

Abstract
Research demonstrates a mismatch between reported and observed maternal feeding practices. This mismatch may be explained by maternal cognitions, attitudes, and motivations relating to dyadic parent–child feeding interactions. These complex constructs may not be apparent during observations nor evidenced in self‐report questionnaire. Therefore, the aim of this study was to use a qualitative approach to gain a more nuanced and contextualized understanding of (a) maternal perceptions of children's food intake control; (b) how parent–child mealtime interactions influence maternal feeding practices; and (c) ways in which mothers may promote healthy child eating and weight outcomes. Semistructured telephone interviews were conducted with 23 mothers (M = 38.4 ± 3.7 years of age) of preschool‐aged children (M = 3.8 ± 0.6 years of age, 19 were normal weight, 14 were girls), who had previously completed child feeding questionnaire and participated in two home‐based mealtime observations, 12 months apart. Interviews were recorded, transcribed, and themes extracted to create the database. Four major themes emerged: (a) Maternal confidence in children's ability to regulate food intake is variable; (b) Implementing strategies for nurturing healthy relationships with food beyond the dining table; (c) Fostering positive mealtime interactions is valued above the content of what children eat; and (d) Situation‐specific practices and inconsistencies. Findings indicate that maternal feeding practices are shaped by both parent and child influences, and child feeding is mostly guided by controlling the family food environment, rather than by directly pressuring or restricting their child's eating. Results also highlighted the need for research to consider both parent and child influences on child feeding.
Keywords: childhood obesity, feeding practices, maternal perceptions, mealtime interactions, preschoolers
Abbreviations
- BDI‐SF
Beck Depression Inventory‐Short form
- BMIz
BMI‐for‐age z scores
- CDC
Centers for Disease Control and Prevention
- PC
participant code
- STAI‐IT
The State‐Trait Anxiety Inventory‐Trait Scale
- T1
time one
- T2
time two
1. INTRODUCTION
Parental use of controlling feeding practices has been implicated in children's eating and weight development (Gregory, Paxton, & Brozovic, 2010; Lumeng et al., 2012; Rodgers et al., 2013). In particular, parental controlling feeding practices, intended to either encourage or discourage when, how much and what children consume, have the potential to disrupt the development of children's dietary self‐regulatory processes (Jansen, Mulkens, & Jansen, 2007; Rollins, Loken, Savage, & Birch, 2014) and influence risk of childhood obesity (Shloim, Edelson, Martin, & Hetherington, 2015).
Studies comparing self‐reported controlling feeding practices and independently observed mealtime interactions fail to show consistency between actual and reported behaviours (Farrow, Blissett, & Haycraft, 2011; Haycraft & Blissett, 2008; Lewis & Worobey, 2011). These studies have, however, identified other important correlates associated with either reported or observed controlling feeding practices, such as maternal and child BMI (Farrow et al., 2011; Haycraft & Blissett, 2008) and maternal concern about child weight (Lewis & Worobey, 2011).
To date, only one published study (Bergmeier, Skouteris, Haycraft, Haines, & Hooley, 2015a) has evaluated relationships between reported and observed controlling practices both cross‐sectionally and prospectively across two time points (12 m apart). The study by Bergmeier et al. (2015a) also failed to show a significant direct association between reported and observed maternal controlling feeding practices. However, self‐reported use of pressure to eat was significantly and positively associated with observed pressure to eat at the second measurement time point, although only among girls. Observed restriction recorded during the first home visit inversely predicted child BMI‐for‐age z scores after 12 months.
Inconsistencies between reported and observed restrictive feeding practices may be accounted for in several ways. First, discrepancy may emerge as a function of comparing general feeding practices against specific practices applied during the time of the filmed meal interactions. For example, maternal self‐reports on the Child Feeding Questionnaire refer to general practices such as restricting sweet foods or encouraging the child to eat enough (Birch et al., 2001). However, actual feeding practices observed during two filmed meals may be subject to the specific constraints of those occasions.
Second, the low congruence between reported and observed feeding practices may involve the failure of the measures used in these previous studies to capture the bidirectionality of parent–child influences during meals. A systematic review of observational measures used to assess mother–child feeding interactions showed the measures implemented, adopting a top‐down uni‐directional perspective, where influence flows from parent to child (e.g., parenting control, support, responsiveness, and sensitivity; Drucker, Hammer, Agras, & Bryson, 1999; Hughes, Power, Fisher, Miller, & Nicklas, 2011). It is clear that observational measures commonly implemented do not comprehensively capture the influence that both the parent and child have on their shared interactions.
Developmental research recognizes that children are shaped by the reciprocal nature of the parent–child dyad; these interactions are necessarily bidirectional in nature (Harrison et al., 2011; Maccoby, 1983; 1999; Kochanska & Murray, 2000). For example, the extent to which children are able to self‐regulate short‐term energy intake, though not measured in the previous studies, has the potential to influence parental feeding practices and concern about child weight (Tan & Holub, 2011; Van den Berg et al., 2011). Believing that a child can regulate food intake is associated with lower restriction during meals (Tan & Holub 2011). Maternal cognitions, motivations, and attitudes that may explain if and why these suggested bidirectional and interactive effects between the parent and child influence feeding practices during mealtimes are complex constructs. Hence, they may not be adequately captured during observations nor evidenced in self‐report questionnaire (Bergmeier, Skouteris, & Hetherington, 2015b; Demir et al., 2012; Harrison et al., 2011; Kiff, Lengua, & Zalewski, 2011). For instance, although mothers may report their intended feeding practices (e.g., appropriate amount of pressure used to encourage child eating), this feeding ethos may be superseded by more immediate concerns (e.g., “is my child eating enough, will my child need to be encouraged to eat?”) when faced with a real‐time observation.
The primary aim of this follow‐up study was to use a qualitative approach to explore mothers' perceptions and experiences of child feeding interactions underpinning their practices, which may not have previously been identified in comparisons between reported and observed maternal feeding practices (Bergmeier, et al., 2015a; Farrow et al., 2011; Haycraft & Blissett, 2008; Lewis & Worobey, 2011). Mothers who had previously participated in a study evaluating relationships between reported and observed feeding practices (Bergmeier, et al., 2015a), were invited to take part. The specific objectives were to gain a contextualized understanding of (a) maternal perceptions of their child's dietary self‐regulation and (b) how parent–child mealtime interactions influence their feeding practices.
Much of the literature has focused on investigating behavioural predictors of obesity risk in children (Shloim et al., 2015); however, it is also necessary to document and investigate the practices used by mothers of children with normal BMI that promote healthy eating and maintain a healthy weight. Hence, the secondary aim of this study was to employ a qualitative approach to uncover strategies that may inform parents and practitioners to promote healthy eating and body weight.
Key messages.
