

Abstract
Background
Early dental decay or demineralised lesions (DLs, also known as white spot lesions) can appear on teeth during fixed orthodontic (brace) treatment. Fluoride reduces decay in susceptible individuals, including orthodontic patients. This review compared various forms of topical fluoride to prevent the development of DLs during orthodontic treatment. This is the second update of the Cochrane Review first published in 2004 and previously updated in 2013.
Objectives
The primary objective was to evaluate whether topical fluoride reduces the proportion of orthodontic patients with new DLs after fixed appliances.
The secondary objectives were to examine the effectiveness of different modes of topical fluoride delivery in reducing the proportions of orthodontic patients with new DLs, as well as the severity of lesions, in terms of number, size and colour. Participant‐assessed outcomes, such as perception of DLs, and oral health‐related quality of life data were to be included, as would reports of adverse effects.
Search methods
Cochrane Oral Health's Information Specialist searched the following databases: Cochrane Oral Health's Trials Register (to 1 February 2019), the Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 1) in the Cochrane Library (searched 1 February 2019), MEDLINE Ovid (1946 to 1 February 2019), and Embase Ovid (1980 to 1 February 2019). The US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the World Health Organization International Clinical Trials Registry Platform were searched for ongoing trials. No restrictions were placed on the language or date of publication when searching the electronic databases.
Selection criteria
Parallel‐group, randomised controlled trials comparing the use of a fluoride‐containing product versus a placebo, no treatment or a different type of fluoride treatment, in which the outcome of enamel demineralisation was assessed at the start and at the end of orthodontic treatment.
Data collection and analysis
At least two review authors independently, in duplicate, conducted risk of bias assessments and extracted data. Authors of trials were contacted to obtain missing data or to ask for clarification of aspects of trial methodology. Cochrane's statistical guidelines were followed.
Main results
This update includes 10 studies and contains data from nine studies, comparing eight interventions, involving 1798 randomised participants (1580 analysed). One report contained insufficient information and the authors have been contacted.
We assessed two studies as at low risk of bias, six at unclear risk of bias, and two at high risk of bias.
Two placebo (non‐fluoride) controlled studies, at low risk of bias, investigated the professional application of varnish (7700 or 10,000 parts per million (ppm) fluoride (F)), every six weeks and found insufficient evidence of a difference regarding its effectiveness in preventing new DLs (risk ratio (RR) 0.52, 95% confidence interval (CI) 0.14 to 1.93; 405 participants; low‐certainty evidence). One placebo (non‐fluoride) controlled study, at unclear risk of bias, provides a low level of certainty that fluoride foam (12,300 ppm F), professionally applied every two months, may reduce the incidence of new DLs (12% versus 49%) after fixed orthodontic treatment (RR 0.26, 95% CI 0.11 to 0.57; 95 participants).
One study, at unclear risk of bias, also provides a low level of certainty that use of a high‐concentration fluoride toothpaste (5000 ppm F) by patients may reduce the incidence of new DLs (18% versus 27%) compared with a conventional fluoride toothpaste (1450 ppm F) (RR 0.68, 95% CI 0.46 to 1.00; 380 participants).
There was no evidence for a difference in the proportions of orthodontic patients with new DLs on the teeth after treatment with fixed orthodontic appliances for the following comparisons: ‐ an amine fluoride and stannous fluoride toothpaste/mouthrinse combination versus a sodium fluoride toothpaste/mouthrinse, ‐ an amine fluoride gel versus a non‐fluoride placebo applied by participants at home once a week and by professional application every three months, ‐ resin‐modified glass ionomer cement versus light‐cured composite resin for bonding orthodontic brackets, ‐ a 250 ppm F mouthrinse versus 0 ppm F placebo mouthrinse, ‐ the use of an intraoral fluoride‐releasing glass bead device attached to the brace versus a daily fluoride mouthrinse.
The last two comparisons involved studies that were assessed at high risk of bias, because a substantial number of participants were lost to follow‐up.
Unfortunately, although the internal validity and hence the quality of the studies has improved since the first version of the review, they have compared different interventions; therefore, the findings are only considered to provide low level of certainty, because none has been replicated by follow‐up studies, in different settings, to confirm external validity.
A patient‐reported outcome, such as concern about the aesthetics of any DLs, was still not included as an outcome in any study. Reports of adverse effects from topical fluoride applications were rare and unlikely to be significant. One study involving fluoride‐containing glass beads reported numerous breakages.
Authors' conclusions
This review found a low level of certainty that 12,300 ppm F foam applied by a professional every 6 to 8 weeks throughout fixed orthodontic treatment, might be effective in reducing the proportion of orthodontic patients with new DLs. In addition, there is a low level of certainty that the patient use of a high fluoride toothpaste (5000 ppm F) throughout orthodontic treatment, might be more effective than a conventional fluoride toothpaste. These two comparisons were based on single studies. There was insufficient evidence of a difference regarding the professional application of fluoride varnish (7700 or 10,000 ppm F). Further adequately powered, randomised controlled trials are required to increase the certainty of these findings and to determine the best means of preventing DLs in patients undergoing fixed orthodontic treatment. The most accurate means of assessing adherence with the use of fluoride products by patients and any possible adverse effects also need to be considered. Future studies should follow up participants beyond the end of orthodontic treatment to determine the effect of DLs on patient satisfaction with treatment.
Plain language summary
Fluorides for preventing early tooth decay (demineralised lesions) during fixed brace treatment
Review question Ugly white or brown marks sometimes appear on the teeth during treatment with braces to straighten teeth. These are due to early tooth decay and usually occur with fixed, glued‐on 'train track', braces, which make it more difficult to clean the teeth.
We know that fluoride in toothpaste helps to prevent tooth decay and think that if extra fluoride is given to people wearing fixed braces, it will protect them from getting these marks. The aim of this Cochrane Oral Health's review was to look at how well fluorides help to prevent early tooth decay during fixed brace treatment and to find out the best way to get fluoride to the teeth.
Background Wearing a fixed brace makes it harder for people to keep their teeth clean and may also cause pain. Pain can make it more difficult for people to brush their teeth. This can lead to a build‐up of dental plaque around the brackets that attach the fixed brace to the teeth, and if the plaque stays on the tooth for long enough, it will cause early tooth decay, which looks like white or brown marks (demineralised lesions, also known as white spot lesions). People often wear braces for 18 months or longer and if the decay is left to progress, it can cause holes, which are sometimes bad enough to need fillings to be done in the teeth.
Fluoride helps the tooth to heal, reducing tooth decay in people who are at risk of developing it. People receiving fixed brace treatment may be given different forms of fluoride treatment. It is important to think about how the fluoride gets to the teeth. Does the fluoride need to be placed by a dentist or dental nurse, or can people having treatment with braces apply the fluoride to their own teeth?
Study characteristics This review is up‐to‐date as of 1 February 2019. The review includes 10 studies but we could only use the information from nine studies involving 1798 randomised people. We have asked for more information about one study. The review looks at eight different ways of applying fluoride to the teeth. People taking part in the studies were all having treatment with fixed braces. The number of people with new decay on the teeth at end of fixed brace treatment, as well as the amount of decay in each person, were measured and counted.
We compared the following treatments: ‐ dentist or nurse‐applied fluoride e.g. varnish, gel or foam, ‐ patient‐applied/used fluoride e.g. toothpaste, mouthwash, gel or foam, and ‐ materials that release fluoride over time e.g. glues, elastic bands.
Key results One study showed that when the dentist applies a foam with a high level of fluoride in it onto the teeth every time the patient is seen, this might reduce the risk of new decay. Another study found that if patients use a toothpaste with a higher level of fluoride than normal, then this might also reduce the risk of new marks on their teeth.
No studies have shown that other ways of giving the teeth extra fluoride reduced the number and/or size of new decay on teeth in people wearing fixed braces. Harmful effects of the different ways of giving the teeth more fluoride were not reported in any of the included studies.
Certainty of the evidence The level of belief we have in these findings is low, due to the lack of studies testing the same fluorides and showing the same results. We suggest that more, well‐conducted studies should be done in this area.
Summary of findings
Background
Description of the condition
During orthodontic treatment with fixed appliances, brackets are attached to the teeth to hold the wires that provide the forces to straighten the teeth. One of the adverse effects of fixed braces is that dental plaque collects around the attachments, leading to accumulation of the types of bacteria that cause dental disease (Naranjo 2006). Build‐up of dental plaque around orthodontic brackets is associated with increased risk of demineralised lesions (DLs, also known as white spot lesions), which can be visible within six months (Tufekci 2011). Demineralisation is an early, but reversible, stage in the development of dental decay (caries). Cariogenic bacteria present in the dental plaque change sugar in the diet into organic acids, which start to damage the tooth enamel. Effective removal of plaque will prevent DLs from occurring; however, the presence of orthodontic appliances in the mouth and associated dental pain may make it more difficult for individuals to adequately clean their teeth and braces. DLs developing on the labial and buccal surfaces of teeth during orthodontic treatment can become a significant problem over the course of treatment, which may last for 18 months or longer, resulting in a poor appearance of the teeth following straightening (Maxfield 2012). In severe cases the caries can make a hole in the tooth that will require a filling (restoration), which may be both painful and costly.
Enaia and colleagues (Enaia 2011) used clinical photographs of the teeth taken before and after fixed brace treatment to show that whereas 32% of people in their study had DLs before the brace was fitted, this rose to 74% after their braces had been taken off. Most of the DLs were minor, but a significant minority of participants (10%) had holes in their teeth, which may have required a filling. Although DLs tend to fade with time as they heal, one study has shown that, even five years after treatment, a significant proportion of people who had worn fixed braces showed some evidence of DLs caused by the braces compared with a control group of people who had not had a fixed brace (Ogaard 1989).
Description of the intervention
Orthodontists are keen to prevent the development of DLs so their patients may have the best possible appearance after orthodontic treatment ‐ straight teeth with no marks. Fluoride is important in the prevention of dental decay (ten Cate 2013). Marinho and colleagues (Marinho 2016) found a definite reduction in dental decay in children and adolescents who performed regular supervised rinsing with a fluoride mouthwash. It has also been shown that fluoride may reduce the number of DLs that develop during brace treatment. When orthodontic participants used a mouthrinse, Geiger et al (Geiger 1992) found a 30% reduction in the number of participants with DLs and a 25% reduction in the incidence of teeth affected by DLs. Many orthodontists recommend the use of a daily fluoride mouthrinse throughout brace treatment to prevent DLs (Kerbusch 2012).
Several methods (in addition to fluoridated toothpaste) are used to deliver fluoride to teeth in patients during orthodontic treatment. These include the following:
topical fluorides (e.g. mouthrinse, gel, varnish or foam) that are applied by the dentist or nurse when the orthodontic patient is seen to adjust their brace;
topical fluorides (e.g. toothpaste, mouthrinse, gel or foam) that the orthodontic patient can apply themselves at home;
fluoride‐releasing materials (e.g. glues used to bond the brackets onto the teeth and orthodontic elastics that are impregnated with fluoride);
dietary fluoride supplementation (e.g. fluoridated milk).
How the intervention might work
Fluoride present in the mouth reduces caries development via three mechanisms: inhibition of the demineralisation of dental enamel, enhancement of the remineralisation of dental enamel producing a remineralised layer that is resistant to acid attack, and inhibition of the bacterial enzymes that produce the acid (Lynch 2006; ten Cate 2013).
Most children undergoing orthodontic treatment will be exposed to some fluoride ‐ low concentrations in the water supply, higher concentrations from fluoridated toothpaste, or both. Use of other topical fluorides or fluoride sources designed to deliver additional fluoride to the at‐risk area, or both, near orthodontic brackets, are likely to further reduce the risk of DL development. Topical fluorides include fluoride toothpastes, mouthrinses, gels, varnishes and dietary sources (e.g. fluoridated milk). Specific orthodontic sources of fluoride include bracket adhesives and orthodontic elastic bands (elastomeric ligatures), which slowly release fluoride into the mouth. All of these fluoride sources release fluoride into saliva that is distributed throughout the mouth.
Why it is important to do this review
Several systematic reviews have concluded that the use of topical fluoride in various forms reduce the prevalence and incidence of dental caries in children and adolescents (Marinho 2003a; Marinho 2003b; Marinho 2004; Marinho 2016). Orthodontists have, therefore, routinely recommended the use of topical fluoride mouthrinses to their patients wearing fixed appliances or apply fluoride in the form of varnish, gel or foam to reduce the risk of orthodontic patients developing dental caries. Others use fluoride‐releasing materials to attach the brackets or bands to the teeth. Clear evidence is lacking, regarding the optimum concentration of topical fluoride, the optimum frequency of use and the effects of topical fluorides and fluoride‐releasing materials over the whole length of orthodontic treatment.
This Cochrane Review was first published in 2004 (Benson 2004). It was updated in 2013 with an amended protocol to only include appropriately designed randomised studies, using parallel groups and measuring relevant outcomes over the full length of orthodontic treatment (Benson 2013). This is the second update.
Objectives
The primary objective of this review was to evaluate whether topical fluoride reduces the proportion of orthodontic patients with new demineralised lesions (DLs) after fixed appliances.
The secondary objectives were to examine the effectiveness of different modes of fluoride delivery in reducing the proportions of orthodontic patients with new DLs, as well as the severity of lesions, in terms of number, size and colour. Participant‐assessed outcomes, such as perception of DLs, and oral health‐related quality of life data were to be included, as would reports of adverse effects.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) in which fluoride was delivered by any method to prevent the development of new enamel demineralised lesions (DLs) during fixed orthodontic treatment. As topical fluorides are distributed throughout the mouth by saliva, the use of a within‐person or split‐mouth study design to evaluate these interventions is inappropriate, due to potential carry‐across effects (Pandis 2013) and any study using this design was excluded. Studies involving multiple arms would be examined and only comparisons between two fluoride interventions or fluoride versus no fluoride interventions would be included in the pairwise analysis.
Types of participants
Included were participants of any age who had orthodontic treatment with fixed braces in situations where DLs were assessed on teeth remaining in the mouth at the end of orthodontic treatment (at debonding, immediately after the active fixed brace is removed). We excluded studies that evaluated demineralisation of extracted teeth (ex vivo) or that were undertaken over short periods of time i.e. less than the whole time the fixed brace was in the mouth.
Types of interventions
Topical fluoride in the form of toothpaste, mouthrinse, gel, varnish, foam or dietary sources at any dose, frequency, duration or method of administration, and with any of the following active agents/ingredients: NaF (sodium fluoride), SMFP (sodium monofluorophosphate), SnF (stannous fluoride), APF (acidulated phosphate fluoride) and amine F (amine fluoride) applied either by a professional in the dental surgery or office, or used by the patient at home.
Materials containing fluoride that is potentially released during treatment, including fluoride‐releasing composite resin‐bonding materials, compomers, glass ionomer cements and resin‐modified glass ionomers for bonding or banding, slow‐release fluoride beads/devices and fluoride‐releasing elastomeric ligatures.
The control group comprising of individuals not subjected to the fluoride intervention, but instead treated with a placebo, such as a non‐fluoride toothpaste and mouthrinse, or given no intervention. Studies involving a control subjected to an alternative fluoride intervention were also included.
Types of outcome measures
Primary outcomes
The primary outcome was the difference in the proportion of participants in the experimental and comparison groups with new DLs on the day the fixed appliance was removed.This could be assessed directly from the participant (clinically) or preferably from start and finish photographs or fluorescent images of the teeth immediately after the active fixed brace was removed. If the number of DLs was not recorded at the start of treatment, the outcome was the presence or absence of DLs at the end of orthodontic treatment, again assessed directly from the participant or indirectly from photographs or fluorescent images of the teeth. It is important that the assessment was carried out on the day the appliance was removed (or as close to this as possible), because the white marks will tend to heal (remineralise) after the brace is removed. The rate at which the DLs remineralise can be variable between individuals and is another potential confounding factor.
Secondary outcomes
Differences in the severity of the new DLs, as assessed by number, size and colour between experimental and control groups at the end of orthodontic treatment.
Any quantitative assessment of enamel mineral loss, such as fluorescent light techniques or microradiography, used with in situ caries models (Benson 2010) at the end of treatment.
Any participant‐assessed outcomes, such as perception of DLs and oral health‐related quality of life data.
Adverse effects.
Search methods for identification of studies
Electronic searches
Cochrane Oral Health's Information Specialist conducted systematic searches in the following databases for randomised controlled trials and controlled clinical trials. There were no language, publication year or publication status restrictions:
Cochrane Oral Health's Trials Register (searched 1 February 2019) (Appendix 1);
Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 1) in the Cochrane Library (searched 1 February 2019) (Appendix 2);
MEDLINE Ovid (1946 to 1 February 2019) (Appendix 3);
Embase Ovid (1980 to 1 February 2019) (Appendix 4).
Subject strategies were modelled on the search strategy designed for MEDLINE Ovid. Where appropriate, they were combined with subject strategy adaptations of the highly sensitive search strategy designed by Cochrane for identifying randomised controlled trials and controlled clinical trials as described in the Cochrane Handbook for Systematic Reviews of Interventions Chapter 6 (Lefebvre 2011).
Searching other resources
The following trial registries were searched for ongoing studies (see Appendix 5 for details of the search terms used):
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (clinicaltrials.gov; searched 1 February 2019);
World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch; searched 1 February 2019).
We searched the reference lists of included studies and relevant systematic reviews for further studies.
We checked that none of the included studies in this review were retracted due to error or fraud.
We did not perform a separate search for adverse effects of interventions used, we considered adverse effects described in included studies only.
Data collection and analysis
Selection of studies
The search was designed to be sensitive and include controlled clinical trials, these were filtered out early in the selection process if they were not randomised.
Two review authors independently examined the title, keywords and abstract of reports identified through electronic searching for evidence of three criteria.
A randomised clinical trial of participants undergoing orthodontic treatment with fixed appliances.
A trial comparing the use of a fluoride‐containing product versus a non‐fluoride control or an alternative fluoride product.
A trial that assessed the prevalence or incidence of DLs either at the start and at the end of orthodontic treatment or just at the end of treatment, where the end was defined as the day of removal of the fixed appliance or as soon as possible thereafter.
For studies that appeared to meet the inclusion criteria, or for which data in the title and abstract were insufficient to allow a clear decision, the full report was obtained. We resolved disagreements by discussion.
No language restrictions were applied. Translations of foreign language articles were produced by contacts within Cochrane Oral Health.
Data extraction and management
Two review authors extracted data independently, in duplicate, using specially designed data extraction forms. The data extraction forms were piloted on several papers and were modified as required before use. Any disagreement was discussed, and a third review author was consulted when necessary. We contacted all study authors for clarification of missing information. Data from studies in which the reporting was incomplete were not included in the analysis until the corresponding author of the study had supplied adequate clarification. If agreement could not be reached, data were excluded from the review. All studies that met the inclusion criteria underwent an assessment of the risk of bias. We extracted data from the published report; however if the report was unclear or lacking in important information then the corresponding author of the article was contacted by e‐mail. We recorded studies rejected at this or subsequent stages, along with reasons for exclusion, in the 'Characteristics of excluded studies' tables.
For each trial, we recorded the following data.
Year of publication and country of origin.
Study design.
Unit of randomisation.
Details of participants, including demographic characteristics and criteria for inclusion.
Details of types of interventions (method of delivery of fluoride, dose, duration of use).
Details of outcomes reported (number, size and severity of DLs), including method of assessment and mean duration of the study.
Assessment of risk of bias in included studies
This assessment was conducted by using the recommended approach for assessing risk of bias in studies included in Cochrane Reviews (Higgins 2011). We used the two‐part tool to address the six specific domains (namely, sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other bias). Each domain includes one or more specific entries in a 'Risk of bias' table. Within each entry, the first part of the tool involves describing what was reported to have happened in the study. The second part of the tool involves assigning a judgement relating to the risk of bias for that entry: either low risk, unclear risk or high risk.
The domains of sequence generation, allocation concealment, incomplete outcome data and selective outcome reporting are addressed in the tool by a single entry for each study. For blinding, two entries were used because assessments need to be made separately for (1) participants and operators/orthodontists and (2) outcome assessors. When the operator/orthodontist assessed the outcome of the trial, this was noted. The final domain ('other sources of bias') was assessed as a single entry for studies as a whole.
Two review authors undertook the risk of bias assessment independently and in duplicate as part of the data extraction process. We resolved disagreements by discussion.
After taking into account additional information provided by the authors of the trials, review authors grouped studies into the following categories.
| Risk of bias | Interpretation | Within a study | Across studies |
| Low risk of bias | Plausible bias unlikely to seriously alter the results | Low risk of bias for all key domains | Most information comes from studies at low risk of bias |
| Unclear risk of bias | Plausible bias that raises some doubt about the results | Unclear risk of bias for one or more key domains | Most information comes from studies at low or unclear risk of bias |
| High risk of bias | Plausible bias that seriously weakens confidence in the results | High risk of bias for one or more key domains | The proportion of information from studies at high risk of bias is sufficient to affect the interpretation of results |
We completed a 'Risk of bias' table for each included study. We also presented the results graphically (Figure 1).
1.
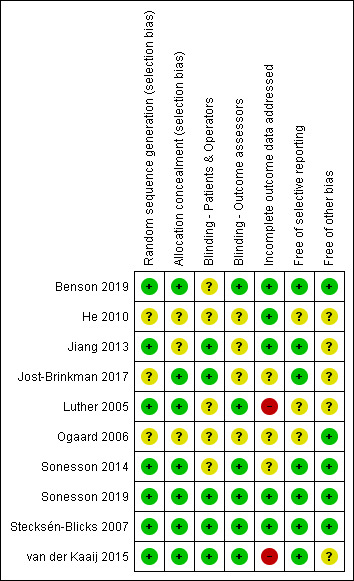
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Measures of treatment effect
For dichotomous outcomes, we expressed the estimate of effect of an intervention as risk ratios (RRs) together with 95% confidence intervals (CIs). For continuous outcomes, we estimated mean differences (MDs) and 95% CIs.
Unit of analysis issues
In parallel‐group trials in which participants are randomly assigned to intervention or to control and a single outcome measure per participant is reported, the analysis is straightforward. When individuals are randomly assigned to treatment, each individual has a number of teeth exposed to the intervention or to the control. When the outcome is reported per number of teeth, the data should be adjusted for clustering within the mouth of each individual to avoid unit of analysis errors. If it was unclear from the reports of included trials whether clustering had been considered, authors were contacted to clarify how this dependence had been accounted for in the analysis.
