

Introduction
The lesions of discoid lupus erythematosus (DLE) are categorized as either localized (presenting above the neck in the scalp, face, and ears), or generalized (involving areas above and below the neck, often in the upper extremities). DLE lesions are commonly incited by trauma, infection, burns, dermatitis, and ultraviolet radiation.1 Previous literature has proposed the term lupus ab igne to describe the development of clinically characteristic DLE lesions induced by chronic heat exposure.2 We present the first case, to our knowledge, of DLE lesions associated with Koebnerization from chronic heat exposure with electronic cigarette (EC) usage.
Case
A 34-year-old woman with a 14-year history of systemic lupus erythematosus (SLE) and Sjogren syndrome presented with a hyperpigmented plaque on the upper lip and hyperpigmented, pruritic patches on the bilateral lower extremities. Her SLE had been managed on hydroxychloroquine for 7 years, with previous flares typically manifesting as cutaneous eruptions and arthralgias. She is an active smoker, using an EC. Her personal medical history was significant only for thyroid disease, and she had no family history of other autoimmune disorders. Physical examination found a hyperpigmented plaque with central pink atrophy and a hypopigmented portion with follicular plugging, telangiectasias, and hyperkeratosis that was observed on examination (Figs 1 and 2). The plaque extended from the vermillion and mucosal lip to the upper cutaneous lip. Her hard and soft palate showed hyperpigmented macules and 2 erosions (Fig 3). There were xerotic, hyperpigmented and lichenified thin plaques on the bilateral anterior lower extremities (Fig 4). No fluorescence was observed on Wood's lamp examination of this area. Laboratory evaluation was significant for rheumatoid factor of 85 IU/mL, positive Sjogren antibody A and B, positive erythrocyte sedimentation rate, antinuclear antibody of 1:640 in a speckled pattern, and a C3/C4 complement level of 114 and 11 respectively. Results for cardiolipin antibodies, β-2 glycoprotein 1 antibodies, lupus anticoagulant, anti-Jo, anti-centromere, ribonucleoprotein antibody, DNA topoisomerase 1 antibody, rapid plasma reagin, HIV, creatine phosphokinase, QuantiFERON, and urinalysis were all unremarkable. An outside skin biopsy done on the upper cutaneous lip showed changes consistent with DLE. Her most recent eruption had been treated with intralesional triamcinolone acetonide and topical triamcinolone with minimal improvement.
Fig 1.

Cutaneous upper lip.
Fig 2.

Vermillion lip.
Fig 3.

