

Abstract
There is limited and inconsistent empirical evidence regarding the role of economic factors in breastfeeding practices, globally. Studies have found both negative and positive associations between low income and exclusive breastfeeding (EBF). Employment, which should improve household income, may reduce EBF due to separation of mother and infant. In the context of a randomized controlled study of lipid‐based complementary feeding in an urban slum in Cap Haitien, Haiti, we examined the economic factors influencing breastfeeding practices using mixed methods. Findings demonstrate relationships between urban context, economic factors, and breastfeeding practices. Poverty, food insecurity, time constraints, and limited social support create challenges for EBF. Maternal employment is associated with lower rates of EBF and less frequent breastfeeding. Extreme food insecurity sometimes leads to increased exclusive breastfeeding among Haitian mothers, what we call “last resort EBF.” In this case, women practice EBF because they have no alternative food source for the infant. Suggested policies and programs to address economic constraints and promote EBF in this population include maternal and child allowances, quality child care options, and small‐scale household urban food production.
Keywords: economic factors, exclusive breastfeeding, Haiti, mixed methods
1. INTRODUCTION
Exclusive breastfeeding (EBF) for the first 6 months of life, early initiation of breastfeeding, and continued breastfeeding for 2 years are internationally accepted standards for infant nutrition (United Nation Children's Fund [UNICEF], 2016b). Globally, about 37% of infants are exclusively breastfed for the recommended 6 months, and in Haiti, the figure is close to 40% (UNICEF, 2016a, 2016b; Victora et al., 2016). As a result of these low rates, many infants are vulnerable to undernutrition and disease (Black et al., 2013). These risks are more prevalent in developing countries with high poverty rates, poor water and sanitation infrastructure, and lack of access to healthcare (UNICEF, 2016b). Therefore, it is important to understand the factors contributing to low rates of EBF in order to develop effective policies and strategies to encourage it.
There is little empirical evidence on the role of economic factors in breastfeeding practices in urban Haiti. Research on infant and young child feeding in Haiti reports that women often value breastfeeding for child health, yet they encounter sociocultural and economic barriers to optimal breastfeeding (Lesorogol, Jean‐Louis, Green, & Iannotti, 2014; Dörnemann & Kelly, 2013; Laterra, Ayoya, Beauliere, Bienfait, & Pachon, 2014). Studies in Haiti and other countries reveal cultural beliefs supporting and inhibiting EBF (Agunbiado & Ogunleye, 2012; Dornemann & Kelly, 2013; Laterra et al., 2014; Njai & Dixey, 2013). Beliefs that breastfeeding is good for child growth and health are common (Agunbiade & Ogunleye, 2012; Dörnemann & Kelly, 2013; Njai & Dixey, 2013), but there is also considerable evidence, not limited to developing countries, of widespread concern among mothers about breast milk insufficiency leading to early introduction of complementary foods (Dörnemann & Kelly, 2013; Kimani‐Murage, Wekesah, Wanjohi, et al., 2015; Laterra et al., 2014; Njai & Dixey, 2013; Obermeyer & Castle, 1997). In Haiti, the notion that breast milk can be spoiled due to mothers' stress or illness has been cited as a reason to stop EBF (Farmer, 1988; Laterra et al., 2014). Social support from partners and in‐laws is another commonly cited factor influencing EBF (Agunbiade & Ogunleye, 2012; Dörnemann & Kelly, 2013; Njai & Dixey, 2013).
There is less evidence regarding the role of economic factors and poverty in breastfeeding practices. Several studies in developing countries that experience high poverty rates similar to those in Haiti have found associations between economic factors and breastfeeding practices, but the evidence is inconsistent. Lower socioeconomic status was associated with higher rates of EBF in studies in Mexico and Latin America (Escamilla, Lutter, Segall, et al., 1995; Flores, Pasquel, Maulen, & Rivera, 2005). In the Gambia, Njai and Dixey (2013) found, in contrast, that low income reduced EBF due to women's lack of access to food for themselves and emotional and physical stress. Mothers' employment has been associated with reduction in EBF in studies in Latin America and Asia (Agunbiade & Ogunleye, 2012; Escamilla et al., 1995; Flores et al., 2005; Lakati, Binns, & Stevenson, 2002; Yimyam & Morrow, 1999). A study in Thailand found that when women work long hours, they tend to experience a decrease in milk supply (Yimyam & Morrow, 1999). A study in Guatemala City found that the strongest determinant of EBF was whether or not the mother worked outside the home (Dearden, Altaye, Maza, et al., 2002).
In Haiti, maternal employment has been posited to influence breastfeeding practices. Dörnemann and Kelly (2013) reported that women listed employment as a reason for other mothers not exclusively breastfeeding their children. The study authors report that women gave this response apparently in order to avoid stigma associated with not exclusively breastfeeding. A small study in rural Leogane near Port‐au‐Prince found a negative association between maternal employment and EBF and that women tend to leave their children behind when they go to the market (Menon, Ruel, Pelto, et al., 2005; Zalla, 2015). There is little direct evidence, both qualitative and quantitative, for the effects of maternal employment on reduced EBF for an urban poor population in Haiti.
