

Abstract
The aims of the current study were to (1) identify dietary patterns in 3‐year‐old children; (2) investigate the extent to which negative affectivity, external parental locus of control and control‐oriented child‐feeding practices (pressure to eat and restriction) relate to these dietary patterns; and (3) to examine to what extent external parental locus of control and control‐oriented child‐feeding practices serve as mediators for these effects. This study was part of the Norwegian Mother and Child Cohort Study, comprising 14 122 mothers completing assessments at 6 months, 18 months and 3 years post‐partum. Factor analysis of the children's diet identified two weakly correlated dietary patterns, labeled ‘unhealthy’ and ‘wholesome’. Mothers high in negative affectivity perceived they had little control over their child's behaviour, which in turn was associated with both pressuring their child to eat and restricting the child's food intake and a less wholesome and a more unhealthy diet in the child. Pressuring the child to eat was independently associated with a less wholesome and a more unhealthy diet. Restricting the child's diet was associated with a more wholesome and a less unhealthy diet. These findings held after controlling for maternal smoking, education, age, body mass index, marital status, homemaker status and child gender.
Keywords: child‐feeding, preschool children, parenting, dietary patterns, maternal mental health, personality
Introduction
With the epidemic increase in childhood obesity, childhood diet has become the focus of much research interest in recent years (Wang & Lobstein 2006). Previous studies of diet in preschool children have identified two main patterns (North & Emmett 2000; Ystrom et al. 2009); one pattern describes the consumption of ‘unhealthy’ sugary foods, such as soda, chocolate and sweets, and the other describes the consumption of ‘wholesome’ foods, such as vegetables, fruit and fish.
The person with the greatest influence on a child's diet during preschool years is arguably the mother, and the mother's characteristics, in turn, influence her food choices on behalf of her child. Being young, overweight, a smoker or having lower educational attainment or more than one child increases the likelihood that a mother feeds her child less wholesome foods and more unhealthy ones (North & Emmett 2000; Ystrom et al. 2009).
Meal times can be emotive for both mother and child. Children often prefer foods with high fat and sugar content (Hill 2002). However, mothers know that their children should not eat too much of these foods, and that they should have their children eat healthier alternatives. This can result in a situation that is familiar to most parents: the frustration of trying to feed a child foods that he or she refuses to eat. This situation is stressful for most mothers. It might be especially so for emotionally unstable mothers, who may perceive they lack control over their child (Lovejoy et al. 1997) and respond to the child inconsistently (Metsapelto & Pulkkinen 2003). Emotional instability, frequently called negative affectivity (NA), is a basic personality trait that is an innate inclination to emotional variability; to frequently experiencing states of negative affect such as anxiety, depression, anger and sadness; and to hold a negative view of the world and one's self (Watson & Clark 1984).
In previous studies, we have shown that mothers characterized by high levels of NA were less likely to breastfeed exclusively throughout the baby's first 6 months (Ystrom et al. 2008) and more likely to feed their children an unhealthy diet at 18 months of age (Ystrom et al. 2009). An explanation for this pattern could be that persons with high levels of NA believe that the behaviour and development of their child is not contingent on their parenting but is largely determined by external forces such as child temperament and chance (Lovejoy et al. 1997). This belief is captured by the construct of external parental locus of control. Parents perceiving they have little control over their child (Janssens 1994) and parents with higher levels of NA (Metsapelto & Pulkkinen 2003) tend to compensate by using excessive parental control. More specifically, mothers who experience states of NA make use of control‐oriented child‐feeding practices, such as pressuring the child to eat and restricting the child's food intake, during the two first years after birth (Farrow & Blissett 2005; Blissett & Farrow 2007; Hughes et al. 2008).
Interest in parental feeding practices has increased in recent years because of their potential to affect child obesity (Birch et al. 2001). Some recently developed scales assess parents' need to control the feeding situation. Contrary to what we might expect, control‐oriented child‐feeding practices predict that the child consumes fewer wholesome and more unhealthy foods (Birch et al. 1987; Fisher & Birch 1999a, 1999b; Fisher et al. 2002; Patrick et al. 2005; Brown et al. 2008).
The present study continues and extends our previous work on the relation of maternal NA and child feeding in children aged 6 and 18 months (2008, 2009). We aim to test the following hypotheses using data from the Norwegian Mother and Child Cohort Study while controlling for key demographic and physical variables:
-
•
Hypothesis 1. In the present study, we seek to re‐identify among 3‐year‐olds the two dietary patterns of wholesome and unhealthy diet that we found in the children when they were 18 months old (Ystrom et al. 2009).
-
•
Hypothesis 2. As high NA is associated with external parental locus of control, and both NA and external parental locus of control are related to an increase in parental control, we hypothesize that mothers high in NA are more likely to use control‐oriented child‐feeding practices. At the same time, we postulate that the effect of NA on control‐oriented child‐feeding practices will be mediated through external parental locus of control (see Fig. 1).
-
•
Hypothesis 3. We hypothesize that mothers with higher levels of NA and external parental locus of control will have a child with both more unhealthy and less wholesome dietary patterns. This association, again, will be mediated through greater use of the two forms of control‐oriented child‐feeding practices of pressuring the child to eat and restricting the child's food intake (Fig. 1).