Palatal involvement.
Fig 4.
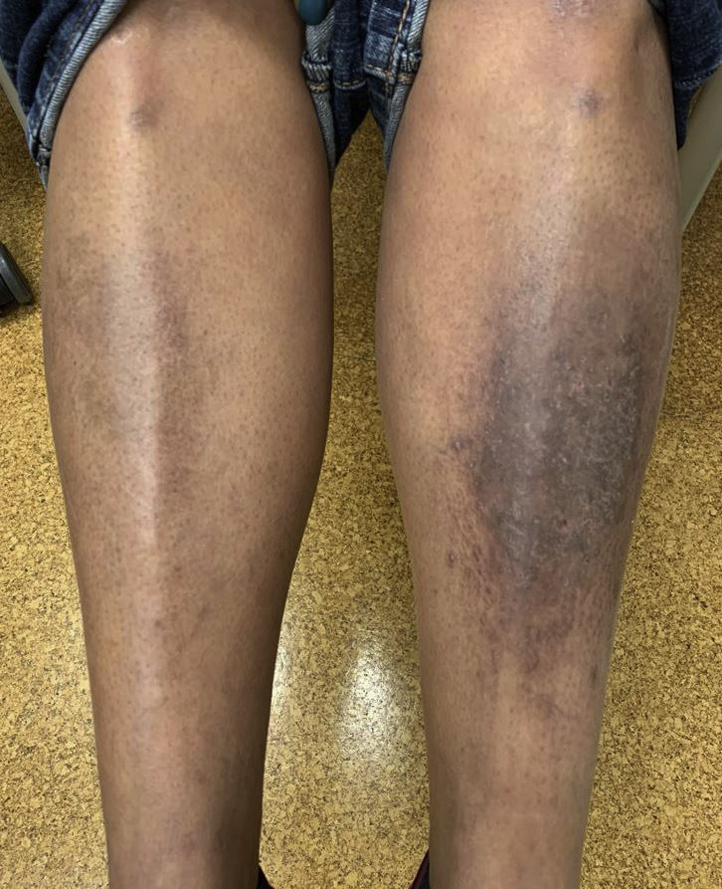
Lower extremity involvement.
Discussion
This patient's cutaneous eruption of the lip is clinically characteristic and histopathologically consistent with DLE. Although these features may represent a cutaneous flare of the patient's SLE, the lesion's development can be more thoroughly explained via Koebnerization secondary to heat exposure with EC usage.
DLE lesions begin as well-demarcated macules or papules that gradually expand into discoid, often coin-shaped plaques. Characteristic clinical features include induration and erythema with overlying scale, atrophy, follicular plugging, and pigmentary changes. Roughly 20% of patients with SLE go on to have DLE during their disease course; more than half of these patients have significant, destructive scarring; and a third have cicatricial alopecia.1, 3
The Koebner phenomenon, also known as the isomorphic response, represents an induction of inflammatory skin lesions as a result of cutaneous trauma, typically from friction, blunt trauma, or heat.4 Koebnerization most commonly occurs in psoriasis and lichen planus.4 Although the mechanism has not been fully elucidated, it likely involves an induction by environmental stimuli followed by the recruitment of autoimmune inflammatory cells and cytokines to the site of injury, such as tumor necrosis factor-α and intercellular adhesion molecule-1 in the case of trauma via heat.4 This autoimmune activation leads to the pathogenesis of Koebnerization and resultant lesions, characteristic to the patient's specific disease.4 Koebnerization among patients with SLE and DLE is relatively underreported in the current literature. Such patients typically present with skin lesions of lupus secondary to contact dermatitis, herpes zoster, or scar formation or external stimuli such as tattoos, scratching, or repetitive trauma from tight clothing.3 Koebnerization secondary to heat can lead to the development of erythema ab igne, which describes a characteristic skin pattern to a level of chronic heat exposure insufficient to cause an overt burn. Atrophy of the epidermis and deposition of melanin and hemosiderin are considered classic histopathologic features.5 Heat sources such as stoves, heating blankets, laptop computers, and electric radiators have been described as inciting causes.
ECs were first developed as an aid to smoking cessation, and their use has since risen steadily. An EC is designed to deliver vaporized nicotine, and is comprised of a mouthpiece, a cartridge containing nicotine suspended in a glycerine/polyethylene glycol base, a heating element, a microprocessor, and a battery.6 A variety of adverse effects have been reported caused by EC use, namely pulmonary complications caused by polyethylene glycol inhalation and burns secondary to contact with an overheating device.7 Although overheating leading to overt burns is not common, low-grade heat is transferred to the mouthpiece and the smoker during normal use via the heated, aerosolized nicotine solution.7
Our patient is a long-term, daily, active smoker, who uses an EC device. The central location on the vermillion border and upper cutaneous lip corresponds to the location of an EC mouthpiece during use, as confirmed by the patient herself. Although the patient was a long-time conventional cigarette smoker, she started using an EC; unfortunately, the patient has not altered her smoking habits despite counseling regarding cessation or changing the placement of electronic cigarette away from her lesion. Her disease remains active with continued exposure. Although the development of this lesion in this location may be entirely coincidental, low-grade chronic heat exposure may be a causal component of the pathogenesis of this lesion via Koebnerization. This case demonstrates an interesting insight into the role that chronic skin trauma caused by heat can play in the pathogenesis of cutaneous lupus and reveals another potential risk factor of the widespread and increasingly common use of ECs.
Footnotes
Funding sources: None.
Conflicts of interest: None disclosed.
References
- 1.Rothfield N., Sontheimer R.D., Bernstein M. Lupus erythematosus: systemic and cutaneous manifestations. Clin Dermatol. 2006;24(5):348–362. doi: 10.1016/j.clindermatol.2006.07.014. [DOI] [PubMed] [Google Scholar]
- 2.Berger E., Robinson M., Patel R., Andrew G.F., Jr. Koebner phenomenon to heat in cutaneous (discoid) lupus erythematosus (lupus ab-igne) Dermatol Online J. 2012;18(12):17. [PubMed] [Google Scholar]
- 3.De Berker D., Dissaneyeka M., Burge S. The sequelae of chronic cutaneous lupus erythematosus. Lupus. 1992;1(3):181–186. doi: 10.1177/096120339200100310. [DOI] [PubMed] [Google Scholar]
- 4.Ueki H. Koebner phenomenon in lupus erythematosus with special consideration of clinical findings. Autoimmun Rev. 2005;4(4):219–223. doi: 10.1016/j.autrev.2004.11.007. [DOI] [PubMed] [Google Scholar]
- 5.Miller K., Hunt R., Chu J., Meehan S., Stein J. Erythema ab igne. Dermatol Online J. 2011;17(10):28. [PubMed] [Google Scholar]
- 6.Jones C.D., Ho W., Gunn E., Widdowson D., Bahia H. E-cigarette burn injuries: Comprehensive review and management guidelines proposal. Burns. 2019;45(4):763–771. doi: 10.1016/j.burns.2018.09.015. [DOI] [PubMed] [Google Scholar]
- 7.Soule E.K., Nasim A., Rosas S. Adverse effects of electronic cigarette use: a concept mapping approach. Nicotine Tob Res. 2015;18(5):678–685. doi: 10.1093/ntr/ntv246. [DOI] [PMC free article] [PubMed] [Google Scholar]