In the context of a randomized controlled study in an urban slum in Cap Haitien, Haiti, examining the effect of a lipid‐based complementary food on infant and young child nutrition, the relationship of factors related to urban poverty and EBF were explored using mixed methods. Our study examined a comprehensive set of economic factors and their potential influence on optimal breastfeeding practices. The mixed methods approach allowed us to validate findings and delve more deeply into the nuances of factors with a view towards identifying programming and policy solutions.
Key messages.
Mothers in a poor urban community in Haiti face economic challenges to exclusive breastfeeding (EBF) including low income, food insecurity, and limited social support.
Food insecurity affects EBF through two pathways—perceived breastmilk insufficiency leading to cessation of breastfeeding, or “last resort” breastfeeding when no other food sources are available to the mother.
Maternal employment is associated with lower rates of EBF due to separation of mother and infant.
Programs that support household food security and income generation have potential to address economic barriers to EBF.
2. METHODS
2.1. Study design
A randomized controlled study using mixed methods and longitudinal design was carried out from 2011 to 2012 and is described in detail elsewhere (Iannotti et al., 2013). In brief, children ages 6–11 months (n = 589) were randomly assigned to one of three groups: (a) control that did not receive lipid‐based nutrient supplement (LNS), (b) LNS supplementation for 3 months, and (c) LNS supplementation for 6 months. The child consumed one sachet of LNS (108 kcal, >80% of recommended critical micronutrients) per day. Children and their mothers made monthly follow‐up visits to Fort Saint Michel (FSM) clinic for 6 months and one additional visit 6 months after the end of the intervention. Trained enumerators collected socioeconomic, demographic, and environmental data at baseline and end line from mothers. Infant feeding practices, dietary intakes, child development, and morbidity data were elicited at each monthly visit through survey questionnaires. Anthropometric measures of height and weight were taken at monthly visits. The primary breastfeeding variables used in this study included early initiation (within 1 hr and within 1 day), EBF (no solids or liquids) for 6 months, and current breastfeeding frequency based on 24‐hr recall. Details for other variables are previously reported (Iannotti et al., 2013).
Qualitative research was conducted concurrently with the quantitative surveys, drawing on the Focused Ethnographic Study approach (Pelto, Armar‐Klemesu, Siekmann, & Schofield, 2013) to learn rapidly and specifically about infant and young child nutrition practices in this population. In‐depth interviews, focus groups, and observations were conducted between November 2011 and March 2012 during the course of the intervention by the qualitative research specialist (a cultural anthropologist) and the study coordinator who was trained in qualitative methods (see Lesorogol et al., 2014). Here, we focus on 29 in‐depth semi‐structured interviews conducted with mothers of children enrolled in the LNS programme. Interviewees were selected purposively to include participants from all three arms of the intervention and across a range of sociodemographic characteristics. Interview guides were developed in English by the research team led by the qualitative research specialist and translated into Haitian Creole by the study coordinator.
Topics covered in the interview included the use, storage, and perceived effects of LNS; breastfeeding and use of complementary foods; means of accessing food; sources of income and assistance from others; housing, water, and sanitation conditions; use of health services; perceptions of health messages; and an elicitation of general needs. Interviews were conducted in women's homes and in a few cases included the women's husbands, partners, or mothers who were present. Interviewers used an interview guide with the main topics listed and used follow‐up questions as probes to encourage participants to clarify and expand on their answers. The interviews ranged from 30 to 90 min and were digitally recorded, transcribed, and translated from Creole into English for analysis.
2.2. Study site
The study drew participants from Petite Anse, the poorest section of Cap Haitien, Haiti's second largest city. Petite Anse's population exceeds 80,000, and many residents are recent migrants to the city from rural areas. It is a low‐lying, densely populated area with poor quality housing, lacking in sanitation, water, and electricity. The leading cause of child death in the community is acute diarrhoea, likely related to poor water and sanitation, affecting around 21% of Haitians (Iannotti et al., 2013). Recruitment to the study was open to all mothers with children under 1‐year meeting eligibility criteria including infant age between 6 and 11 months; in good health; not severely malnourished (WLZ [weight for length z‐score] < −3); household not receiving other food aid; and residence within the catchment area. Although a census was not conducted, study team members made extensive outreach efforts to women in the community through public meetings and visits to different neighbourhoods and at the Fort Saint Michel (FSM) clinic. Eligible mothers were informed of the study protocol, and informed consent was obtained. In total, 709 infants were recruited and screened for eligibility. Of those, 113 were excluded due to age, 2 twin pairs were excluded, and 5 were excluded due to undernutrition status, leaving 589 pairs enrolled in the study and randomized to the three groups. There was a 29% attrition by the end of the intervention, mostly due to participants leaving the area1 (Iannotti et al., 2013). Data used for this analysis are baseline data taken from the entire sample (n = 589), thus not affected by attrition. The study was approved by the National Bioethics Committee of the Ministry of Public Health and Population in Haiti and the Institutional Review Board of the Human Resource Protection Office of Washington University, St Louis, MO.