-
•
Hypothesis 4. Because it is possible that control‐oriented child‐feeding practices affect diet over and above the effects of maternal personality and parental control beliefs, we hypothesize that pressuring the child to eat and restricting the child's food intake will have an independent negative effect on the child's wholesome dietary pattern and a positive effect on the unhealthy dietary pattern (Fig. 1).
Figure 1.
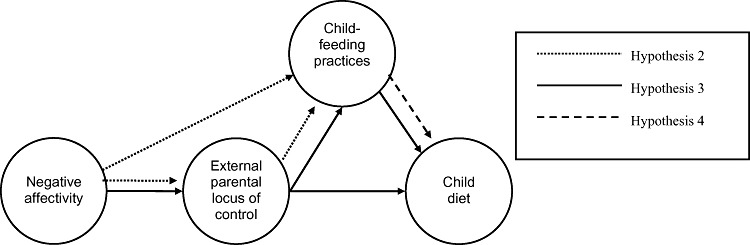
Conceptual model of the interrelation between maternal negative affectivity, external parental locus of control, child‐feeding practices and child diet.
Key messages
-
•
Studies have found that child diet can be divided into a pattern of two main factors. One ‘wholesome’ factor comprising fruit, vegetables and fish and an ‘unhealthy’ factor comprising sugary food of low nutritional value.
-
•
Control‐oriented child feeding has to a great extent an independent detrimental effect on child diet over and beyond that of negative affectivity and external parental locus of control.
-
•
Mothers' experience of control in the preventing situation is of substantial relevance with regards to child diet and it can be viewed as an important malleable mechanism for healthy eating in preschool‐aged children.
Methods
Study population
The data collection was conducted as a part of the Norwegian Mother and Child Cohort Study (MoBa) at the Norwegian Institute of Public Health. The study was launched in 1999 with the purpose of finding causes of serious diseases among mothers and children (Magnus et al. 2006). There are no exclusion criteria, and all maternity units in Norway with more than 100 births annually are included. Mothers are recruited for the study when they undergo their first prenatal ultrasound examination at 17 to 18 weeks gestation. The participation rate in MoBa is 42.7%. Mothers fill out questionnaires at 17 weeks gestation and at child age 6 months, 18 months and 3 years. Response rates are 95% during pregnancy; after birth, they are 87% at 6 months, 77% at 18 months and 62% at 3 years (Magnus et al. 2006; Magnus 2007). For our study, we used information from the questionnaires administered at the assessment points mentioned above. In addition, we used the Medical Birth Registry of Norway, which contains information about all births in Norway (Irgens 2000). The study was approved by the appropriate regional committees for ethics in medical research and the Norwegian National Data Inspectorate.
At the time we conducted this study, questionnaires from 15 103 participating mothers with a child that had reached 3 years of age were available. We excluded 6.5% (n = 981) of the participants because of missing data on categorical independent variables. The final sample therefore consisted of 14 122 mothers.
Compared with participants, a greater proportion of the mothers who were single were excluded because of missing data. There was no other significant difference in demographic and physical variables between participating mothers and those excluded because of missing data (see Table 1).
Table 1.
Characteristics of the mothers included and those excluded because of missing data*
| Included (n = 14 122) | Excluded (n = 981) | |
|---|---|---|
| Child gender boy (%) | 51.2 | 48.9 [978] |
| Daily smoking (%) | 11.0 | 23.1 [26] |
| Education (years) | 14.4 ± 2.4 † | 14.4 ± 2.4 |
| Homemaker (%) | 30.2 | 27.6 [261] |
| Maternal age (years) | 33.0 ± 4.6 | 32.9 ± 4.5 |
| Maternal BMI | 24.8 ± 4.4 | 24.7 ± 3.8 |
| Single marital status (%) | 6.0 | 10.1 [238] ‡ |
Number of cases in brackets.
† Mean (standard deviation) (all such values).
Significantly different from the included cases (χ2 test): P < 0.05. BMI, body mass index.
Measures
Demographic and physical risk factors
We gathered information on child gender and maternal age from the Medical Birth Registry of Norway. We retrieved information on the mothers' smoking status (current regular smoker or non‐smoker), education (years attained), current homemaker vs. working status, current body mass index (BMI) and current marital status (single or cohabiting/married) from the MoBa questionnaires.
NA
To assess maternal NA, we constructed a latent factor from several scales tapping different facets of NA, each measured three times in the questionnaires completed at child age 6 months, 18 months and 3 years. The anxiousness/depressiveness component of NA was assessed using an 8‐item short version of the Hopkins Symptom Checklist (SCL‐8) (Strand et al. 2003). The anger component of NA was assessed by means of the Anger subscale of the Differential Emotions Scale (Izard et al. 1993). The self‐esteem component of NA was assessed using a 4‐item short version of the Rosenberg Self‐Esteem Scale (Rosenberg 1989).
We used confirmatory factor analysis (CFA) for ordinal data with polychoric correlations (Flora & Curran 2004) to construct the NA components anxiousness/depressiveness, anger and self‐esteem. By forcing the thresholds of the response categories within each item, the scaling of each item and the factor structure of each scale to be equal across time points, we secured syntactically equal measurement. As a first step, we combined the three NA components at each time point into a latent variable of time‐specific NA. Second, we forced the factor loadings of the NA measure to be equal across time. In the last step, we constructed a time‐invariant NA‐latent variable by setting the factor loadings equal across time. This procedure assured that the time‐specific individual deviations were removed from the NA variable. The score therefore constitutes the individual characteristic across time. A detailed overview of factor loadings for this measurement model is presented elsewhere (Ystrom et al. 2009).
