeks, 6–8 weeks, 6–8 months, 18 months, 2.5–3.5 years and 4–5 years as per national guidelines (NSW Health 2003). C&FH nurses also provide proactive and opportunistic health‐promotional information to parents on the day‐to‐day caring and rearing of their children (Long 2001). In this role, these nurses are uniquely positioned to link families to each other, as well as to other community resources and services.
Child and family health nurses are prepared through specialty postgraduate education programmes that include breastfeeding. Most are also midwives although current workforce shortages are resulting in non‐midwives working in this specialist field. Many have additional qualifications in breastfeeding by achieving International Board of Lactation Consultants certification, although this is not a prerequisite to employment.
Women in Australia can access the C&FH service through individual (‘one‐to‐one’) contact with a C&FH nurse either through an appointment system or on a ‘drop in’ basis. Contact with the same nurse (continuity) is varying across the country. The C&FH centre in which this study was undertaken supported three nursing positions and attempted to offer continuity of care to women where possible.
For many years, C&FH nurses have used groups to convey information to parents, particularly on issues such as infant feeding and related problems (Scott et al. 2001a). Traditionally, new mothers’ groups are ‘closed’ to a predetermined number of participants, and run as a short‐term ‘course’ of around 6 weeks, for 2–3 hours each session. Generally, babies are 8 weeks or older before the mother is provided with an opportunity to attend a group (Clarke et al. 1995; Freeman & Lamb 1997; Clune 1999). Specific, predetermined topics on common parenting issues are covered each week, often with guest speakers who have known professional authority in the field. The role of the nurse is central, and she/he is seen as the leader or expert in the group.
The increasing tendency to adopt more client‐directed groups in which the participants set the agenda and determine their own goals and resources provides a contrast in approach to service delivery. In these client‐led groups, the health professional remains a member of the group and is respected by the group for the contribution she/he makes as a nurse, midwife and educator (Rodwell 1996). The facilitator encourages the women to identify their own needs and set their own agenda. By doing this, the nurse promotes empowerment of the group, which can result in enhanced self‐esteem, the ability to set and reach goals, and a sense of control over one’s life (Rodwell 1996).
The Earlybird Program
The EBP was introduced by C&FH nurses as a pilot site in one sector of an area health service in metropolitan Sydney. The programme aims to increase the confidence of new mothers, to improve breastfeeding duration, to heighten maternal–infant attachment, and to promote mother‐to‐mother support (SESIAHS 2005). The programme was adapted from the UK‐based ‘Deptford model’ (Leap 1993; Leap 2000) to provide professional support and to facilitate peer support for families as soon as possible after birth. Birthing details of women within the catchment area are sent to the C&FH service in the form of a discharge summary. The C&FH nurse will telephone all women within several days of discharge, outline the range of services offered, and invite the woman and her baby to either a one‐to‐one appointment or an Earlybird group.
Earlybird Programs are ‘open’ 2 and run on a continual basis for parents with babies up to 8 weeks of age. The restricted time frame is in recognition that the first 8 weeks are crucial in establishing breastfeeding and confidence in parenting. It also ensures that all participants are at a similar stage of parenting. Once their infants are 8 weeks old, parents have the opportunity to attend groups catering for infants aged 2–6 months. While first‐time parents are in the majority, women with more than one child are welcome and provide wisdom and support from their own parenting experiences. Partners, relatives and friends are also invited, with fathers and grandmothers commonly participating. Women with mental health disorders, including post‐natal depression, are not excluded from the groups.
The EBP facilitator and co‐facilitator provide information and other central services through the group that would usually be carried out on a one‐to‐one basis in the health centre setting. Child health checks and development assessments and baby weighs are available at the beginning and end of each session. While there is no set agenda, mothers in the group typically raise issues that would be provided in traditional C&FH nursing interactions. These include immunization, mother–infant attachment, age‐appropriate behaviours, contraception, sudden infant death syndrome and post‐natal depression. The nurses supplement discussions with current evidence‐based information.
Time is made available at the end of each session for individual attention to clients’ needs and referral for additional appointments if required. Documentation of attendance and any relevant information is recorded in each client’s file. The co‐facilitator keeps a record of the discussion and individual client issues throughout the session.
Although experienced at running groups, all facilitators received education in adult education, group process and the model of open groups, and skills in working in partnership prior to facilitating EBP groups. This is in recognition of the different skills required when facilitating groups within a partnership model that places equal value on the expertise and contribution of the women and their support people (SESIAHS 2005). Each nurse is also accredited in conducting open groups by the area health service. Two facilitators are present for each EBP group and allocate time at the end of each session to debrief with each other and discuss individual women who may require additional support or follow‐up.