Maternal feeding practices during meals may vary to account for contextual influences, including child characteristics.
Mothers prioritize promoting positive parent–child relationships and relationships with food during meals above the content of what their child eats.
A disconnect between reported and observed feeding practices may have arisen because self‐report measures fail to capture the bidirectionality of parent–child influences during meals.
2. MATERIALS AND METHOD
2.1. Participants
This study was approved by the Deakin University Human Research Ethics Committee and was conducted in Victoria, Australia. The current study comprised a subsample of 23 mothers who had previously participated in two filmed home‐based lunchtime observations with their preschool‐aged children (Bergmeier et al., 2015a).
2.2. Procedure
Details pertaining to the previous study's home visits have previously been published (Bergmeier et al., 2015). Questionnaire packs containing demographics, maternal mental health, child eating, child feeding, and parenting styles questionnaire, and reply paid envelopes were sent to participants at two time points 12 months apart (T1 and T2).
After the collection of data at T2, mothers who had provided consent to be contacted again regarding participating in future research (n = 81) were sent letters, plain language statements, and reply paid envelopes inviting them to take part in telephone interviews. Of the 28 participants who responded to the invitation, some (n = 3) did not answer follow‐up telephone calls; 1 stated that she was too busy; 1 mother said her child had been diagnosed with a neurological condition affecting eating; so in all, 23 mothers were interviewed between 11 and 23 months (M = 16.6; SD = 3.5) following the collection of T2 data. The interview schedule consisted of open and closed questions (see Table 1) and was developed to elicit mothers' perceptions of their preschool child's regulation of food intake, their child's weight development, their own feeding practices, and parent–child mealtime interactions. The first author of this paper (HJB) conducted all telephone interviews, which lasted approximately 30–45 min. The semistructured interview schedule guided the discussions; participants were encouraged to elaborate and provide examples where appropriate. Audiotapes of the semistructured interviews were transcribed verbatim, and speakers were tagged with their participant identification number in the transcripts.
Table 1.
Overview of semistructured interview schedule questions
| 1. Tell me about your child's capacity to decide if he or she has eaten enough. |
| 2. Can you give an example of a time that you have had to intervene when your child has eaten enough but has wanted to keep eating? |
| 3. If you have to intervene, how often do you feel you need to do so and what strategies do you use? |
| 4. Can you give me an example of what happens when your child asks for more food? |
| 5. Under what circumstances would you hide certain foods from your child? How often do you hide foods from your child? |
| 6. If your child was given free access to any food group, including novelty foods such as confectionary, chips, and desserts, what do you think they would do? Why do you think this is the case? |
| 7. How impulsive is your child around food? Can you give an example of a time when your child has held off on a food that they really liked? (e.g., when full, when wanted to wait until later, or when saving it for a special occasion). |
| 8. How often does your child refuse to eat? How do you respond? |
| 9. How would you describe the quality of your relationship with your child during meal times? How does the quality of your relationship with your child during meal times compare to the quality of your relationship during other times of the day? |
| 10. If you would like your child to eat their vegetables, how do you ensure this happens? |
| 11. If you would like your child to pack up their toys, how would you ensure this happens? |
| 12. How satisfied are you with your child's weight development? |
| 13. Do you ever worry that your child could be underweight or overweight? If so, why might that be the case? |
2.3. Measures
Mothers were asked to complete a home observation typicality ratings questionnaire at the completion of each home visit to confirm the extent to which filmed mother–child interactions and routines were consistent with their usual practices. Weight and height for mother–child dyads were collected by trained research staff during each home visit using standardised anthropometry equipment. Maternal BMI was subsequently calculated (weight/height2, kg/m2), and child BMI‐for‐age z scores were computed according to the Centers for Disease Control and Prevention (Ogden et al., 2002) criteria.
Characteristics of mothers that might influence their feeding practices were collected to explore how the profiles of this sample may represent a subgroup of the population associated with the use of more healthful child feeding characteristics (Harrison et al., 2011; McPhie, Skouteris, Daniels, & Jansen, 2014): The State‐Trait Anxiety Inventory‐Trait Scale (STAI‐IT; Spielberger & Reheiser, 2009) was administered to assess the frequency of maternal anxiety symptoms. The 20 items are scored from 1 to 4, with possible scores ranging from 20 to 80. A mean score of 36.35 (SD = 11.39) has been reported in an Australian adult population (Crawford et al., 2009). The 13‐item Beck Depression Inventory‐Short form (Beck & Beck, 1972) was used to assess the presence and severity of maternal depressive symptoms. Items are scored from 0 to 3, and possible total scores could range from 0 to 39. Mean scores for females in a general population sample have been shown to be 2.8 (SD = 3.5; Knight, 1984). Mothers were also asked to report sociodemographic information including their highest level of education achieved and annual family income.
2.4. Data analysis
Analysis of the transcripts proceeded in line with the steps outlined by Braun and Clarke (2006) for thematic analysis. Thematic analysis is a widely used foundational, theoretical method of qualitative analysis for extracting rich and detailed meanings from data (Braun & Clarke, 2006). The analysis considered inductive (bottom‐up approach where meaning is driven by the data itself) and latent (examines underlying ideas, assumptions, and conceptualisations of the data) levels of analysis and comprised of the phases outlined in Figure 1.
Figure 1.
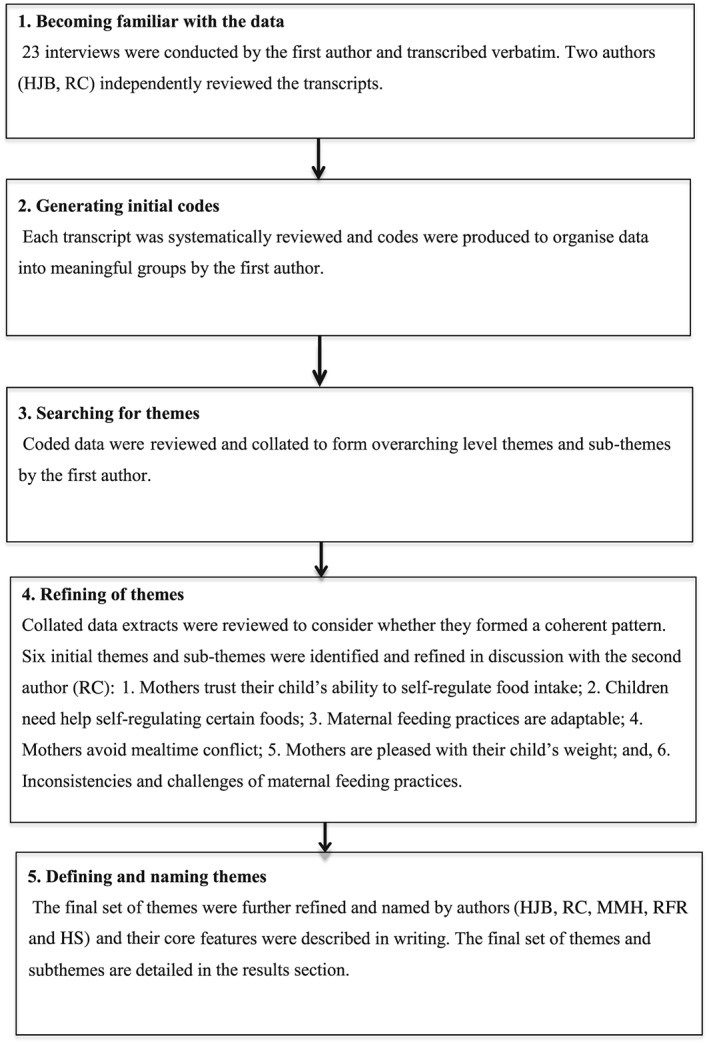
Phases of thematic analysis (based on Braun & Clarke, 2006)
3. RESULTS
Mother and child participant characteristics are presented in Tables 2, 3, showing the sample comprised predominately of well‐educated mothers of children with a healthy weight range. Mean maternal anxiety and depression scores aligned with the general population. There were no significant differences between mothers who participated in the semistructured interviews and those who did not respond to the follow‐up study invitation.