The construct of Neuroticism fully overlaps with NA (Clark & Watson 1999). In an earlier study, we showed that our present operationalization of NA correlates 0.92 with Neuroticism (Ystrom et al. 2009). This suggests that the NA measure used here is valid.
Parental locus of control
External parental locus of control was assessed at child age 3 years by means of five items from the Parental Locus of Control Scale (Appendix S1) (Campis et al. 1986). The Parental Locus of Control Scale is a measure of the extent to which parents believe that the behaviour of their child is controlled by their own parenting skills or by other events external to their parenting. A high score on the Parental Locus of Control Scale indicates an external parental locus of control, and a low score indicates a more internal parental locus of control.
To construct a variable for parental locus of control, we performed CFA for ordinal data on the items from the Parental Locus of Control Scale. The items loaded freely on a factor with variance set to 1. Because the Parental Locus of Control Scale can be divided into sub‐dimensions, we allowed the items that were from the same sub‐dimension to correlate in the CFA.
Child‐feeding practices
Two forms of control‐oriented child‐feeding practices, restriction of child food intake and pressuring the child to eat, were measured at age 3 using the ‘restriction’ and ‘pressure to eat’ subscales of the Child Feeding Questionnaire (Birch et al. 2001). The Child Feeding Questionnaire is a tool for assessing parents' perceptions, beliefs, attitudes and practices regarding child feeding. A typical question from the subscale ‘pressure to eat’ is ‘My child should always eat all of the food on her plate’, and a typical question from the subscale ‘restriction’ is ‘I have to be sure that my child does not eat too many sweets (candy, ice cream, cake, or pastries)’. For each statement, the respondents indicated to ‘agree’ or ‘disagree’ on a 5‐point scale.
To construct variables for the child‐feeding practices of ‘restriction’ and ‘pressure to eat’, we used CFA for ordinal data with polychoric correlations. The items loaded freely on a factor with variance set to 1. To account for internal dependencies between the items from the ‘restriction’ scale combined in parcels by Birch et al. (2001), the residual variance of the indicators within each item parcel was allowed to correlate.
Child's diet
Mothers described the current diets of their 3‐year‐olds on a food frequency questionnaire with 37 items. For each food and drink item, mothers reported the frequency of consumption in a usual month using response categories ranging from ‘never or less than one serving per week’ to ‘four or more servings per day’ for non‐dinner foods and drinks and ‘once per month or less’ to ‘five or more times per week’ for dinner foods.
Statistical analyses
We conducted independent t‐tests with the continuous variables and chi‐squared tests with the categorical variables to compare the characteristics of the mothers included in the analysis and those excluded because of missing data. We used Mplus 5.1 (Muthén & Muthén, Los Angeles, CA, USA) for the exploratory factor analysis (EFA), confirmatory factor analyses and structural equation modeling (SEM).
Dietary patterns
To identify dietary patterns from the 37 dietary items, we calculated a polychoric correlation coefficient matrix from the frequency with which each child was reported to consume each food in a month. We then conducted EFA with this correlation matrix.The combination of the polychoric correlation matrix and EFA is a technique for assessing the multivariate factor structure of data measured on an ordinal scale. To rotate the factor solution, we used the geomin oblique rotation (Browne 2001). We analyzed the scree plot and identified the first two dietary pattern factors. In the present analysis, we sought to find the smallest number of factors that could explain the greatest amount of multivariate covariance.
Mediation analysis
A mediator is defined as the mechanism through which the independent variable influences the dependent variable (Baron & Kenny 1986). Baron & Kenny (1986) specify four steps as the sine qua non (i.e. prerequisite) of mediation. First, the independent variable and the dependent variable have to be associated. Second, the independent variable has to be related to the mediator. Third, the mediator has to be related to the dependent variable. Last, the relationship between the independent variable and the dependent variable has to disappear or be weakened. Complete mediation is achieved when the association between the independent variable and the dependent variable disappears after controlling for the mediator; partial mediation is achieved when the association is reduced, although not a specific criterion for mediation: if there is an interaction effect between the mediator and the independent variable in relation to the dependent variable, one cannot exclude the possibility of a competing moderator approach.
Structural equation modeling
The EFA of child diet, the CFAs of the psychometric measures, and the physical and demographic variables were included in a final SEM model and jointly estimated. We defined NA, the demographic variables and the physical variables as independent variables; external parental locus of control and child‐feeding practices as independent or mediation variables; and the two predicted dietary patterns as correlated dependent variables in a multivariate linear regression using SEM.
We chose robust weighted least‐squares estimation (robust WLS) to identify the model (Flora & Curran 2004; Muthén & Muthén, Los Angeles, CA, USA), as CFA using polychoric correlations has been proven to be robust to the non‐normal distribution typical for behavioural data. Using robust WLS in Mplus 5.1 with covariates included in the model prohibited us from estimating confidence intervals (CI) of the standardized coefficients. The unstandardized coefficients and confidence intervals are available upon request.