2.3. Data analysis
Qualitative and quantitative components of the study were first analysed separately using appropriate techniques such as statistical analysis for quantitative responses and thematic analysis for qualitative interviews.2 In order to understand the relationship of economic factors to breastfeeding, the investigators compared relevant quantitative and qualitative findings. In the following discussion, both types of results are presented. Quantitative results suggest relationships between economic factors and breastfeeding practices and qualitative results provide information regarding the potential pathways or mechanisms through which the economic factors influence these practices. Thus, the effort is made to triangulate findings and deepen the analysis by using multiple methods.
Qualitative interview transcripts were analysed in Nvivo10 software and coded for themes following a grounded theory approach where themes emerge from the data rather than being identified a priori (Charmaz, 2014). Coding was led by the qualitative research specialist and a research assistant who jointly developed the major themes relating to all aspects of the study. Here, we focus on the economic themes that emerged from the interviews. A framework matrix analysis (not shown) of a subset of nine interviews across the study arms analysing five economic themes (access to food, employment status, help from others, needs, water, and sanitation conditions) did not demonstrate systematic differences in responses across study arms. Therefore, results are pooled for presentation below and variations reported reflect individual differences or overall patterns rather than differences across study arms.
Quantitative survey data, taken at baseline, on breastfeeding practices and economic factors related to income, assets, and livelihoods were analysed using descriptive statistics followed by univariate analyses using chi‐squared and t tests. Water, hygiene, and sanitation variables were included in the original trial quantitative data collection (Iannotti et al., 2013) but were not used in these analyses due to the correlation with the economic factors, the primary focus here. Findings from the univariate analyses were then used to build regression models that could more rigorously test the associations between economic variables and breastfeeding practices. Logistic regression and ordinary least squares regression modelling was applied in this phase of the quantitative analyses. Data analyses were performed with STATA software (version 13.1; StataCorp, College Station, TX).3
2.4. Conceptual framework
The conceptual framework (Figure 1) illustrates the factors found to have effects on women's decisions regarding EBF and suggests pathways from different factors to breastfeeding practices. The two primary economic factors that influence breastfeeding practices are employment status and income. Each of these factors affects household food security but in different ways. For example, women who are employed may have higher food security due to their income but tend to spend less time with infants making EBF difficult to maintain. As a result, they often do not practice EBF and instead purchase complementary foods for their infants. In contrast, women who are not employed tend to have lower income and greater household food insecurity. Low income and associated food insecurity appear to influence EBF in two ways. In some cases, women substitute breastfeeding with purchased foods, often due to perceptions of breast milk insufficiency. In other cases, women with very low income exclusively breastfeed as a kind of “last resort,” because they are unable to afford any other food for the baby. Both of these pathways were found in this study and will be presented below. The conceptual framework indicates the source of data, quantitative (Quant), and/or qualitative (Qual) for each factor.4 In the analysis presented below, the factors, their interrelationships, and effects on breastfeeding are discussed. The first two sections of Section 3 include quantitative and qualitative data on employment and income patterns and the pathways to food insecurity in Petit Anse. Section 3.3 examines the linkages between these factors and breastfeeding practices and is followed by a general discussion of the findings, programme and policy implications, limitations, and strengths and the conclusion.
Figure 1.
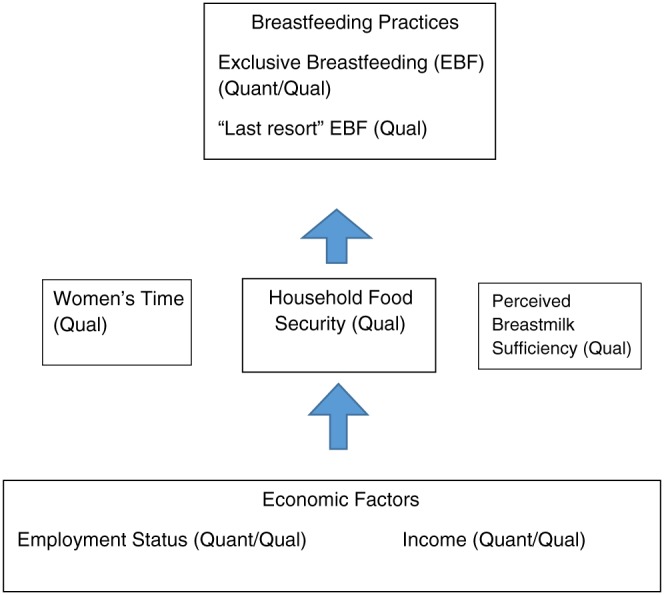
Conceptual model of factors related to breastfeeding practices in Cap Haitien, Haiti
3. RESULTS
3.1. Income and employment status of the sample
Quantitative data for the entire sample (n = 589), taken at baseline, is shown in Table 1. The economic situation of the participants measured across several wealth variables showed high levels of poverty. About one third of households had incomes less than $2 a day, and 6% had incomes less than $1 a day, both indicators of extreme poverty. About one third of the sample owned their homes, but less than half had access to electricity in the home, and other indicators of housing quality (proxies for economic status) show significant percentages with unfinished floors and metal roofs. Slightly over half of the mothers in the study reported being employed. Of mothers reporting employment, over one third worked in the market or had a small business. There were a higher proportion of fathers reporting any kind of employment compared to mothers.