Table 2.
Characteristics of mother–child dyads
| Characteristics | Interviewed (n = 23) | No Follow Up (n = 75) |
|---|---|---|
| Maternal | ||
| BMI classificationa (mean ± SD) | 24.9 ± 4.1 | 26.7 ± 5.6 |
| Obese, n (%) | 3 (13.0) | 11 (15.5) |
| Overweight, n (%) | 6 (26.1) | 30 (42.3) |
| Healthy weight, n (%) | 14 (60.9) | 30 (42.3) |
| Depression (mean ± SD) | 2.7 (2.2) b | 3.8 (3.3) c |
| Anxiety (mean ± SD) | 37.1 (7.1) d | 37.1 (9.5) e |
| Age, y (mean ± SD)f | 38.4 ± 3.7 | 37.6 ± 4.5 |
| Country/region of birth, (mean) | Australia | Australia |
| Australia, n (%) | 20 (86.6) | 56 (74.7) |
| Europe, n (%) | 1 (4.3) | 8 (10.6) |
| New Zealand, n (%) | 1 (4.3) | 4 (5.3) |
| North America, n (%) | 1 (4.3) | 1 (1.3) |
| Middle East, n (%) | 0 | 1 (1.3) |
| Southern and Central Asia, n (%) | 0 | 2 (2.7) |
| Southern, Central and West Africa, n (%) | 0 | 3 (4.0) |
| Annual Family Incomeg (mean range) | A$85–105,000 | A$85–105,000 |
| Above A$145,001, n (%) | 5 (21.7) | 9 (12.1) |
| A$85,001–$145,000, n (%) | 7 (30.4) | 42 (56.7) |
| A$45,001–$85,000h, n (%) | 8 (34.8) | 19 (25.7) |
| Below A$45,000, n (%) | 2 (8.7) | 4 (5.4) |
| Highest Level of Education (mean) | Graduate diploma | Graduate diploma |
| Tertiary qualification achieved, n (%) | 17 (73.9) | 51 (68.0) |
| Child | ||
| BMI classificationi (mean ± SD) | 16.7 ± 1.1 j | 15.8 ± 1.7 k |
| Obese, n (%) | 1 (4.7) | 2 (3.2) |
| Overweight, n (%) | 1 (4.7) | 6 (9.3) |
| Healthy weight, n (%) | 19 (90.5) | 42 (67.7) |
| Underweight, n (%) | 0 | 12 (19.3) |
| Age, y (mean ± SD)i | 3.8 ± 0.6 | 3.9 ± 0.8 |
| Sex (M/F), n (%) | 9 (39.0)/14 (61.0) | 37 (49.0)/38 (51.0) |
Based on adult cutoff points, which classify a BMI of 25 kg/m2 as overweight and 30 kg/m2 as obese (Cole et al., 2000), collected at second home visit.
Sample score range: 0.0–08.0.
Sample score range: 0.0–15.0.
Sample score range: 24.0–50.0:
Sample score range: 21.0–64.0.
Maternal age at second home visit.
Family income data not reported by one mother.
Recent data show the median Australian gross household income is approximately A$72,000 (Greenville, Pobke, & Rogers, 2013). bSample score range: 0.0–08.0. cSample score range: 0.0–15.0. dSample score range: 24.0–50.0: eSample score range: 21.0–64.0. kChild age at second home visit.
Based on objective measures of child weight and height, age appropriate BMI classifications (Ogden et al., 2002), collected at second home visit.
Objective child BMI data not available for two children.
Objective child BMI data available for 62 children.
Table 3.
Reported mother–child dyad food preparation and mealtime routines at time one (T1) and after 12 months at time two (T2)
| T1 (n = 21)a | T2 (n = 23) | |
|---|---|---|
| Do you usually ask your child what they would like for lunch? | ||
| Yes | 17 | 18 |
| Is your child near you when you prepare their meal? | ||
| Yes | 20 | 20 |
| How often do you interact/engage with your child when preparing their meal? | ||
| All the time | 8 | 7 |
| Usually | 11 | 12 |
| Sometimes | 2 | 3 |
| How do you engage your child? | ||
| Discuss what you are making | 19 | 20 |
| Involve them in preparation | 17 | 17 |
| Play with them or talk | 13 | 18 |
| Where does your child usually eat? | ||
| Table/kitchen bench/children's table | 21 | 22 |
| How often is the TV on? | ||
| All the time | 1 | 0 |
| Usually | 1 | 3 |
| Sometimes | 4 | 3 |
| Rarely | 5 | 6 |
| Never | 10 | 11 |
| Does your child require assistance when eating? | ||
| Yes | 9 | 6 |
| What kind of assistance does your child require? | ||
| Cutting up food | 8 | 2 |
| Feeding | 1 | 0 |
| Encouragement to eat | 6 | 4 |
| How often do you sit with your child while eating? | ||
| Almost never | 4 | 2 |
| Sometimes | 1 | 4 |
| Often | 12 | 11 |
| All the time | 4 | 5 |
| How often do you eat with your child? | ||
| Almost never | 2 | 0 |
| Sometimes | 5 | 3 |
| Often | 12 | 13 |
| All the time | 2 | 6 |
Mealtime questionnaire completed by 21/23 mothers at T1.