Dealing with missing data
When data were not available in the printed report, or when data were unclear, we contacted the corresponding author of the study to obtain the missing data. The analysis generally includes only available data (ignoring missing data); we would, however, have used methods of estimating missing standard deviations as provided in Section 7.7.3 of theCochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), if appropriate. Otherwise, we did not undertake any imputations or use statistical methods to allow for missing data.
Assessment of heterogeneity
Pooling of data and meta‐analysis were carried out only if sufficient similarities were noted between studies in types of participants, interventions and outcomes, including the time of the outcome measurement. If any trials were pooled, the significance of discrepancies in the estimates of treatment effects from the different trials was to be assessed by using Cochran's test for heterogeneity, by which heterogeneity was considered significant if P < 0.1 (Higgins 2011).
The I2 statistic, which describes the percentage total variation across studies that is due to heterogeneity rather than to chance, was used to quantify heterogeneity, with I2 greater than 50% considered to show substantial heterogeneity (Higgins 2011: Section 9.5.2).
Assessment of reporting biases
Only a proportion of research projects conducted are ultimately published in an indexed journal and become easily identifiable for inclusion in systematic reviews. Reporting biases arise when reporting of research findings is influenced by the nature and direction of the findings of the research. We investigated and attempted to minimise in this review potential reporting biases, including publication bias, time lag bias, multiple (duplicate) publication bias and language bias.
If more than ten studies were included for one outcome, we would have constructed a funnel plot. Any asymmetry in the funnel plot indicating possible publication bias would have been investigated by statistical analysis using the methods introduced by Egger 1997 (continuous outcome) and Rücker 2008 (dichotomous outcome) (such analysis would have been done in STATA 11.0). However, insufficient trials were included in this review to enable the review authors to investigate publication bias.
Data synthesis
A meta‐analysis was to be conducted only if studies of similar comparisons reported the same outcome measures. Risk ratios would have been combined for dichotomous data and mean differences for continuous data, using random‐effects models, provided more than three studies were included in the meta‐analysis.
Subgroup analysis and investigation of heterogeneity
We planned to investigate clinical heterogeneity by examining the different sources of fluoride. Provided sufficient studies were identified for each intervention and outcome, we planned a priori to conduct subgroup analyses for different sources of fluoride (mouthrinse, gel, varnish dentifrice, bracket adhesive, elastomeric ligature).
Sensitivity analysis
It was planned to undertake sensitivity analyses to examine the effects of quality assessment items on the assessment of overall estimates of effect. In addition, the effect on findings of the review of including unpublished literature was to be examined. However, insufficient trials were included in the review for a sensitivity analysis to be undertaken.
Summary of findings
We developed 'Summary of findings' tables for the comparisons that were considered most important for decision makers and the outcomes number of participants with new DLs on the day the fixed appliance was removed, number of participants with more severe DLs, and number of participants with adverse effects using GRADEpro GDT software (GRADEpro GDT 2015). We assessed the level of certainty in the findings with reference to the risk of bias assessments, the directness of the evidence, the inconsistency of the results, the precision of the estimates, and the risk of publication bias. The level of certainty for each of the comparisons was categorised as high, moderate, low, or very low.
Results
Description of studies
Results of the search
Searches were originally done in July 2003, then repeated in May 2012, January 2013, December 2016, January 2018 and February 2019.
The first version of this review included 14 trials, involving 613 participants. The review protocol was amended for the 2013 update to include only randomised studies (excluding quasi‐randomised or controlled clinical trials), using parallel groups and measuring relevant outcomes over the full length of orthodontic treatment. This resulted in the exclusion of all included studies from the first version, for the following reasons: five were quasi‐randomised (Banks 2000; Dyer 1982; Hirschfield 1978; Millett 2000; Sonis 1989), five were within‐person or split‐mouth designs (Chung 1998; Czochrowska 1998; Gillgrass 2001; Marcusson 1997; Twetman 1997) and three had ex vivo outcomes on extracted teeth (Gorton 2003; Ogaard 1986; Pascotto 2004). Ogaard 2001 was excluded because investigators compared fluoride versus fluoride plus an antiseptic solution.
The 2013 update included three studies (Luther 2005; Ogaard 2006; Stecksén‐Blicks 2007), involving 458 randomised participants (391 analysed). For the 2019 update a further seven studies were identified for inclusion (Benson 2019; He 2010; Jiang 2013; Jost‐Brinkman 2017; Sonesson 2014; Sonesson 2019; van der Kaaij 2015). Three ongoing studies were also identified (DRKS00012533; DRKS00012540; IRCT2016122531558N1).
For details of the studies examined and reasons for inclusion or exclusion, please see Characteristics of included studies and Characteristics of excluded studies tables. The search process and results are presented as a flow chart in Figure 2.
2.
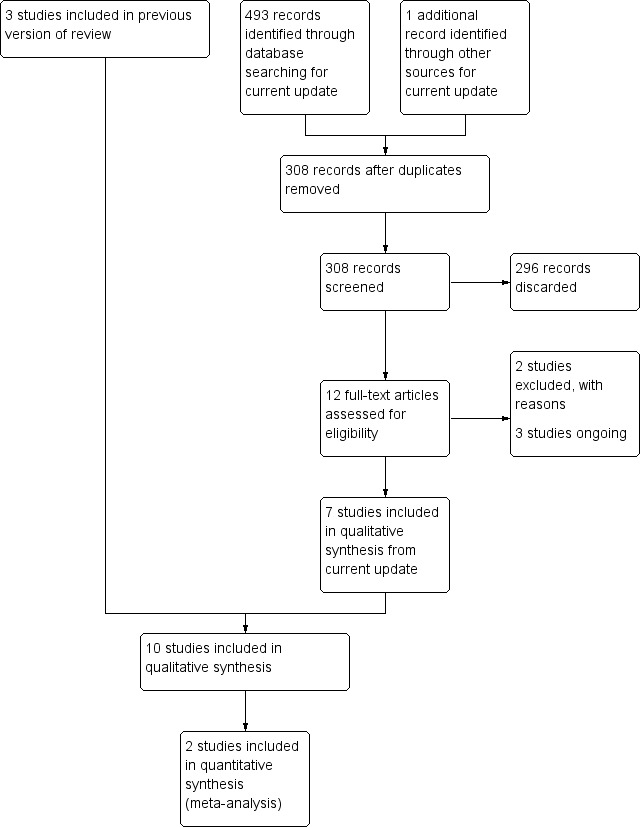
Study flow diagram.
Included studies
Characteristics of the trial participants and settings
Seven of the included studies were conducted in Europe, involving Sweden (Ogaard 2006; Sonesson 2014; Sonesson 2019; Stecksén‐Blicks 2007), the UK (Luther 2005), the UK and Republic of Ireland (Benson 2019), and the Netherlands (van der Kaaij 2015). One study was undertaken in Germany and Israel (Jost‐Brinkman 2017) and two in China (He 2010; Jiang 2013). Participant age ranged from 10 years at the start of treatment (Jost‐Brinkman 2017) to 60 years (Jost‐Brinkman 2017). All participants in the included trials were recruited at the start of their orthodontic treatment with fixed appliances and were followed until their fixed appliances were removed.
Characteristics of the interventions
We have grouped the included trials into three broad comparisons.
Dentist or nurse‐applied fluoride in the form of varnish (He 2010; Sonesson 2019; Stecksén‐Blicks 2007), foam (Jiang 2013), and gel (Jost‐Brinkman 2017), both home use once a week and professional application every three months.
Patient‐applied/used fluoride in the form of toothpaste/mouthrinse combinations (Ogaard 2006; Sonesson 2014; van der Kaaij 2015).
Fluoride‐releasing materials in the form of intraoral fluoride‐releasing glass beads device (Luther 2005) and resin‐modified glass ionomer cement for bonding orthodontic brackets (Benson 2019).
One study (Jost‐Brinkman 2017) investigated both a dentist/nurse‐applied and a patient‐applied fluoride intervention in the same participants. Adherence to home use is more difficult to assess than adherence to dentist or nurse‐applied therefore it was categorised in the latter. There were no studies investigating dietary fluoride supplementation.
Five studies were placebo‐controlled, comparing a fluoride‐containing product with the same product not containing fluoride, where participant, clinician/operator and assessor were all masked as to group allocation (Jiang 2013; Jost‐Brinkman 2017; Sonesson 2019; Stecksén‐Blicks 2007; van der Kaaij 2015). In four studies just the assessor was masked for group allocation, due to differences in the nature of the interventions. One study was a comparison of fluoride varnish versus placebo (He 2010). One study was a comparison of two products containing fluoride (Sonesson 2014), one was a comparison of two methods of delivering fluoride (Luther 2005) and one study compared one fluoride and one non‐fluoride containing bonding material (Benson 2019). One study compared two fluoride products, but the masking was unclear (Ogaard 2006).
Characteristics of the outcomes
Seven studies reported our primary outcome of number of participants in each group with new demineralised lesions (DLs) (Benson 2019; Jost‐Brinkman 2017; Luther 2005; Sonesson 2014; Sonesson 2019; Stecksén‐Blicks 2007; van der Kaaij 2015). One study reported the number of teeth in each group with new DLs (Jiang 2013), one study reported a mean index score (Ogaard 2006), and in one study the outcome was unclear (He 2010).
All reported some outcomes on the severity of DLs in terms of differences in the number, size, colour, or quantitative measurement of mineral loss. None of the included studies reported outcomes of participant perception of their DLs or oral health‐related quality of life, and only one study reported adverse effects (Sonesson 2019).
Excluded studies
The details and reasons for exclusion are outlined in the Characteristics of excluded studies table. The main reasons for exclusion were that participants were not followed to the end of their orthodontic treatment and an inappropriate research methodology was used (within‐person or split‐mouth design).
Risk of bias in included studies
Overall risk of bias assessments for all included studies are shown in Figure 1. Two studies were assessed at low risk of bias for all domains (Sonesson 2019; Stecksén‐Blicks 2007). Two studies were assessed as at unclear risk of bias in one or two domains (Benson 2019; Sonesson 2014) and four in more than two domains (He 2010; Jiang 2013; Jost‐Brinkman 2017; Ogaard 2006). Two studies were assessed as at high risk of bias in one domain (Luther 2005; van der Kaaij 2015) due to a high proportion of participants withdrawing or dropping out of the studies. The authors of the studies have been contacted for further information, but at the time of publication we are awaiting clarification from the authors of two studies (Jost‐Brinkman 2017; Ogaard 2006) and one is currently uncontactable (He 2010).
Allocation
We assessed six of the included studies at low risk of bias, because the method of sequence generation and clear allocation concealment were considered adequate from either the description in the reported or following further clarification from the study authors (Benson 2019; Luther 2005; Sonesson 2014; Sonesson 2019; Stecksen‐Blicks 2007; van der Kaaij 2015).
Three studies (He 2010; Jiang 2013; Ogaard 2006) reported the method of sequence generation (randomisation table), but did not mention how they achieved equal numbers of participants in each group (since clarified for Jiang 2013) or method of allocation concealment. One study described the method of allocation concealment, but did not report the method of sequence generation (Jost‐Brinkman 2017). They were all assessed as at unclear risk of selection bias.
Blinding
In five studies the participant, clinician and assessor were all considered masked to group allocation, because the authors reported that the substances provided to the active and control groups were identical in presentation, taste, appearance and consistency (Jiang 2013; Jost‐Brinkman 2017; Sonesson 2019; Stecksén‐Blicks 2007; van der Kaaij 2015). Due to the nature of the materials used in three studies it was not possible to mask the clinician as to group allocation and the participant could have guessed (Benson 2019; Luther 2005; Sonesson 2014). It is not clear how knowledge of group allocation might affect the behaviour of the clinician and participant, so these were judged to be an unclear risk of performance bias. In one study the masking was not clear (Ogaard 2006) and the author has been contacted. In one study, the participants received different preventative regimens, at different times, therefore neither participants or operators could be masked (He 2010).
Nine studies reported that the outcome assessors were masked as to group allocation. In four of these studies more than one expert judge was involved in assessing before treatment and day of debond or close to debond photographs for new DLs (Benson 2019; Sonesson 2014; Sonesson 2019; Stecksén‐Blicks 2007). In two studies only one assessor was involved, but using relatively objective measures of demineralisation (image analysis (Luther 2005), and quantitative light‐induced fluorescence (QLF) (van der Kaaij 2015)). These were judged to be at low risk of detection bias.
We are still awaiting clarification from Jost‐Brinkman 2017 about who and how many undertook the clinical assessments, whether they were calibrated and whether any assessment of reproducibility was undertaken.
Jiang 2013 reported that assessments were undertaken clinically by one masked assessor. Although the assessor was described as having participated in the 'initial calibration trial' and intraexaminer agreement was assessed before the start of the trial, it is not clear if the repeatability was good for the full length of the trial and whether the assessor agreed with other calibrated assessors. This study was therefore assessed to be an unclear risk of detection bias.
Ogaard 2006 indicates that clinical assessments and colour photographs were obtained prior to bonding and at debond, but does not state that the photographs were used in the assessment. There are no details about who carried out the assessments or whether they were calibrated. No repeatability or reproducibility assessments are reported and this study was therefore judged to be an unclear risk of detection bias.
In He 2010 the number of assessors was unclear. It was also judged to be an unclear risk of detection bias.
Incomplete outcome data
The proportion of post‐randomisation exclusions was reported as zero in one study (He 2010), and low in four studies (Benson 2019; Jiang 2013; Sonesson 2019; Stecksén‐Blicks 2007). The numbers and reasons for exclusion were similar for each group and the risk of attrition bias and the effect of this on the interpretation of the findings is outlined in the 'Risk of bias' tables for each study. The report by Benson 2019 had a flow diagram and fully reported the reasons for withdrawal or dropout, which were about equal in the two groups. Two studies were assessed as an unclear risk of attrition bias (Ogaard 2006; Sonesson 2014). The reasons for this are given in the 'Risk of bias' tables for each study. The report by Ogaard 2006 had neither a flow diagram, nor a detailed explanation of the reasons for withdrawal or dropout. Sonesson 2014 had a flow diagram and reported the reasons for withdrawal or dropout, however it reports that a number of participants "did not comply with the study protocol" and were excluded from the analysis, but the definition of non‐compliance is unclear. Due to inconsistencies on the number of exclusions from analyses and lack of clarity on non‐compliance Jost‐Brinkman 2017 was also assessed as at unclear risk of attrition bias. Two studies were assessed as at high risk of attrition bias, because a significant proportion of the participants who were randomised were not included in the analysis (47% (Luther 2005), 33% (van der Kaaij 2015)).
Selective reporting
Ogaard 2006 reported the change in the mean Gorelick Index scores, as well as the numbers of teeth with new DLs and was assessed as at unclear risk of reporting bias. The report by Luther 2005 had some information missing and the denominators were not stated, so this study was assessed at unclear risk of reporting bias. In He 2010 the definition of incidence is unclear (difference between start and finish) and it does not state how they took into account the clustering of teeth within the mouth, therefore the study was also assessed at unclear risk of reporting bias.
Other potential sources of bias
Four studies reported data for the number of participants with new DLs at or near the date of debond (Benson 2019; Sonesson 2014; Sonesson 2019; Stecksén‐Blicks 2007). All these studies assessed the number of new DLs (incidence) by comparing pre‐treatment and at or near debond photographs and were considered to be at low risk of other potential sources of bias. Other potential sources of bias are discussed for these studies, but they were assessed at low potential risk of bias, as was the study by Ogaard 2006. Luther 2005 was assessed at unclear risk of other bias, because of possible differences between the groups in terms of compliance, duration of orthodontic treatment and exposure to topical fluorides. van der Kaaij 2015 was also assessed as at unclear risk of bias, because it is unclear if all the QLF images were collected and analysed from the day of debond. The authors state that the "WSL assessments were made at an average of 52 d (days) after debonding (with a range of 0‐156 d)." Those undertaken at five months following debond might have undergone quite extensive remineralisation unrelated to mouthrinse use. Jiang 2013 was also assessed as unclear risk of bias in this domain, because it was not clear from the report how many operators were involved in the study and how the investigators controlled for other sources of fluoride. We are still awaiting clarification about other sources of bias from Jost‐Brinkman 2017 and were not able to contact the authors of He 2010.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5
Summary of findings for the main comparison. Dentist/nurse‐applied fluoride: fluoride varnish compared to non‐fluoride (placebo) varnish for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| Fluoride varnish compared to non‐fluoride (placebo) varnish for preventing early tooth decay (demineralised lesions) during fixed brace treatment | |||||||
| Patient or population: orthodontic patients (any age) Setting: orthodontic clinics in Sweden Intervention: fluoride varnish Comparison: non‐fluoride (placebo) varnish | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With non‐fluoride (placebo) varnish | With fluoride varnish | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: pre‐treatment and day of debond clinical intraoral photographs Follow‐up: 1.7 years |
28.80% | 15% (4 to 55.60) | 13.80% fewer (24.80 fewer to 26.80 more) | RR 0.52 (0.14 to 1.93) | 405 (2 RCTs) | ⊕⊕⊝⊝ LOWa,b | The evidence that professional application of fluoride varnish (7700 or 10,000 ppm F) every 6 weeks to the teeth of patients wearing fixed orthodontic braces reduces the number of new DLs is equivocal |
| Number of participants with more severe DLs (severity of DLs) (score 3 or 4 versus score 1 or 2) Follow‐up: 1.7 years |
26% | 12% (5.70 to 24.70) | 14.10% fewer (20.30 fewer to 1.30 fewer) | RR 0.46 (0.22 to 0.95) | 148 (1 RCT) | ⊕⊕⊝⊝ LOWc,d | The evidence suggests that when a dentist or nurse applies 7700 ppm F (ammonium fluoride) varnish every 6 weeks to a patient wearing a fixed orthodontic brace there may a reduction in the number of orthodontic patients with more severe DLs (score 3 or 4 versus score 1 or 2) |
| Number of participants with adverse effects (adverse effects) Follow‐up: 1.7 years |
No evidence that the intervention had adverse effects | 148 (1 RCT) | ⊕⊕⊝⊝ LOWd,e | Only 1 participant with an adverse event and not clear if this was directly related to the intervention | |||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; F: fluoride; ppm: parts per million; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 1 level for indirectness (evidence from only 2 studies) (Stecksén‐Blicks 2007; Sonesson 2019). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guideline 300 to 400 events)). cDowngraded 1 level for imprecision (insufficient number of participants with the more severe DLs (guideline 300 to 400 events)). dDowngraded 1 level for indirectness (evidence from only 1 study) (Sonesson 2019). eDowngraded 1 level for imprecision (insufficient number with adverse events and not clear if directly related to the intervention).
Summary of findings 2. Dentist/nurse‐applied fluoride: 12,300 ppm F APF foam compared to 0 ppm F placebo foam for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| 12,300 ppm F APF foam compared to 0 ppm F placebo foam for preventing early tooth decay (demineralised lesions) during fixed brace treatment | |||||||
| Patient or population: orthodontic patients (any age) Setting: orthodontic department at dental hospital in China Intervention: 12,300 ppm F APF foam Comparison: 0 ppm F placebo foam | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Certainty of the evidence (GRADE) | Number of participants (studies) | Comments | ||
| With 0 ppm F placebo foam | With 12,300 ppm F APF foam | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: clinical assessment Follow‐up: mean 18 months |
48.90% | 12.70% (5.40 to 27.90) | 36.20% fewer (43.60 fewer to 21 fewer) | RR 0.26 (0.11 to 0.57) | ⊕⊕⊝⊝ LOWa,b | 95 (1 RCT) | The evidence suggests that when foam, containing 12,300 ppm F, is applied by a dentist or a nurse, every 2 months, to the teeth of patients wearing fixed orthodontic appliances there might be a reduction in the number of patients who have at least 1 new DL |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | ||||||
| Number of participants with adverse effects (adverse effects) | None of the trials reported this outcome | ||||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). APF: acidulated phosphate fluoride; CI: confidence interval; DLs: demineralised lesions; F: fluoride; ppm: parts per million; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aAlthough effect size is large this was only for 1 study at unclear risk of bias and therefore downgraded 1 level (Jiang 2013). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guideline 300 to 400 events)).
Summary of findings 3. Patient‐applied/used fluoride: 5000 ppm F toothpaste compared to 1450 ppm F toothpaste for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| 5000 ppm F toothpaste compared to 1450 ppm F toothpaste for preventing early tooth decay (demineralised lesions) during fixed brace treatment | |||||||
| Patient or population: orthodontic patients (any age) Setting: home use Intervention: 5000 ppm F toothpaste Comparison: 1450 ppm F toothpaste | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With 1450 ppm F toothpaste | With 5000 ppm F toothpaste | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: pre‐treatment and post‐treatment clinical intraoral photographs Follow‐up: 1.8 years |
26.60% | 18.10% (12.20 to 26.60) | 8.50% fewer (14.30 fewer to 0 fewer) | RR 0.68 (0.46 to 1.00) | 380 (1 RCT) | ⊕⊕⊝⊝ LOWa,b | The evidence suggests that in patients wearing an orthodontic fixed brace use of a daily 5000 ppm F toothpaste compared with a daily 1450 ppm F toothpaste throughout treatment may lead to a reduction in the number of orthodontic patients with new DLs |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | ||||||
| Number of participants with adverse effects (adverse effects) | None of the trials reported this outcome | ||||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; F: fluoride; ppm: parts per million; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 1 level due to single study at unclear risk of bias (Sonesson 2014). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guideline 300 to 400 events)).
Summary of findings 4. Patient‐applied/used fluoride: 250 ppm F mouthrinse (100 ppm F amine F/150 ppm NaF) compared to 0 ppm F placebo mouthrinse for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| 250 ppm F mouthrinse (100 ppm amine F/150 ppm NaF) compared to 0 ppm F placebo mouthrinse for preventing early tooth decay (demineralised lesions) during fixed brace treatment | |||||||
| Patient or population: orthodontic patients (any age) Setting: home use Intervention: 250 ppm F mouthrinse (100 ppm amine F/150 ppm NaF) Comparison: 0 ppm F placebo mouthrinse | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With 0 ppm F placebo mouthrinse | With 250 ppm F mouthrinse (100 ppm amine F/150 ppm NaF) | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: QLF Follow‐up: 24.5 months |
46.70% | 30.30% (17.30 to 54.60) | 16.30% fewer (29.40 fewer to 7.90 more) | RR 0.65 (0.37 to 1.17) | 81 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | The evidence is very uncertain about the effect of a daily 250 ppm F mouthrinse (100 ppm amine F/150 ppm NaF) compared with a daily 0 ppm F placebo mouthrinse on the number of patients wearing a fixed orthodontic brace with new DLs |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | ||||||
| Number of participants with adverse effects (adverse effects) | None of the trials reported this outcome | ||||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; F: fluoride; NaF: sodium fluoride; ppm: parts per million; QLF: quantitative light‐induced fluorescence; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 2 levels: single study with a relatively small number of participants (81), at high risk of bias due to high attrition (33%) (van der Kaaij 2015). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guidance 300 to 400 events)).