As a part of the final SEM model, we estimated missing data for dependent variables as a function of the covariates in the model. We imputed missing data on continuous independent variables with the information from continuous covariates using the expectation‐maximization algorithm. Furthermore, as mentioned above in the sample description, we excluded cases with missing data on categorical independent variables from the analyses. To evaluate model fit to the data, we interpreted the root mean square of approximation (RMSEA), where a point value below 0.06 is considered necessary for a good fit (Hu & Bentler 1998). Using robust WLS, it was not possible for us to calculate a confidence interval for the RMSEA.
Results
The SEM analysis, which simultaneously included all the CFAs and the multiple regression analysis, had a good fit to the covariance matrix (RMSEA of 0.03).
CFA of mother's NA, parental locus of control and child‐feeding practices
The factor structure and loadings from the CFA for ordinal data on mother's personality were meaningful. The median item factor loadings for anxiety/depressiveness, anger and self‐esteem were 0.79, 0.79 and 0.78, respectively. The median factor loading of the time‐specific NA variables was 0.74. For the time‐invariant NA variable, the median factor loading was 0.86. The factor loadings from the CFA on the items from the Parental Locus of Control Scale were adequate and are presented in Appendix S1. The factor loadings for the two scales measuring child‐feeding practices were less coherent and are presented in Appendix S1.
The time‐specific measures of anxiousness/depressiveness, anger, self‐esteem and NA were not differentially related to external parental locus of control, child feeding or child diet. This indicates that the general NA variable does not obscure the relation between domain or time‐specific measures of NA and the predicted outcomes.
Hypothesis 1: identification of dietary patterns
When inspecting the scree plot (Fig. 2) from the EFA of the child's diet, we found that a two‐factor solution gave the best‐fitting parsimonious solution. Because this factor pattern was nearly identical to the pattern found at child age 18 months in the same sample, we labelled the first factor unhealthy and the second factor wholesome. In summing the indicators with factor loadings above 0.30, the unhealthy factor describes a pattern of eating characterized by consumption of chips, buns, cakes, waffles, chocolate, cookies, sweets, soda, ice cream, popsicles, bread with jam or honey, pizza and soda with artificial sweeteners (Table 2). The wholesome factor describes a pattern characterized by consumption of white fish, oily fish, boiled vegetables, raw vegetables, fruit, bread with fish products, egg, bread with meat, Norwegian brown cheese and fish products (Table 2).
Figure 2.
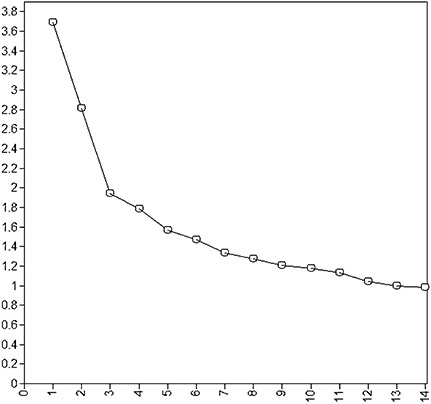
Scree plot from the exploratory factor analysis of child diet. Factor number on the x‐axis and eigenvalues on the y‐axis. Two factors were extracted.
Table 2.
Standardized rotated factor loadings of various dietary items in the two dietary factors identified in 3‐year‐old children based on the food frequency questionnaire (loadings above 0.3 are shown in bold)
| Unhealthy | Wholesome | |
|---|---|---|
| Chocolate | 0.62 | −0.08 |
| Chips | 0.56 | −0.06 |
| Sweets | 0.56 | −0.07 |
| Buns, cakes and waffles | 0.54 | 0.05 |
| Ice cream | 0.54 | 0.10 |
| Cookies | 0.54 | −0.02 |
| Popsicle | 0.51 | 0.08 |
| Soda | 0.48 | −0.07 |
| Bread with jam or honey | 0.33 | −0.02 |
| Pizza | 0.30 | 0.02 |
| Soda with artificial sweeteners | 0.30 | −0.15 |
| Pancakes | 0.21 | 0.03 |
| Juice | 0.18 | 0.11 |
| Meat, sausage and meatballs | 0.16 | 0.08 |
| Slices per day of fibre‐rich bread | −0.14 | 0.09 |
| Flavoured yogurt | 0.13 | 0.04 |
| Bread, slices per day | −0.11 | 0.07 |
| Skimmed and semi‐skimmed milk | −0.07 | 0.00 |
| Boiled vegetables | −0.10 | 0.50 |
| White fish | −0.04 | 0.50 |
| Oily fish | −0.08 | 0.49 |
| Raw vegetables | −0.07 | 0.44 |
| Fruit | −0.09 | 0.37 |
| Bread with fish products | −0.05 | 0.35 |
| Egg | 0.16 | 0.35 |
| Potatoes | 0.00 | 0.28 |
| Bread with cheese | 0.04 | 0.27 |
| Soup | 0.16 | 0.26 |
| Fish products | 0.05 | 0.26 |
| Raisins | 0.08 | 0.25 |
| Bread with meat | 0.04 | 0.24 |
| Rice | 0.02 | 0.18 |
| Plain yogurt | −0.06 | 0.17 |
| Norwegian brown cheese | −0.03 | 0.17 |
| Soured milk with LGG | −0.07 | 0.16 |
| Pasta | 0.09 | 0.15 |
| Full‐cream milk | 0.08 | 0.14 |
The two dietary factors correlate: −0.11 (P < 0.01). LGG, Lactobacillus rhamnosus GG.