Four major themes emerged from the interviews (see Table 4): (a) Maternal confidence in children's ability to self‐regulate food intake is variable; (b) Implementing strategies for nurturing healthy relationships with food beyond the dining table; (c) Fostering positive mealtime interactions is valued above the content of what children eat; and (d) Situation‐specific practices and inconsistencies. Within major themes, subthemes were identified, along with supporting quotes. Quotes are verbatim from participants (PC = participant code). Colloquial language such as “um” was removed to improve readability. With the exception of quoted descriptions, the term “unhealthy” has been used in this paper to describe mothers' references to energy‐dense, low‐nutrient foods and diets; the term “healthy” describes references to nutrient‐dense foods and balanced diets.
Table 4.
Frequency of emerging themes and subthemes
| Emerging Themes | Frequency |
|---|---|
| Maternal confidence in children's ability to self‐regulate | 23 |
| Trust in children's self‐regulation is learned over time | 8 |
| The important of parenting experience | 17 |
| Implementing strategies for nurturing healthy relationships with food beyond the dining table | 22 |
| Using health reasoning | 6 |
| Limit setting | 14 |
| Using covert practices | 22 |
| Fostering positive mealtime interactions is valued above content of what children eat | 8 |
| Fostering parent–child interactions | 8 |
| Reflecting on childhood experiences | 12 |
| Avoiding battles over food | 11 |
| Trying before rejecting it | 8 |
| Situation specific practices and inconsistencies | 15 |
3.1. Maternal confidence in children's ability to self‐regulate food intake is variable
Mothers spoke confidently about their trust in their children's capacity to self‐regulate food intake, particularly in relation to deciding when they had eaten enough. Overall, mothers were adamant that their children provided clear cues that they had the capacity to self‐regulate their eating, and they indicated this by stopping eating, playing with their food, or vocalizing that they had reached a state of satiety. Two subthemes relating to maternal experiences of children's dietary regulation emerged: (a) Trust in children's regulation is learned over time and (b) The importance of parenting experience.
3.1.1. Trust in children's regulation is learned over time
Discussions revealed that for the majority of mothers, trust in their child's capacity to self‐regulate food intake had not been instinctive but rather developed over time in line with gains in parenting experience. In particular, mothers' responses largely indicated that being able to recognize associations between variations in children's appetite and physiological factors (i.e., growth spurts, illness, and energy expenditure) had enabled them to obtain evidence of their children's ability to respond to their innate satiety cues:
“She seems to go through growth spurts but at the moment she's eating like a horse. She just eats, and eats, and eats, and eats. You give her a full meal and she wants more. I think possibly she eats more than me some days…it might go on for I'd say two or three weeks. When she's not having a growth spurt, probably the majority of the time, she doesn't finish meals.” (PC 16; Journalist and mother of two)
This example illustrates the trust this mother places in her child to decide how much to eat depending on physiological requirements, which vary according to growth or hunger. Trust in the self‐regulatory system as a means to balance out large or frequent meals is demonstrated by this mother's confidence that variability is typical and appears not to warrant concern. In addition, this mother notes the timescale of regulation (more than a day or so), which compared well with scientific evidence of regulation in adults (see de Castro, 2000).
3.1.2. The importance of parenting experience
A number of mothers also described how learning about their children's dietary self‐regulation had been based on “trial and error”. For instance, they reported that child birth order influenced their approach, becoming more confident and relaxed about their children's eating with each addition to the family. This was due in part to observing firstborns “grow out of” challenging feeding stages and the time to develop effective parenting approaches, thus gaining confidence to guide their later born children's eating behaviours. The following quote represents this idea:
“…I was probably more conscious of what the book was saying to do as opposed to observing his cues…and I am much more relaxed the second time around…It takes time to learn to read someone.” (PC 06; Nurse and mother of two)
This example illustrates that although mothers are confident that children are capable of self‐regulating food intake, nevertheless, there is a skill in understanding the specific cues provided by each child. Thus, replacing reliance on books with learning “to read” their child's signals.
3.2. Implementing strategies for nurturing healthy relationships with food beyond the dining table
Although mothers reported feeling confident in their child's ability to self‐regulate food intake, they acknowledged that there were circumstances during which they felt it was necessary to guide their child's eating; those instances predominantly related to specific “favourite” foods, i.e., those with high energy density and highly palatable snacks, such as sweets or biscuits. Mothers reported placing a higher priority on implementing practices designed to nurture healthy relationships with food, rather than applying fixed food rules about when, what, and how much a child should eat; believing this would help their children to become independent healthy eaters. Three subthemes relating to maternal strategies designed to reduce children's unhealthy eating emerged: (a) Mothers used health reasoning to encourage their children to limit their unhealthy food consumption; (b) Mothers involved their children in discussions about setting limits on favourite food intake; and (c) Mothers used covert practices to limit their child's unhealthy food intake.
3.2.1. Using health reasoning to limit children's unhealthy food consumption
When asked to provide examples of occasions when they thought they needed to guide their child's eating, mothers emphasized that it was important that their children understood the health implications of eating unhealthy foods, such as experiencing low energy levels. Mothers were particularly conscious of using language that would help their children focus on the nutritional benefits of food as they did not wish to highlight problematic eating behaviours or body image issues. Hence, they attempted to avoid using food descriptions such as “fattening” or “bad” foods.
Mothers also commented that their children appeared interested in learning about the relationship between nutrition and health and described instances when children had attempted to apply their learned health knowledge:
“…if she eats half and has had enough… I'll relate it to a particular activity, like I'll say: 'you know how you want to learn how to run and run really fast and ride your bike really fast, you have to eat really healthily’…so we will have that conversation (about nutritional content of food), to give her an example so she can understand why we have to eat well. And it's interesting because she'll say, 'Daddy doesn't eat well and he can't run or ride a bike’.” (PC 04; Nurse and mother of two)
These quotes illustrate the ways in which children themselves (voiced through the accounts of their mothers) accept and repeat ideas about healthy lifestyles from dominant discourses including those which link healthy eating to well‐being. This suggests ways in which children become “health literate” even in early life, where mothers make efforts to connect physical well‐being with nutrition and having the energy to engage in activities fuelled by food.
3.2.2. Involving children in discussions about setting limits on unhealthy food
Mothers' responses indicated that they believed that restricting particular foods could in fact increase their child's desire for that specific food item:
“The truth is I don't want them eating all the junk stuff but I don't want them to get that excited that when they see it they can't help themselves either, so I try and do a bit of moderation.” (PC 21; Human resources manager and mother of three)
Instead, mothers sought to involve their children in discussions about setting limits on favourite food intake by encouraging them to consider which foods should be eaten regularly and which ones should be eaten infrequently. When making decisions about unhealthy food, many of the mothers invited their children to think about how much they should eat in one sitting in order to promote opportunities for them to become healthful, independent eaters, as well as reduce the level of maternal control required during eating:
“If he's had a choc‐chip cookie today, and then later in the day, someone says, ‘would you like a biscuit?’, he'll say: ‘no, I've already had my choc‐chip cookie today.’ So he knows that that's an occasional food and that we don't like to have it too regularly sort of thing.” (PC 08; Teacher and mother of two)
Guidance on portion control (having one biscuit or no more than two sweets) has been provided to children who have in turn accepted the need for limits. This further illustrates the notion of learning about health literacy, including adjusting portions of highly palatable food items.