Summary of findings 5. Fluoride‐releasing materials: resin‐modified glass ionomer cement compared to light‐cured composite resin for bonding orthodontic brackets for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| Resin‐modified glass ionomer cement compared to light‐cured composite resin for bonding orthodontic brackets for preventing early tooth decay (demineralised lesions) during fixed brace treatment | |||||||
| Patient or population: orthodontic patients (any age) Setting: 2 dental teaching hospitals and 4 specialist orthodontic practices in UK and Republic of Ireland Intervention: resin‐modified glass ionomer cement Comparison: light‐cured composite resin | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With light‐cured composite resin | With resin‐modified glass ionomer cement | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: before and day of debond clinical intraoral photographs Follow‐up: 17.6 months |
22.40% | 26.20% (15.40 to 44.50) | 3.80% more (6.90 fewer to 22.10 more) | RR 1.17 (0.69 to 1.99) | 173 (1 RCT) | ⊕⊕⊝⊝ LOWa,b | The evidence suggests that resin‐modified glass ionomer cement for bonding orthodontic brackets compared with light‐cured composite resin results in little to no difference in the number of orthodontic patients with new DLs |
| Number of participants with more severe DLs of aesthetic concern (severity of DLs) Assessed with: pre‐treatment and day of debond clinical intraoral photographs Follow‐up: 17.6 months |
8.00% | 9.40% (3.60 to 24.80) | 1.40% more (4.40 fewer to 16.90 more) | RR 1.18 (0.45 to 3.12) | 173 (1 RCT) | ⊕⊕⊝⊝ LOWa,b | The evidence suggests that using resin‐modified glass ionomer cement for bonding orthodontic brackets compared with light‐cured composite resin results in little to no difference in the number of orthodontic patients with more severe DLs of aesthetic concern |
| Number of participants with adverse effects (adverse effects) Follow‐up: 17.6 months |
No evidence that either intervention had adverse effects | 173 (1 RCT) | ⊕⊕⊝⊝ LOWa,b | ‐ | |||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 1 level: single study at unclear risk of bias (Benson 2019). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs or more severe DLs (guidance 300 to 400 events)).
The 10 studies included in this review evaluated different modes of fluoride application, which we have categorised into three broad methods.
Professionally‐applied (dentist or nurse‐applied) fluoride in the form of varnish (He 2010; Sonesson 2019; Stecksén‐Blicks 2007), foam (Jiang 2013) and gel (Jost‐Brinkman 2017), both home use once a week and professional application every three months.
Patient‐applied/used fluoride in the form of toothpaste/mouthrinse combinations (Ogaard 2006; Sonesson 2014; van der Kaaij 2015).
Fluoride‐releasing materials in the form of intraoral fluoride‐releasing glass bead device (Luther 2005) and resin‐modified glass ionomer cement for bonding orthodontic brackets (Benson 2019).
Although the study by Jost‐Brinkman and colleagues (Jost‐Brinkman 2017) investigated both a dentist/nurse‐applied and a patient‐applied fluoride intervention in the same participants, we have placed this in the dentist or nurse‐applied category for the reasons explained previously. Summaries of the methods, participants, interventions and outcomes for each study are provided in the Characteristics of included studies tables.
Dentist or nurse‐applied fluoride
Primary outcome
Stecksén‐Blicks 2007 reported a prevalence of DLs before treatment of 4.3% in participants who received the professionally‐applied fluoride varnish (experimental group) and 4.0% in those receiving the professionally‐applied non–fluoride placebo varnish (control group). At debond the proportions of participants with DLs was 11.7% in the experimental group and 29.7% in the control group, which the authors state as an incidence of 7.4% and 25.7% respectively. The authors report a risk reduction or preventive fraction (1‐RR) of 0.69 for new DLs. The authors calculated that nearly 6 (5.5) individuals would need to receive the fluoride varnish every orthodontic visit (approximately every six weeks) to prevent one patient from having a new DL (number needed to treat or NNT). This result should be treated with caution, because another trial by Sonesson and colleagues (Sonesson 2019) using a slightly lower concentration of fluoride varnish (7000 parts per million (ppm) fluoride) had different findings. They reported a prevalence of DLs before treatment of 8.0% (6 out of 75) in participants who received the professionally‐applied fluoride varnish (experimental group) and 9.6% (7 out of 73) in those receiving the professionally‐applied non‐fluoride placebo varnish (control group). At debond the proportions of participants with DLs (index scores of 2 and above) was 41.3% (31 out of 75) in the experimental group and 43.8% (32 out of 73) in the control group. Combining the data from these two studies the calculated risk ratio (RR) for the development of new lesions with professionally‐applied fluoride varnish was 0.52 (95% confidence interval (CI) 0.14 to 1.93; 405 participants; Analysis 1.1), which is a non‐significant reduction.
1.1. Analysis.
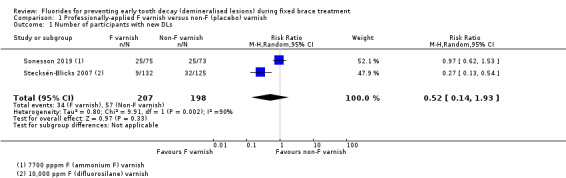
Comparison 1 Professionally‐applied F varnish versus non‐F (placebo) varnish, Outcome 1 Number of participants with new DLs.
Jost‐Brinkman 2017, who applied fluoride gel every three months (as well as home‐used gel), found no difference in the development of DLs between those who were allocated to the fluoride gel and those to the placebo gel (RR 0.99, 95% CI 0.76 to 1.27; 312 participants; Analysis 2.1).
2.1. Analysis.
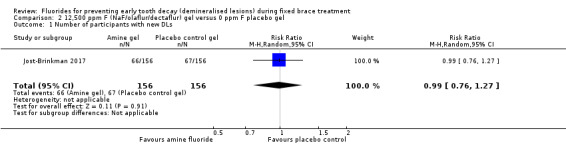
Comparison 2 12,500 ppm F (NaF/olaflur/dectaflur) gel versus 0 ppm F placebo gel, Outcome 1 Number of participants with new DLs.
Jiang 2013 found that applying a fluoride‐containing foam professionally every two months reduces the incidence of new DLs after fixed orthodontic treatment (RR 0.26, 95% CI 0.11 to 0.57; 95 participants analysed; Analysis 3.1).
3.1. Analysis.
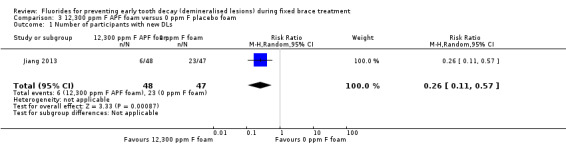
Comparison 3 12,300 ppm F APF foam versus 0 ppm F placebo foam, Outcome 1 Number of participants with new DLs.
As previously stated we were not able to contact the authors of He 2010.
Secondary outcomes
Stecksén‐Blicks 2007 stated that they calculated a "progression score" by "subtracting the debond score from that registered at baseline." The progression scores were mean 0.8 (standard deviation (SD) 2.0) for participants who received the fluoride varnish and mean 2.6 (SD 2.8) for those who received the placebo varnish. We interpret this as the control group having a greater number of teeth with lesions, as well as a greater incidence. In terms of severity Figure 2 in the study shows that the great majority of new lesions were minor (Gorelick Index score 2: slight white spot formation, thin rim) and the aesthetic impact of the new DLs was not assessed.
Sonesson 2019 reported a reduction in the number of participants with the more severe DLs (index score of 3 or 4) at debond in the experimental group who received the fluoride varnish (12%, 9 out of 75), compared with the non‐fluoride control (26%, 19 out of 73). This is a RR of 0.46 (95% CI 0.22 to 0.95) and a number needed to treat of 7 (but with a wide confidence interval 3.80 to 71.10).
Jiang 2013 reported that the "mean net increment" in the scores was 0.7 (SD 2.8) for those who received the fluoride foam and 4.4 (SD 5.4) for those who received the non‐fluoride foam. This is a large increase, which we interpret as those not receiving the fluoride foam having a greater number of teeth affected by DLs. The authors cite a NNT, but we believe this is calculated on the number of teeth with new DLs, not participants, which is not appropriate. Again, the severity scores (Figure 2) were mostly minor (Gorelick Index 2) and the aesthetic impact is uncertain.
There were no data reported from any of the studies about participant perception of their DLs or any measure of oral health‐related quality of life. Only Sonesson 2019 reported adverse effects and that one participant who received the fluoride varnish withdrew from their study, due to a feeling of slight nausea during the trial.
Patient‐applied/used various fluoride toothpaste/mouthrinse combinations
Primary outcome
Sonesson 2014 found that the proportions of participants with DLs before orthodontic treatment were 17% in the high concentration fluoride (5000 ppm) toothpaste group and 19% in the standard concentration fluoride (1450 ppm) toothpaste group. These proportions increased to 35% and 45% respectively, on the day of debond. The calculated RR of developing a new DL is 0.68 (95% CI 0.46 to 1.00; 380 participants; Analysis 4.1). Although the upper confidence interval contacts the line of no difference, we believe that this provides evidence that the use of high fluoride toothpaste by patients wearing fixed orthodontic appliances does provide some protection against new DLs, with a risk reduction or preventive fraction (1‐RR) of 0.32 and a NNT of 12. As with the trial by Stecksén‐Blicks 2007, however, the results of this trial should be interpreted with caution until further clinical trials confirm this finding.
4.1. Analysis.
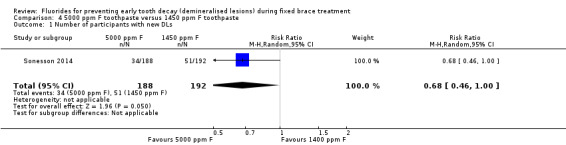
Comparison 4 5000 ppm F toothpaste versus 1450 ppm F toothpaste, Outcome 1 Number of participants with new DLs.
van der Kaaij 2015 states that none of their participants had DLs before the start of treatment. They report that 11 of 36 participants in the fluoride mouthrinse group developed at least one new DL, compared with 21 of 45 participants in the non‐fluoride mouthrinse group. However, the calculated RR is 0.65 (95% CI 0.37 to 1.17; 81 participants; Analysis 5.1) and the confidence interval crosses the line of no difference. The lack of statistical significance could be due to the small number of participants and the large proportion of withdrawals and dropouts.
5.1. Analysis.
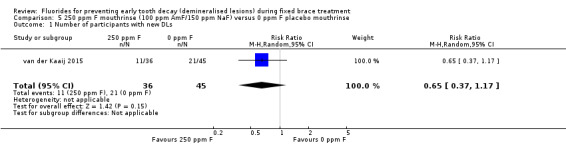
Comparison 5 250 ppm F mouthrinse (100 ppm AmF/150 ppm NaF) versus 0 ppm F placebo mouthrinse, Outcome 1 Number of participants with new DLs.
Ogaard 2006 reported the outcome of new DLs at the tooth level with no indication of correction for clustering of teeth within the mouth. The author has been contacted to provide these data at the participant level.
Secondary outcomes
Sonesson 2014 reported that the mean numbers of DLs before the start of treatment were 0.3 (SD 1.0) in the high concentration fluoride (5000 ppm) toothpaste group and 1.0 (SD 1.8) in the standard concentration fluoride (1450 ppm) toothpaste group. These increased to 0.4 (SD 1.0) and 1.2 (SD 1.8) respectively, at debond. They also stated that the "vast majority of all new WSL were thin rims (score 2) in both groups," with only 1.2% in the high fluoride toothpaste group and 2.3% in the standard fluoride toothpaste group having teeth affected with the more severe Gorelick Index scores of 3 or 4. The aesthetic impact of the DLs is, therefore, unclear. Like most studies they report that lateral incisors were the most frequently affected teeth in both groups, followed by the canines and premolars.
van der Kaaij 2015 reported that the number of new DLs ranged from 1 to 5 in participants who received the fluoride mouthrinse (experimental group) and 1 to 15 in those receiving the non‐fluoride mouthrinse (control group). The quantitative light‐induced fluorescence (QLF) measurements revealed a mean fluorescence loss (delta F; DL – sound enamel) of 11.6% (SD 5.0) in the experimental group and 10.3% (SD 3.0) in the control group. The lesion depths were 0.9 mm2 (SD 0.6) and 1.3 mm2 (SD 1.6 mm) respectively. Neither were reported as statistically significant and there is no indication in the report how these QLF measurements can be interpreted in terms of aesthetic impact.
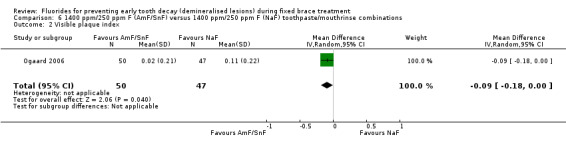
Ogaard 2006 found a greater mean change in the 'white spot lesion index' from baseline in a group of participants using a neutral sodium fluoride toothpaste (1400 ppm, pH 6.7) twice daily and a sodium fluoride mouthrinse (250 ppm fluoride (F), pH 6.3) at night compared with a group using amine fluoride/stannous fluoride toothpaste (Meridol 140 ppm F, pH 4.5) twice daily and an amine fluoride/stannous fluoride mouthrinse (250 ppm F, pH 4.0) after toothbrushing at bedtime (97 participants; Analysis 6.1). This suggest that the sodium fluoride combination was less effective than the amine fluoride/stannous fluoride. They also found a slightly larger increase in both the visible plaque index and the gingival bleeding index over the duration of treatment in the group exposed to sodium fluoride (97 participants; Analysis 6.2; Analysis 6.3). These differences, however, should be interpreted cautiously until the results can be independently replicated.
6.1. Analysis.
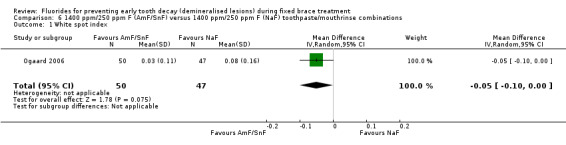
Comparison 6 1400 ppm/250 ppm F (AmF/SnF) versus 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse combinations, Outcome 1 White spot index.
6.2. Analysis.
Comparison 6 1400 ppm/250 ppm F (AmF/SnF) versus 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse combinations, Outcome 2 Visible plaque index.
6.3. Analysis.
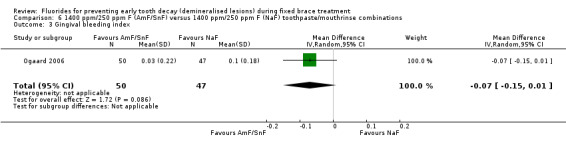
Comparison 6 1400 ppm/250 ppm F (AmF/SnF) versus 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse combinations, Outcome 3 Gingival bleeding index.
There were no data reported from any of the studies about participant perception of their DLs, any measure of oral health‐related quality of life, and/or reports of adverse effects.
Fluoride‐releasing materials
Primary outcome
Benson 2019 did not assess the number of DLs at baseline, rather the assessors were asked to look concurrently at the before treatment and day of debond images and determine if they saw new DLs. On this basis 23 out of 88 participants who received the fluoride‐containing bonding material (resin‐modified glass ionomer cement) were assessed as having new DLs versus 19 out of 85 who received the material containing no fluoride (light‐cured composite resin). The calculated RR was 1.17 (95% CI 0.69 to 1.99; 173 participants; Analysis 7.1); therefore, there was no difference statistically or clinically in the proportion of participants with new DLs between the two groups.
7.1. Analysis.
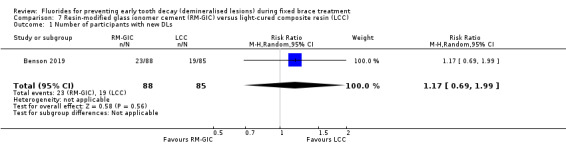
Comparison 7 Resin‐modified glass ionomer cement (RM‐GIC) versus light‐cured composite resin (LCC), Outcome 1 Number of participants with new DLs.
Luther 2005 reported that, of those participants completing the trial, 10 of the 18 receiving the fluoride‐containing glass beads developed DLs, compared with 7 out 19 receiving the fluoride mouthrinse. The calculated RR was 1.51 (95% CI 0.73 to 3.10; 37 participants; Analysis 8.1), which is not statistically significant.
8.1. Analysis.
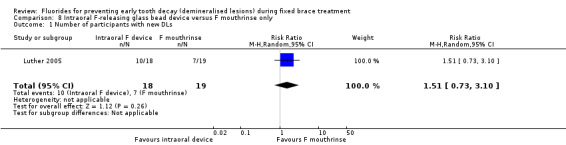
Comparison 8 Intraoral F‐releasing glass bead device versus F mouthrinse only, Outcome 1 Number of participants with new DLs.
Secondary outcomes
Unlike any of the other studies, Benson 2019 undertook an assessment of the aesthetic impact of the new DLs. They found that in only 15 of the 42 participants with new DLs were the lesions judged to be of aesthetic concern by a majority of the expert and lay assessors. Therefore, the incidence of aesthetically displeasing new DLs was 9% compared with the overall incidence of 24% and there was no difference between the groups (fluoride material 8 out of 23; non‐fluoride material 7 out of 19). Like other studies they found that upper lateral incisors were affected most, followed by upper central incisors and upper canines. This study also reported the proportion of bond failures, which was not an outcome in this review.
Luther 2005 reported that, for those participants who completed their trial, there was no statistically significant difference in the numbers of teeth affected by DLs between the two groups (fluoride‐releasing beads 17 out of 108 teeth; fluoride mouthrinse 19 out of 114).
There were no data reported from any of the studies about adverse effects, participant perception of their DLs and/or any measures of oral health‐related quality of life.
Discussion
Summary of main results
There is insufficient evidence of a difference from two trials, judged to be at a low risk of bias, on the effectiveness of fluoride varnish applied, by a professional, every six weeks in reducing new demineralised lesions (DLs) during fixed orthodontic treatment (Table 1). Evidence from one trial judged to be at unclear risk of bias, provides a low level of certainty that fluoride foam (12,300 parts per million (ppm) fluoride), professionally applied every two months, reduces the incidence of new DLs after fixed orthodontic treatment (Table 2). Similarly, one trial, assessed as at unclear risk of bias, provides a low level of certainty that use of a high‐concentration fluoride toothpaste by patients throughout their fixed orthodontic treatment reduces the incidence of new DLs, compared with a conventional concentration of fluoride toothpaste (Table 3).
Evidence is insufficient to show whether the use of a professionally‐applied amine fluoride gel reduces new DLs (Additional Table 6), or patient use of a sodium fluoride/amine fluoride mouthrinse (Table 4) or amine fluoride and stannous fluoride toothpaste/mouthrinse combination (Additional Table 7) is more or less effective than a non‐fluoride mouthrinse or a sodium fluoride toothpaste/mouthrinse combination respectively. Finally, there is no evidence that either a fluoride‐containing material to bond brackets (Table 5) or an intraoral fluoride‐releasing glass bead device (Additional Table 8) reduces the incidence of new DLs.
1. Summary of findings for 12,500 ppm F (NaF/olaflur/dectaflur) fluoride gel compared to 0 ppm F placebo gel for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| Patient or population: orthodontic patients (any age) Setting: dental clinics in Germany and Israel and home use Intervention: 12,500 ppm F (NaF/olaflur/dectaflur) fluoride gel Comparison: 0 ppm F placebo gel | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With 0 ppm F placebo gel | With 12,500 ppm F (NaF/olaflur/dectaflur) fluoride gel | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: clinical examination Follow‐up: mean 16.6 months |
42.90% | 42.50% (32.60 to 54.50) | 0.40% fewer (10.30 fewer to 11.60 more) | RR 0.99 (0.76 to 1.27) | 312 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b,c | The evidence is very uncertain about the effect of an amine fluoride gel compared with a placebo gel on the number of patients wearing fixed orthodontic braces with new DLs |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | ||||||
| Number of participants with adverse effects (adverse effects) Follow‐up: mean 16.6 months |
0.60% | 0.00% (0 to 0) | 0.60% fewer (0.60 fewer to 0.60 fewer) | Not estimable | 312 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,c,d | Authors write "Most AEs (96.4%) were unrelated to the study treatment. Only a single AE (hay fever) was considered related to the study treatment (placebo)." They go on to state "The use... for a maximum of 32.5 months was not associated with any unexpected ARs or AEs. Thus, there are no safety issues to be considered for long‐term use of elmex® gel" |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AE: adverse effects; CI: confidence interval; DLs: demineralised lesions; F: fluoride; NaF: sodium fluoride; ppm: parts per million; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 1 level due to single study at unclear risk of bias (Jost‐Brinkman 2017). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guidance 300 to 400 events)). cDowngraded 1 level for publication bias (data collection for the trial was completed in 2011. The results were obtained from the study report that was published in 2016, but not yet submitted to a peer‐reviewed journal). dDowngraded 1 level for imprecision (insufficient number with adverse events).
2. Summary of findings for 1400 ppm/250 ppm F (amine F/SnF) toothpaste/mouthrinse compared to 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| Patient or population: orthodontic patients (any age) Setting: home use Intervention: 1400 ppm/250 ppm F (amineF/SnF) toothpaste/mouthrinse Comparison: 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse | Risk with 1400 ppm/250 ppm F (amineF/SnF) toothpaste/mouthrinse | |||||
| Number of participants with new DLs (new DLs) Follow‐up: 1.5 years |
Outcome not reported. White spot lesion index, visible plaque index and gingival bleeding index reported instead: MD 0.05 lower (0.10 lower to 0) white spot index, MD 0.09 lower (0.18 lower to 0) visible plaque index, MD 0.07 lower (0.15 lower to 0.01 higher) gingival bleeding index for 1400 ppm/250 ppm F (amine F/SnF) toothpaste/mouthrinse | ‐ | 97 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b,c | The evidence is very uncertain about the effect of daily 1400 ppm/250 ppm F (amine F/SnF) versus 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse combinations on the white spot index, visible plaque index and on the gingival bleeding index in patients wearing fixed orthodontic braces | |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | |||||
| Number of participants with adverse effects (adverse effects) | None of the trials reported this outcome | |||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; F: fluoride; MD: mean difference; NaF: sodium fluoride; ppm: parts per million; RCT: randomised controlled trial; SnF: stannous fluoride. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded 1 level due to single study assessed at unclear risk of bias (Ogaard 2006). bDowngraded 1 level for indirectness (outcomes assessed were not the most useful for answering this question). cDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guideline 300 to 400)).