Two years following the implementation of the EBP, an evaluation was undertaken. The findings reporting women’s experiences with the group are published elsewhere (Kruske et al. 2004). In order to determine the impact of the EBP on breastfeeding duration, a retrospective audit of central records of all firstborn infants in a 12‐month period held in one child health centre was undertaken.
Materials and methods
This was a retrospective study that compared the breastfeeding patterns of first‐time mothers who attended the EBP at the study site in a 12‐month period, with the breastfeeding patterns of mothers who only accessed individual appointments with the C&FH nurses. Ethics approval for this study was obtained from the Area Health Human Research Ethics Committee.
Setting
The study site was a C&FH centre in metropolitan Sydney. The C&FH centre services part of the local council municipality. Thirty per cent of the council population was born overseas, with China being the largest country of birth for migrants (SES Council 2003). Thirty‐five per cent of the population speaks a language other than English in the home. After English, the most common languages spoken at home include Greek, Mandarin, Cantonese, Arabic, Italian and Macedonian. The area has a slightly lower proportion of low‐income households than Sydney as a whole.
Sample
The centre records of all infants born during a 12‐month period to first‐time mothers seen by C&FH nursing services formed the study sample. These families accessed the service by individual consultations or through the EBP. The sample comprised 224 records.
Data collection and analysis
A total of 224 C&FH centre records were audited by the first author. A data collection tool was developed for the purposes of the study and recorded the following variables: age of mother, country of birth, employment, age of baby at first visit, method of feeding at first visit and at 8 weeks, number of visits to the service, number of one‐to‐one consultations, and number of visits to the EBP and referral to other services. Complete data were obtained for 193 records. There was no apparent difference between the women’s characteristics for the 193 records included in the analysis and the 31 records that were incomplete.
Data were entered in spss and analysed using descriptive statistics and logistic regression. Differences between the women who selected the EBP and those who did not were examined using chi‐square for categorical variables and Student’s t‐test for non‐categorical variables. A logistic regression was used to determine the predictors of breastfeeding cessation at 8 weeks post‐natal. Maternal employment, maternal age, non‐English speaking background, exclusive breastfeeding at first visit, age of first visit and number of visits to the C&FH service, and EBP attendance were entered into the model alone and then adjusted for all other variables. The relative risk of continuing to breastfeed at 8 weeks when women attended the EBP was also calculated.
Results
The total sample comprised 193 C&FH records. The demographic characteristics of the sample are presented in Table 1. The mean age of mothers was 30 years (range 17–43). Sixty‐six per cent of the sample was recorded as being employed prior to the birth of their baby. Forty‐five per cent were from non‐English speaking backgrounds. Twenty‐seven women (14%) were discharged from hospital early and supported by the midwifery support domiciliary programme.
Table 1.
Sample characteristics
| Variable | Total sampleN = 193 | Total sample (excluding records = not breastfeeding at first visit to C&FH nurse) N = 170 | ||||||
|---|---|---|---|---|---|---|---|---|
| EarlybirdN = 106 (72%) | Centre Only N = 64 (38%) | |||||||
| Frequency | % | Frequency | % | Frequency | % | Test statistic | P‐value | |
| Employed | 128 | 66 | 80 | 75 | 36 | 56 | χ2(df1) 6.80 | 0.009 |
| NESB | 87 | 45 | 40 | 38 | 38 | 59 | χ2(df1) 7.52 | 0.006 |
| Infant feeding at first visit to C&FH nurse | ||||||||
| Not breastfeeding | 23 | 12 | – | – | – | – | ||
| Partially breastfeeding | 25 | 13 | 12 | 11 | 13 | 20 | χ2(df1) 2.57 | 0.109 |
| Exclusively breastfeeding | 145 | 75 | 94 | 89 | 51 | 80 | ||
| Infant feeding at 8 weeks | χ2(df1) 37.27 | >0.001 | ||||||
| Not breastfeeding | 63 | 33 | 12 | 11 | 28 | 44 | ||
| Partially breastfeeding | 30 | 15 | 13 | 12 | 17 | 26 | ||
| Exclusively breastfeeding | 100 | 52 | 81 | 76 | 19 | 30 | ||
| Median | Range | Median | Range | Median | Range | Test statistic | P‐value | |
| Number of C&FH nurse visits at 8 weeks | ||||||||
| Earlybird group | 2 | 0–8 | 4 | 1–8 | – | – | ||
| Centre | 2 | 0–9 | 1 | 0–9 | 3 | 1–9 | t (168)6.81 | 0.001 |
| Total | 4 | 1–11 | 6 | 1–11 | 3 | 1–9 | t (168)−7.09 | 0.001 |
| Maternal age | 30 | 17–43 | 30 | 20–39 | 30 | 17–43 | t (168)0.091 | 0.93 |
| Infant’s age (in days) at first visit to C&FH service | 12 | 5–56 | 12 | 5–47 | 12 | 5–38 | t (168)−1.06 | 0.29 |
C&FH, child and family health; NESB, non‐English speaking background.