Table 1.
Descriptive statistics for BF and economic factors (n = 589)
| Economic variables | |
|---|---|
| Income $ per day, mean (SD) | 3.48 (3.09) |
| Poverty (income <$2 per day) % | 30.5 |
| Abject poverty (income <$1 per day) % | 6.3 |
| Assets—home ownership, % | 37.4 |
| Electricity, % | 48.0 |
| Flooring—finished, % | 87.3 |
| Roof material | |
| Metal, % | 61.7 |
| Concrete, % | 38.3 |
| Employment—Mother | |
| Any employed, % | 51.5 |
| Market or small business, % | 35.9 |
| Employment—Father | |
| Any employment, % | 87.7 |
| BF variables | |
| Early BF initiation | |
| Within 1 hr, % | 56.6 |
| Within 1 day, % | 92.4 |
| Exclusive BF 6 months, % | 56.9 |
| BF 24 hr frequency, mean (SD) | 8.3 (3.8) |
Note.SD = standard deviation; BF = breastfeeding.
Reported breastfeeding practices showed relatively high compliance with recommendations for early initiation within 1 day but lower levels of EBF (Table 1). Approximately one in five mothers had given only breastmilk in the previous 24 hr before the survey (23.3%). Those reporting that neither solids nor liquids had been introduced before 6 months were 56.9%.
In qualitative interviews (n = 29), we learned more about income and employment among families in our sample. Mothers and fathers reported that finding employment was difficult. Most respondents worked in the informal sector and jobs were unstable and low paying. Men's informal sector jobs included working on a “taptap” (public transport vehicle), selling water, working as a mason, and delivering goods using a wheelbarrow. Examples of more stable jobs for men included teaching, construction, taxi chauffeur, working at a bank, and working on a boat.
Most of the mothers in the qualitative sample were not currently employed and were reliant on assistance from their husbands or partners. A major reason that women gave for not working was that they were staying home with their babies. Some of the mothers had worked before but stopped working to take care of their infants and young children. For example, one woman reported that she used to work but was not currently working and implied she would not return until the child was school aged:
I have sold things in the past. But now, my child hasn't started school yet, so I can't leave the house. (Interview 22, Group 2)
In another case, a woman who works in the market reported returning to work after 6 months:
I returned to the market after the baby has breastfed for 6 months. I had the patience to breastfeed for 6 months. When I returned at seven months, I started giving her nutritious foods. When I noticed they were eating everything well at 8 or 9 months, I was able to leave them and return to the market. (Interview 23, Group 1)
This woman clearly chose to stay home and breastfeed her baby, although it meant forgoing income from her former market employment. The most common work for mothers was selling goods at the market. Although many others wanted to start small businesses, they could not afford it or seek out the resources to do so. A handful of mothers had businesses but stopped operating them because of their babies or because they were not making a profit. A mother who discontinued EBF at 3 months to return to work reported that working in the market cannot fully support her family, but she still feels compelled to work:
[My business] can't support me. If you go out and earn 100 gourde, you are obligated to do this. In the time you are sitting here at home, you can go out and earn 100 gourde. It is not enough to support the children, but you have to do it. (Interview 25, Group 1)
In another case, a mother with economic difficulties who has not been able to exclusively breastfeed reports that her business was not making a profit, thus not helping support her family.
I used to sell things, but I don't anymore. It wasn't profitable. I can't afford to run the business. (Interview 06, Group 3)
In addition, her husband was not currently employed and did not receive help from others with money. The mother reported that her husband is occasionally able to help find money to support their children:
When my husband leaves, God helps him find money to help the children survive. (Interview 06, Group 3)
Although many women reported staying home with their babies, others said that they did return to work, with negative effects for EBF. One mother reported that she did not exclusively breastfeed because she needed to return to her business 15 days after giving birth.