3. Summary of findings for intraoral fluoride‐releasing glass bead device compared to 250 ppm F mouthrinse for preventing early tooth decay (demineralised lesions) during fixed brace treatment.
| Patient or population: orthodontic patients (any age) Setting: teaching hospital in UK and home use Intervention: intraoral fluoride‐releasing glass bead device Comparison: 250 ppm F mouthrinse | |||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | ||
| With 250 ppm F mouthrinse | With intraoral fluoride‐releasing glass bead device | Difference | |||||
| Number of participants with new DLs (new DLs) Assessed with: clinical intraoral photographs Follow‐up: 19 months |
36.80% | 55.60% (26.90 to 100) | 18.80% more (9.90 fewer to 77.40 more) | RR 1.51 (0.73 to 3.10) | 37 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | The evidence is very uncertain about the effect of intraoral fluoride‐releasing glass bead devices compared with daily 250 ppm F mouthrinses on the number of patients wearing a fixed orthodontic brace with new DLs |
| Number of participants with more severe DLs (severity of DLs) | None of the trials reported this outcome | ||||||
| Number of participants with adverse effects (adverse effects) Follow‐up: 19 months |
‐ | ‐ | ‐ | ‐ | 37 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b,c | Current design of fluoride glass bead inadequate. The authors write "an improved method of attachment is needed before it can be established whether FGBs (fluoride glass beads) are more effective than FR (fluoride mouthrinse)."c |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DLs: demineralised lesions; F: fluoride; ppm: parts per million; RCT: randomised controlled trial; RR: risk ratio. | |||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | |||||||
aDowngraded 2 levels due to single study at high risk of bias (high attrition (47%)) (Luther 2005). bDowngraded 1 level for imprecision (insufficient number of participants with new DLs (guidance 300 to 400 events)). cHigh attrition partly due to breaks of the glass beads. The authors write "Some patients in the FGB (fluoride glass bead) group experienced a large number of bead breakages, resulting in a number of patients requesting to leave the trial." Numbers not supplied.
Overall completeness and applicability of evidence
As with the last version, the update of this review has included only parallel‐group trials, in which the individual participant is the unit of randomisation. This was decided upon because of the possibility of cross‐contamination between experimental and control teeth in the same mouth, either between upper and lower arches or between sides of the mouth, which might lead to under‐estimation of the effectiveness of any fluoride products.
Interventions that rely on the patient for delivery, including fluoride mouthrinse and toothpaste, will work only if they are used regularly. They rely greatly on patient compliance to succeed; however, evidence suggests that compliance with mouthrinsing is poor among orthodontic patients. One study (Geiger 1992) found that only 42% of participants rinsed with a sodium fluoride mouthrinse at least every other day. Results also showed that those who complied least with fluoride rinsing regimens tended to have more DLs. It is important to consider the acceptability of interventions to both adolescents and adults with a view toward increasing compliance with recommended dental hygiene practices.
Interventions that are professionally applied and deliver fluoride 'passively', such as fluoride varnish, fluoride‐releasing bracket cements and fluoride‐releasing elastics, avoid the need for patient compliance. In addition, these materials deliver fluoride close to the bracket, where it is most needed. Many fluoridated materials release large amounts of fluoride initially, but the level drops rapidly and might not be sufficient to prevent decay over the whole course of orthodontic treatment. Reapplication of fluoride varnish and frequent replacement of fluoride‐releasing elastics are likely to be required. In the parallel‐group trial of a fluoride varnish intervention included in this review, varnish was reapplied every six weeks at each orthodontic check‐up appointment. We found no parallel‐group trials of fluoride‐releasing cements or elastics that met the inclusion criteria for this review.
An interesting addition, since the initial review was carried out, is the further development of materials that produce a slow and sustained release of fluoride (Luther 2005). This trial was small and at high risk of bias, and evidence was insufficient to reveal whether these devices are more or less effective than a mouthrinse in reducing the development of DLs. It is possible, that with further refinement, this technique could potentially be effective. Intraoral fluoride‐releasing devices should be evaluated by parallel‐group randomised controlled trials with appropriate masking of participants, clinicians/operators and assessors.
When examining the effectiveness of a fluoride product in preventing dental decay, one should consider two aspects: first, whether the fluoride product reduces the number of DLs appearing during treatment, and second, whether it reduces the severity of DLs in terms of the size or area of the tooth surface affected, the amount of mineral lost or the depth of decay. Banks et al (Banks 2000) developed the Enamel Decalcification Index, which is an ordinal index that includes an assessment of the area covered. Assessment of the size of the lesion is a useful outcome measure, but none of the studies included in this review reported this outcome.
Ideally the appearance of the tooth should be recorded before and after orthodontic treatment, so that the change in appearance of the tooth is measured (incidence), not just its appearance at the end (prevalence). There are many different causes of coloured marks on the teeth, many of which occur during their development. It is important that these development lesions, as well as decay that has occurred before the brace is fitted, are excluded from the analysis, hence the need for the clinical photographs or fluorescent images taken before treatment. Measurement of both incidence and severity will depend on the method used to record DLs. Two main methods may be used: visual inspection and clinical images. Both methods are associated with problems. One problem with visual inspection is that the examiner or examiners will require calibration at the start and regular recalibration throughout the experimental period to ensure consistency of measurement. The duration of the experiment, including the recruitment and data collection will be long because, as discussed later, the product should be tested over the entire length of orthodontic treatment. This can take between 18 and 30 months ‐ sometimes longer. Another problem with visual recording clinically involves masking of the assessor to the allocated intervention. To reduce bias, the examiner should not know whether the participant has received a fluoride product and this will complicate the way the experiment is run.
Images have the advantage of providing a permanent record of the appearance of the tooth. Assessments can be carried out by several people independently or in groups, whereby a consensus is achieved. The images can be placed in a random order and the judges masked to group allocation. In addition, because the assessment can be performed over a short period of time the problem of examiner drift, whereby an assessor might subtly change his or her assessment over time, is reduced. The challenge of using clinical photographs consists of achieving consistency in lighting and reducing reflections that can mask or mimic DLs. When a careful photographic technique is applied, however, the advantages of photographs outweigh their potential disadvantages. Several optical and fluorescent methods are available for measuring lesions on the teeth (Angmar‐Mansson 1996). These methods require specialised equipment, which would add considerably to the cost of a clinical study, but they provide an objective measurement of the amount of decay in terms of mineral loss or lesion depth or both.
Quality of the evidence
Two studies included in this review were judged to be at low risk of bias in all domains; however clarification over some issues was required from some of the authors before these judgements could be confirmed. Both the design and the reporting of trials of fluorides for preventing DLs have improved since the first version of this review and we hope that this may continue. Undoubtedly the increasing use of the CONSORT guidelines for the reporting of randomised controlled trials has been a factor.
Several of the studies were assessed at some risk of bias as a result of the proportion of participants randomised to the intervention not been included in the analysis following withdrawal or dropout. It is inevitable that some patients will move away during a course of orthodontic treatment, but every effort should be made to collect records and data at the appropriate times, even if the treatment is finished early.
Another issue in orthodontic research is that it is often not possible to mask the clinician/operator to the allocated intervention. In these situations the participant can also usually work out to which group they have been allocated and, therefore, triple‐blinding is difficult, if not impossible to achieve. It is, however, not clear how much this will affect the behaviour of the clinician and the participant. It is known that patients respond favourably to simply being part of a clinical trial, irrespective of whether they have received the active intervention or the control (McCarney 2007). This is the so‐called Hawthorne effect, named after a Chicago electrical company works, whose workers were subjected to a series of experiments during the 1920s and 1930s. The investigators noticed that no matter how they changed the working conditions of the workers their productivity improved and concluded it was because they knew they were part of an experiment. We believe that it would be harsh to judge all trials that are not triple‐blind as a potentially high risk of bias when the effects are not known and perhaps this should be an area of research in the future.
Potential biases in the review process
We undertook a sensitive search of several electronic sources, supplemented by searches of references lists. We placed no restriction on language or publication status. The review authors have tried, as far as possible, to identify all possible studies that might meet the inclusion criteria for this review. Study authors have been contacted, and many have replied; however, some were not able to supply the requested information, as their records have been destroyed or lost.
When a product, such as a bonding material, can be applied to single teeth, it is tempting to use an experimental design whereby the material being tested is used in two quadrants of the mouth and the control material is used in the other two quadrants. This is called a split‐mouth design. The main advantage of the split‐mouth design over a conventional parallel‐group study design, in which the two materials are tested in two separate groups of individuals, is that the experimental material is tested in the same mouth, under the same conditions as the control material. In theory, any differences in outcome between the two materials are due only to their properties ‐ not to other factors, such as differences in oral hygiene and diet between participants (with a parallel design) or even differences in oral hygiene and diet over time within the same participants (with a cross‐over design).
Unfortunately, when one is examining the ability of fluoride products to reduce decay, it is highly unlikely that the fluoride released will be confined to only the quadrants/teeth in which the experimental material has been placed, and some contamination of the 'untreated' teeth is inevitable. This contamination will reduce the difference in outcomes between treated and untreated teeth. The previous version of this review included split‐mouth studies, which failed to show any difference between treated and untreated teeth; this may be due to cross‐over contamination between control and experimental sides and may reflect our contention of contamination. For this reason, we have decided to exclude split‐mouth studies from the previous update of our review.
Agreements and disagreements with other studies or reviews
Three other systematic reviews gathering evidence for the most effective means of preventing caries/demineralisation during fixed orthodontic appliance treatment have been reported in the literature. Derks et al (Derks 2004) examined all preventive measures for preventing demineralisation ‐ not just fluoride products. These review authors had to exclude many published studies as well, because of inappropriate research design or poor reporting and were unable to provide firm, evidence‐based recommendations as to the prevention of DLs during fixed orthodontic treatment.
A second systematic review (Chadwick 2005) investigated the effectiveness of topical fluorides used alone in preventing demineralisation during orthodontic treatment. These review authors included seven studies in their review; these studies, however, were excluded from our review, because the outcomes were not appropriate (DMFT/DMFS (decayed, missing, and filled teeth/surfaces)), or the participants were not examined immediately after removal of the fixed appliance(s). Although they suggest that according to their outcome measure (preventive fraction), some evidence shows that the addition of a topical fluoride preparation helps in the prevention of demineralisation during fixed orthodontic treatment, this conclusion must be viewed with caution, because these review authors were not able to calculate confidence intervals. We support their request that researchers design and report their studies using standard outcomes, so that in the future, data may be pooled and overall recommendations on preventive measures may be provided.
Rogers et al (Rogers 2010) included 10 studies in their systematic review investigating the effectiveness of fluoride‐containing bonding adhesives used in orthodontics to prevent demineralisation. Five of these studies were excluded from our review because they were not randomised, and a further three studies were excluded because data in the report were insufficient, and the study authors, when contacted, were unable to provide requested data. Rogers' conclusions are consistent with ours with regard to the design of trials and the quality of reporting and statistical analyses.
Wang 2013 included 20 studies (19 articles) in their review, which is written in Chinese and only includes data from Chinese studies. They included studies with quasi‐randomised designs and it is not clear if they included studies with a within‐person (split‐mouth) design and those not following patients for the full length of orthodontic treatment.
The following reviews were also examined: Höchli 2017; Lapenaite 2016; Lopatiene 2016; Nascimento 2016; Rahimi 2017; Sardana 2019a; Sardana 2019b; Tasios 2019. These reviews either investigated interventions other than fluoride to prevent DLs, such as casein phosphopeptide‐amorphous calcium phosphate (CCP‐ACP), treatment of DLs after the appliance was removed or included quasi‐ and non‐randomised studies, studies with short follow‐up or outcomes that are not particularly relevant to patients and clinicians. No new studies were identified from the references in these articles to include in this review.
Authors' conclusions
Implications for practice.
There was insufficient evidence of a difference from two clinical trials that professional application of fluoride varnish (7700 or 10,000 parts per million (ppm) fluoride) every six weeks to the teeth of patients wearing fixed orthodontic braces reduces the number of new demineralised lesions (DLs).
One study provides a low level of certainty that a 12,300 ppm fluoride foam professionally applied every two months, reduces the incidence of new DLs after fixed orthodontic treatment.
Evidence for the use of fluoride products at home by patients includes one trial, providing a low level of certainty that a high fluoride (5000 ppm) toothpaste used throughout orthodontic treatment with fixed appliances might reduce the number of patients with new DLs, compared to a conventional fluoride toothpaste.
Evidence is insufficient for review authors to recommend the use of fluoride‐containing materials to attached braces to the teeth or intraoral fluoride‐releasing devices. Such interventions, provided they sustain the release of fluoride, have the potential to be effective, as they reduce the requirement for patient adherence to their use.
The use of fluoride mouthrinses by patients/participants, in addition to fluoride toothpastes, has been found to be effective in reducing caries in non‐orthodontic patients. No direct evidence, however, from this review indicates that this combination of fluoride delivery is effective in reducing DLs during fixed orthodontic appliance treatment.
Implications for research.
More evidence is required before the most effective way of delivering fluoride to the orthodontic patient can be determined with confidence. In particular, fluoride delivery methods that do not require patient adherence should be studied. Adequately powered, appropriately masked, placebo‐controlled trials, with suitable randomisation, allocation concealment and masking of outcome assessment, are needed. A placebo‐only group, however, may be considered unethical. The use of factorial designs, whereby two or more experimental interventions are evaluated simultaneously allowing for the evaluation of possible interaction between the interventions, can be evaluated separately. Researchers should, however, be aware that increasing the number of arms in a trial will substantially increase the number of participants required to demonstrate a statistical difference between interventions.
The use of images to record the condition of the tooth before and after treatment should be encouraged. Images provide a permanent record, allowing before and after comparisons of the incidence and severity of DLs with proper assessor masking, error analysis and consensus measures. To provide a reproducible method of recording DLs using photographs, a standard technique is required, with thought given to reduction of flash reflection, magnification and drying of the teeth. Optical and fluorescent methods of providing a quantitative measurement of mineral loss might be useful if funding allows, but it is important that outcomes are clinically relevant and meaningful to patients and clinicians.
Finally, we would encourage researchers in this area to use more than one assessor when determining the presence or absence of new DLs. The assessment is to a certain extent subjective, open to interpretation and may lead to detection bias if only one opinion is obtained. We would also suggest that an assessment of the aesthetic impact of the DLs should be made. Some DLs, although present, are small, barely noticeable and will probably remineralise with time. Although every effort should be made to prevent these lesions from forming, their impact on the individual and the long‐term health of the dentition will probably be minimal. Studies ideally should assess patient‐centred outcomes, including the effect of DLs on quality of life, particularly six months or a year after treatment.
What's new
| Date | Event | Description |
|---|---|---|
| 13 March 2019 | New citation required and conclusions have changed | Changes to author byline. Review update including 7 new studies bringing the total to 10 included studies. Conclusions changed. |
| 1 February 2019 | New search has been performed | Searches updated to 1 February 2019. |
History
Protocol first published: Issue 3, 2002 Review first published: Issue 3, 2004
| Date | Event | Description |
|---|---|---|
| 3 December 2013 | New citation required and conclusions have changed | Changes to inclusion criteria, 3 parallel‐group studies added and 14 previously included studies now excluded. New methods implemented and 'Summary of findings' table added. Conclusions changed. |
| 1 May 2013 | New search has been performed | Searches updated to January 2013. |
Acknowledgements
Thanks are due to Helen Worthington (Cochrane Oral Health) for invaluable help with the statistics and to Sylvia Bickley and Anne Littlewood, past and present Information Specialist for Cochrane Oral Health, for carrying out the searches for the review, Janet Lear (Cochrane Oral Health) for organising the translations, and Luisa Fernandez Mauleffinch, Managing Editor for Cochrane Oral Health, for her assistance and for copy editing the review.
For help with the translations of foreign papers, our thanks go to Regina Mitezki (German), Luisa Fernandez Mauleffinch (Spanish), Dr Mikako Hayashi (Japanese) and Dr Chang Liu and Professor Chengge Hua (Chinese).
We would also like to thank the following investigators who replied to our requests for additional information about their trials: PA Banks (Fairfield General Hospital, Burnley), AJ Borislow (Albert Einstein Medical Center), JP Fricker (Westmead Centre Dental Clinical School), G Pauw (University of Ghent), JDB Featherstone (University of California at San Francisco), CR Mattick (University of Newcastle upon Tyne), L Mitchell (St Luke's Hospital, Bradford), B Øgaard (University of Oslo), RC Pascotto (State University of Maringa), M Persson (Umeå University), AL Sonis (Harvard School of Dental Medicine), C Stecksen‐Blicks (Umeå University), PJ Turner (University of Birmingham), S Twetman (Umeå University), N van der Kaaij (Academic Centre for Dentistry Amsterdam (ACTA)), M Sonesson (Malmö University) and H Jiang and M Du (Wuhan University).
We acknowledge the contribution of Suzy Vine, who assessed the eligibility of trials, extracted data and assessed the quality of the trials in the original version of this review; and of Susan Furness, who contacted authors, entered the data, carried out the statistical analysis and helped writing the review in the 2013 update of this review.
For their help as peer reviewers of the different versions of this review, we express our thanks to Jayne Harrison, Sylvia Bickley, Helen Worthington, Anne‐Marie Glenny, Lee Hooper, Richard Ellwood, Sue Higham, the late Aubrey Sheiham, Scott Deacon, Ruth Floate, Anne Littlewood, Phil Riley and Fang Hua.
Appendices
Appendix 1. Cochrane Oral Health's Trials Register search strategy
Cochrane Oral Health's Trials Register is available via the Cochrane Register of Studies. For information on how the register is compiled, see oralhealth.cochrane.org/trials
From December 2016, searches of the Cochrane Oral Health's Trials Register for this review were undertaken using the Cochrane Register of Studies and the search strategy below:
orthodontic*
(cariostatic* OR fluoride* OR naf OR "glass ionomer*" OR "cermet cement*" OR compomer* OR "composite resin*")
("dental enamel solubility" OR caries OR "dental fissures" OR demineriali* OR reminerali* OR decalcifi* OR "white spot*" or lesion*)
#1 AND #2 AND #3
Previous searches were undertaken using the Procite software, and the search strategy below:
(orthodontic* AND (cariostatic* OR fluoride* OR naf OR "glass ionomer*" OR "cermet cement*" OR compomer* OR "composite resin*") AND ("dental enamel solubility" OR caries OR "dental fissures" OR demineriali* OR reminerali* OR decalcifi* OR "white spot*" or lesion*))
Appendix 2. Cochrane Central Register of Controlled Trials (CENTRAL) search strategy
#1 MeSH descriptor Orthodontics explode all trees #2 orthodontic* #3 (#1 OR #2) #4 MeSH descriptor Sodium Fluoride explode all trees #5 MeSH descriptor Fluorides, Topical explode all trees #6 fluoride* #7 topical next fluoride* #8 NaF #9 MeSH descriptor Glass Ionomer Cements, this term only #10 glass next ionomer* #11 (#4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10) #12 MeSH descriptor Dental Enamel Solubility explode all trees #13 MeSH descriptor Tooth Demineralization explode all trees #14 reminerali* or deminerali* or decalcif* #15 white next spot* #16 (#12 OR #13 OR #14 OR #15) #17 (#3 AND #11 AND #16)
Appendix 3. MEDLINE Ovid search strategy
exp ORTHODONTICS/
orthodontic$.mp.
1or 2
exp SODIUM FLUORIDE/
exp FLUORIDES TOPICAL/
fluoride$.mp.
NaF.ti,ab.
Glass Ionomer Cements/
(glass adj ionomer$).mp.
or/4‐9
exp DENTAL ENAMEL SOLUBILITY/
TOOTH DEMINERALIZATION/
(reminerali$ or deminerali$ or decalcif$).mp.
((white adj spot$) or lesion$).mp.
11 or 12 or 13 or 14
3 and 10 and 15
This subject search was linked to the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials (RCTs) in MEDLINE: sensitivity‐ maximising version (2008 revision) as referenced in Chapter 6.4.11.1 and detailed in box 6.4.c of theCochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 (updated March 2011) (Lefebvre 2011).
randomized controlled trial.pt.
controlled clinical trial.pt.
randomized.ab.
placebo.ab.
drug therapy.fs.
randomly.ab.
trial.ab.
groups.ab.
or/1‐8
exp animals/ not humans.sh.
9 not 10
Appendix 4. Embase Ovid search strategy
exp ORTHODONTICS/
orthodontic$.mp.
1 or 2
exp SODIUM FLUORIDE/
exp FLUORIDES TOPICAL/
fluoride$.mp.
NaF.ti,ab.
Glass Ionomer Cements/
(glass adj ionomer$).mp.
or/4‐9
exp DENTAL ENAMEL SOLUBILITY/
TOOTH DEMINERALIZATION/
(reminerali$ or deminerali$ or decalcif$).mp.
((white adj spot$) or lesion$).mp.
or/11‐14
3 and 10 and 15
This subject search was linked to an adapted version of the Cochrane Centralised Search Project filter for identifying RCTs in Embase Ovid (see www.cochranelibrary.com/central/central‐creation for information:
Randomized controlled trial/
Controlled clinical study/
Random$.ti,ab.
randomization/
intermethod comparison/
placebo.ti,ab.
(compare or compared or comparison).ti.
((evaluated or evaluate or evaluating or assessed or assess) and (compare or compared or comparing or comparison)).ab.
(open adj label).ti,ab.
((double or single or doubly or singly) adj (blind or blinded or blindly)).ti,ab.
double blind procedure/
parallel group$1.ti,ab.
(crossover or cross over).ti,ab.
((assign$ or match or matched or allocation) adj5 (alternate or group$1 or intervention$1 or patient$1 or subject$1 or participant$1)).ti,ab.
(assigned or allocated).ti,ab.
(controlled adj7 (study or design or trial)).ti,ab.
(volunteer or volunteers).ti,ab.
trial.ti.
or/1‐18
(exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.)