The mean infant age at the first visit to C&FH services was 12 days (range 5–56 days). All mothers and babies in the sample either had a C&FH centre visit and/or attended the EBP at this time. Nineteen per cent (37/217) of the sample chose to attend the EBP only, 41% (79/193) attended the C&FH centre for individual consultations, and 40% (77/193) attended both the EBG and the centre.
Twenty‐three women (12%) in the sample were not breastfeeding at all by their first visit to the C&FH service either in the centre or in the EBP. Of the remaining women, 75% were exclusively breastfeeding and 13% were partially breastfeeding. By 8 weeks, 52% were exclusively breastfeeding and 30% were partially breastfeeding.
The women who were not breastfeeding during their first visit to the C&FH service were excluded from the sample for the remaining analyses as it was considered unlikely that these women would require C&FH nurses’ support for breastfeeding. The remaining analyses are based on a sample of 170 women who were exclusively or partially breastfeeding at their first visit to the C&FH service. Table 1 presents the differences between women who attended the EBP (either alone or combined with centre visits) and those women who did not select to attend the EBP when it was offered and attended only the C&FH centre (‘Centre Only’). Seventy‐two per cent of the sample (106/170) attended the EBP at some time in the first 8 weeks after birth.
There was no difference between the EBP group and the Centre Only group in the average age of the woman or the age of the infant at the first visit to the C&FH service (see Table 1). However, women who selected to attend the EBP were significantly more likely to be employed (75% vs. 38%) and less likely to be categorized as being from a non‐English speaking background. Women who chose to attend EBP were also more likely to be exclusively breastfeeding at their first visit (89% vs. 80%), although this did not reach statistical significance. On average, women in the EBP group compared with the Centre Only group had more visits to the C&FH service in total (median number of total C&FH visits 6 vs. 3), and had fewer of these visits one‐to‐one at the C&FH centre (medium number of centre visits 1 vs. 3). By 8 weeks, the EBP group were less likely to have ceased breastfeeding compared with the Centre Only group (11 vs. 44%), and were more likely to be breastfeeding exclusively (76% vs. 30%) at 8 weeks after birth. This difference was statistically significant [χ2(df1) 37.27, P = 0.001].
Logistic regression was used to determine the best predictors of breastfeeding cessation at 8 weeks and is presented in Table 2. Maternal employment, maternal age, non‐English speaking background, exclusive breastfeeding at first visit to the C&FH service, age of first visit and number of visits to the C&FH service, and EBP attendance were entered into the model alone (unadjusted) and then adjusted for all other variables.
Table 2.
Logistic regression results for exclusive breastfeeding at 8 weeks
| Variables | Unadjustedodds ratio† | 95% CI unadjustedodds ratio | Adjustedodds ratio‡ | 95% CI adjustedodds ratio |
|---|---|---|---|---|
| Employed | 1.61 | 0.77–3.37 | 1.26 | 0.53–2.97 |
| Maternal age | 0.94 | 0.88–1.02 | 0.96 | 0.89–1.04 |
| NESB | 1.05 | 0.51–2.14 | 2.04 | 0.84–4.96 |
| Infant’s age (in days) at first visit | 1.05 | 0.99–1.10 | 1.04 | 0.98–1.10 |
| BF status at first visit | 4.73* | 1.96–11.52 | 4.48* | 1.63–12.32 |
| Total number of visits to CFHS | 0.72* | 0.59–0.87 | 0.96 | 0.75–1.21 |
| Earlybird Program | 6.09* | 2.79–13.26 | 6.52* | 2.46–17.31 |
Statistically significant at P < 0.05;
† odds ratio entered into logistic regression alone;
‡ odds ratio entered into logistic regression adjusted for other variables. BF, breastfeeding; CFHS, child and family health service; NESB, non‐English speaking background.
Exclusive breastfeeding at the first visit, the total number of visits to the C&FH service and attending the EBP independently predicted breastfeeding cessation at 8 weeks. Women who were partially breastfeeding at the first visit compared with exclusively breastfeeding were more likely to cease breastfeeding at 8 weeks. Women who had more visits to the C&FH service were less likely to stop breastfeeding, and women who did not attend the EBP were more likely to cease breastfeeding (see Table 2).