… I didn't have time to breastfeed, I had to return to commerce and all my other responsibilities. Right after I gave birth, I did not breastfeed because I knew I had to return to my business. (Interview 19, Group 3)
She further explained how her need to return to work caused stress, which affected her breast milk production:
Yes, I had breast milk, but as soon as I returned to the market, it stopped coming. If you have “bad blood” (move san), it will stop; if you are worried, it will stop. (Interview 19, Group 3)
This participant mentions “move san,” the Haitian idea that stress can negatively affect women's breast milk quality and production, suggesting the impact of stress on breastfeeding.
Mothers were more inclined to return to work when they had help from others watching their baby. For example, those who have family living close by, especially mothers or sisters, were able to leave their children with them when they were going to be away from home:
I have a sister that lives here. She doesn't go out, so I could leave my baby with her. (Interview 14, Group 1)
Due to the recent migration from rural areas, however, many mothers and husbands do not have family nearby to help them.
This kind of help is difficult to find. For example, my parents live in the countryside but they do not have the means to help, they don't have anything. Things like charcoal or other small things, they can't help with. (Interview 04, Group 1)
Receiving social support from family was more the exception than the rule among interviewees. Furthermore, women did not report being able to bring their children to work with them. Thus, without someone to help take care of the baby, women often stopped working to stay home with their baby.
3.2. Urban residence exacerbates food insecurity
In addition to low levels of employment and associated low income, residing in an urban area had negative consequences for food security due to high reliance on the cash economy to purchase food and water and a lack of opportunities to produce food or access it from rural family members. Qualitative interviews revealed that mothers and their families rely heavily on the cash economy. Food is bought from markets in the community, but the closest markets do not always have what is needed, necessitating travelling longer distances to purchase food. When one mother, who exclusively breastfed and planned to continue breastfeeding until her baby was 22 months, was asked about access to a market in her community she responded:
There is nothing. We have to leave the community if we need anything …. There is a market in a neighbouring community on the water …. You have to cross the bridge and there is a market in Campagne. It's far. (Interview 21, Group 3)
Most women interviewed reported not producing any of their own food, with the exceptions of one family with a banana tree and another family with a small garden. Many families reported that they would like to have a garden to provide food for themselves or to sell, but say they do not have the means to start one. Although most women had family residing in the rural areas, they did not visit them due to lack of time and money. They reported that they did not receive food from their rural families. A father explained that his parents live in an area that has potential to grow crops but are unable to help his family:
My parents live in the countryside but they do not have the means to help, they don't have anything. (Interview 04, Group 1)
When a mother was asked about her parents' garden in the countryside, she reports she would use it but does not have the means to visit every year:
I can't go every year [to countryside where parents live] …. My parents have a garden, but I don't have a garden myself … I think I could [use parent's garden]. (Interview 22, Group 2)
In another case, one mother reported having a brother who lived in a rural area and occasionally helped with food:
My brother works in the country. Both our parents have died …. My brother sometimes comes with food for me, like plantains, beans, corn, and cornmeal. That's all. (Interview 23, Group 1)
In addition to purchasing all their food, women reported that there were no free community clean water sources so families were required to pay between 20 and 40 gourde (equivalent to $0.37–0.73) for a gallon of treated water. Families reported paying 5 gourde ($0.09) for a gallon of untreated water at a pump or well, whereas others responded that they have access to a free pump for untreated water. Depending on the size of the family, a gallon of water lasts from 2 to 7 days. Women reported buying chlorine tablets (aquatab) costing 5–10 gourde that they used to disinfect water they obtained from local, untreated sources. Many of the mothers reported that they are not able to afford enough water for their families. At the time of the study, many women said that it was becoming more difficult to access water, because construction on the nearby airport was destroying community water sources. Some mothers had to pay for transportation to a site to buy water and return home with it, adding time and expense to access clean water.
3.3. Relationships among employment, income, and breastfeeding
3.3.1. Quantitative data
Multivariate regressions indicate a negative association between employment, economic status, and EBF (Table 2). Mothers who were employed were 36% less likely to exclusively breastfeed. Of those, women who worked in the market or as small business women were 42% less likely to exclusively breastfeed, suggesting that something about these types of work makes EBF less likely, which is further discussed below. Mothers who were employed also reported significantly reduced breastfeeding frequency. Father's employment was also associated with less frequent breastfeeding. Additionally, those with electricity (a proxy for wealth) were 60% less likely to initiate breastfeeding within 1 day. Flooring, another proxy for wealth, was associated with lower frequency of breastfeeding. Early initiation of breastfeeding practice was also included in the models for EBF and breastfeeding frequency and found to trend to significance for predicting these outcomes, but not mediate the relationship between economic factors and EBF and breastfeeding frequency. No association was found for income, home ownership, or roofing materials with breastfeeding practices in the quantitative data.
Table 2.