19 not 20
Appendix 5. US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the WHO International Clinical Trials Registry Platform search strategy
orthodontic and fluoride
Data and analyses
Comparison 1. Professionally‐applied F varnish versus non‐F (placebo) varnish.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 2 | 405 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.14, 1.93] |
| 2 Number of participants with more severe DLs (scores 3 or 4 versus scores 1 or 2) | 1 | 148 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.22, 0.95] |
1.2. Analysis.
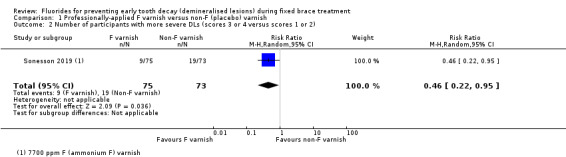
Comparison 1 Professionally‐applied F varnish versus non‐F (placebo) varnish, Outcome 2 Number of participants with more severe DLs (scores 3 or 4 versus scores 1 or 2).
Comparison 2. 12,500 ppm F (NaF/olaflur/dectaflur) gel versus 0 ppm F placebo gel.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 312 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.76, 1.27] |
Comparison 3. 12,300 ppm F APF foam versus 0 ppm F placebo foam.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 95 | Risk Ratio (M‐H, Random, 95% CI) | 0.26 [0.11, 0.57] |
Comparison 4. 5000 ppm F toothpaste versus 1450 ppm F toothpaste.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 380 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.46, 1.00] |
Comparison 5. 250 ppm F mouthrinse (100 ppm AmF/150 ppm NaF) versus 0 ppm F placebo mouthrinse.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 81 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.37, 1.17] |
Comparison 6. 1400 ppm/250 ppm F (AmF/SnF) versus 1400 ppm/250 ppm F (NaF) toothpaste/mouthrinse combinations.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 White spot index | 1 | 97 | Mean Difference (IV, Random, 95% CI) | ‐0.05 [‐0.10, 0.00] |
| 2 Visible plaque index | 1 | 97 | Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.18, ‐0.00] |
| 3 Gingival bleeding index | 1 | 97 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.15, 0.01] |
Comparison 7. Resin‐modified glass ionomer cement (RM‐GIC) versus light‐cured composite resin (LCC).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 173 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.69, 1.99] |
| 2 Number of participants with more severe DLs of aesthetic concern | 1 | 173 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [0.45, 3.12] |
7.2. Analysis.
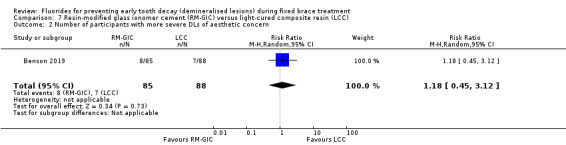
Comparison 7 Resin‐modified glass ionomer cement (RM‐GIC) versus light‐cured composite resin (LCC), Outcome 2 Number of participants with more severe DLs of aesthetic concern.
Comparison 8. Intraoral F‐releasing glass bead device versus F mouthrinse only.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants with new DLs | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | 1.51 [0.73, 3.10] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Benson 2019.
| Methods | Design: multicentre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participant, stratified on operator Setting: 6 centres, 2 dental teaching hospitals and 4 specialist orthodontic practices, UK and Republic of Ireland Recruiting period: February 2009 to March 2012 |
|
| Participants | Inclusion criteria: 11 years and older; full permanent dentition, requiring upper and lower fixed appliances; in good general health; oral hygiene was considered by the operator to be sufficient for fixed appliance treatment Exclusion criteria: patients with a cleft of the lip and/or palate; or who require orthognathic surgery Mean age at baseline, years: 15.5 years (SD 3.3 years, range 11 to 34) Number randomised: 210 (109 LCC, 101 RM‐GIC) Number evaluated: 173 (88 LCC, 85 RM‐GIC) Duration of treatment: 17.6 SD 7.1 months (17.3 SD 7.3 months RM‐GIC, 17.9 SD 7.0 months LCC) |
|
| Interventions | Comparison: resin‐modified glass ionomer cement (RM‐GIC ‐ GC Fuji ORTHO™ LC, GC Corp, Tokyo, Japan) versus light‐cured composite resin (LCC ‐ Transbond™ XT Light Cure Adhesive, 3M Unitek, Diegem, Belgium) for bonding orthodontic brackets | |
| Outcomes | Primary outcome: presence or absence of new DLs, on any teeth from the right second premolar to the left second premolar in both arches, assessed using the pre‐treatment and day of debond clinical photographic images. Minimum of 3 and maximum of 5 assessors Secondary outcomes: judgements about the aesthetic appearance of new DLs, as well as the number of first time bond failures (any bracket anterior to the first molars) during treatment, taken from clinical records |
|
| Notes | Funding source: Sheffield Hospitals Charitable Trust and GC Corporation donated a proportion of the Fuji ORTHO™ LC bonding adhesive | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisations using a computer generated random number sequence stratified on the operator to ensure that each operator was allocated the same number of participants in the 2 groups |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered opaque envelopes at each centre |
| Blinding ‐ Patients & Operators | Unclear risk | Blinding of patients and operators not possible because of the nature of the 2 materials. Not sure if this would affect the outcome, because it is not certain if or how participants or operators might change their behaviour as a result of knowing they were in one group or the other. The impact of this is unclear |
| Blinding ‐ Outcome assessors | Low risk | The examiners assessing the clinical photographic images were masked to group allocation |
| Incomplete outcome data addressed | Low risk | 4 participants dropped out as they moved away, but 9 were withdrawn from 2 centres because these centres failed to recruit a useful number of patients. 23 participants had missing final photographs and 1 had inadequate photographs. Dropouts and withdrawals equally distributed between the groups. The risk of bias was considered low as in the worse scenario (all those dropouts and withdrawals who were bonded with composite had new DLs) the risk ratio changed from 1.25 (95% CI 0.74 to 2.13) to 0.73 (95% CI 0.48 to 1.13) and the conclusions (no difference in the incidence of new DLs) would be the same |
| Free of selective reporting | Low risk | Relevant outcomes reported, including whether or not the DLs were considered unaesthetic and bond failures (not part of this review) |
| Free of other bias | Low risk | According to flow diagram all participants randomised received their allocated intervention. No protocol deviations were reported. Complete‐case analysis undertaken presumably (but not reported) based on the assumption that data for participants who withdrew or dropped out were missing at random (MAR), which seems reasonable. Stratification by operator meant that participants in 1 setting had an equal chance of being in either group. This should account for confounders, such as difference in treatment materials and methods by different operators and environmental factors, such as level of fluoride in water supply (e.g. Cork is fluoridated) |
He 2010.
| Methods | Design: single centre, randomised controlled trial, assessing superiority with 3 parallel groups Unit of randomisation: participant Setting: 1 centre (Department of Stomatology, the Fourth People's Hospital of Shenzhen, Shenzhen City, China) Recruiting period: June 2007 to September 2009 |
|
| Participants | Inclusion criteria: from translation "with fixed orthodontic" ‐ but need to check they were recruited and allocated before the fixed was placed, although mean duration of experimental period would suggest that this was the case Exclusion criteria: from translation: "Participants with dental hard tissue well developed, without tetracycline teeth or dental fluorosis, and without cavities or fillings on the buccal surface" Mean age at baseline, years: mean age 14.3 years (range 12 to 17 years, no SD provided) Number randomised: 75 (25 in each group) Number evaluated: 75 (intention‐to‐treat) Duration of treatment: Group A: mean 21.3 months, Group B: mean 22.7 months, Group C: mean 21.6 months (range 18 to 24 months; no SD was reported) |
|
| Interventions | Group A (experimental group): fluor protector (Vivadent, Swiss) per 3 months by the dentist + Bass method of toothbrushing Group B (alternative intervention group): tooth mousse (GC, Japan) (complex of casein phosphopeptide amorphous calcium phosphate, CPP‐ACP) per night by the participant's self + Bass method of toothbrushing Group C (placebo group): Bass method of toothbrushing |
|
| Outcomes | Primary and secondary outcomes not explicitly stated and no justification of sample size therefore primary outcome cannot be inferred Measured DLs using the Enamel Demineralization Index (EDI) devised by Mizrahi (1982) recorded using photographs Abstract states "After finishing the orthodontic treatment, photos were taken under the same condition [sic], then the degree of enamels [sic] demineralization was examined." This suggests that photographs were taken before and after treatment, but not clear if they were compared and only new DLs scores | |
| Notes | Funding source: abstract states "Supported by Research Fund of Bureau of Science and Technology of Futian District Shenzhen City (Grant Number FTWS056)
No sample size calculation
Not reported whether participants used additional oral measures, such as toothpastes with or without fluoride A message, asking for additional information, sent to the first author contact details in the report (He Wen‐dan hewendan@yahoo.com.cn) on 8 August 2018, but was returned as undeliverable |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Translation: "In the order of treatment time, participants were divided randomly into 3 groups." No details of method of randomisation, stratification and how they achieved equal numbers in the 2 groups |
| Allocation concealment (selection bias) | Unclear risk | No details |
| Blinding ‐ Patients & Operators | Unclear risk | Participants received different preventative regimens, at different times, therefore neither participants or operators could be masked. The impact of this is unclear |
| Blinding ‐ Outcome assessors | Unclear risk | Translation: "EDI was measured by our research member(s) who was/were blind to the treatment." Not clear how many assessors were involved |
| Incomplete outcome data addressed | Low risk | No dropouts (quite unusual over the more than 2‐year period of the study) |
| Free of selective reporting | Unclear risk | The definition of incidence is unclear (difference between start and finish ‐ new DLs or just at the finish?). Also report "the incidence of teeth's enamel calcification [sic]" and do not state how they took into account the clustering of teeth within the mouth |
| Free of other bias | Unclear risk | Not reported how many operators were involved in the study or whether participants used additional oral measures, such as toothpastes with or without fluoride |
Jiang 2013.
| Methods | Design: single centre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participant, no reported stratification Setting: 1 centre, Orthodontic Department Hospital of Stomatology, Wuham University, China Recruiting period: July 2007 to December 2010 |
|
| Participants | Inclusion criteria: 10 and 20 years old, satisfactory general health, requiring fixed orthodontic treatment for at least 6 months Exclusion criteria: periodontal probing depth greater than 3 mm; history of long‐term use of antibiotics; active caries; enamel hypoplasia, dental fluorosis, or tetracycline‐stained teeth Mean age at baseline, years: 13.5 SD 2.2 years (range not reported) Number randomised: 100 (50 experimental foam, 50 control foam) Number evaluated: 95 (48 experimental foam, 47 control foam) Duration of treatment: 18 months (SD 3.2, range 10.6 to 32 months) |
|
| Interventions | Comparison: 12,300 ppm F acidulated phosphate fluoride (APF) foam (Dentology, Suntech Medical Appliances Co, Ltd, Beijing, China) versus fluoride‐free (0 ppm F) foam prepared by the same company. Professionally applied in trays for 4 minutes every 2 months | |
| Outcomes | Primary outcomes: 2 reported ‐ incidence of 'WSLs' (per cent) and the increment of 'WSLs' scores during orthodontic treatment; however sample size calculation based on detecting a mean difference of 2.0 'WSL' increments (Gorelick index) Secondary outcome: distribution of 'WSLs' score (per cent) in both the 1.23 per cent APF foam and placebo groups after debonding Assessed by 1 calibrated and masked examiner before and on day of debond |
|
| Notes | Funding source: National Key Technologies R&D Program of the Eleventh‐five Year Plan, the Ministry of Science and Technology of China, Beijing (no 2007BAI18B01) Data presented for teeth not for participants on report but clarification obtained from study authors Corresponding authors (Baojun Tai ‐ taibaojin@126.com, Minquan Du ‐ minquandu@163.com) contacted 8 August 2018 for data on participant with new DLs and to clarify aspects of methodology, including method of randomisation and allocation concealment. No response so follow‐up e‐mail on 22 January 2019 and response eventually received 5 September 2019 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The report states that random sequence was generated using a "table of random numbers", but it was not clear how they achieved equal numbers in the 2 groups. The authors were contacted and replied that they used a block method |
| Allocation concealment (selection bias) | Unclear risk | The reports states that the "subjects, clinicians, and examiners were blind to group allocations" however the exact method of allocation concealment was unclear. The authors were contacted and replied that "No particular methods were used to conceal the random sequence", so this is still unclear |
| Blinding ‐ Patients & Operators | Low risk | Both foams had the same consistency, appearance and odour stored in same bottles labelled A or B |
| Blinding ‐ Outcome assessors | Unclear risk | Examiner blind to group allocation. Only 1 assessor undertook clinical assessments. Report does describe that the examiner was involved in an "initial calibration", but not clear if this was maintained for the full length of the trial. Intraexaminer agreement assessed on 10 patients (kappa 0.75), but better to have multiple assessors to reach a consensus |
| Incomplete outcome data addressed | Low risk | Low number of reported dropouts and withdrawals (5 out of 100 participants randomised, 5%) |
| Free of selective reporting | Low risk | Unclear if Table 2 refers to proportion of participants affected or proportions of teeth affected. The authors were contacted and have supplied the data for the numbers of participants with at least 1 new DL |
| Free of other bias | Unclear risk | According to flow diagram (Figure 1) 10 participants were excluded between 'enrolment' and randomisation, but it is not clear why. No protocol deviations reported. Complete‐case analysis undertaken presumably (but not reported) based on the assumption that data for participants who withdrew or dropped out were missing at random (MAR), which seems reasonable. Unclear how many operators were involved Participants were "instructed to brush their teeth twice daily with the toothbrushes (V type) provided" and "forbidden from using any other oral hygiene measures or using fluoride in addition to fluoride toothpaste." Suggests they were allowed to use fluoride toothpaste (1450 ppm?), but no other mouthrinse. Not clear if GDP provided topical fluoride. Fluoride concentration in the drinking water was low (0.1 to 0.3 ppm), but participants were all from the same district anyway, so randomisation should account for this potential confounder |
Jost‐Brinkman 2017.
| Methods | Design: randomised, placebo‐controlled, parallel‐group trial Unit of randomisation: participant Setting: 2 centres (Berlin, Germany and Jerusalem, Israel) Recruiting period: not stated |
|
| Participants | Inclusion criteria: healthy; aged 10 years or older; 10 teeth or more to be bonded with fixed orthodontic appliances labially; highly effective birth control for girls and women of child‐bearing age. The reason for the latter inclusion criteria is unclear Exclusion criteria: known allergy to one of the components of the test products; disabled and unable to brush their own teeth; pathological desquamation changes; known pregnancy; breastfeeding; eating disorders; enamel or dentine disorder; participation in another clinical trial within 30 days Screened: 321; randomised: 320 (additional report states 321 – checking with study authors); ITT analysis n = 312 Mean age at baseline: 16 years (SD 7) intervention group; 16 years (SD 6) placebo control Slightly higher proportion of males in intervention group (50.6% versus 42.9%) and most were of Caucasian origin (88.5% versus 91.7%) Mean treatment duration: 16.6 months (SD 7.3; range 1.3 to 32.5 months) |
|
| Interventions | Comparison: amine fluoride‐containing gel (Elmex® gel) (1.25% fluoride, including 1% fluoride from NaF and 0.25% fluoride from olaflur/dectaflur, approximately 12,500 ppm; 10% solution pH 4.3‐5.3) versus placebo gel (comparator product formulation number 447/2221; 10% solution pH 6.5‐7.5) pHs were different, but presume the 2 gels were identical in taste, colour; consistency and packing Home gel brushing, once per week, approximately 0.5 g gel Tray application 4 times per year, approximately 8 g gel Study products manufactured by Colgate were delivered to the study site by GABA GmbH Lörrach (Germany) or TEVA Pharmaceuticals, Netanya (Israel) Participants were reminded by SMS or e‐mail once a week, to brush their teeth with their gel and to bring along their study products to each visit (normally every 6 weeks) for weighing |
|
| Outcomes | Primary outcome: time and frequency of visually detected DLs according to modified DMFS (D1 'white spot' < 2 mm; D2 'white spot' > 2 mm; D3 cavitation; D4 cavitation deep into dentine; M missing due to caries; F filled) and bitewing radiographs. Occurrence of a DL was defined as: cavitation; any DL exceeding 2 mm in any direction; new or progressing approximal lesion detectable by bitewing radiographs; more than 4 teeth affected with DLs of any size Secondary outcomes: frequency of DL (endpoints, based on patients and teeth); time of occurrence of DL (endpoints); mineral loss according to QLF findings; changes in the caries index according to modified DMFS; radiographic findings on bitewings during the study; approximal plaque index (API) At baseline (before orthodontic bonding), each participant underwent examination ‐ visual, radiographic bitewings, QLF measurements. The final visit took place at the end of the 30‐month study or after debonding |
|
| Notes | Funding: Colgate‐Palmolive Europe Sàrl, (Colgate) Sample size calculation based on a time‐to‐event analysis for the occurrence of new DLs, testing the following hypothesis with a log‐rank test: DLs occur earlier in patients using the placebo gel (without fluoride) than in patients using the fluoride gel (Elmex® gel) Paul‐Georg Jost‐Brinkmann (Paul‐G.Jost‐Brinkmann@charite.de) contacted 19 December 2018 to clarify some issues (Were the assessments carried out on the day of debond? If not how long after? Who carried out these assessments? Were they calibrated? Any reproducibility assessments undertaken?). No reply so follow‐up e‐mail sent 22 January 2019 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The study participants were randomly allocated to one of the two study groups" Comment: no details of method of random sequence generation or if a block design or stratification was used |
| Allocation concealment (selection bias) | Low risk | Investigator "received a sealed random‐code envelope for each individual subject number." The sealed envelopes were to be opened only in case of emergency when knowledge of the actual treatment was medically necessary |
| Blinding ‐ Patients & Operators | Low risk | Quote: "Patients, investigators, study monitors, study coordinators, and data managers were unaware of the study product being administered" |
| Blinding ‐ Outcome assessors | Unclear risk | Quote: "Patients, investigators, study monitors, study coordinators, and data managers were unaware of the study product being administered" Comment: unclear who and how many undertook the clinical assessments, whether they were calibrated and whether any assessment of reproducibility was undertaken |
| Incomplete outcome data addressed | Unclear risk | Screened: 321; randomised: 320 (additional report states 321 – checking with study author); eligible for the safety analysis: 318 ITT analysis (all randomised patients who received at least 1 dose of the study product and had at least 1 assessment of efficacy: n = 312 (Elmex® gel: n = 156, placebo gel: n = 156) ‐ not clear why 8 or 9 were excluded from those randomised (no flow diagram); per‐protocol analysis (all randomised patients who satisfied the following criteria: no missing data for the primary efficacy variable; no major protocol violations) n = 265 (Elmex® gel: n = 135, placebo: n = 130) Authors state that "In 15 patients in the Elmex® gel group and 15 patients in the placebo group, non‐compliance with the study requirements led to the premature discontinuation of the study (ITT set)", but only 8 were excluded according to the above figures (checking with study authors). They go on to state that "only a small number of patients (n = 5; Elmex®: n = 1; placebo: n = 4) were excluded from the PP analysis because of non‐compliance" and "The main reason for excluding patients from the PP analysis set was the use of disallowed concomitant medications, both in the Elmex® gel and placebo gel groups" The Statistical Summary Tables ITT documentation (Appendix 12.5 ‐ requested) provides the complete listing of individual reasons for exclusion from the per‐protocol analysis |
| Free of selective reporting | Low risk | Thorough report into complete list of adverse events occurring to participants during the study. Most were nothing to do with taking part in the trial |
| Free of other bias | Unclear risk | Protocol deviation reported for the analysis, as they examined data for number of teeth rather than number of participants. Unclear how many operators were involved in each centre, but unlikely to be a significant risk of bias. If they had stratified the randomisation by setting this would have meant that participants in 1 setting had an equal chance of being in either group. This would have accounted for confounders, such as difference in treatment materials, methods by different operators and other sources of fluoride from diet or water. Participants could use their own toothpaste, but not clear if GDP was asked to not provide additional topical fluoride |
Luther 2005.
| Methods | Trial design: single centre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participant, no stratification reported Setting: 1 centre, teaching hospital, Leeds UK Recruitment period: December 1998 to December 1999 |
|
| Participants | Inclusion criteria: participants with upper incisors and canines developing and at least 3 upper permanent incisors and 1 upper permanent canine erupted, prior to commencement of orthodontic treatment with fixed upper appliances 40 female/28 male (numbers incorrect as 70 were randomised) Exclusion criteria: participants with grossly damaged, restored or defective upper permanent canines or incisors, participants living in areas with fluoridated water supply, physically or mentally handicapped individuals, those with comorbidities or requiring antibiotic cover and pregnant or nursing females Mean age at baseline, years: 15.7 years (range 11 to 45) Number randomised: 70 (34 fluoride‐releasing glass bead and 36 fluoride rinse) Number evaluated: 37 (18 fluoride‐releasing glass bead and 19 fluoride rinse) Duration of treatment: approximately 19 months (recruitment ended December 1999; final data collection September 2002) |
|
| Interventions | Comparison: fluoride‐releasing glass beads versus fluoride mouthrinse Group A (n = 18): fluoride‐releasing glass bead (containing 13.3% F) attached to appliance Group B (n = 19): fluoride rinse (Endekay 0.05% NaF). Participants instructed to use 5 drops in 10 ml of water and to rinse once daily |
|
| Outcomes | Primary outcome: not explicit, but did assess presence or absence of new DLs assessed from before and after cross‐polarised images of 6 upper anterior teeth. 1 masked assessor using image analysis Secondary outcomes: not explicit, but measured salivary fluoride levels |
|
| Notes | Funding source: BDA Research Foundation Shirley Glasstone Hughes Memorial Prize Fund and the Listerine Preventive Care Award Background exposure to fluoride not reported: unclear whether participants used fluoride toothpaste Power calculation reported that 28 participants/group would be needed to show the expected 75% difference (high); it was planned to recruit 35 per group to allow for dropouts Large numbers of participants both withdrawing or dropping out (total 14: 6 control, 8 experimental), as well as insufficient data for analysis (total 19: 11 control, 8 experimental). Null findings should be interpreted with caution, as investigators lost so many in their sample, which means that it is likely that this study lacks statistical power, hence no conclusion overall can be made about this intervention |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A random number table was generated on an Excel spreadsheet by the trial's statistical advisor" |
| Allocation concealment (selection bias) | Low risk | Quote: "Each time a patient agreed to take part in the study, a dental nurse who was not involved in the running of the study accessed the concealed table and crossed off the next number, informing the operator of the treatment to be used i.e. whether the patient had been allocated to the fluoride rinse or FGB group" |
| Blinding ‐ Patients & Operators | Unclear risk | Not possible to blind participants or operators to allocated intervention. The impact of this is unclear |
| Blinding ‐ Outcome assessors | Low risk | Quote: "Analysis was undertaken blind by one operator, who was unaware of which group the teeth being analysed came from" |
| Incomplete outcome data addressed | High risk | 14 participants (8 fluoride‐releasing glass bead and 6 mouthrinse) dropped out ‐ reasons not given. Further 19 (8 fluoride‐releasing glass bead and 11 mouthrinse) excluded from analysis because of insufficient data, and reasons not explained. 47% of randomised participants not included in the analysis. High rate of breakage of fluoride‐releasing glass beads. Substantial risk of attrition bias due to dropouts and withdrawals (33 out of 70 randomised; 47%) |
| Free of selective reporting | Unclear risk | Numbers of participants and teeth with DLs reported at the beginning and at the end of the trial, but denominators were unclear. No indication of mean size of lesions in each group. Salivary fluoride levels not reported |
| Free of other bias | Unclear risk | Number of breakages of fluoride‐releasing glass beads reported, but no indication of level of compliance in fluoride rinse group. No information on duration of trial and therefore duration of exposure to fluoride in each group |
Ogaard 2006.