After adjusting for other variables in the model, the number of visits to the C&FH service no longer significantly predicted breastfeeding cessation, and only exclusive breastfeeding at the first visit and attending the EBP were associated with continuing to breastfeed at 8 weeks.
Figure 1 presents the proportion of women who were exclusively breastfeeding at 8 weeks for different types of service (EBP and Centre Only) and number of visits (1–3, 4–6, >6). For the EBP group, the proportion of women exclusively breastfeeding increased and the proportion of those weaning decreased as the number of visits increased. These trends were not apparent for the Centre Only group.
Figure 1.
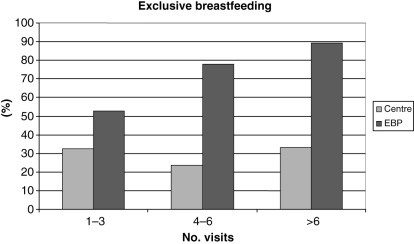
Breastfeeding status at 8 weeks by number of visits and type of service attended. EBP, Earlybird Program.
The relative advantage (RA) for breastfeeding (both exclusive and partial) at 8 weeks post‐natal for women who attended the EBP compared with those who did not is 1.58 (95% confidence interval RA 1.26–1.98). If a woman was exclusively breastfeeding at the first visit, the RA of breastfeeding at 8 weeks for EBP compared with the Centre Only group is 1.74 (95% confidence interval RA 1.35–2.24). If women were partially breastfeeding at the first visit, the RA between EBP and Centre Only groups was not apparent [RA = 0.54 (95% confidence interval RA 0.29–1.34)], although cell sizes were small.
Discussion
The EBP is a strategy developed by nurses in an area health service in metropolitan Sydney to improve professional and peer support for new mothers, in order to increase breastfeeding duration and maternal confidence, to heighten maternal–infant attachment, and to facilitate social support, peer support and learning. Since the introduction of the EBP, a number of C&FH centres in New South Wales have adopted this style of service and combine the EBP with universal home visiting and centre‐based services. This study attempted to examine the variables that influenced continued breastfeeding at 8 weeks post‐natal.
Limitations of the study
There are several limitations of this study that must be acknowledged. The study design was a retrospective audit of child health records with no random allocation to groups. This limits the predictive ability of the findings. This study can only examine associations between variables, and causality cannot be assumed. Women self‐selected into the EBP, and the two groups differed significantly in a number of variables, including the employment status prior to birth, the number of women from non‐English speaking backgrounds, the number of visits to the C&FH service, and the number of women who were exclusively breastfeeding at the first visit. It is likely that the women who self‐selected into the two groups had different resources, motivations and intentions, which may have influenced the outcome for the two groups.
We are unable to determine whether the two groups differed in their intention to breastfeed. However, a sample of 334 women from the same hospitals that provided care to women in the Earlybird study completed self‐reported surveys throughout the ante and post‐natal period (Cooke et al. 2006). The data were collected during an overlapping period with this Earlybird project. It is likely that many of the women were represented in both studies, but we are unable to link the data. In the hospital study, 86% of women antenatally reported the intention to breastfeed. Post‐natally, a further 86% of the women who ceased breastfeeding within 3 months reported ceasing breastfeeding earlier than planned (Cooke et al. 2006).
We are unable to determine whether women who attended the EBP would have continued breastfeeding whether they received the EBP or not, or whether women who attended only the centre would have benefited from the EBP had they received it. A randomized control design would be more appropriate to determine whether the EBP affects duration of breastfeeding.
It also needs to be acknowledged that this study only examined infant records from one C&FH centre. Over this period of time there was stability in the workforce, and over the 12‐month period three nurses worked at the C&FH centre. While each of these nurses also facilitated or co‐facilitated the EBP groups, one of these nurses was the main facilitator at each group during the period, and it may be that the breastfeeding outcomes for this sample are more related to the skill and style of this particular nurse than it is to any particular feature of the EBP.
Earlybird group and breastfeeding outcomes
This comparative analysis of retrospective child health record data suggests that there are several variables that are related to breastfeeding beyond 8 weeks post‐natal. These factors are exclusively breastfeeding at the first visit to the C&FH service, the number of visits, and whether the women have attended the EBP. These results support other studies that indicated that the earlier and more intensive support for breastfeeding can improve breastfeeding rates (Sikorski et al. 2003).