The two factors, unhealthy and wholesome diet, were modestly inversely associated (r = −0.11; 95% CI −0.09 to −0.12). After adjusting for NA, external parental locus of control, child‐feeding, and physical and demographic characteristics, the residual correlation was non‐significant (r = −0.04; 95% CI −0.08 to 0.00).
Hypothesis 2: effect of NA on child‐feeding practices mediated through parental locus of control
To investigate whether there was no, partial or full mediation of NA through external parental locus of control on the child‐feeding practices, we first identified associations between NA and the child‐feeding practices, second between both NA and external parental locus of control, and third between external parental locus of control and the child‐feeding practices. The criteria for mediation as described in the statistics section were met, because all associations among independent, mediator and dependent variables were significant, and there were no interaction effects between the independent and mediation variable (Baron & Kenny 1986). When we allowed for mediation of the effect of NA on child‐feeding practices through external parental locus of control, the mediation was complete, meaning that the entire effect of NA on child feeding was mediated through external parental locus of control.
The results showed clearly that mothers with external parental locus of control were more likely to both pressure their children to eat and restrict their diets (Fig. 3). The effect of external parental locus of control on restriction and pressure to eat fully accounted for the effect of NA on these two child‐feeding practices (Fig. 3).
Figure 3.
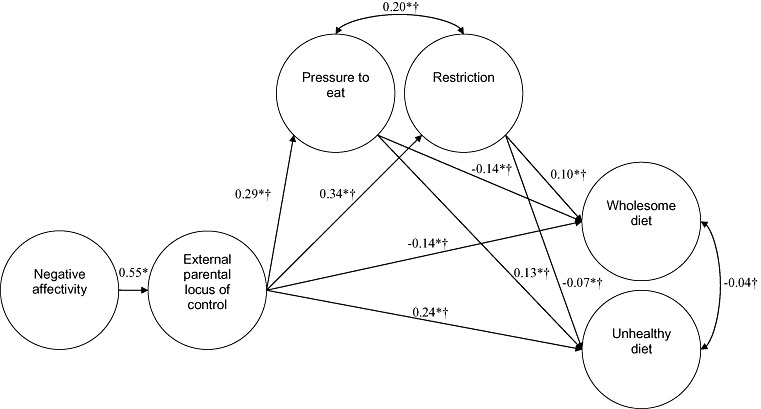
Structural equation model on influences of maternal negative affectivity and external parental locus of control on child‐feeding practices and child diet. One‐headed arrow denotes a regression coefficient, and a two‐headed arrow denotes a residual correlation coefficient. *P < 0.01. †Adjusted for physical and medical variables (results from adjusting variables in Table 3).
An additional finding was that external parental locus of control explained part of the correlation between pressure to eat and restriction (χ2 = 16.61, 1 df).
The demographic and physical variables influenced child‐feeding practices in several ways (see Table 3). The effects of the continuous variables in Table 3– maternal education, age and BMI – are given as incremental change per interval. For example, a 3‐year increase in maternal education should be interpreted as a threefold incremental difference in standard deviation on the dependent variable. With respect to pressuring the child to eat, we found mothers who had more years of education, higher BMI, were older and single were less likely to pressure the child to eat, and homemakers were more likely to pressure the child to eat. With respect to restricting the child's food intake, we found that mothers who had more years of education, were homemakers and had boys were more likely to restrict the child's food intake, and mothers who were older and had higher BMIs were less likely to restrict their child's food intake. External parental locus of control, more years of education and being a homemaker were all strongly associated with pressuring the child to eat. The mothers' level of external parental locus of control was the only strong predictor of restricting the child's food intake.
Table 3.
Regression coefficients for the demographic and physical adjusting variables in the structural equation modeling analysis
| Pressure to eat[Link], [Link] | Restriction[Link], [Link] | Wholesome[Link], [Link] | Unhealthy[Link], [Link] | |
|---|---|---|---|---|
| (Adj. β) | (Adj. β) | (Adj. β) | (Adj. β) | |
| Child gender boy | 0.00 | 0.04 § | −0.08 ¶ | −0.00 |
| Daily smoking | 0.04 | −0.05 | −0.07 § | 0.22 ¶ |
| Education (years) | −0.05 ¶ | 0.02 ¶ | 0.03 ¶ | −0.01 ¶ |
| Homemaker | 0.13 ¶ | 0.08 ¶ | −0.03 | 0.34 ¶ |
| Maternal age (years) | −0.01 ¶ | −0.01 ¶ | 0.02 ¶ | 0.01 ¶ |
| Maternal BMI | −0.01 § | −0.01 ¶ | −0.01 ¶ | 0.01 ¶ |
| Single marital status | −0.08 § | −0.01 | 0.08 | −0.12 ¶ |
*Standardized score. † Adjusted for parental locus of control. ‡ Adjusted for parental locus of control, pressure to eat and restriction. § P < 0.05; ¶ P < 0.01. BMI, body mass index.
Hypothesis 3: effect of NA and parental locus of control on child dietary patterns mediated through child‐feeding practices
We tested the extent of mediation of the effect of NA on the two dietary patterns through external parental locus of control. There was a positive association among NA, external parental locus of control and both dietary patterns, and no interaction effects. When we tested for mediation, the entire effect of NA on both wholesome and unhealthy diet was completely mediated by external parental locus of control.