Multivariate regression of economic determinants of breastfeeding practices
| Early BF initiation—1 daya | Exclusive BFa | BF frequency 24hrb | |
|---|---|---|---|
|
Electricity, % |
0.40 [0.20, 0.82] p = .01 | — | — |
| Finished flooring (concrete or ceramic), % | — | — |
−0.94 ± 0.48 p = 0.05 |
|
Employment—Mother Any employed, %
Market or small business, % |
— |
0.64 [0.43, 0.96] p = .03
0.58 [0.37, 0.90] p = .01 |
−0.96 ± 0.31 p = .002 |
|
Employment—Father Any employment, % |
— | — | −1.06 ± 0.49 p = .03 |
Logistic regression model; adjusted odds ratios (AOR) presented with 95% confidence interval and p value. Models were adjusted for maternal education and child age.
Ordinary least squares (OLS) linear regression models: Coefficient ± standard error and p value presented. Models adjusted for child age.
3.3.2. Qualitative data
Qualitative interviews suggested that as a result of unstable and low‐paying employment and lack of access to social and economic support, women reported difficulty accessing enough food and other basic needs for themselves and their children creating a situation of food insecurity. Food insecurity, in turn, influenced breastfeeding practices in different ways. Some mothers who could not afford enough food for themselves decided to discontinue breastfeeding due to weakness and perceived breast milk insufficiency. For example, one woman reported that she curtailed breastfeeding due to her own lack of adequate nutrition:
I didn't breastfeed for six months, I breastfed for three months before giving him food because I couldn't afford enough food. (Interview 12, Group 3)
In another case, a woman's husband reported that his wife did not have sufficient breast milk to feed the baby and attributed that to the family's lack of food:
I see that she has problems breastfeeding when we don't have food. It is hard for the milk to come out. (Interview 04, Group 1)
Undernutrition among mothers has negative effects on the mother and child, especially if it causes the mother to become weak and discontinue breastfeeding, increasing the risk of childhood illnesses. Although scientific evidence suggests that only severely malnourished women would suffer from an absolute insufficiency of breast milk (Black et al., 2013), perceptions of breast milk insufficiency are widespread even among women who are not undernourished (Obermeyer & Castle, 1997). In our study where many families were food insecure, mothers often perceived that they were too weak to breastfeed and thus decided to stop.
3.3.3. Last resort exclusive breastfeeding
Conversely, some mothers reported increased breastfeeding when they could not afford enough food for their children. In this case, breastfeeding was seen as the only way to continue to feed the baby in the absence of other foods (e.g., for complementary feeding).
When you're poor, you can't stop breastfeeding too early. When you're poor you don't have other food to give. We understand you have to continue feeding. When you're poor you have to continue breastfeeding. (Interview 11, Group 1)
If I had the means, I could buy milk for her and I could stop breastfeeding. But I don't have money for it. (Interview 04, Group 1)
I don't have money to stop breastfeeding. So I am obligated to continue breastfeeding until I have money. (Interview 15, Group 2)
One mother who is unemployed and does not live with her husband reports that when she is not able to find any money for food she stays at home to breastfeed as an alternative to buying food for the baby:
Sometimes, when I have a little money, I will have a little food for my baby. When I don't have money, I stay here and give him a little [breast] milk. For three or four days, I will give him milk because I don't have anything else. (Interview 24, Group 2)
In each of these cases, mothers report that they continue breastfeeding due to a lack of alternatives, even if they would have preferred to feed the baby something else, they lack the means to obtain other foods and thus rely on breastfeeding as a last resort. Thus, the qualitative findings suggest that food insecurity created by the urban setting of Petit Anse affects EBF through two pathways—perceived breast milk insufficiency leading to cessation of breastfeeding and introduction of complementary foods or last resort breastfeeding when no other food sources are available to the mother.
4. DISCUSSION
The findings from quantitative and qualitative data indicate relationships between the factors outlined in the conceptual framework (Figure 1) illustrating pathways from economic factors (employment and income) through women's time (at work or otherwise away from the infant), household food insecurity, and perceived breast milk insufficiency, to breastfeeding practices (early cessation or last resort EBF). Low levels of employment, particularly among women, the difficulty of finding childcare in order to continue working, and the norm against taking babies to work with them leave women with few good choices. Many decide to stay at home to take care of their infants. This might appear to increase the odds of EBF, but because these women forgo income they could have earned from employment, household food insecurity is likely to increase. In addition, the high reliance on the cash economy for virtually all household needs coupled with limited social and economic support further increase the vulnerability to poverty and stress in this population. Under these conditions, women are more likely to perceive breast milk insufficiency and introduce complementary foods early. In extreme cases when even purchasing complementary foods is not possible, women resort to EBF. Similar findings were reported for an urban slum in Nairobi, Kenya, where mothers were overwhelmed with domestic work and did not receive help from others. The additional stress and lack of support decreased optimal breastfeeding practices (Kimani‐Murage et al., 2015). In this study, women also reported low levels of social support and high stress, and we suspect that these factors contribute to the breastfeeding decisions discussed here. One woman quoted above was explicit about the role of stress in leading to breast milk insufficiency (move san) and others implied that the daily stress of finding money, food, and other necessities made EBF harder. Further research is needed to fully specify the mechanisms (biological or otherwise) from social support and stress to breastfeeding.