3.2.3. Using covert practices to limit children's unhealthy food consumption
Another subtheme that emerged was the use of covert practices to guide their child's eating choices in order to limit intake of undesirable foods and limit their need to exert restrictive feeding practices. Common strategies included reducing their child's exposure to unhealthy types of food by controlling the home food environment (e.g., not purchasing certain foods and keeping these foods on a high shelf out of child's line of vision) and instead providing wide access to healthy types of food (e.g., fruit bowls on display):
“Lollies or cakes or junk sort of stuff goes in our pantry, is up quite high, not at immediate eye range so I try to keep things that I am not overly excited about them eating less visible, but I've always got a bowl of fruit on display.” (PC 21; Human resources manager and mother of three)
This quote illustrates the tension between trusting children to self‐regulate food intake but having to deploy a variety of covert practices to support that self‐regulation and food choices. On the one hand, mothers trust their child to know what to eat but some foods are identified as “high risk” to the dietary regulation ethos. In addition to providing overt guidance about serving size, covert practices ensure that undesired foods are out of sight or out of reach, providing another level of control. In contrast, fruit, which represents “healthy” foods, is made available and is in clear sight for ease of access. If mothers were entirely confident that children would self‐regulate intake of highly palatable foods, these too might be in view and easy to access. Thus, mothers are aware of the power of certain foods to be tempting and capable of undermining self‐regulation.
3.3. Fostering positive mealtime interactions is valued above the content of what children eat
When asked to reflect on the quality of parent–child interactions during eating, the majority of mothers described mealtimes as being equally or more enjoyable than other shared daily activities. Four subthemes relating to strategies mothers used to foster positive‐mealtimes emerged: (a) fostering positive parent–child interactions; (b) reflecting on mother's own childhood mealtime experiences; (c) avoiding battles over food; and (d) trying food before rejecting it.
3.3.1. Fostering positive parent–child interactions
Most mothers reported viewing mealtimes as providing regular occasions for families to gather and enjoy each other's company; mealtimes presented unique opportunities to focus on interacting with their child, compared to other shared daily activities, when mothers' attention was typically divided between multiple demands:
“I'm probably more engaged with him during meals. I find as a parent it's really hard; I work part time, on the days that I'm home I feel so busy, I'm with them, but I'm doing laundry, or I'm cleaning the dishes or I'm preparing a meal…most nights we would sit down at the dinner table and that's our coming together to share what's happened today.” (PC 06; Nurse and mother of two)
This example illustrates the ways in which meals offer a time of social interaction. These times are considered precious, focused, and more mindful than other occasions, which are more busy, chaotic features of daily life. As an example, it provides an insight into the importance placed on meals as a protected time, and ideally as a time to focus on food and on being together.
3.3.2. Reflecting on childhood mealtime experiences
Mothers thought about their own childhood experiences when considering the best practices to use to facilitate positive mealtime interactions. Although mothers said they had adopted many of their own parents' general approaches to child rearing, some of the mothers attributed their own or their siblings' persistent eating and weight issues to negative child feeding experiences, such as being forced to clean the plate, to eat beyond satiety, or to eat food they strongly disliked (examples of pressure to eat):
“I have a brother who had a real fear of food as a child. He would eat very little and I think mum and dad just tried to push him and push him and every mealtime was a battle. And they never won the battle…That food phobia has continued into adult life…in the eighties there was no psychology to deal with that kind of thing so I think we both agree that to push doesn't help. And I've always had the attitude that I wouldn't push the kid so I just encourage him, try and just model good eating habits.” (PC 08; Teacher and mother of two)
This example shows the link between past and present experiences during meals, and that memories of problem eating were still evident in relation to current meal practices, specifically not pressuring children to eat certain foods but accepting that foods vary in their appeal and that modelling intake promotes healthy eating. Again, this utterance underlines the need for guidance in encouraging children to eat (that regulation is not entirely innate), but that too much pressure produces a negative outcome.
3.3.3. Avoiding battles over food
Mothers emphasized the importance of fostering positive mealtime interactions to build healthy relationships with food, including a conscious avoidance of conflict around food:
“So there are some things he doesn't like but I don't think it matters that he doesn't eat it...His Dad has never been able to eat fresh tomato, and he (child) just can't, so I just thought, he chooses and if he doesn't like it, he doesn't like it. I always keep offering it. I always put tomato on his plate but he is very consistent in not liking it.” (PC 07; Stay at home mother of two)
“If she doesn't want bananas, I know that she's not going to eat them at the moment. There are other alternatives, other fruits, so it's not a big deal… I've got my own battles with food; I don't want to give them any.” (PC 11; Stay at home mother of two)
These examples provide an important insight into the meal as a potential time of conflict. This was hinted at above in relation to mothers' memories of their own mealtimes as children, and here, there is a suggestion of food as a source of conflict (e.g., “battles”, and presenting food repeatedly even when it is clear it is not likely to be eaten). Mothers may be suggesting that they are aware of not allowing meals to be a time of conflict, while admitting that they themselves may have their own issues (current or historic) around food to consider.
3.3.4. Trying food before rejecting it
Although mothers generally reported avoiding conflict and not enforcing strict food rules, many mentioned that they wanted their children to try food before rejecting it:
“She doesn't like peas, she's not keen on peas but she'll try it. She might just go ‘Mum they are disgusting’, and I'll go, ‘that's fine but you tried it’. We don't make a fuss about it too much.” (PC 14; Receptionist and mother of one)
Overall, these quotes demonstrate the difference between a general ethos to trust the child's capacity to self‐regulate food intake (to know what is best) but still wishing to provide a disliked food as a means to expand the repertoire of acceptable foods. This underlines the stark difference between those foods, which mothers apply covert practices to limit (high energy, palatable foods) and overt practices to encourage intake of low energy dense, less palatable foods, simultaneously avoiding conflict at the meal by not pressuring children to eat a certain food.
3.4. Situation‐specific practices and inconsistencies
Although our sample comprised of predominantly mothers who disclosed their conviction to promote positive parent–child mealtime interactions, a number of surprisingly inconsistent practices emerged, with some mothers acknowledging variability of their practices from day to day. Overarching reasons given for these inconsistencies included (a) whether mothers had the energy to follow through with their ideals; (b) considerations for children's energy intake and expenditure on a particular day (i.e., “what has my child eaten and how much running around have they done?”; and (c) children's individual characteristics:
“He's pretty good with new foods. He'll give something a try. Sometimes he won't. But sometimes he will just flat out refuse to eat what I've put on his sandwich…(how I respond) depends on how strong and stubborn I feel.”