Likewise, we tested whether the effect of external parental locus of control on diet was mediated through feeding practices. A small portion of the effects of external parental locus of control on both wholesome and unhealthy diet were partially mediated through both pressure to eat and restriction. The indirect effects of NA within the aforementioned mediated effects were also significant. The mediation was only partial, and most of the effect of child‐feeding on child diet was independent of that of external parental locus of control.
In the SEM analysis, mother's level of NA, external parental locus of control and child‐feeding practices were associated with the child's diet (Fig. 3). Mothers who had higher NA scores had a more external parental locus of control, which was associated with both a more unhealthy and a less wholesome diet in the child. Furthermore, only a minor part of the effect of NA and external parental locus of control on diet was mediated through child‐feeding practices (Fig. 3). Mothers with a high level of NA and external parental locus of control were more inclined to both pressure their child to eat and restrict their child's diet (Fig. 3). The children of those mothers were therefore more likely to have a less wholesome and more unhealthy diet due to their mothers' pressuring them to eat, and at the same time more likely to have a more wholesome diet and a less unhealthy diet due to their mothers' restricting their diet. When combined, these two small opposite indirect effects of high NA and external parental locus of control on wholesome diet fully cancel each other out and partially cancel each other out on unhealthy diet.
Demographic and physical variables were associated with the children's diet in several ways (Table 3). Mothers who were regular smokers, had a higher BMI or who had boys were less likely to have children with a wholesome diet. Mothers with more years of education, who were homemakers or older tended to have children with more wholesome diets. Mothers who had more years of education or were single tended not to have children with an unhealthy diet. Mothers who were regular smokers, homemakers, older or had a higher BMI were more likely to have children with an unhealthy diet.
Hypothesis 4: independent effect of child‐feeding practices
Most of the effects of the two control‐oriented child‐feeding practices on diet were independent of NA and external parental locus of control. Mothers who pressured their children to eat had children with a less wholesome and more unhealthy diets (Fig. 3). Restriction had the opposite effect on diet; mothers who restricted their children's diets had children with more wholesome diets and less unhealthy diets.
Discussion
The key findings of this study are as follows: first, the two child dietary patterns identified in the MoBa sample at 18 months after birth were broadly corroborated by being identified again at age 3 years. Unhealthy and wholesome diets were only modestly associated initially and no longer significantly associated after adjusting for other variables. This means that a child's intake of chocolate, chips and soda at 3 years of age is not related to his or her intake of vegetables, fish and fruit, once parental locus of control, control‐oriented child‐feeding practices and the demographic and physical characteristics are taken into account. Second, mothers with high levels of NA were more inclined to restrict their child's diet or to pressure the child to eat, and these behaviours were entirely mediated through external parental locus of control. Moreover, external parental locus of control explained a part of the association between pressure to eat and restriction; mothers' external parental locus of control could therefore be interpreted as a common aetiological factor for both feeding practices. Third, mothers high in NA and high in external parental locus of control were more likely to have a child eating a less wholesome and a more unhealthy diet. Furthermore, the relation of NA and parental locus of control with child diet was partly mediated by the use of the two control‐oriented child‐feeding practices. Fourth, in accordance with our hypotheses, children of mothers that pressured them to eat did not eat more wholesome foods than other children but rather consumed more unhealthy foods. Contrary to our hypotheses, mothers who restricted their children's food intake tended to have a child eating more wholesome diets and less unhealthy diets. The effects of child‐feeding practices were largely independent of NA and external parental locus of control.
Relationships between the demographic and physical variables and children's diets were in accordance with earlier studies of 18‐month‐old and 3‐year‐old children (North & Emmett 2000; Ystrom et al. 2009). Maternal smoking and the mother being a homemaker were substantial risk factors for unhealthy eating in the children.
We assume that mothers high in NA tend to have an external parental locus of control because they tend to negatively perceive their environment, experience little success with parenting and use ineffective strategies when coping with stress (Lovejoy et al. 1997; Vollrath 2001). Perceiving that they have little control over the child's eating behaviour, these mothers may tend to enforce control by using pressure and restriction as feeding strategies (Farrow & Blissett 2005; Blissett & Farrow 2007; Hughes et al. 2008). At the same time, mothers perceiving little control will be less able to cope with the child's demand for sweet and fatty foods and less able to ensure that the child eats a wholesome diet. Lastly, mothers perceiving little control tend to believe that the child is incapable of internal self‐regulation in the feeding situation (Janssens 1994); therefore, it makes sense for them to exert control.
The finding that the association between NA and control‐oriented child feeding was fully mediated through external parental locus of control is not only a replication of Farrow & Blissett (2005), Blissett & Farrow (2007) and Hughes et al. (2008), but also extends prior knowledge by suggesting external parental locus of control as a possible mechanism for the relationship between NA and control‐oriented child feeding.
The finding that pressuring a child to eat is associated with a less wholesome diet and a more unhealthy diet is in line with earlier research (Fisher et al. 2002; Brown et al. 2008). Children that are pressured to eat certain foods are at risk of acquiring an aversion towards just these foods (Fisher et al. 2002). In a similar vein, it has been suggested that the control‐oriented feeding practice of restriction appears to be related to a preference for an unhealthy diet (Fisher & Birch 1999a, 1999b). Our results did not replicate these findings; on the contrary, we found restriction to be associated with the opposite dietary pattern, a more wholesome diet and a less unhealthy diet.