Widespread poverty, as shown in the survey data and interviews, results in household food insecurity. Women in our study reported that a lack of food often leads to feelings of weakness and perceptions of breast milk insufficiency, ultimately resulting in breastfeeding cessation and early introduction of complementary foods. Dörnemann and Kelly (2013) and Laterra et al. (2014) showed similar results in their studies where lower levels of economic status among mothers tended to correlate with decreased rates of EBF. Similarly, studies in Gambia (Njai & Dixey, 2013) and Kenya (Kimani‐Murage et al., 2015) found that low income levels were associated with the decision to discontinue breastfeeding due to the perception of breast milk insufficiency from malnutrition.
Conversely, extreme food insecurity sometimes leads to increased EBF among Haitian mothers, what we call “last resort EBF”. In this case, women practice EBF because they have no alternative food source for the infant. Similar findings exist in Mexico, Brazil, and Honduras, where less access to food, attributed to lack of income, was shown to increase rates of EBF (Escamilla et al., 1995; Flores et al., 2005). Although last resort EBF may be interpreted as supporting the international breastfeeding recommendations, the question remains whether this practice puts mother and child at risk of serious undernutrition. Our study thus finds both dynamics identified in prior studies—food insecurity leading in some cases to lowered EBF and in other cases to last resort EBF.
Those women who are employed were much less likely to practice EBF according to our quantitative data. The qualitative interviews showed that women who did resume work shortly after giving birth reported reducing breastfeeding as a result. Work compromised the possibility for EBF because women did not take their babies with them to work, but rather left them with relatives. This finding is consistent with previous research showing that mothers who work outside of the home have lower rates of EBF (Escamilla et al., 1995; Flores et al., 2005; Kimani‐Murage et al., 2015). Employment requires women to be away from infants for extended periods of time. In addition to employment, other time consuming activities such as leaving home to purchase food and water, as reported in interviews, may also compromise breastfeeding frequency and EBF.
4.1. Policy and program recommendations
The primary findings of this study are that food insecurity and time away from an infant due to employment or other tasks have negative effects on EBF. Drawing on this and other studies as well as programme experience, a number of existing policy and programme approaches to alleviate these problems are recommended for this setting. At policy level, a maternal and child allowance or cash transfer would enable women to purchase enough food for themselves, at least for the first 6 months of the child's life. This would allow women to stay home with infants without sacrificing food security. Considering the importance of market work to women and the difficulty of bringing young children to the market, it would be worth investigating measures to provide quality childcare for young children. Childcare facilities located in urban neighbourhoods would also employ women as caregivers. Another strategy would be to support “market substitutes,” someone to help out with a woman's market duties while she is breastfeeding. Improving household food security and nutrition through kitchen gardens, small livestock, or similar small‐scale food production appropriate to this urban environment would be beneficial. Women and men in our study expressed interest in having gardens and with some assistance could supplement their diet with nutritious foods.
4.2. Study strengths and limitations
Limitations of the current study include the cross‐sectional nature of the quantitative results that limit ability to make causal claims about the relationships of economic factors to EBF. Analysis was confined to the variables included in the household survey that was designed for the purpose of the larger study rather than focused on economic factors related to EBF. The qualitative findings are limited due to the one‐off nature of the interviews. More prolonged engagement would reveal deeper insights regarding the mechanisms of the posited relationships. As well, the quantitative variables may have been more extensive to further validate relationships. Income was measured using only reported income, likely to have some bias. However, we used multiple other markers of wealth and were primarily interested in the direction rather than strength, of relationships, which may be represented in these variables. The study does provide an in‐depth consideration of several features of poverty in an urban slum in Haiti, and the mixed method approach enables greater understanding of the relationships among contextual and economic factors and breastfeeding practices.
5. CONCLUSION
Poor women and their families in the Petite Anse area of Cap Haitien, Haiti, face serious challenges due to poverty. When a woman has a baby, she often faces a stark choice between staying home with the baby in order to exclusively breastfeed but forgoing income from employment or leaving the baby at home while she works and forgoing EBF. In either case, household income may be so low that food insecurity persists, triggering perceptions of breast milk insufficiency leading to abandonment of EBF, or continuation of last resort EBF that might put mother and child at risk of undernutrition. This study used mixed methods to show the relationships among urban context, poverty factors and breastfeeding practices. Food insecurity, women's time, and employment all have negative implications for EBF. Policies and programmes that address these constraints may increase EBF with positive implications for maternal and child health.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
CL designed qualitative study and led analysis of qualitative findings and manuscript writing. CB assisted with qualitative analysis and manuscript writing. SD assisted with qualitative study including conducting interviews. LI led the overall study, designed and analyzed quantitative data, and assisted with manuscript writing.