(PC 10; Stay at home mother of two)
“I think it is their personality, but also the fact that once you've got two of them, you are working full time, you need to get them to bed after child care; I'm probably not as patient as I used to be.” (PC 18; Engineer and mother of two)
These quotes illustrate an inconsistent application of mothers' feeding ethos. Thus, mothers themselves are aware of the discrepancy between holding a general feeding ethos but having to adapt to situational and contextual constraints. Mothers are clearly holding opposing views, which they must negotiate day to day. On the one hand, having confidence that children are able to regulate food intake and, on the other hand, ensuring limits are placed on tempting foods, similarly, presenting mealtimes as an ideal social interaction and positive focus, yet acknowledging the potential for conflict around foods, which may be disliked or unwanted. Daily negotiations are set against a background of childhood memories, current knowledge, and having the “energy” to pursue the greater goal of achieving a healthy diet and a balanced approach to feeding.
Another inconsistency noted throughout the discussions was that some mothers did not seem able to distinguish between concepts relating to practices designed to guide children's eating, such as teaching children to set limits on the consumption of unhealthy food and the enforcement of fixed food rules. For instance, two of the mothers had put locks on their pantries to enable them to monitor what their children ate throughout the day, another mother said she helped her child learn to limit her confectionary intake by allowing her to eat the same amount of sweets as her current age, and other mothers had rules about which foods were negotiable:
“Generally if I use a veggie stir fry mix, there's something they don't like, I might give them the option to leave one thing, but they can only leave one thing. So I want them to eat all of their vegetables but if there is one thing that they hate, that's ok, but they're not allowed to hate their breaky (breakfast).” (PC 21; Human resources manager and mother of three)
“I do have friends who think it's funny that my kids ask for a fruit course after they've had tea. They know they can't have anything for dessert unless they've got a plate of fruit first.” (PC 12; Stay at home mother of three)
Interestingly, the mothers here demonstrate the tension between the ideal and the practical in trusting children to know what is best. The very nature of the negotiation is one of compromise, balancing responsiveness against demandingness to guide healthy choices. This in part may help to explain the disconnect between reported and observed feeding practices in the research context.
4. DISCUSSION
To our knowledge, this study was the first to conduct follow‐up interviews with mothers who had previously been involved in research assessing relationships between observed and self‐reported controlling feeding practices. It was evident that many of the approaches undertaken by mothers certainly aimed to nurture children's positive feeding experiences and healthy relationships with food. However, it was also clear that parenting within the mother feeding and child eating context is unique, compared to other parenting domains (e.g., asking children to keep a tidy room), in the extent that mothers pondered over striking the optimal balance between instilling healthful eating practices and inadvertently promoting increased desire for foods that they wished their children consumed sparingly and associated weight issues to. Moreover, decisions relating to practices executed during the feeding and eating context appeared to be weighed against the relational, emotional, and physical values mothers and their children attached to food.
Our interviews also revealed that although mothers' strategies were often inconsistent across meals, this sometimes reflected gains in parenting acumen, with mothers adjusting approaches in line with their children's situational needs, largely guided by children's temperamental traits, developmental shifts (i.e., improved language skills and ability to feed self), and mothers' capacity to be in tune with their child and accommodate practices accordingly. To a lesser extent, the execution of consistent practices was also driven by mothers' capacity (i.e., energy levels) on a given day. The profile of mothers in our study represented a subgroup of the population that has been associated with lower use of problematic feeding practices (Harrison et al., 2011; McPhie et al., 2014). However, the literature recognizes that child weight development is shaped by interactions between child (i.e., self‐regulation and genetic predisposition to obesity) and parental characteristics (e.g., parenting styles, parenting practices, nutritional knowledge, education, and diet), which interact with broader factors (e.g., advertising of energy‐dense foods for children; Harrison et al., 2011; Mitchell, Farrow, Haycraft, & Meyer, 2013). Therefore, it is not surprising that despite the best intentions, maternal feeding practices are subject to variability.
The findings simultaneously revealed that mothers were particularly mindful of promoting positive child eating behaviours and relationships with food, thus sought to limit overt controlling feeding practices. In contrast to these controlling feeding practices, associated with disrupting children's innate ability to gauge satiety cues (Rollins et al., 2014; Rodgers et al., 2013), health reasoning and limit‐setting approaches used by mothers in our study may allow parents to guide children's eating in a way that promotes regulation. These strategies appear to align with the structured‐based feeding framework proposed by Rollins, Savage, Fisher, and Birch (2015), which involves the parental provision of consistent rules and routines that consider the child's perspective and allows for joint problem solving. Furthermore, battles surrounding restricting children's unhealthy food consumption during mealtimes were largely avoided by controlling the home food environment (i.e., rarely purchasing unhealthy food options and providing unrestricted access to healthy food choices). Although overt and covert control strategies are positively correlated, they are conceptually distinct constructs (Ogden et al., 2006); given that the latter strategy is intended to occur without the child's awareness, it is unlikely to be evident during mealtime observations.
The practice of putting locks on pantries, as described by two mothers, was inconsistent with the same mothers who reported confidence in their children's general ability to self‐regulate food intake. These views were also at odds with the perspectives expressed by the majority of the participants. The mothers explained that the practice allowed them to monitor how often their children accessed the pantry; however, it reiterates the limitations of relying on mothers to fully understand the level of control their practices may elicit, accurately report their practices, and understand the potential influence these practices could have on child eating.
Mothers in our study viewed mealtimes as unique opportunities to nurture parent–child relationships and foster children's healthier long‐term relationships with food. Parent feeding practices denote what parents do to guide child eating. However, the parent and child each contribute to the quality of the shared relationship, which sets the relational context in which parent‐feeding interactions occur (Jansen, Daniels, & Nicholson, 2012; Skouteris et al., 2011). There is now evidence linking parent–child relationship quality with self‐regulation and child weight status (Anderson & Keim, 2016; Blewitt, Bergmeier, Macdonald, Olsson, & Skouteris, 2016). Hence, it is possible that any disconnect between reported and observed feeding practices in this sample may be due to limitations of the measures to identify and assess contextualized bidirectional parent–child interactions that shape maternal feeding practices during feeding (Bergmeier et al., 2015b).