The finding that external parental locus of control partially explained the association between pressure to eat and restriction is novel. The implication here is that if pressure to eat and restriction are conceptualized as caused by a common factor of control‐oriented child feeding, this factor could be confounded by the parent's belief of being in control. This finding is important for both interpretation of results deriving from applications of the Child Feeding Questionnaire and for future construction of child‐feeding concepts and scales.
While pressure to eat has been related to an overt form of control‐oriented child feeding, and is hence perceivable to the child, restriction on the other hand has been described as a covert form of control‐oriented child feeding (Ogden et al. 2006). While the overt form of child feeding has been related to more unhealthy snacking and lower fruit and vegetable intakes in children, the covert form of child feeding relates to less snacking and higher fruit and vegetable intake (Brown et al. 2008). It could be that when a mother attempts to restrict her child's food intake, it is less obvious than pressuring the child to eat, and therefore, the child does not react negatively to the mother's control efforts by becoming averse to wholesome or healthy foods. Another reason might be the young age of the children. They are bound to eat what is made available to them.
There are some limitations to the current study that should be addressed. First, the food frequency questionnaire was limited in the range of foods it asked about, although this probably reflects the fact that 3‐year‐olds have a limited diet. The food types used in the food frequency questionnaire were selected to assess general patterns of food intake, rather than to assess the intake of specific nutritional components. Second, the indirect mediated effect of NA on diet was small. Yet, it was the same size or larger than the effects of some demographic and physical factors commonly deemed important, such as maternal age and maternal BMI. Third, and most importantly, our assessment was, except for maternal NA, all cross‐sectional. This implies that there is a spectrum of alternative structural models that might explain our data equally well. One meaningful alternative model could have posited maternal NA and parental locus of control as correlated rather than causally related predictors. However, the construct of parental locus of control taps a narrow set of beliefs referring to a specific activity – parenting – whereas NA represents a broad, basic trait construct that is causally preceding a plethora of specific beliefs and behaviours. Another meaningful alternative model could have reversed the causal relationship between maternal feeding practices and child diet or even modeled a reciprocal relation between these construct. However, only more fine‐grained longitudinal assessments would permit a more conclusive resolution of the causal relation between feeding practices and child diet.
In spite of these limitations, we believe that our findings are interesting and can serve as a starting point for future elaborative studies. For instance, because external parental locus of control partially explained the association between pressure to eat and restriction, future studies should investigate the role of personality and parenting in explaining the covariation between child‐feeding practices. Moreover, because the effect of external parental locus of control on diet was largely independent of the two control‐oriented child‐feeding practices, future research ought to assess a range of child‐feeding practices and aspects of parenting other than those directly related to feeding. There may be other mechanisms by which parental perceptions of control are affecting their children's diets. Furthermore, a full spectrum or personality traits should be included to relate both child feeding and diet to different forms of personality‐related motivation and stress coping (Vollrath 2001). Finally, our study, utilizing a large population‐wide cohort sample and adjusting for a range of factors, did not replicate the link between restriction in child feeding and unhealthy child diet, but moreover identified an inverse link. Future population‐based studies should reinvestigate this link.
Source of funding
Norwegian Institute of Public health was the sole source of funding.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Supporting information
Appendix S1. Standardized factor loadings for the measurement models. 6, 18 and 36 denote time points in months after birth.
Please note: Wiley‐Blackwell are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
Supporting info item
Acknowledgements
We would like to thank Karina Corbett and Ellen Russon for proofreading the manuscript.
References
- Baron R.M. & Kenny D.A. (1986) The moderator‐mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology 51, 1173–1182. [DOI] [PubMed] [Google Scholar]
- Birch L.L., McPhee L., Shoba B.C., Pirok E. & Steinberg L. (1987) What kind of exposure reduces children's food neophobia? Looking vs. tasting. Appetite 9, 171–178. [DOI] [PubMed] [Google Scholar]
- Birch L.L., Fisher J.O., Grimm‐Thomas K., Markey C.N., Sawyer R. & Johnson S.L. (2001) Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 36, 201–210. [DOI] [PubMed] [Google Scholar]
- Blissett J. & Farrow C. (2007) Predictors of maternal control of feeding at 1 and 2 years of age. International Journal of Obesity 31, 1520–1526. [DOI] [PubMed] [Google Scholar]
- Brown K.A., Ogden J., Vogele C. & Gibson E.L. (2008) The role of parental control practices in explaining children's diet and BMI. Appetite 50, 252–259. [DOI] [PubMed] [Google Scholar]