Women who accessed the EBP were more likely to breastfeed at 8 weeks than those women who did not attend the programme. This relationship holds even when variables such as breastfeeding status at first visit and the number of visits to the C&FH service are controlled for. The design of the study does not allow one to conclude that this effect was necessarily due to the EBP. Nevertheless, the proportion of women who were exclusively breastfeeding increased with the number of visits to the EBP, and the increase in the proportion of women exclusively breastfeeding because of the number of visits did not appear to occur with women who only attended the C&FH centre for individual consultations. It should, however, be noted that only a small number of women who attended the C&FH centre went more than three times in the 8 weeks, and the intensity of support for the Centre Only group may have been insufficient.
Alternatively, women who attended the EBP may have been more satisfied and found it more enjoyable or received more mother‐to‐mother support and therefore attended it more frequently. Women who accessed the EBP have reported elsewhere that they received substantial support in the establishment and maintenance of breastfeeding. Support around breastfeeding was seen to come from the observation that many women initially struggled but problems were quickly resolved. ‘It is so reassuring to know that so many other women have problems breastfeeding and to see that it actually does get easier’ (Kruske et al. 2004, p. 35).
Furthermore, when women who were exclusively breastfeeding at the first visit were examined separately, the results held. That is, women who attended the EBP and were exclusively breastfeeding at the first visit were more likely than women in the Centre Only group and were exclusively breastfeeding to continue to breastfeed beyond 8 weeks. However, there was no difference in the rates of breastfeeding at 8 weeks for women who were partially breastfeeding at the first visit regardless of whether they received EBP or Centre Only programmes. It would appear that neither the EBP or one‐to‐one support from the centre staff can influence a woman’s decision to breastfeed once the process and perhaps the decision to cease breastfeeding has begun. Again this supports the importance of promoting exclusive breastfeeding in the initial weeks after birth and of early intervention.
As this study did not use a controlled, experimental design, it may be that women who access the EBP are more motivated to breastfeed and therefore go to the groups as well as utilize the one‐to‐one service more often. Thus, they are more ‘successful’ at breastfeeding. Women who were not breastfeeding at first contact with the service were less likely to access the EBP. It must be acknowledged that women who formula feed their infants may be reluctant to access a group that appear to be dominated by breastfeeding women. However, women who did attend the EBP and were formula feeding reported that they felt supported and did not ‘feel judged’ by the nurses and other group participants (Kruske et al. 2004).
The nurses facilitating the groups reported that one of the strengths of the EBP was the provision of support early in the post‐partum period, with some women attending the group when their infant was as young as 6 days old (SESAHS 2001). The importance of early access to professional support is considered a factor in increasing breastfeeding duration (Renfrew et al. 2000; Sikorski et al. 2003), and the women who participated in the evaluation of the EBP (Kruske et al. 2004) believed that early attendance impacted on continued breastfeeding. However, there was no difference in the age of the baby at the first visit between women who were breastfeeding at the first visit and those who were not. It appears that early access to professional support was also available to women choosing individual consultations because of the availability of some women to the EBP. This could be explained by anecdotal reports by the nurses that the EBP resulted in more centre time being available for appointments for women who preferred this option.
Women who accessed the EBP were less likely to be from a non‐English speaking background. This was to be expected, however, as the EBP is conducted only in English and Chinese (facilitated by a bilingual C&FH nurse). Only the child health records of women who had access to the programme conducted in English were examined in this study. Ethnicity and low socio‐economic status has been reported to be an important predictor of breastfeeding (Scott et al. 2001b; Lin et al. 2004). However, in a recent review in New South Wales, the only ethnic group related to lower rates of both initiation and duration was Aboriginal women (Hector et al. 2004). There were no Aboriginal women in this study of the EBP, and there were no differences in the breastfeeding rates between English‐speaking and non‐English speaking women.
Improving professional support through the Earlybird Program
In the absence of social exposure to breastfeeding and low levels of knowledge and community support, it is argued that breastfeeding women benefit from support provided by health professionals (Renfrew et al. 2000). The findings of this retrospective analysis of health record data suggest that early and intensive support provided to a group of new mothers with professional facilitation may have the potential to increase exclusive breastfeeding at 8 weeks post‐partum. The qualitative evaluation reported by Kruske et al. (2004) suggests that the nature of the professional support provided by C&FH nurses facilitating the EBP can provide a better understanding of what may be the elements of ‘successful’ breastfeeding interventions (Sikorski et al. 2003).