| Methods | Trial design: 2‐centre, parallel‐group randomised controlled trial Unit of randomisation: participant, no stratification Setting: 2 orthodontic clinics of Falköping and Lidköping in Sweden Recruitment period: starting orthodontic treatment in 1999, last patient debonded November 2003 |
|
| Participants | Inclusion criteria: participants were those starting orthodontic treatment in 1999 with fixed appliances in both arches Exclusion criteria: none stated Age at baseline: mean 14.5 years Number randomised: 115 Number evaluated: 97 (numbers per group not stated) Duration of treatment: "average approximately 1.5 years" |
|
| Interventions | Comparison: 2 different fluoride toothpastes and mouthrinses Group A (n = 50): participants were instructed to brush twice daily with toothpaste containing amine fluoride and stannous fluoride combination (AmF/SnF2 140 ppm, pH 4.5) and to rinse every evening after toothbrushing with a solution containing amine fluoride and stannous fluoride Group B (n = 47): participants were instructed to brush twice daily with toothpaste containing neutral sodium fluoride (NaF 1400 ppm, pH 6.7) and to rinse every evening after toothbrushing with a solution containing NaF (250 ppm, pH 6.3) Fluoride treatments were continued for the whole duration of orthodontic treatment with fixed appliances |
|
| Outcomes | 'White spot lesion' index, visible plaque index, gingival bleeding index, measured at baseline and at debonding | |
| Notes | Funding source: the study was supported by GABA International, Basel, Switzerland Background exposure to fluoride: not reported Power calculation: not reported Corresponding author contacted (Bjørn Øgaard ‐ bogaard@odont.uio.no) contacted by e‐mail (14 August 2018) for clarification about a number of issues. Replied 24 September 2018 "Thank you for your interest in the cited study about white spot lesion development in orthodontic patients. I am sorry for the late response, but I have almost retired. The study was carried out in Sweden for more than 15 years ago. The investigator in charge died two years ago, and the statistician has retired many years ago. However, I will try to answer your questions below." Follow‐up message on 22 January 2019 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "allocated to two groups at bonding according to a randomized table" Comment: assumed this refers to random number table, but it is not clear how they achieved equal numbers in each group |
| Allocation concealment (selection bias) | Unclear risk | Not described Comment: assumed not done |
| Blinding ‐ Patients & Operators | Unclear risk | Quote: "The toothpaste tubes/bottles were similar and coded either A or B. The colour and taste of the toothpastes and the rinsing solutions were as close to identical as possible" Comment: the above suggests they were not identical and operator and/or participant might be able to guess which group they were allocated to |
| Blinding ‐ Outcome assessors | Unclear risk | Quote: "Neither the subjects nor the research team were informed about which group each participant belonged to" Comment: the report indicates that clinical assessments and colour photographs were obtained prior to bonding and at debond, but does not state that the photographs were used in the assessment. No details about who carried out the assessments or whether they were calibrated. No repeatability or reproducibility assessments reported |
| Incomplete outcome data addressed | Unclear risk | No flow diagram. Report that of the 115 patients "initially invited to participate" 18 "did not complete treatment according to the requirements in the protocol in 2003." Not stated which groups they were from or reasons for withdrawal or dropout apart from "mainly due to moving." Moderate risk of attrition bias for demineralisation assessments due to dropouts and withdrawals (16%). Unable to calculate the risk ratios because of the type of data presented, therefore the impact of the withdrawals and dropouts is unclear |
| Free of selective reporting | Unclear risk | Only data on mean changes in 'white spot index' before and after reported. No data on number of participants with new DLs in each group |
| Free of other bias | Low risk | Presumably the orthodontic clinics were public facilities and not private practices. Unclear how many operators were involved in each centre. If they had stratified the randomisation by setting or operator this would have meant that participants in 1 setting had an equal chance of being in either group. This would have accounted for confounders, such as difference in treatment materials and methods by different operators. Both groups were supplied with the same type of toothbrush (GABA). Not clear if participants were encouraged to use any other fluoridated products or GDP informed about not applying fluoride. Environmental factors, such as level of fluoride in water supply should not be a factor as Sweden has a low level of public water fluoridation, which was reported (less than 0.3 ppm) |
Sonesson 2014.
| Methods | Trial design: multicentre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participants, no stratification reported Setting: 5 centres, 4 public specialist clinics and 1 university teaching hospital in southern Sweden Recruitment period: started "2008" and "trial was completed in May 2012." Unclear what the recruitment period was |
|
| Participants | Inclusion criteria: aged 11 to 16 years, 2‐arch pre‐adjusted edgewise fixed appliances, treatment duration at least 1 year Exclusion criteria: participants with special needs, such as chronic diseases and/or disabilities Mean age at baseline, years: test group (high fluoride (HF)) 14.8, SD 1.7 years; control (conventional adult fluoride (CF)) 14.6, SD 1.7 years Number randomised: 424 (211 HF; 213 CF) Number evaluated: 380 (188 HF; 192 CF) Duration of treatment: 1.8 years (SD 0.53) |
|
| Interventions | Comparison: high fluoride toothpaste (5000 ppm) versus conventional adult fluoride toothpaste (1450 ppm) used at home by participants | |
| Outcomes | Quote: "Primary and secondary outcomes were the prevalence and incidence of WSL at time of debonding" Sample size based on difference in proportion of participants with new DLs at debonding, so this is primary outcome and therefore measuring incidence Secondary outcome: severity according to Gorelick Index Assessed from projected pre and post‐treatment digital photographic images, by 2 masked "experienced and calibrated orthodontists." Disagreements resolved by re‐examination of photographs and discussion. Agreement assessed using 50 participants images after 1 month (interexaminer kappa statistic 0.70, intraexaminer kappa 0.80) |
|
| Notes | Funding source: the Swedish Patent Revenue Fund 2007; toothpaste and toothbrushes donated by Colgate‐Palmolive | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computer generating" Comment: no stratification or block allocation mentioned |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered opaque envelopes supplied by "an independent person, not involved in the treatments or data analyses" |
| Blinding ‐ Patients & Operators | Unclear risk | Toothpaste supplied by Colgate‐Palmolive and described as same flavour and consistency; however the study was not truly triple‐blind. Quote (Discussion page 681): "...we were unable to secure a true double‐blind performance of the study because it was not possible for the manufacturer to produce identical packing of the two different toothpastes. Even if the participating subjects were not informed on the different toothpaste characteristics, it was not unlikely that they became aware of their assignment during the study period, especially since the diameter of the tube openings differed" |
| Blinding ‐ Outcome assessors | Low risk | Assessors were "not involved in treatment of patients and blinded for group assignment" |
| Incomplete outcome data addressed | Unclear risk | 44 out of 424 (10%) randomised were dropouts or withdrawals and reasons were included in flow diagram. However, the authors report that 18 participants (HF 10; CF 8) "did not comply with the study protocol" and were excluded from the analysis, but the definition of non‐compliance is unclear. Consequently a per‐protocol rather than an intention‐to‐treat analysis was undertaken. In the worse scenario (all participants in the experimental group who dropped out or withdrew had new DLs) the risk ratio changes from 0.68 (95% CI 0.46 to 1.00) to 1.02 (95% CI 0.74 to 1.41) |
| Free of selective reporting | Low risk | Relevant outcomes reported. Measure of severity was Gorelick Index, which is relatively crude. The "vast majority" of new lesions (98.8% HF; 97.7% CF) as "slight white spot formation (thin rim)" and therefore probably not an aesthetic problem. |
| Free of other bias | Low risk | Unclear how many operators were involved in each centre, but multiple operators makes this a 'real world' study. It might have been better to have stratified the randomisation by setting or operator, which would have meant that participants in 1 setting had an equal chance of being in either group. This would have accounted for confounders, such as difference in treatment materials and methods by different operators. Not clear if participants were encouraged to use any other fluoridated products. Environmental factors, such as level of fluoride in water supply should not be factor as Sweden has a low level of public water fluoridation, which was reported (less than 0.3 ppm) |
Sonesson 2019.
| Methods | Trial design: 3‐centre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participants, stratified on centre Setting: 3 orthodontic specialist clinics (1 university, 2 private) in Scania region, Sweden Recruitment period: January 2015 to November 2017 |
|
| Participants | Inclusion criteria: scheduled treatment with direct bonded fixed maxillary pre‐adjusted edgewise appliances during a period of at least 12 months Exclusion criteria: severe chronic conditions such as asthma and allergy, neuropsychiatric disorders and regular use of oral antiseptics and previous fixed orthodontic appliance treatment Mean age at baseline, years: test group (high fluoride (HF)) 14.1 years, SD 1.7, range 11.3 to 18.7 years; control (conventional adult fluoride (CF)) 13.8 years, SD 1.8, range 10.1 to 18.0 years Number randomised: 166 (85 HF; 81 CF) Number evaluated: 148 (75 HF; 73 CF) Duration of treatment: 1.7 years (SD 0.5) |
|
| Interventions | Comparison: high fluoride varnish (7700 ppm ammonium fluoride dissolved in ethanol, water and acrylate polymer ‐ Fluor Protector S, Ivoclar Vivadent, Liechtenstein) versus no fluoride varnish All patients seen every 6th week for wire adjustment. Test or control varnish applied by clinical staff at the end of each visit with a small brush around the base of the brackets in the upper arch. This was left to dry for 1 minute and participants instructed not to eat or drink within 60 minutes. Participants were encouraged to brush twice a day with a 1450 ppm fluoride toothpaste. No additional fluoride recommended |
|
| Outcomes | Primary outcome: "prevalence and severity" of DLs, but sample size based on detecting a 15% difference between the 2 groups (which difference not specifically stated, but presumably number of DLs). Pre and post‐treatment photos projected on a screen and scored by 2 "experienced and calibrated specialists" using Gorelick Index (reported data for before and after so incidence or new DLs assessed). When in doubt lower score give, disagreements resolved through consensus (presumably between 2 assessors) Secondary outcomes: severity of DLs |
|
| Notes | Funding from "author's institutions and partly supported by Ivocalr Vivadent AG" who provided the varnishes Water is not fluoridated in Sweden |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated random sequence, blocks of 15, but on further enquiry author replied that the centres recruited in blocks of 30 (1 centre 90, 1 centre 60, 1 centre 30 ‐ 15 test and 15 controls) |
| Allocation concealment (selection bias) | Low risk | Not in the report, but authors replied "consecutive numbers" and the "list was secured by .....a person not involved in the clinical part of the trial" |
| Blinding ‐ Patients & Operators | Low risk | Taste, colour, handling and packing the same for both varnishes therefore neither participant or clinician were aware of group allocation |
| Blinding ‐ Outcome assessors | Low risk | Scoring done on photographs and the lead study author confirmed that the assessors were not involved in treating the participants and were masked to group allocation |
| Incomplete outcome data addressed | Low risk | All accounted for |
| Free of selective reporting | Low risk | Flow diagram provided and accounts for withdrawals and dropouts reported (10/85 or 12% experimental; 8/81 or 10% controls). Reasons given and similar in each group. Assuming the worse scenario (all participants in experimental group who dropped out or withdrew had new DLs) this would change the risk ratio from 0.96 (95% CI 0.65 to 1.41) to 1.34 (95% CI 0.97 to 1.86) and would not change the interpretation of the findings |
| Free of other bias | Low risk | According to the flow diagram all participants randomised received their allocated intervention. No protocol deviations reported Complete‐case analysis undertaken presumably (but not reported) based on the assumption that data for participants who withdrew or dropped out were missing at random (MAR), which seems reasonable. Unclear how many operators were involved in each site, but multiple operators makes this a 'real‐world' study. Randomisation stratified by site means that participants in 1 site had an equal chance of being in either group |
Stecksén‐Blicks 2007.
| Methods | Trial design: 2‐centre, randomised controlled trial, assessing superiority with 2 parallel groups Unit of randomisation: participants, no stratification reported Setting: 2 public orthodontic clinics at Skelleftea and Lycksele, northern Sweden Recruitment period: not stated |
|
| Participants | Inclusion criteria: children 12 to 15 years of age scheduled for maxillary treatment with fixed orthodontic appliances for an expected duration of at least 6 months Exclusion criteria: none stated Mean age at baseline, years: 14.3 SD 1.6 years Number randomised: 273 (137 fluoride varnish; 136 placebo varnish) Number evaluated: 257 (132 fluoride varnish; 125 placebo varnish) Duration of treatment: not given, but mean number of applications of varnish was 10, and assuming they were seen every 6 weeks, the mean duration was 60 weeks or just over 1 year (which is quite short) |
|
| Interventions | Comparison: fluoride varnish (Fluor Protector) versus placebo varnish Group A (n = 137): Fluor Protector varnish (0.1% F difluorosilane in polyurethane base, which is 1000 ppm fluoride in a homogeneous solution; however, according to the manufacturer's literature, after the varnish has dried, the concentration is approximately 10 times higher) applied after bonding and at each check‐up (approximately every 6 weeks) until debonding Group B (n = 136): placebo varnish, identical in appearance to active, applied after bonding and at the end of each check‐up (every 6 weeks) until debonding In both groups, after removal of visible plaque with an explorer, 0.2 to 0.3 ml varnish was applied around the bracket bases in a thin layer with a minibrush and was allowed to dry for 2 minutes. Participants were instructed to avoid all eating and drinking for 2 hours and to not brush teeth until the following day All children strongly advised to brush teeth with 1000 to 1500 ppm fluoride toothpaste at least twice daily Fluoride in piped drinking water in these communities was < 0.2 ppm |
|
| Outcomes | Primary outcome: reported as "incidence or progression" or DLs. Sample size based on a 20% reduction in the incidence therefore this is the presumably the primary outcome and severity (as judged by Gorelick Index) is a secondary outcome. Before and after clinical photographs assessed for presence and severity of DLs by 2 "experienced and calibrated judges." Disagreements resolved and consensus achieved through discussion. Interexaminer agreement (kappa statistic 0.69) and intraexaminer agreement (kappa 0.77) determined by repeat assessments on random 50 participant records after 1 month | |
| Notes | Funding source: grants from the County Council of Vasterbotten and Swedish Dental Society, with varnishes supplied by Ivoclar Vivadent and brackets by 3M Unitek | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (author): "The patients were assigned to one of the two groups on the basis of odd and even numbers from a dice" Comment: the corresponding author was asked how investigators obtained equal numbers in all groups but does not seem to have answered this |
| Allocation concealment (selection bias) | Low risk | Quote (author): "The study was coordinated from the Department of Paediatric Dentistry and the randomization was performed there by an independent technician not involved in the clinical work and collection of data" Comment: presumably remote allocation through telephone, but author has not confirmed |
| Blinding ‐ Patients & Operators | Low risk | Quote (author): "The placebo varnish applied had an identical composition but without fluoride. Both varnishes were uncoloured and obtained from the producer in identical bottles coded by colour. Neither clinicians nor patients knew whether they were treated with fluoride or placebo varnish" Comment: the study was double‐blind |
| Blinding ‐ Outcome assessors | Low risk | The two "experienced and calibrated" judges who scored the photographs for presence/absence and severity of DLs "were not involved in the treatment of the patients and blinded for group assignment" |
| Incomplete outcome data addressed | Low risk | Flow diagram provided and withdrawals and dropouts reported (5/137 or 4% experimental; 11/136 or 8% control). Reasons given and similar in each group. Assuming the worse scenario (all participants in experimental group who dropped out or withdrew had new DLs) this would change the risk ratio from 0.27 (95% CI 0.13 to 0.54) to 0.39 (95% CI 0.22 to 0.71) and would not change the interpretation of the findings |
| Free of selective reporting | Low risk | Planned outcome was 'white spot lesions' at debonding in each group. Reported as percentage of prevalence with P value for difference between groups. According to Figure 2 there were a very low proportion (< 3%) of Gorelick Index scores of 3 ('Excessive white spot formation (thicker bands)'). The majority were scored 2 ('Slight white spot formation (thin rim)'), so the aesthetic impact is unclear |
| Free of other bias | Low risk | According to the flow diagram all participants randomised received their allocated intervention. No protocol deviations reported Complete‐case analysis undertaken presumably (but not reported) based on the assumption that data for participants who withdrew or dropped out were missing at random (MAR), which seems reasonable. Unclear how many operators were involved in each centre, but multiple operators makes this a 'real‐world' study. If they had stratified the randomisation by setting or operator this would have meant that participants in 1 setting had an equal chance of being in either group. This would have accounted for confounders, such as difference in treatment materials and methods by different operators. Not clear if participants were encouraged to use any other fluoridated products. Environmental factors, such as level of fluoride in water supply should not be factor as Sweden has a low level of public water fluoridation, which was reported (less than 0.3 ppm) |
van der Kaaij 2015.