- Browne M.W. (2001) An overview of analytic rotation in exploratory factor analysis. Multivariate Behavioral Research 36, 111–150. [Google Scholar]
- Campis L.K., Lyman R.D. & Prentice‐Dunn S. (1986) The Parental Locus of Control Scale: development and validation. Journal of Clinical Child Psychology 15, 260–267. [Google Scholar]
- Clark L.A. & Watson D. (1999) ‘Temperament: a new paradigm for trait psychology,’. In Handbook of Personality: Theory and Research (eds Pervin L.A. & John O.P.), 2nd edn, pp. 399–423. Guilford Press: New York. [Google Scholar]
- Farrow C.V. & Blissett J.M. (2005) Is maternal psychopathology related to obesigenic feeding practices at 1 year?. Obesity Research 13, 1999–2005. [DOI] [PubMed] [Google Scholar]
- Fisher J.O. & Birch L.L. (1999a) Restricting access to foods and children's eating. Appetite 32, 405–419. [DOI] [PubMed] [Google Scholar]
- Fisher J.O. & Birch L.L. (1999b) Restricting access to palatable foods affects children's behavioral response, food selection, and intake. American Journal of Clinical Nutrition 69, 1264–1272. [DOI] [PubMed] [Google Scholar]
- Fisher J.O., Mitchell D.C., Smiciklas‐Wright H. & Birch L.L. (2002) Parental influences on young girls' fruit and vegetable, micronutrient, and fat intakes. Journal of the American Dietetic Association 102, 58–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flora D.B. & Curran P.J. (2004) An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods 9, 466–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill A.J. (2002) Developmental issues in attitudes to food and diet. The Proceedings of the Nutrition Society 61, 259–266. [DOI] [PubMed] [Google Scholar]
- Hu L.T. & Bentler P.M. (1998) Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychological Methods 3, 424–453. [Google Scholar]
- Hughes S.O., Shewchuk R.M., Baskin M.L., Nicklas T.A. & Qu H.Y. (2008) Indulgent feeding style and children's weight status in preschool. Journal of Developmental and Behavioral Pediatrics 29, 403–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irgens L.M. (2000) The Medical Birth Registry of Norway. Epidemiological research and surveillance throughout 30 years. Acta Obstetricia Et Gynecologica Scandinavica 79, 435–439. [PubMed] [Google Scholar]
- Izard C.E., Libero D.Z., Putnam P. & Haynes O.M. (1993) Stability of emotion experiences and their relations to traits of personality. Journal of Personality and Social Psychology 64, 847–860. [DOI] [PubMed] [Google Scholar]
- Janssens J.M.A.M. (1994) Authoritarian child‐rearing, parental locus of control, and the childs behavior style. International Journal of Behavioral Development 17, 485–501. [Google Scholar]
- Lovejoy M.C., Verda M.R. & Hays C.E. (1997) Convergent and discriminant validity of measures of parenting efficacy and control. Journal of Clinical Child Psychology 26, 366–376. [DOI] [PubMed] [Google Scholar]
- Magnus P. (2007) The Norwegian Mother and Child Cohort Study (MoBa) – new research possibilities. Norwegian Journal of Epidemiology 17, 107–110. [Google Scholar]
- Magnus P., Irgens L.M., Haug K., Nystad W., Stoltenberg C. & The MoBa Study Group (2006) The Norwegian Mother and Child Cohort Study. International Journal of Epidemiology 35, 1146–1150. [DOI] [PubMed] [Google Scholar]
- Metsapelto R.L. & Pulkkinen L. (2003) Personality traits and parenting: neuroticism, extraversion, and openness to experience as discriminative factors. European Journal of Personality 17, 59–78. [Google Scholar]
- North K. & Emmett P. (2000) Multivariate analysis of diet among three‐year‐old children and associations with socio‐demographic characteristics. European Journal of Clinical Nutrition 54, 73–80. [DOI] [PubMed] [Google Scholar]
- Ogden J., Reynolds R. & Smith A. (2006) Expanding the concept of parental control: a role for overt and covert control in children's snacking behaviour? Appetite 47, 100–106. [DOI] [PubMed] [Google Scholar]
- Patrick H., Nicklas T.A., Hughes S.O. & Morales M. (2005) The benefits of authoritative feeding style: caregiver feeding styles and children's food consumption patterns. Appetite 44, 243–249. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. (1989) Society and the adolescent self‐image, Rev. Wesleyan University Press: Middletown, CT. [Google Scholar]
- Strand B.H., Dalgard O.S., Tambs K. & Rognerud M. (2003) Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL‐25, SCL‐10, SCL‐5 and MHI‐5 (SF‐36). Nordic Journal of Psychiatry 57, 113–118. [DOI] [PubMed] [Google Scholar]
- Vollrath M. (2001) Personality and stress. Scandinavian Journal of Psychology 42, 335–347. [DOI] [PubMed] [Google Scholar]
- Wang Y. & Lobstein T. (2006) Worldwide trends in childhood overweight and obesity. International Journal of Pediatric Obesity 1, 11–25. [DOI] [PubMed] [Google Scholar]
- Watson D. & Clark L.A. (1984) Negative affectivity: the disposition to experience aversive emotional states. Psychological Bulletin 96, 465–490. [PubMed] [Google Scholar]
- Ystrom E., Niegel S., Klepp K.‐I. & Vollrath M.E. (2008) The impact of maternal negative affectivity and general self‐efficacy on breast‐feeding: the Norwegian Mother and Child Cohort Study. Journal of Pediatrics 152, 68–72. [DOI] [PubMed] [Google Scholar]
- Ystrom E., Niegel S. & Vollrath M.E. (2009) The impact of maternal negative affectivity on dietary patterns of 18‐month‐old children in the Norwegian Mother and Child Cohort Study. Maternal and Child Nutrition 5, 234–242. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Standardized factor loadings for the measurement models. 6, 18 and 36 denote time points in months after birth.
Please note: Wiley‐Blackwell are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
Supporting info item