In a review of the literature on breastfeeding initiation and duration, Dennis et al. (2002) identify the value of health professionals employing specific confidence‐building strategies, such as: drawing attention to the successful or improved aspects of breastfeeding; reinforcement of positive breastfeeding skills; provision of consistent advice on breastfeeding; encouragement to recall the positive aspects of breastfeeding experience rather than focusing solely on current difficulties; and, provision of anticipatory guidance to acknowledge and normalize a mother’s anxiety, the discomfort or pain and fatigue .
While these strategies can be effective in one‐to‐one consultations with mothers, the observation data collected for the evaluation of the EBG indicate that on a weekly basis, the C&FH nurses facilitating the EBP use such strategies in the context of group‐based new parenting programmes (Kruske et al. 2004).
Improving peer support through the Earlybird Program
It could be argued that one of the key components on the success of the programme is the specific facilitation skills of the nurses who adopted a partnership model that recognized and promoted the expertise of the mothers. This was achieved by the use of open questions, by reflecting questions back to the participants, by asking the women whether they had experienced similar situations or feelings, and by assisting the women to reflect on their experience in a way that more explicitly assesses their own learning (SESIAHS 2005).
This form of facilitation combines the key concepts of ‘peer support groups’ in which participants learn from each other and ‘working in partnership with families’ (Davis et al. 2002), in which the content expertise of the professional/facilitator is not required nor is the key focus of the group discussion. The nurse has content expertise to allow immediate access to relevant information when required. This combined ‘partnership and peer support model’ assumes that a respectful partnership between parents and nurses is a powerful support in its own right and the means by which parents’ confidence may be increased (SESIAHS 2005).
In the context of the EBP, the ‘peer supporters’ are mothers who are moving through the same temporal period. In an informal way, mothers share experiences and provide affirmation and reassurance for each other. As one mother who participated in the qualitative evaluation of the EBP described, ‘I thought that mothers didn’t know anything like me, but it is amazing how we all helped each other’ (Kruske et al. 2004, p. 34).
Involving clients in actively recognizing and drawing on their own resources is more likely to lead to sustained behaviour change and improved health (Davis et al. 2002). Dispensing advice and information without client involvement will likely inhibit development and independent mobilizing of client resources (Cowley 1999; Houston & Cowley 2002). In the EBP, the approach is to ‘de‐professionalise’ infant feeding by linking mothers to credible and informed advice from other women. In this way, nurses value women’s own knowledge and experience.
The skills required to effectively facilitate the EBP require a fundamental paradigm shift from ‘expert’ to ‘partner’ and can be challenging for nurses who have worked within an authoritative model throughout their professional lives. Adequate educational preparation and ongoing support in both breastfeeding and facilitation skills using the combined ‘professional and peer support model’ is essential for the EBP to achieve its aims.
Developing partnerships with mothers
It is thus important that the design of strategies to support breastfeeding and other aspects of parenting draws on the concepts of partnership and a strengths‐based approach. The EBP attempts to build confidence in women by utilizing a strengths‐based approach to practice by valuing the experience and knowledge of new mothers and their supports. Not only do the groups provide support for the individual mother, it also allows her to provide similar support in return, and this cannot occur with individual consultations (Bowes 2004).
It must be recognized that some clients may be seen as not wanting to work in partnership with the practitioners (Waterworth & Luker 1990). This may occur if they feel too overwhelmed to make any contributions of their own, or if they perceive self‐participation as weakness or incompetence on behalf of the practitioner (Barnes & Freude‐Lagevardi 2003).
In light of the decrease in breastfeeding rates in the first 8 weeks across Australia and abroad, further research is needed to examine the way in which C&FH nurses approach the promotion, or support of, breastfeeding, either in one‐to‐one centre consultations or in new parents’ groups.
Questions remain concerning the role and competency of nurses in the promotion and support of breastfeeding both in individual consultations between C&FH nurses and mothers and in new mothers’ groups. Given that there was less uptake of centre consultations compared with the EBP, further research could explore the ways in which C&FH nurses can engage women who choose not to access parenting groups and who prefer individual face‐to‐face consultations.
Conclusion
There is ample evidence on the rapid fall in breastfeeding rates in the first months of infant life, with much of that occurring in the first 4 weeks (Hector et al. 2004). This paper identifies the importance of early and intensive support for breastfeeding. It suggests that a combination of professional and peer support through effective facilitation by the C&FH nurse to work in partnership with women is valuable in the early weeks of parenting. A randomized controlled trial is required to determine the effect of EBP on breastfeeding, and more research is required to explore the ways in which C&FH nurses can engage women who choose not to access parenting groups and who prefer individual face‐to‐face consultations.
Acknowledgements
The authors thank all the child and family health nurses in St George Child and Family Health Services in Sydney, Australia, for their support in this programme.