| Methods | Design: single centre, randomised controlled trial, assessing superiority with 2 parallel groups Setting: 1 teaching hospital orthodontic department, Amsterdam, the Netherlands Recruitment period: April 2009 to January 2011 |
|
| Participants | Inclusion criteria: aged 10 to 18 years, good general health, no medications, "no demineralizations in need of restorations present at a buccal surface." Go on to state that all "received fixed appliances (Roth Ovation) in both jaws" Exclusion criteria: none stated Mean age at baseline, years: 13.3 years (range 10.0 to 16.6): fluoride 13.1 years (range 10.0 to 16.6), placebo 13.6 years (range 11.7 to 16.5) Number randomised: 120 (61 fluoride; 59 placebo) Number analysed: 81 (36 fluoride; 45 placebo) Duration of treatment: 24.5 months (SD 5.5) |
|
| Interventions | Comparison: 250 ppm fluoride mouthrinse (100 ppm amine F; 150 ppm NaF) versus placebo mouthrinse (0 ppm F) used at home by participants | |
| Outcomes | Primary outcome: number of DLs, determined by QLF as measured by a single trained and calibrated examiner. Figure 1 seems to indicate that QLF images were collected on day of debond, but Table 2 indicates that the data collected at a mean of 6 weeks (range 0 to 156 days) were used in the analysis Pre‐treatment images were subtracted from post‐treatment images, so did measure incidence Secondary outcomes: severity of DLs (fluorescence loss and lesion depth from QLF), ICDAS, DMFS, bleeding indices. Authors state that number of lesions per participant was calculated and, for every participant having at least 1 lesion, mean fluorescence loss and area were calculated, so this took into account clustering of teeth within the mouth |
|
| Notes | Funding source: authors declare that study was "supported by Elmex research/Colgate‐Palmolive Europe" Corresponding author (Nicoline van der Kaaij ‐ n.vd.kaaij@acta.nl) contacted 21 August 2018 for clarification of some issues. No reply, follow‐up message sent 22 January 2019 to which a reply was received |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Report not clear. Author response (24 January 2019): "In Excel, a list with 120 unique random numbers was created and then fixed by an independent researcher. These were alternatingly allotted group A or B (60 in each group, second column). Then the list was ordered from small to large numbers, giving a random order of group assignment" |
| Allocation concealment (selection bias) | Low risk | Report not clear. Author response (24 January 2019): "The list with group assignments was controlled by the administration desk, were [sic] patients schedule their appointments. Patients were assigned in the order of their last appointment prior to bracket placement" |
| Blinding ‐ Patients & Operators | Low risk | Participants were provided with solution A or B. The bottles containing the rinse were "tested and regulated by Colgate‐Palmolive Europe" (presumably prepared as well) and were identical in appearance, consistency, taste and smell. Author response (24 January 2019): "Products were contained in identical flasks labeled: product for study use group A or B" |
| Blinding ‐ Outcome assessors | Low risk | Quote: "after analysing all data obtained, the code regarding the rinse was broken" so truly triple‐blind |
| Incomplete outcome data addressed | High risk | Comprehensive flowchart provided with reasons for withdrawals and dropouts. Substantial risk of attrition bias for demineralisation assessments due to dropouts and withdrawals (39 out of 120; 33%). Even higher dropout for secondary outcomes, particularly bleeding. A larger number "decided not to participant any further" in the fluoride rinse group (10) compared with the placebo rinse group (1). 17 participants were still in treatment when the study was stopped, as "a result of unforeseen treatment complication or non‐compliance." A shame they were not followed to the end of treatment |
| Free of selective reporting | Low risk | Differences in the mean fluorescence loss and lesion difference between the 2 groups was small and not clear if the lesions were of aesthetic impact |
| Free of other bias | Unclear risk | According to flow diagram all participants randomised received their allocated intervention. No protocol deviations reported. Complete‐case analysis undertaken presumably based on the assumption that data for participants who withdrew or dropped out were missing at random (MAR), however substantial attrition of participants, partly because they decided to stop the trial before all participants had completed their orthodontic treatment (see Incomplete outcome data addressed box above).Treatment delivered by orthodontic postgraduates, not clear how many and what level of experience. Participants dentist "informed about study and instructed not to apply extra fluoride." Also "Participants instructed not to use any fluoride‐containing products other than fluoride toothpaste", but this was not standardised. QLF images captured by 1 trained and calibrated examiner. Not entirely clear if all the images were collected and analysed from the day of debond, as they state "The WSL assessments were made at an average of 52 days after debonding (with a range of 0 to 156 days)." Those undertaken at 5 months following debond might have undergone quite extensive remineralisation unrelated to mouthrinse use Author response (24 January 2019): "We did use the pictures of TD1 for the WSL analyses (as is mentioned in the legend of figure 1 and in table 2). We choose this date since it is known that gingival swelling at time of debonding can obscure a part of the lesion (Boersma et al, Caries Research 2005;39(1):41‐7). The range was 0‐156 days, with a mean of 52 and the median being 45 days. Indeed it is possible that remineralisation will happen after debonding, in the study of M Beerens (European Journal of Orthodontics 2018;40(5):457‐64) it can be seen that only after 12 months there was a significant difference in fluorescence loss, caused by remineralisation. At 6 weeks, 3 and 6 months after debonding no significant difference was seen in that study. Also the study of T Matthousch (European Journal of Orthodontics 2007;29(3):294‐8) showed no improvement at 6 weeks, and only at 6 months an improvement in fluorescence loss. The range is because we did the research in normal practice settings, thus patients cancelling there [sic] appointments or coming at not scheduled time points happened" |
CI = confidence interval; DLs = demineralised lesions; DMFS = decayed, missing and filled surface; F = fluoride; GDP = general dental practitioner; ICDAS = International Caries Detection and Assessment System; ITT = intention‐to‐treat; LCC = light‐cured composite resin; NaF = sodium fluoride; ppm = parts per million; QLF = quantitative light‐induced fluorescence; RM‐GIC = resin‐modified glass ionomer cement; SD = standard deviation; WSLs = white spot lesions.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Al Mulla 2010 | Compared modified fluoride toothpaste technique to normal toothbrushing rather than 2 fluoride products |
| Alexander 2000 | Clinical assessment carried out 1 month after debonding not immediately after |
| Alwi 1994 | Abstract only. Insufficient information to include in review. Contacted author. Unable to provide sufficient data for analysis. No subsequent publication identified |
| Banks 1997 | Split‐mouth study |
| Banks 2000 | CCT with alternate allocation to fluoride or non‐fluoride elastomeric ligatures |
| Blanco 1988 | "Patients chosen at random" and divided into 2 groups. Report is unclear about the details of allocation to each group, groups are unequal in size, no baseline characteristics, and no outcome data presented per participant. Unable to contact authors and unable to include this study based on available information |
| Boyd 1992 | Demineralisation assessed 3 months after debonding rather than immediately |
| Boyd 1993 | Demineralisation assessed 3 months after debonding rather than immediately |
| Boyles 2007 | Not RCT |
| Buyukyilmaz 1994 | Split‐mouth study |
| Chung 1998 | Split‐mouth study |
| Czochrowska 1998 | Split‐mouth study |
| D'Agostino 1988 | Outcomes were DMFT and DMFS not demineralised white lesions |
| Demito 2011 | Split‐mouth study |
| Dyer 1982 | Not RCT |
| Dénes 1988 | Assessed DMFS not white spot lesions |
| Dénes 1989 | Assessed DMFS not white spot lesions |
| Dénes 1991 | Assessed DMFS not white spot lesions |
| Enerbäck 2019 | Did not follow to the end of orthodontic treatment only 1 year from start and outcomes not relevant for this review (caries risk and bacteria levels) |
| Farhadian 2008 | Not RCT |
| Fricker 1985 | Not RCT |
| Fricker 1987 | Not RCT |
| Gaworski 1999 | Not RCT |
| Geiger 1988 | Not RCT |
| Geiger 1992 | Not RCT |
| Gillgrass 2001 | Split‐mouth study |
| Gorton 2003 | Ex vivo study ‐ outcomes measured on extracted teeth |
| Hirschfield 1978 | Not RCT |
| Leizer 2010 | Appears to be allocation based on study number (odd or even) and teeth allocated alternately. CCT. No reply to emails sent to contact author |
| Maijer 1988 | Not RCT |
| Marcusson 1997 | Split‐mouth study |
| Marini 1999 | Duration of intervention 12 months but outcomes assessed at end of treatment period not at the end of treatment with fixed orthodontic appliances |
| Mattick 2001 | Split‐mouth RCT |
| Millett 1999 | Split‐mouth study, allocation of each side to treatment by alternation. Not RCT |
| Millett 2000 | Split‐mouth study, allocation of each side to treatment by alternation. Not RCT |
| Mitchell 1992 | Split‐mouth study, no random allocation. Author contacted |
| Neumann 1976 | Abstract only. Insufficient data, no subsequent publication identified |
| O'Reilly 1987 | Ex vivo study ‐ outcomes measured on extracted teeth |
| Ogaard 1986 | Ex vivo study ‐ outcomes measured on extracted teeth |
| Ogaard 1992 | Random allocation to treatment not mentioned. Author contacted |
| Ogaard 1996 | Not RCT. Author contacted |
| Ogaard 1997 | Effect of fluoride confounded by co‐intervention. Both groups had fluoride varnish. The experimental group had in addition an antimicrobial varnish therefore the study looks at the efficacy of the antimicrobial varnish rather than the fluoride varnish |
| Ogaard 2001 | Effect of fluoride confounded by co‐intervention. 2 randomised groups and 1 non‐randomised control group. Both randomised groups received fluoride varnish every 12 weeks, fluoride exposure was not different between the 2 randomised groups |
| Pascotto 2004 | Ex vivo study ‐ outcomes measured on extracted teeth |
| Robertson 2011 | Duration of intervention 12 months but outcomes assessed at end of treatment period not at the end of treatment with fixed orthodontic appliances |
| Salzmann 1976 | Abstract only. No subsequent publication identified |
| Shan 2008 | Split‐mouth study |
| Shannon 1978 | Allocation method not stated. Unable to contact the authors |
| Shannon 1979 | Allocation method not stated. Unable to contact the authors |
| Sköld‐Larsson 2013 | Intervention period was short (12 weeks) and assessments were not undertaken at the start and end of orthodontic treatment |
| Sonis 1989 | Not RCT |
| Trimpeneers 1996 | Split‐mouth study. All participants had the same product used in the same quadrants. Not RCT.Contacted author (LR Dermaut). Unable to provide further data for statistical analysis |
| Turner 1993 | Split‐mouth study |
| Twetman 1997 | Split‐mouth study |
| Ullsfoss 1994 | Both groups had fluoride mouthrinse. The experimental group had in addition an antimicrobial mouthrinse, therefore the study looks at the efficacy of the antimicrobial mouthrinse rather than the fluoride mouthrinse |
| Underwood 1989 | Random allocation not mentioned. Brackets on alternate teeth bonded with each adhesive. Not RCT |
| van der Linden 1998 | Split‐mouth study |
| Vivaldi‐Rodrigues 2006 | Split‐mouth study |
| Wenderoth 1999 | Not RCT |
CCT = controlled clinical trial; DMFS/DMFT = decayed, missing and filled surfaces/teeth; RCT = randomised controlled trial.
Characteristics of ongoing studies [ordered by study ID]
DRKS00012533.
| Trial name or title | Efficacy of the fluoride varnish enamelast for preventing white spot lesions and gingivitis in fixed orthodontic treatment of patients with low to moderate caries risk ‐ a randomised controlled trial |
| Methods | Single centre (specialist practice, Memmingen Germany), triple‐blind, RCT, 2‐arm parallel groups, assessing superiority |
| Participants | Target sample size: 104 |
| Interventions | Group 1: Intervention 1: instructions on home oral hygiene and nutrition; Intervention 2: study‐independent fixed orthodontic therapy in buccal technique; Intervention 3: 1‐time application of a placebo varnish at the beginning of fixed therapy (once at 6 months) Group 2: Intervention 1: instructions on home oral hygiene and nutrition; Intervention 2: study‐independent fixed orthodontic therapy in buccal technique; Intervention 3: 1‐time application of fluoride varnish enamelast at the beginning of fixed therapy (once at 6 months) |
| Outcomes | Measurement of white spot/caries progression by clinical‐visual assessment of the extent of the enamel/demineralisation/initial caries on the buccal tooth surfaces with a score value (Likert scale). Time points: T‐1, recruitment: appointment at least 30 days before the start of the fixed orthodontic therapy; T0, baseline: after bonding the brackets and removing the excess material; T1, 3 months: after 3 months of fixed therapy; T2, 6 months: after 6 months of fixed therapy (in case of a coincidence with the therapy end before debonding) Modified plaque index according to Silness and Loe (MPI) Gingival index according to Silness and Loe (1963) |
| Starting date | Date of first enrolment: 12 June 2017 |
| Contact information | Christian Kirschneck (christian.kirschneck@ukr.de) |
| Notes | Contacted author on 21 August 2018 who responded straight away. Only planning to collect data at 6 months, not at the end of treatment, so we will probably not include study but will contact again in future to see if the participants will be followed up |
DRKS00012540.
| Trial name or title | Efficacy of Fluor‐Protector S fluoride varnish for preventing white spot lesions and gingivitis in fixed orthodontic treatment of patients with high risk of caries ‐ a randomised controlled trial |
| Methods | Single centre (specialist practice, Memmingen Germany), triple‐blind, RCT, 2‐arm parallel groups, assessing superiority |
| Participants | Target sample size: 44 |
| Interventions | Group 1: Intervention 1: instructions on home oral hygiene and nutrition; Intervention 2: study‐independent fixed orthodontic therapy in buccal technique; Intervention 3: application of a placebo varnish at the beginning of fixed therapy and after 3 months (once at 3 months) Group 2: Intervention 1: instructions on home oral hygiene and nutrition; Intervention 2: study‐independent fixed orthodontic therapy in buccal technique; Intervention 3: application of Fluor Protector S varnish at the beginning of fixed therapy and after 3 months (once at 3 months) |
| Outcomes | Measurement of white spot/caries progression by clinical‐visual assessment of the extent of the enamel/demineralisation/initial caries on the buccal tooth surfaces with a score value (Likert scale). Time points: T‐1, recruitment: appointment at least 30 days before the start of the fixed orthodontic therapy; T0, baseline: after bonding the brackets and removing the excess material; T1, 3 months: after 3 months of fixed therapy; T2, 6 months: after 6 months of fixed therapy (in case of a coincidence with the therapy end before debonding) Modified plaque index according to Silness and Loe (MPI) Gingival index according to Silness and Loe (1963) |
| Starting date | Date of first enrolment: 12 June 2017 |
| Contact information | Christian Kirschneck (christian.kirschneck@ukr.de) |
| Notes | Contacted author on 21 August 2018 who responded straight away. Only planning to collect data at 6 months, not at the end of treatment, so we will probably not include study but will contact again in future to see if the participants will be followed up |
IRCT2016122531558N1.
| Trial name or title | A clinical trial of comparing the effect of fluoride varnish and chlorhexidine gel on white spots and gingival indexes in orthodontic patients |
| Methods | Single centre (Faculty of Dentistry, Isfahan, Iran), RCT, 4‐arm parallel groups, assessing superiority |
| Participants | Target sample size: 40 |
| Interventions | Intervention 1: fluoride varnish 5% which is made in USA will be applied on teeth every 3 months until 9 months Intervention 2: chlorhexidine gel 0.2% which is made in Spain, in dose of 5 mg will be applied on teeth every 3 months until 9 months Intervention 3: placebo group: sorbitol solution (70% W/W) will be applied on teeth every 3 months until 9 months Intervention 4: control group: no intervention |
| Outcomes | States 3 primary outcomes and no secondary outcomes: White spots. Time points: before the first intervention, 3, 6 and 9 months after that and before the intervention in each time. Method of measurement: visual inspection with intraoral examination mirror ‐ not clear what index will be used or by whom Gingival index. Time points: before the first intervention, 3, 6 and 9 months after that and before the intervention in each time. Method of measurement: dental probe Plaque index. Time points: before the first intervention, 3, 6 and 9 months after that and before the intervention in each time. Method of measurement: visual inspection |
| Starting date | 20 January 2017 |
| Contact information | Navid Yaraghi (alavi@dnt.mui.ac.ir) |
| Notes | Contacted on 21 August 2018 ‐ awaiting a reply |
ppm = parts per million; RCT = randomised controlled trial; W/W = weight/weight.
Differences between protocol and review
In the 2013 update of this review, controlled clinical trials (quasi‐randomised) were excluded.
A point of clarification was added to the inclusion criteria for this review. For a randomised controlled trial to be included, demineralised lesions (DLs) must be assessed on teeth remaining in the mouth. Studies that evaluated demineralisation of extracted teeth were excluded from the 2013 update of this review because they measured the effects of short‐term exposure to fluoride (four to six weeks between application and extraction of the teeth). Furthermore, it was decided that evaluation of demineralisation must take place at the end of treatment with fixed orthodontic appliances (debonding).
As stated in the Discussion of the 2013 update of this review, the use of a split‐mouth study design to evaluate these interventions is potentially inappropriate. It is unlikely that the fluoride released will be confined to only the quadrants or the specific teeth in which the experimental material has been placed, and some 'contamination' of teeth in the control quadrants is inevitable. This will reduce the difference in outcome between experimental and control teeth and will reduce the power of the trial to find a difference. Indeed split‐mouth studies included in the previous version of this review found no difference between teeth with fluoridated bracket adhesives and those without, supporting the view that this design is inappropriate for evaluating topical fluorides. Split‐mouth studies were excluded from the 2013 update of this review, and the Methods section of this review was amended to remove methods that were used to deal with split‐mouth studies.
Contributions of authors
Philip Benson wrote the original protocol and co‐ordinated the review and subsequent updates. Philip Benson, Fiona Dyer, Peter Germain, Declan Millett and Nicola Parkin independently and in duplicate assessed the eligibility of trials, extracted data and assessed the quality and risk of bias. Philip Benson and Fiona Dyer (2019 update) contacted authors, entered the data, carried out the statistical analysis (with help from Helen Worthington) and wrote the review. Declan Millett proofread the review.
Sources of support
Internal sources
School of Clinical Dentistry, University of Sheffield, UK.
Dental School, University College Cork, Ireland.
External sources
-
Cochrane Oral Health Global Alliance, Other.
The production of Cochrane Oral Health reviews has been supported financially by our Global Alliance since 2011 (oralhealth.cochrane.org/partnerships‐alliances). Contributors over the past year have been the American Association of Public Health Dentistry, USA; AS‐Akademie, Germany; the British Association for the Study of Community Dentistry, UK; the British Society of Paediatric Dentistry, UK; the Canadian Dental Hygienists Association, Canada; the Centre for Dental Education and Research at All India Institute of Medical Sciences, India; the National Center for Dental Hygiene Research & Practice, USA; New York University College of Dentistry, USA; NHS Education for Scotland, UK; and the Swiss Society for Endodontology, Switzerland.
-
National Institute for Health Research (NIHR), UK.
This project was supported by the NIHR, via Cochrane Infrastructure funding to Cochrane Oral Health. The views and opinions expressed are those of the authors and not necessarily those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care.
Declarations of interest
Three of the review authors (Philip Benson, Declan Millett and Fiona Dyer) were authors for one of the included studies (Benson 2019). The evaluation of this study, including data extraction and methodological quality assessments, was reviewed and confirmed by two authors not involved in this study (Nicola Parkin and Peter Germain).
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Benson 2019 {published data only}
- Benson PE, Alexander‐Abt J, Cotter S, Dyer FMV, Fenesha F, Patel A, et al. Resin‐modified glass ionomer cement vs composite for orthodontic bonding: a multicenter, single‐blind, randomized controlled trial. American Journal of Orthodontics and Dentofacial Orthopedics 2019;155(1):10‐8. [DOI] [PubMed] [Google Scholar]
He 2010 {published data only}
- He WD, Liu YZ, Xu YY, Chen D. Study on application of CPP‐ACP on tooth mineralization during orthodontic treatment with fixed appliance. Shanghai Kou Qiang Yi Xue 2010;19(2):140‐3. [PubMed] [Google Scholar]
Jiang 2013 {published data only}
- Jiang H, Hua F, Yao L, Tai B, Du M. Effect of 1.23% acidulated phosphate fluoride foam on white spot lesions in orthodontic patients: a randomised trial. Pediatric Dentistry 2013;35(3):275‐8. [PubMed] [Google Scholar]
Jost‐Brinkman 2017 {published and unpublished data}
- Jost‐Brinkman PG, Redlich M, Klasser M, Egger‐Heigold B. Prevention of incipient carious lesions (white spot lesions) in patients with fixed orthodontic appliances following the application of elmex® gel. GCP Study Report 2017.
Luther 2005 {published and unpublished data}
- Luther F, Tobin M, Robertson AJ, Toumba KJ. Fluoride‐releasing glass beads in orthodontic treatment to reduce decay: a randomized, controlled clinical trial. World Journal of Orthodontics Supplement 2005;6(5):166‐7. [Google Scholar]
Ogaard 2006 {published and unpublished data}
- Ogaard B, Alm AA, Larsson E, Adolfsson U. A prospective, randomized clinical study on the effects of an amine fluoride/stannous fluoride toothpaste/mouthrinse on plaque, gingivitis and initial caries lesion development in orthodontic patients. European Journal of Orthodontics 2006;28(1):8‐12. [DOI] [PubMed] [Google Scholar]
Sonesson 2014 {published data only}
- Sonesson M, Twetman S, Bondemark L. Effectiveness of high‐fluoride toothpaste on enamel demineralization during orthodontic treatment ‐ a multicenter randomized controlled trial. European Journal of Orthodontics 2014;36(6):678‐82. [DOI] [PubMed] [Google Scholar]
Sonesson 2019 {published and unpublished data}
- Sonesson M, Brechter A, Abdulraheem S, Lindman R, Twetman S. Fluoride varnish for the prevention of white spot lesions during orthodontic treatment with fixed appliances: a randomized controlled trial. European Journal of Orthodontics 2019 Jun 14 [Epub ahead of print]. [DOI: 10.1093/ejo/cjz045] [DOI] [PubMed]
Stecksén‐Blicks 2007 {published and unpublished data}
- Stecksén‐Blicks C, Renfors G, Oscarson ND, Bergstrand F, Twetman S. Caries‐preventive effectiveness of fluoride varnish: a randomized controlled trial in adolescents with fixed orthodontic appliances. Caries Research 2007;41(6):455‐9. [DOI] [PubMed] [Google Scholar]
van der Kaaij 2015 {published data only}
- Kaaij NCW, Veen MH, Kaaij MAE, Cate JM. A prospective, randomized placebo‐controlled clinical trial on the effects of a fluoride rinse on white spot lesion development and bleeding in orthodontic patients. European Journal of Oral Sciences 2015;123(3):186‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Alexander 2000 {published data only}
- Alexander SA, Ripa LW. Effects of self‐applied topical fluoride preparations in orthodontic patients. Angle Orthodontist 2000;70(6):424‐30. [DOI] [PubMed] [Google Scholar]
Al Mulla 2010 {published data only}
- Al Mulla AH, Al Kharsa S, Birkhed D. Modified fluoride toothpaste technique reduces caries in orthodontic patients: a longitudinal, randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics 2010;138(3):285‐91. [DOI] [PubMed] [Google Scholar]
Alwi 1994 {published data only}
- Alwi NBH, Creanor SL. The influence of fluoride‐releasing composites on the development of white‐spot lesions near orthodontic brackets: an in vivo investigation (Research Reports 1993: Abstract). British Journal of Orthodontics 1994;21(1):118. [Google Scholar]
Banks 1997 {published data only}
- Banks PA, Burn A, O'Brien K. A clinical evaluation of the effectiveness of including fluoride into an orthodontic bonding adhesive. European Journal of Orthodontics 1997;19(4):391‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Banks 2000 {published data only}
- Banks PA, Chadwick SM, Asher‐McDade C, Wright JL. Fluoride‐releasing elastomerics ‐ a prospective controlled clinical trial. European Journal of Orthodontics 2000;22(4):401‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Blanco 1988 {published data only}
- Blanco Parra R. Evaluation of the presence of white spots following orthodontic treatment. Revista Iberoamericana de Ortodoncia 1988;8(1):31‐8. [PubMed] [Google Scholar]
Boyd 1992 {published data only}
- Boyd RL. Two‐year longitudinal study of a peroxide‐fluoride rinse on decalcification in adolescent orthodontic patients. Journal of Clinical Dentistry 1992;3(3):83‐7. [MEDLINE: ] [PubMed] [Google Scholar]
Boyd 1993 {published data only}
- Boyd RL. Comparison of three self‐applied topical fluoride preparations for control of decalcification. Angle Orthodontist 1993;63(1):25‐30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Boyles 2007 {published data only}
- Bagby MD, Boyles GAC, Martin C, Kao E, Ngan P. Effects of fluoride varnishes on enamel decalcification around orthodontic appliances. American Association of Dental Research poster abstract; 2008 March 31‐April 5; Dallas (TX).