It is also important to note that although other studies comparing maternal reported and observed feeding have shown relationships between maternal weight (or weight concerns) and feeding practices (Blissett & Haycraft, 2011; Musher‐Eizenman, de Lauzon‐Guillain, Holub, Leporc, & Charles, 2009), mothers in our study appeared to demonstrate a good deal of insight into their own histories of negative relationships with food and weight issues and had taken steps to become informed about nutrition as well as how to best nurture healthy child eating behaviours; most children had a BMI within the healthy weight range.
Findings relating to mealtime routines and interactions revealed that most mothers asked their child what they would like to eat. Children who are actively involved in deciding what to eat presumably find their meals appealing, and their parents are less inclined to feel the need to prompt their children to eat (Dovey, Staples, Gibson, & Halford, 2008; Mitchell, Farrow, Haycraft, & Meyer, 2013). Given that parents also reported controlling the home food environment as a way of encouraging healthy eating, it is likely that they are confident that if they allow their child to choose their meals, they will be doing so from a range of options that they are happy for them to eat.
We must acknowledge that this study had a number of limitations. First, data included in the previous study evaluating self‐reported and observed feeding practices could not be crossed matched with the current study's interview findings as some of the videos (6/23) were excluded from the original analysis (see Bergmeier et al., 2015a). Data were collected via telephone, and this may be considered a limitation. However, a review of face‐to‐face and telephone interview approaches showed there is little evidence that the interpretation or quality of findings is compromised when data are collected by telephone (Novick, 2008). Also, it is not clear that the data were free from contamination in that mothers may have been primed to think about their mealtime interactions given their involvement in the previous study's mealtime observations and completion of self‐report questionnaire on feeding practices. Nevertheless, it is argued that despite these potential limitations, the findings reveal much about why reported and observed mealtime feeding practices might be discrepant and provide insights into the complexity of the meal as a time for promoting healthy eating, providing a social occasion to enjoy, and a time to avoid conflicts around food. Self‐report measures are always subject to social desirability issues, and observational studies are subject to problems with behaving for the camera. Nonetheless, mothers demonstrate significant insight into the balance to be struck between a general feeding practice ethos, and the pragmatic, specific strategies needed to promote self‐regulation, healthy food choice, and meals as an ideal time for social engagement and learning. Strategies described by mothers may benefit parents and practitioners working to alter child eating behaviours and weight status.
Further research using high‐quality longitudinal data capturing parent, child, and dyadic level interactions around feeding routines is needed to further our understanding of the potential influence that mother–child mealtime interactions may have on strategies aimed at altering child feeding and weight trajectories.
SOURCE OF FUNDING
This research was part of an Australian Research Council Discovery Grant (DP1092804).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
HJB and HS designed the study. HJB recruited participants and conducted the interviews. HJB and RC analysed the data. HJB, RC, HS, MMH, and RFR refined themes. HJB drafted the manuscript. All authors have read and commented on drafts of this paper.
ACKNOWLEDGMENT
We would like to thank all the women who kindly participated in this study and shared their time and experiences with us.
Bergmeier HJ, Skouteris H, Hetherington MM, Rodgers RF, Campbell KJ, Cox R. Do maternal perceptions of child eating and feeding help to explain the disconnect between reported and observed feeding practices?: A follow‐up study. Matern Child Nutr. 2017;13:e12420 10.1111/mcn.12420
REFERENCES
- Anderson, S. E. , & Keim, S. A. (2016). Parent–child interaction, self‐regulation, and obesity prevention in early childhood. Current Obesity Reports, 5(2), 192–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck, A. T. , & Beck, R. W. (1972). Screening depressed patients in family practice: A rapid technique. Postgraduate Medicine, 52, 81–85. [DOI] [PubMed] [Google Scholar]
- Bergmeier, H. J. , Skouteris, H. , Haycraft, E. , Haines, J. , & Hooley, M. (2015a). Reported and observed controlling feeding practices predict child eating behavior after 12 months. The Journal of Nutrition, 145(6), 1311–1316. [DOI] [PubMed] [Google Scholar]
- Bergmeier, H. , Skouteris, H. , & Hetherington, M. (2015b). Systematic research review of observational approaches used to evaluate mother–child mealtime interactions during preschool years. The American Journal of Clinical Nutrition, 101(1), 7–15. [DOI] [PubMed] [Google Scholar]
- Birch, L. L. , Fisher, J. O. , Grimm‐Thomas, K. , Markey, C. N. , Sawyer, R. , & Johnson, S. L. (2001). Confirmatory factor analysis of the child feeding questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite, 36(3), 201–210. [DOI] [PubMed] [Google Scholar]
- Blewitt, C. , Bergmeier, H. , Macdonald, J.A. , Olsson, C.A. and Skouteris, H. , 2016. Associations between parent–child relationship quality and obesogenic risk in adolescence: A systematic review of recent literature. Obesity Reviews . [DOI] [PubMed]
- Blissett, J. , & Haycraft, E. (2011). Parental eating disorder symptoms and observations of mealtime interactions with children. Journal of Psychosomatic Research, 70(4), 368–371. [DOI] [PubMed] [Google Scholar]
- Braun, V. , & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. [Google Scholar]
- Cole, T. J. , Bellizzi, M. C. , Flegal, K. M. , & Dietz, W. H. (2000). Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ, 320(7244), 1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford, J. R. , Garthwaite, P. H. , Lawrie, C. J. , Henry, J. D. , MacDonald, M. A. , Sutherland, J. , & Sinha, P. (2009). A convenient method of obtaining percentile norms and accompanying interval estimates for self‐report mood scales (DASS, DASS‐21, HADS, PANAS, and sAD). British Journal of Clinical Psychology, 48(2), 163–180. [DOI] [PubMed] [Google Scholar]
- de Castro, J. M. (2000). Eating behavior: Lessons from the real world of humans. Nutrition, 16(10), 800–813. [DOI] [PubMed] [Google Scholar]
- Demir, D. , Skouteris, H. , Dell'Aquila, D. , Aksan, N. , McCabe, M. P. , Ricciardelli, L. A. , … Baur, L. A. (2012). An observational approach to testing bi‐directional parent–child interactions as influential to child eating and weight. Early Child Development and Care, 182(8), 943–950. [Google Scholar]