For her added contribution, grateful acknowledgement is also extended to Ivy Sutton, who assisted Sue Kruske in the collection of data. The authors also acknowledge the contribution and support of the late Joan O’Hare, previous manager of the C&FH team and ardent supporter of the programme. This evaluation was funded by the Australian Department of Health and Aged Care under the National Childhood Nutrition Project.
Facilitators’ Manual: a manual on the programme is available through: Nurse Unit Manager, St George Child and Family Health Service, Suite 65, 23–27, MacMahon St, Hurstville, NSW 2220, Australia. Tel: 02 9580 5843; Fax: 02 9350 6018.
Footnotes
In Australia, the title varies across the states and territories, and includes: maternal and child health nurses (Victoria and the Australian Capital Territory); child health nurses (Western Australia, Queensland and the Northern Territory); child and youth health nurses (South Australia); and child and family health nurses in New South Wales and Tasmania.
No bookings are required, and there are no restrictions to the number of women allowed to attend.
References
- Barnes J. & Freude‐Lagevardi A. (2003) From Pregnancy to Early Childhood: Early Interventions to Enhance Mental Health in Children and Families. The Mental Health Foundation: London. [Google Scholar]
- Bowes J. (2004) From theory to practice: issues arising for a novice home visitor. Australian Journal of Primary Health 10, 83–91. [Google Scholar]
- Clarke V., Hanna B., Rolls C., Grant A., Bethune E., Horne R. et al. (1995) Evaluation of Group Sessions for First Time Mothers Provided by the Victorian Maternal and Child Health Service. Deakin University: Geelong. [Google Scholar]
- Clune L. (1999) Parenting Education: A Review of Current Services. South Eastern Sydney Area Health Service: Sydney. [Google Scholar]
- Cooke M., Schmied V. & Sheehan A. (2006) An exploration of the relationship between postnatal distress, maternal role attainment, breastfeeding problems and breastfeeding cessation. Midwifery (in press). [DOI] [PubMed]
- Cowley S. (1999) Resources revisited: salutogenesis from a lay perspective. Journal of Advanced Nursing 29, 994–1004. [DOI] [PubMed] [Google Scholar]
- Davis H., Day C. & Bidmead C. (2002) Working in Partnership with Parents: The Parent Advisor Model. The Psychological Corporation Limited: London. [Google Scholar]
- Dennis C., Hodnett E., Gallop R. & Chalmers B. (2002) The effect of peer support on breast‐feeding women: a randomised controlled trial. Canadian Medical Association Journal 166, 21–28. [PMC free article] [PubMed] [Google Scholar]
- Donath S. & Amir L. (2000) Rates of breastfeeding in Australia by state and socioeconomic status: evidence from the 1995 National Health Survey. Breastfeeding Review 8, 23–27. [PubMed] [Google Scholar]
- Dykes F. (2003) Infant Feeding Initiative: A Report Evaluating the Breastfeeding Practice Projects 1999–2002. UK Department of Health: London. [Google Scholar]
- Freeman A. & Lamb C. (1997) New Mothers Group Program Evaluation. Central Sydney Area Health Service, Early Childhood Health Services: Sydney. [Google Scholar]
- Guise J., Palda V., Westhoff C., Helfand M. & Lieu T. (2003) The effectiveness of primary care‐based interventions to promote breastfeeding: systematic evidence review and meta‐analysis for the US Preventive Services Task Force. Annals of Family Medicine 1, 70–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hector D., Webb K. & Lymer S. (2004) State of Food and Nutrition in NSW Series: Report on Breastfeeding in NSW 2004. NSW Centre for Public Health Nutrition/NSW Department of Health: Sydney. Available at: http://www.health.nsw.gov.au/pubs/2005/breastfeeding_rep.html [Google Scholar]
- Hoddinott P. & Pill R. (1999) Qualitative study of decisions about infant feeding among women in East End of London. British Medical Journal 318, 30–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houston A. & Cowley S. (2002) An empowerment approach to needs assessment in health visiting practice. Journal of Clinical Nursing 11, 640–650. [DOI] [PubMed] [Google Scholar]
- Kisten N., Abrahanson R. & Dublin P. (1994) Effect of peer counselors on breastfeeding initiation, exclusivity and duration among low‐income urban women. Journal of Human Lactation 10, 11–15. [DOI] [PubMed] [Google Scholar]