- Boyles GA. Effects of Fluoride Varnishes and Adhesives on Bond Strength and Preventing Enamel Decalcification Around Orthodontic Appliances: an In Vitro and In Vivo Study [Masters thesis]. Morgantown, West Virginia (USA): West Virginia University, 2007. [Google Scholar]
Buyukyilmaz 1994 {published data only}
- Buyukyilmaz T, Tangugsorn V, Ogaard B, Arends J, Ruben J, Rolla G. The effect of titanium tetrafluoride (TiF4) application around orthodontic brackets. American Journal of Orthodontics and Dentofacial Orthopedics 1994;105(3):293‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Buyukyilmaz T, Tangugsorn V, Ogaard B, Arends J, Ruben J, Rolla G. The effect of titanium tetrafluoride (TiF4) application around orthodontic brackets. European Journal of Orthodontics 1993;15(4):334. [DOI] [PubMed] [Google Scholar]
Chung 1998 {published and unpublished data}
- Chung CK, Millett DT, Creanor SL. Cariostatic ability of resin‐modified glass ionomer cements for orthodontic bonding. European Journal of Orthodontics 1996;18(5):513. [Google Scholar]
- Chung CK, Millett DT, Creanor SL, Gilmour WH, Foye RH. Fluoride release and cariostatic ability of a compomer and a resin‐modified glass ionomer cement used for orthodontic bonding. Journal of Dentistry 1998;26(5‐6):533‐8. [DOI] [PubMed] [Google Scholar]
Czochrowska 1998 {published data only}
- Czochrowska E, Ogaard B, Duschner H, Ruben J, Arends J. Cariostatic effect of a light‐cured, resin‐reinforced glass‐ionomer for bonding orthodontic brackets in vivo. A combined study using microradiography and confocal laser scanning microscopy. Journal of Orofacial Orthopedics 1998;59(5):265‐73. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
D'Agostino 1988 {published data only}
- D'Agostino RB, Cancro LP, Fischman S. Effects of anticaries dentifrices on orthodontic subjects. Compendium of Continuing Education in Dentistry 1988;11:S384‐9. [PubMed] [Google Scholar]
Demito 2011 {published and unpublished data}
- Demito CF, Rodrigues GV, Ramos AL, Bowman SJ. Efficacy of a fluoride varnish in preventing white‐spot lesions as measured with laser fluorescence. Journal of Clinical Orthodontics 2011;45(1):25‐9. [PubMed] [Google Scholar]
Dénes 1988 {published data only}
- Dénes J, Gábris K. Results of a 3‐year Elmex program during orthodontic treatment with fixed appliances. ZWR 1988;97(10):863‐8. [PubMed] [Google Scholar]
Dénes 1989 {published data only}
- Dénes J, Domokos G, Gábris K, Juhász G, Nagy B, Radóczi B, et al. Results of the use of amine‐fluoride preparations in orthodontic practice. Fogorvosi Szemle 1989;82(9):257‐61. [PubMed] [Google Scholar]
Dénes 1991 {published data only}
- Dénes J, Gábris K. Results of a 3‐year oral hygiene programme, including amine fluoride products, in patients treated with fixed orthodontic appliances. European Journal of Orthodontics 1991;13(2):129‐33. [DOI] [PubMed] [Google Scholar]
Dyer 1982 {published data only}
- Dyer JR, Shannon IL. MFP versus stannous fluoride mouthrinses for prevention of decalcification in orthodontic patients. ASDC Journal of Dentistry for Children 1982;49(1):19‐21. [MEDLINE: ] [PubMed] [Google Scholar]
Enerbäck 2019 {published data only}
- Enerbäck H, Möller M, Nylén C, Ödman Bresin C, Östman Ros I, Westerlund A. Effects of orthodontic treatment and different fluoride regimens on numbers of cariogenic bacteria and caries risk: a randomized controlled trial. European Journal of Orthodontics 2019;41(1):59‐66. [DOI: 10.1093/ejo/cjy025] [DOI] [PubMed] [Google Scholar]
Farhadian 2008 {published and unpublished data}
- Farhadian N, Miresmaeili A, Eslami B, Mehrabi S. Effect of fluoride varnish on enamel demineralization around brackets: an in‐vivo study. American Journal of Orthodontics and Dentofacial Orthopedics 2008;133(4 Suppl):S95‐8. [DOI] [PubMed] [Google Scholar]
Fricker 1985 {published data only}
- Fricker JP, McLachlan MD. Clinical studies of glass ionomer cements. Part I‐A twelve month clinical study comparing zinc phosphate cement to glass ionomer. Australian Orthodontic Journal 1985;9(1):179‐80. [PubMed] [Google Scholar]
Fricker 1987 {published data only}
- Fricker JP, McLachlan MD. Clinical studies on glass ionomer cements. Part 2‐A two year clinical study comparing glass ionomer cement with zinc phosphate cement. Australian Orthodontic Journal 1987;10(1):12‐4. [PubMed] [Google Scholar]
Gaworski 1999 {published data only}
- Gaworski M, Weinstein M, Borislow AJ, Braitman LE. Decalcification and bond failure: a comparison of a glass ionomer and a composite resin bonding system in vivo. American Journal of Orthodontics and Dentofacial Orthopedics 1999;116(5):518‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Geiger 1988 {published data only}
- Geiger AM, Gorelick L, Gwinnett AJ, Griswold PG. The effect of a fluoride program on white spot formation during orthodontic treatment. American Journal of Orthodontics and Dentofacial Orthopedics 1988;93(1):29‐37. [DOI] [PubMed] [Google Scholar]
Geiger 1992 {published data only}
- Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing. American Journal of Orthodontics and Dentofacial Orthopedics 1992;101(5):403‐7. [DOI] [PubMed] [Google Scholar]
Gillgrass 2001 {published and unpublished data}
- Gillgrass TJ, Benington PC, Millett DT, Newell J, Gilmour WH. Modified composite or conventional glass ionomer for band cementation? A comparative clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics 2001;120(1):49‐53. [DOI] [PubMed] [Google Scholar]
Gorton 2003 {published data only}
- Gorton J, Featherstone JD. In vivo inhibition of demineralization around orthodontic brackets. American Journal of Orthodontics and Dentofacial Orthopedics 2003;123(1):10‐4. [DOI] [PubMed] [Google Scholar]
Hirschfield 1978 {published data only}
- Hirschfield RE. Control of decalcification by use of fluoride mouthrinse. ASDC Journal of Dentistry for Children 1978;45(6):458‐60. [PubMed] [Google Scholar]
Leizer 2010 {published and unpublished data}
- Leizer C, Weinstein M, Borislow AJ, Braitman LE. Efficacy of a filled‐resin sealant in preventing decalcification during orthodontic treatment. American Journal of Orthodontics and Dentofacial Orthopedics 2010;137(6):796‐800. [DOI] [PubMed] [Google Scholar]
Maijer 1988 {published data only}
- Maijer R, Smith DC. A comparison between zinc phosphate and glass ionomer cement in orthodontics. American Journal of Orthodontics and Dentofacial Orthopedics 1988;93(4):273‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcusson 1997 {published and unpublished data}
- Marcusson A, Norevall LI, Persson M. White spot reduction when using glass ionomer cement for bonding in orthodontics: a longitudinal and comparative study. European Journal of Orthodontics 1997;19(3):233‐42. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marini 1999 {published data only}
- Marini I, Pelliccioni GA, Vecchiet F, Alessandri Bonetti G, Checchi L. A retentive system for intra‐oral fluoride release during orthodontic treatment. European Journal of Orthodontics 1999;21(6):695‐701. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Mattick 2001 {published data only (unpublished sought but not used)}
- Mattick CR, Mitchell L, Chadwick SM, Wright J. Fluoride‐releasing elastomeric modules reduce decalcification: a randomized controlled trial. Journal of Orthodontics 2001;28(3):217‐9. [DOI] [PubMed] [Google Scholar]
Millett 1999 {published data only}
- Millett DT, Nunn JH, Welbury RR, Gordon PH. Decalcification in relation to brackets bonded with glass ionomer cement or a resin adhesive. Angle Orthodontist 1999;69(1):65‐70. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Millett 2000 {published and unpublished data}
- Millett DT, McCluskey LA, McAuley F, Creanor SL, Newell J, Love J. A comparative clinical trial of a compomer and a resin adhesive for orthodontic bonding. Angle Orthodontist 2000;70(3):233‐40. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Mitchell 1992 {published data only}
- Mitchell L. An investigation into the effect of a fluoride releasing adhesive on the prevalence of enamel surface changes associated with directly bonded orthodontic attachments. British Journal of Orthodontics 1992;19(3):207‐14. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Neumann 1976 {published data only}
- Neumann HF. A clinical evaluation of decalcification under orthodontic bands following pretreatment with acidulated phosphate‐fluorides and adhesive plastic coatings. American Journal of Orthodontics 1976;69(6):698‐9. [MEDLINE: ] [Google Scholar]
O'Reilly 1987 {published data only}
- O'Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic appliances: an in vivo study. American Journal of Orthodontics and Dentofacial Orthopedics 1987;92(1):33‐40. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ogaard 1986 {published and unpublished data}
- Ogaard B, Arends J, Schuthof J, Rolla G, Ekstrand J, Oliveby A. Action of fluoride on initiation of early enamel caries in vivo. A microradiographical investigation. Caries Research 1986;20(3):270‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ogaard 1992 {published data only}
- Ogaard B, Rezk‐Lega F, Ruben J, Arends J. Cariostatic effect and fluoride release from a visible light‐curing adhesive for bonding of orthodontic brackets. American Journal of Orthodontics and Dentofacial Orthopedics 1992;101(4):303‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ogaard 1996 {published data only}
- Ogaard B, Duschner H, Ruben J, Arends J. Microradiography and confocal laser scanning microscopy applied to enamel lesions formed in vivo with and without fluoride varnish treatment. European Journal of Oral Sciences 1996;104(4 Pt 1):378‐83. [DOI] [PubMed] [Google Scholar]
Ogaard 1997 {published data only}
- Ogaard B, Larsson E, Glans R, Henriksson T, Birkhed D. Antimicrobial effect of a chlorhexidine‐thymol varnish (Cervitec) in orthodontic patients. A prospective, randomized clinical trial. Journal of Orofacial Orthopedics 1997;58(4):206‐13. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ogaard 2001 {published data only}
- Ogaard B, Larsson E, Henriksson T, Birkhed D, Bishara SE. Effects of combined application of antimicrobial and fluoride varnishes in orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics 2001;120(1):28‐35. [DOI] [PubMed] [Google Scholar]
Pascotto 2004 {published data only}
- Pascotto RC, Navarro MF, Capelozza Filho L, Cury JA. In vivo effect of a resin‐modified glass ionomer cement on enamel demineralization around orthodontic brackets. American Journal of Orthodontics and Dentofacial Orthopedics 2004;125(1):36‐41. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Robertson 2011 {published data only}
- Johnson D. MI Paste Plus research. American Journal of Orthodontics and Dentofacial Orthopedics 2012;141(5):526. [PUBMED: 22554734] [DOI] [PubMed] [Google Scholar]
- Robertson MA, Kau CH, English JD, Lee RP, Powers J, Nguyen JT. MI Paste Plus to prevent demineralization in orthodontic patients: a prospective randomized controlled trial. American Journal of Orthodontics and Dentofacial Orthopedics 2011;140(5):660‐8. [DOI] [PubMed] [Google Scholar]
Salzmann 1976 {published data only}
- Salzmann JA. A clinical evaluation of decalcification under orthodontic bands following pretreatment with acidulated phosphate‐fluorides and adhesive plastic coatings. American Journal of Orthodontics 1976;69(6):698. [Google Scholar]
Shan 2008 {published and unpublished data}
- Shan LH, Cui ZQ, Shen QH, Gao Q, Qiu ZX. Application of light‐cure resin‐modified glass ionomer cement in orthodontic practice. Journal of Clinical Rehabilitative Tissue Engineering Research 2008;12(6):1149‐52. [Google Scholar]
Shannon 1978 {published data only}
- Shannon IL, Clair JR, Pratt GA, West DC. Stannous fluoride versus sodium fluoride in preventive treatment of orthodontic patients. Australian Orthodontic Journal 1978;5(1):18‐24. [Google Scholar]
Shannon 1979 {published data only}
- Shannon IL, West DC. Prevention of decalcification in orthodontic patients by daily self‐treatment with 0.4% SnF2 gel. Pediatric Dentistry 1979;1(2):101‐2. [MEDLINE: ] [PubMed] [Google Scholar]
Sköld‐Larsson 2013 {published data only}
- Sköld‐Larsson K, Sollenius O, Karlsson L, Petersson LG, Twetman S. Effect of fluoridated milk on enamel demineralization adjacent to fixed orthodontic appliances. Acta Odontologica Scandinavica 2013;71(3‐4):464‐8. [DOI] [PubMed] [Google Scholar]
Sonis 1989 {published data only}
- Sonis AL, Snell W. An evaluation of a fluoride‐releasing, visible light‐activated bonding system for orthodontic bracket placement. American Journal of Orthodontics and Dentofacial Orthopedics 1989;95(4):306‐11. [DOI] [PubMed] [Google Scholar]
Trimpeneers 1996 {published data only}
- Trimpeneers LM, Dermaut LR. A clinical evaluation of the effectiveness of a fluoride‐releasing visible light‐activated bonding system to reduce demineralization around orthodontic brackets. American Journal of Orthodontics and Dentofacial Orthopedics 1996;110(2):218‐22. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Turner 1993 {published data only (unpublished sought but not used)}
- Turner PJ. The clinical evaluation of a fluoride‐containing orthodontic bonding material. Journal of Orthodontics 1993;20(4):307‐13. [DOI] [PubMed] [Google Scholar]
Twetman 1997 {published data only}
- Twetman S, McWilliam JS, Hallgren A, Oliveby A. Cariostatic effect of glass ionomer retained orthodontic appliances. An in vivo study. Swedish Dental Journal 1997;21(5):169‐75. [PubMed] [Google Scholar]
Ullsfoss 1994 {published data only}
- Ullsfoss BN, Ogaard B, Arends J, Ruben J, Rolla G, Afseth J. Effect of a combined chlorhexidine and NaF mouthrinse: an in vivo human caries model study. Scandinavian Journal of Dental Research 1994;102(2):109‐12. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Underwood 1989 {published data only}
- Underwood ML, Rawls HR, Zimmerman BF. Clinical evaluation of a fluoride‐exchanging resin as an orthodontic adhesive. American Journal of Orthodontics and Dentofacial Orthopedics 1989;96(2):93‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
van der Linden 1998 {published data only}
- Linden RP, Dermaut LR. White spot formation under orthodontic bands cemented with glass ionomer with or without Fluor Protector. European Journal of Orthodontics 1998;20(3):219‐24. [DOI] [PubMed] [Google Scholar]
Vivaldi‐Rodrigues 2006 {published and unpublished data}
- Vivaldi‐Rodrigues G, Demito CF, Bowman SJ, Ramos AL. The effectiveness of a fluoride varnish in preventing development of white spot lesions. World Journal of Orthodontics 2006;7:138‐44. [PubMed] [Google Scholar]
Wenderoth 1999 {published data only}
- Wenderoth CJ, Weinstein M, Borislow AJ. Effectiveness of a fluoride‐releasing sealant in reducing decalcification during orthodontic treatment. American Journal of Orthodontics and Dentofacial Orthopedics 1999;116(6):629‐34. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
DRKS00012533 {published and unpublished data}
- DRKS00012533. Efficacy of the fluoride varnish enamelast for preventing white‐spot lesions and gingivitis in fixed orthodontic treatment of patients with low to moderate caries risk ‐ a randomized controlled trial. drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00012533 (first received 8 June 2017).
DRKS00012540 {published and unpublished data}
- DRKS00012540. Efficacy of Fluor‐Protector S fluoride varnish for preventing white‐spot lesions and gingivitis in fixed orthodontic treatment of patients with high risk of caries ‐ a randomized controlled trial. drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00012540 (first received 8 June 2017).
IRCT2016122531558N1 {published and unpublished data}
- IRCT2016122531558N1. Effect of preventive agents on oral health in orthodontic patients [A clinical trial of comparing the effect of fluoride varnish and chlorhexidine gel on white spots and gingival indexes in orthodontic patients]. en.irct.ir/trial/24800 (first received 24 June 2017).
Additional references
Angmar‐Mansson 1996
- Angmar‐Mansson B, al‐Khateeb S, Tranaeus S. Monitoring the caries process. Optical methods for clinical diagnosis and quantification of enamel caries. European Journal of Oral Science 1996;104(4 Pt 2):480‐5. [DOI] [PubMed] [Google Scholar]
Benson 2010
- Benson PE. Fluoride‐containing materials and the prevention of demineralization during orthodontic treatment – which research method should we now use?. Seminars in Orthodontics 2010;16(4):293‐301. [Google Scholar]
Chadwick 2005
- Chadwick BL, Roy J, Knox J, Treasure ET. The effect of topical fluorides on decalcification in patients with fixed orthodontic appliances: a systematic review. American Journal of Orthodontics and Dentofacial Orthopedics 2005;128(5):601‐6. [DOI] [PubMed] [Google Scholar]
Derks 2004
- Derks A, Katsaros C, Frencken JE, van't Hof MA, Kuijpers‐Jagtman AM. Caries‐inhibiting effect of preventive measures during orthodontic treatment with fixed appliances. Caries Research 2004;38(5):413‐20. [DOI] [PubMed] [Google Scholar]
Enaia 2011
- Enaia M, Bock N, Ruf S. White‐spot lesions during multibracket appliance treatment: a challenge for clinical excellence. American Journal of Orthodontics and Dentofacial Orthopedics 2011;140(1):e17‐e24. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- Hamilton (ON): McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 15 March 2019. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Höchli 2017
- Höchli D, Hersberger‐Zurfluh M, Papageorgiou SN, Eliades T. Interventions for orthodontically induced white spot lesions: a systematic review and meta‐analysis. European Journal of Orthodontics 2017;39(1):122‐33. [DOI] [PubMed] [Google Scholar]
Kerbusch 2012
Lapenaite 2016
- Lapenaite E, Lopatiene K, Ragauskaite A. Prevention and treatment of white spot lesions during and after fixed orthodontic treatment: a systematic literature review. Stomatologija 2016;18:3‐8. [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Lopatiene 2016
- Lopatiene K, Borisovaite M, Lapenaite E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: a systematic literature review. Journal of Oral Maxillofacial Research 2016;7(2):e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lynch 2006
- Lynch RJ, Mony U, Cate JM. The effect of fluoride at plaque fluid concentrations on enamel de‐ and remineralisation at low pH. Caries Research 2006;40(6):522‐9. [DOI] [PubMed] [Google Scholar]
Marinho 2003a
- Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2003, Issue 1. [DOI: 10.1002/14651858.CD002278] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marinho 2003b
- Marinho VCC, Higgins JPT, Logan S, Sheiham A. Topical fluoride (toothpastes, mouthrinses, gels or varnishes) for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2003, Issue 4. [DOI: 10.1002/14651858.CD002782] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marinho 2004
- Marinho VCC, Higgins JPT, Sheiham A, Logan S. Combinations of topical fluoride (toothpastes, mouthrinses, gels, varnishes) versus single topical fluoride for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD002781.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marinho 2016
- Marinho VCC, Chong LY, Worthington HV, Walsh T. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2016, Issue 7. [DOI: 10.1002/14651858.CD002284.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Maxfield 2012
- Maxfield BJ, Hamdan AM, Tufekci E, Shroff B, Best AM, Lindauer SJ. Development of white spot lesions during orthodontic treatment: perceptions of patients, parents, orthodontists, and general dentists. American Journal of Orthodontics and Dentofacial Orthopedics 2012;141(3):337‐44. [DOI] [PubMed] [Google Scholar]
McCarney 2007
- McCarney R, Warner J, Iliffe S, Haselen R, Griffin M, Fisher P. The Hawthorne Effect: a randomised, controlled trial. BMC Medical Research Methodology 2007;7:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Naranjo 2006
- Naranjo AA, Triviño ML, Jaramillo A, Betancourth M, Botero JE. Changes in the subgingival microbiota and periodontal parameters before and 3 months after bracket placement. American Journal of Orthodontics and Dentofacial Orthopedics 2006;30(3):275.e17‐275.e22. [DOI] [PubMed] [Google Scholar]
Nascimento 2016
- Nascimento PL, Fernandes MT, Figueiredo FE, Faria‐E‐Silva AL. Fluoride‐releasing materials to prevent white spot lesions around orthodontic brackets: a systematic review. Brazilian Dental Journal 2017;27(1):101‐7. [DOI] [PubMed] [Google Scholar]
Ogaard 1989
- Ogaard B. Prevalence of white spot lesions in 19‐year‐olds: a study on untreated and orthodontically treated persons 5 years after treatment. American Journal of Orthodontics and Dentofacial Orthopedics 1989;96(5):423‐7. [DOI] [PubMed] [Google Scholar]
Pandis 2013
- Pandis N, Walsh T, Polychronopoulou A, Katsaros C, Eliades T. Split‐mouth designs in orthodontics: an overview with applications to orthodontic clinical trials. European Journal of Orthodontics 2013;35(6):783‐9. [DOI: 10.1093/ejo/cjs108] [DOI] [PubMed] [Google Scholar]
Rahimi 2017
- Rahimi F, Sadeghi M, Mozaffari HR. Efficacy of fluoride varnish for prevention of white spot lesions during orthodontic treatment with fixed appliances: a systematic review study. Biomedical Research and Therapy 2017;4(8):1513‐26. [Google Scholar]
Rogers 2010
- Rogers S, Chadwick B, Treasure E. Fluoride‐containing orthodontic adhesives and decalcification in patients with fixed appliances: a systematic review. American Journal of Orthodontics and Dentofacial Orthopedics 2010;390:e1‐8. [DOI] [PubMed] [Google Scholar]
Rücker 2008
- Rücker G, Schwarzer G, Carpenter J. Arcsine test for publication bias in meta‐analyses with binary outcomes. Statistics in Medicine 2008;27:746‐63. [DOI] [PubMed] [Google Scholar]
Sardana 2019a
- Sardana D, Zhang J, Ekambaram M, Yang Y, McGrath CP, Yiu CKY. Effectiveness of professional fluorides against enamel white spot lesions during fixed orthodontic treatment: a systematic review and meta‐analysis. Journal of Dentistry 2019;82(1):1‐10. [DOI: 10.1016/j.jdent.2018.12.006] [DOI] [PubMed] [Google Scholar]
Sardana 2019b
- Sardana D, Manchanda S, Ekambaram M, Yang Y, McGrath CP, Yiu CKY. Effectiveness of self‐applied topical fluorides against enamel white spot lesions from multibracketed fixed orthodontic treatment: a systematic review. European Journal of Orthodontics 2019 Apr 9 [Epub ahead of print]. [DOI: 10.1093/ejo/cjz015] [DOI] [PubMed]
Tasios 2019
ten Cate 2013
- Cate JM. Contemporary perspective on the use of fluoride products in caries prevention. British Dental Journal 2013;214(4):161‐7. [DOI] [PubMed] [Google Scholar]
Tufekci 2011
- Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthodontist 2011;81(2):206‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2013
- Wang M, Guo Y, Jiang H. Effectiveness of topical fluoride on prevention of enamel demineralization in China: a systematic review. Chinese Journal of Evidence‐Based Medicine 2013;13(7):875‐84. [Google Scholar]
References to other published versions of this review
Benson 2002
- Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed brace treatment. Cochrane Database of Systematic Reviews 2002, Issue 3. [DOI: 10.1002/14651858.CD003809] [DOI] [PubMed] [Google Scholar]
Benson 2004
- Benson PE, Parkin N, Millett DT, Dyer F, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed brace treatment. Cochrane Database of Systematic Reviews 2004, Issue 3. [DOI: 10.1002/14651858.CD003809.pub2] [DOI] [PubMed] [Google Scholar]
Benson 2013
- Benson PE, Parkin N, Dyer F, Millett DT, Furness S, Germain P. Fluorides for the prevention of early tooth decay (demineralised white lesions) during fixed brace treatment. Cochrane Database of Systematic Reviews 2013, Issue 12. [DOI: 10.1002/14651858.CD003809.pub3] [DOI] [PubMed] [Google Scholar]