- Dovey, T. M. , Staples, P. A. , Gibson, E. L. , & Halford, J. C. (2008). Food neophobia and ‘picky/fussy'eating in children: a review. Appetite, 50(2), 181–193. [DOI] [PubMed] [Google Scholar]
- Farrow, C. , Blissett, J. , & Haycraft, E. (2011). Does child weight influence how mothers report their feeding practices? International Journal of Pediatric Obesity, 6(3–4), 306–313. [DOI] [PubMed] [Google Scholar]
- Greenville, J. , Pobke, C. , & Rogers, N. (2013). Trends in the distribution of income in Australia. Melbourne: Productivity Commission. [Google Scholar]
- Gregory, J. E. , Paxton, S. J. , & Brozovic, A. M. (2010). Pressure to eat and restriction are associated with child eating behaviours and maternal concern about child weight, but not child body mass index, in 2‐to 4‐year‐old children. Appetite, 54(3), 550–556. [DOI] [PubMed] [Google Scholar]
- Harrison, K. , Bost, K. K. , McBride, B. A. , Donovan, S. M. , Grigsby‐Toussaint, D. S. , Kim, J. , … Jacobsohn, G. C. (2011). Toward a developmental conceptualization of contributors to overweight and obesity in childhood: The Six‐Cs model. Child Development Perspectives, 5(1), 50–58. [Google Scholar]
- Haycraft, E. L. , & Blissett, J. M. (2008). Maternal and paternal controlling feeding practices: Reliability and relationships with BMI. Obesity, 16(7), 1552–1558. [DOI] [PubMed] [Google Scholar]
- Jansen, E. , Daniels, L. A. , & Nicholson, J. M. (2012). The dynamics of parenting and early feeding–constructs and controversies: A viewpoint. Early Child Development and Care, 182(8), 967–981. [Google Scholar]
- Jansen, E. , Mulkens, S. , & Jansen, A. (2007). Do not eat the red food!: Prohibition of snacks leads to their relatively higher consumption in children. Appetite, 49(3), 572–577. [DOI] [PubMed] [Google Scholar]
- Kiff, C. J. , Lengua, L. J. , & Zalewski, M. (2011). Nature and nurturing: Parenting in the context of child temperament. Clinical Child and Family Psychology Review, 14(3), 251–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knight, R. G. (1984). Some general population norms for the short form Beck Depression Inventory. Journal of Clinical Psychology., 40(3), 751–753. [DOI] [PubMed] [Google Scholar]
- Kochanska, G. , & Murray, K. T. (2000). Mother–child mutually responsive orientation and conscience development: From toddler to early school age. Child development, 71(2), 417–431. [DOI] [PubMed] [Google Scholar]
- Lewis, M. , & Worobey, J. (2011). Mothers and toddlers lunch together. The relation between observed and reported behavior. Appetite, 56(3), 732–736. [DOI] [PubMed] [Google Scholar]
- Lumeng, J. C. , Ozbeki, T. N. , Appugliese, D. P. , Kaciroti, N. , Corwyn, R. F. , & Bradley, R. H. (2012). Observed assertive and intrusive maternal feeding behaviors increase child adiposity. The American Journal of Clinical Nutrition, 95(3), 640–647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maccoby, E. , & Martin, J. (1983). Socialization in the context of the family: Parent‐child interaction In Hetherington E. M. (Ed.), Handbook of child psychology: Socialization, personality, and social development (Vol. 4, pp. 1–101). New York: Wiley. [Google Scholar]
- Maccoby, E. (1999). The uniqueness of the parent‐child relationship In Collins W. & Laursen B. (Eds.), Relationships as developmental contexts (pp. 157–175). Hillsdale, NJ: Lawrence Erlbaum. [Google Scholar]
- McPhie, S. , Skouteris, H. , Daniels, L. , & Jansen, E. (2014). Maternal correlates of maternal child feeding practices: a systematic review. Maternal & Child Nutrition, 10(1), 18–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell, G. L. , Farrow, C. , Haycraft, E. , & Meyer, C. (2013). Parental influences on children's eating behaviour and characteristics of successful parent‐focussed interventions. Appetite, 60, 85–94. [DOI] [PubMed] [Google Scholar]
- Musher‐Eizenman, D. R. , de Lauzon‐Guillain, B. , Holub, S. C. , Leporc, E. , & Charles, M. A. (2009). Child and parent characteristics related to parental feeding practices. A cross‐cultural examination in the US and France. Appetite, 52(1), 89–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Novick, G. (2008). Is there a bias against telephone interviews in qualitative research? Research in Nursing & Health, 31(4), 391–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogden, C. L. , Kuczmarski, R. J. , Flegal, K. M. , Mei, Z. , Guo, S. , Wei, R. , … Johnson, C. L. (2002). Centers for Disease Control and Prevention 2000 growth charts for the United States: Improvements to the 1977 National Center for Health Statistics version. Pediatrics, 109(1), 45–60. [DOI] [PubMed] [Google Scholar]
- Ogden, J. , Reynolds, R. , & Smith, A. (2006). Expanding the concept of parental control: a role for overt and covert control in children's snacking behaviour? Appetite, 47(1), 100–106. [DOI] [PubMed] [Google Scholar]
- Rodgers, R. F. , Paxton, S. J. , Massey, R. , Campbell, K. J. , Wertheim, E. H. , Skouteris, H. , & Gibbons, K. (2013). Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. International Journal of Behavioral Nutrition and Physical Activity, 10(1), 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rollins, B. Y. , Loken, E. , Savage, J. S. , & Birch, L. L. (2014). Maternal controlling feeding practices and girls' inhibitory control interact to predict changes in BMI and eating in the absence of hunger from 5 to 7 y. The American Journal of Clinical Nutrition, 99(2), 249–257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rollins, B. Y. , Savage, J. S. , Fisher, J. O. , & Birch, L. L. (2015). Alternatives to restrictive feeding practices to promote self‐regulation in childhood: A developmental perspective. Pediatric Obesity. [DOI] [PubMed]
- Shloim, N. , Edelson, L. R. , Martin, N. , & Hetherington, M. M. (2015). Parenting styles, feeding styles, feeding practices, and weight status in 4–12 year‐old children: A systematic review of the Literature. Frontiers in Psychology, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skouteris, H. , McCabe, M. , Swinburn, B. , Newgreen, V. , Sacher, P. , & Chadwick, P. (2011). Parental influence and obesity prevention in pre‐schoolers: A systematic review of interventions. Obesity Reviews, 12(5), 315–328. [DOI] [PubMed] [Google Scholar]
- Spielberger, C. D. , & Reheiser, E. C. (2009). Assessment of emotions: Anxiety, anger, depression, and curiosity. Applied Psychology: Health and Well‐Being, 1(3), 271–302. [Google Scholar]
- Tan, C. C. , & Holub, S. C. (2011). Children's self‐regulation in eating: Associations with inhibitory control and parents' feeding behavior. Journal of Pediatric Psychology, 36(3), 340–345. [DOI] [PubMed] [Google Scholar]
- Van den Berg, L. , Pieterse, K. , Malik, J. A. , Luman, M. , van Dijk, K. W. , Oosterlaan, J. , & Delemarre‐van de Waal, H. A. (2011). Association between impulsivity, reward responsiveness and body mass index in children. International Journal of Obesity, 35(10), 1301–1307. [DOI] [PubMed] [Google Scholar]