- Kruske S., Schmied V., Sutton I. & O’Hare J. (2004) Mothers’ experiences of facilitated peer support groups and individual child health nursing support: a comparative evaluation. Journal of Perinatal Education 13, 31–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leap N. (1993) Helping You to Make Your Own Decisions. Antenatal and Postnatal Groups in Deptford, South East London. VHS Video: 30 mins. Available online: http://www.birthinternational.com.au [Google Scholar]
- Leap N. (2000) The less we do, the more we give In: The Midwife–Mother Relationship (ed. Kirkham M.), pp. 1–18. Macmillan Press: London. [Google Scholar]
- Lin L., Zhang M., Scott J. & Binns C. (2004) Factors associated with the initiation and duration of breastfeeding of Chinese mothers in Perth, Western Australia. Journal of Human Lactation 20, 188–195. [DOI] [PubMed] [Google Scholar]
- Locklin M. (1995) Telling the world: low income women and their breastfeeding experiences. Journal of Human Lactation 11, 285–291. [DOI] [PubMed] [Google Scholar]
- Long A. (2001) The effectiveness of parenting programmes facilitated by health visitors. Journal of Advanced Nursing 34, 611–620. [DOI] [PubMed] [Google Scholar]
- Lowe T. (1993) Regional and socio‐economic variations in the duration of breastfeeding in Victoria. Breastfeeding Review 2, 312–315. [Google Scholar]
- Murphy E. (1999) ‘Breast is Best’: infant feeding decisions and maternal deviance. Sociology of Health and Illness 21, 187–208. [Google Scholar]
- NHMRC (2003) Dietary Guidelines for Children and Adolescents: Incorporating the Infant Feeding Guidelines for Health Workers. National Health and Medical Research Council: Canberra. [Google Scholar]
- NSW Health (2003) Personal Health Record. NSW Health: Sydney. [Google Scholar]
- Nutbeam D., Wise M., Bauman A. & Harris E. (1993) Goals and Targets for Australia’s Health in the Year 2000 and Beyond. Australian Government Publishing Service: Canberra. [Google Scholar]
- Nystrom K. & Ohrling K. (2004) Parenthood experiences during the child’s first year: literature review. Journal of Advanced Nursing 46, 319–330. [DOI] [PubMed] [Google Scholar]
- Renfrew M., Woolridge M. & McGill R. (2000) Enabling Women to Breastfeed: A Review of Practices Which Promote or Inhibit Breastfeeding –With Evidence‐Based Guidance for Practice. Mother and Infant Research Unit, University of Leeds: London. [Google Scholar]
- Rodwell C. (1996) An analysis of the concept of empowerment. Journal of Advanced Nursing 23, 305–313. [DOI] [PubMed] [Google Scholar]
- Schmied V. & Lupton D. (2001) Blurring the boundaries: breastfeeding and maternal subjectivity. Sociology of Health and Illness 23, 234–250. [Google Scholar]
- Scott D., Brady S. & Glynn P. (2001a) New mother groups as a social network intervention: consumer and maternal and child health nurse perspectives. Australian Journal of Advanced Nursing 18, 23–29. [PubMed] [Google Scholar]
- Scott J., Aitkin I., Binns C. & Aroni R. (1999) Factors associated with the duration of breastfeeding amongst women in Perth, Australia. Acta Paediatrica 88, 416–421. [DOI] [PubMed] [Google Scholar]
- Scott J., Landers M., Hughes R. & Binns C. (2001b) Factors associated with breastfeeding at discharge and duration of breastfeeding. Journal of Paediatrics and Child Health 37, 254–261. [DOI] [PubMed] [Google Scholar]
- SESAHS (2001) Early Bird Evaluation Report. Kogarah Child and Family Health Centre: Sydney. [Google Scholar]
- SES Council (2003) Kogarah’s People. Kogarah Council: Kogarah. [Google Scholar]
- SESIAHS (2005) Earlybird Program: A Parenting Program for Families with Infants Newborn to Eight Weeks. South Eastern Sydney Illawara Area Health Service: Sydney. [Google Scholar]
- Shaw E. & Kaczorowski J. (1999) The effect of a peer counseling program on breastfeeding initiation and longevity in a low income rural population. Journal of Human Lactation 15, 19–25. [DOI] [PubMed] [Google Scholar]
- Sikorski J., Renfrew M., Pindoria S. & Wade A. (2003) Support for breastfeeding mothers: a systematic review. Paediatric and Perinatal Epidemiology 17, 407–417. [DOI] [PubMed] [Google Scholar]
- Waterworth S. & Luker K. (1990) Reluctant collaborators: do patients want to be involved in decisions concerning care? Journal of Advanced Nursing 15, 971–976. [DOI] [PubMed] [Google Scholar]