ACKNOWLEDGMENTS
The authors gratefully acknowledge funding from the Alive and Thrive Small Grants Program; University of California, Davis; The Inter‐American Development Bank; The World Bank; and The United Nations World Food Programme.
Lesorogol C, Bond C, Dulience SJL, Iannotti L. Economic determinants of breastfeeding in Haiti: The effects of poverty, food insecurity, and employment on exclusive breastfeeding in an urban population. Matern Child Nutr. 2018;14:e12524 10.1111/mcn.12524
ENDNOTES
Analyses showed minimal differences between participants that left the study and those who completed it (see Iannotti et al., 2013).
Quantitative and qualitative components of the study were conducted simultaneously. Because much of the qualitative study was exploratory, it was not possible to anticipate all of the findings from the qualitative interviews. Once analysis of qualitative and quantitative data was underway, the importance of economic factors emerged, leading to the current effort at an integrated discussion of results.
Not all quantitative results are shown here due to space limitations. Relevant descriptive statistics and the final regression models are included.
The quantitative survey did not include questions about all the factors that were revealed to be important in the course of the qualitative research and therefore are not included in the regression model.
REFERENCES
- Agunbiade, O. , & Ogunleye, O. (2012). Constraints to exclusive breastfeeding practice among breastfeeding mothers in Southwest Nigeria: Implications for scaling up. International Breastfeeding Journal, 7(5), 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black, R. E. , Victora, C. G. , Walker, S. P. , Bhutta, Z. A. , Christian, P. , de Onis, M. , … Martorell, R. (2013). Maternal and child undernutrition and overweight in low‐income and middleincome countries. Lancet, 382, 427–451. [DOI] [PubMed] [Google Scholar]
- Charmaz, K. (2014). Constructing grounded theory (2nd ed.). Thousand Oaks, CA: Sage. [Google Scholar]
- Dearden, K. , Altaye, M. , Maza, I. , De Oliva, M. , Stone‐Jimenez, M. , Morrow, A. L. , & Burkhalter, B. R. (2002). Determinants of optimal breast‐feeding in peri‐urban Guatemala City, Guatemala. Revista Panamericana de Salud Pública, 12(3), 185–192. [DOI] [PubMed] [Google Scholar]
- Dörnemann, J. , & Kelly, A. H. (2013). ‘It is me who eats, to nourish him’: A mixed‐method study of breastfeeding in post‐earthquake Haiti. Maternal & Child Nutrition, 9(1), 74–89. 10.1111/j.1740-8709.2012.00428.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Escamilla, R. , Lutter, C. , Segall, A. , Rivera, A. , Treviño‐Siller, S. , & Sanghvi, T. (1995). Exclusive breast‐feeding duration is associated with attitudinal, socioeconomic, and biocultural determinants in three Latin American countries. American Institute of Nutrition, 2972–2984. [DOI] [PubMed] [Google Scholar]
- Farmer, P. (1988). Bad blood, spoiled milk: Bodily fluids as moral barometers in rural Haiti. American Ethnologist, 15(1), 62–83. [Google Scholar]
- Flores, M. , Pasquel, M. , Maulen, M. , & Rivera, J. (2005). Exclusive breastfeeding in 3 rural localities in Mexico. Journal of Human Lactation, 21, 276–283. [DOI] [PubMed] [Google Scholar]
- Iannotti, L. , Jean Louis Dulience, S. , Green, J. , Joseph, S. , Francois, J. , Antenor, M. L. , … Nickerson, N. (2013). Linear growth increased in young children in an urban slum in haiti: A randomized controlled trial of a lipid‐based nutrient supplement. American Journal of Clinical Nutrition. 10.3945/ajcn.113.063883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimani‐Murage, E. , Wekesah, F. , Wanjohi, M. , Kyobutungi, C. , Ezeh, A. C. , Musoke, R. N. , … Griffiths, P. (2015). Factors affecting actualization of the WHO breastfeeding recommendations in urban poor settings in Kenya. Maternal & Child Nutrition, 11(3), 314–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lakati, A. , Binns, C. , & Stevenson, M. (2002). The effect of work status on exclusive breastfeeding in Nairobi. Asia‐Pacific Journal of Public Health, 14(2), 85–90. [DOI] [PubMed] [Google Scholar]
- Laterra, A. , Ayoya, M. , Beauliere, J. , Bienfait, M. , & Pachon, H. (2014). Infant and young child feeding in four departments in Haiti: Mixed‐method study on prevalence of recommended practices and related attitudes, beliefs, and other determinants. Revista Panamericana de Salud Pública, 36(5), 306–313. [PubMed] [Google Scholar]
- Lesorogol, C. , Jean‐Louis, S. , Green, J. , & Iannotti, L. (2014). Preventative lipid‐based nutrient supplements (LNS) and young child feeding practices: Findings from qualitative research in Haiti. Maternal and Child Nutrition. 10.1111/mcn.12122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menon, P. , Ruel, M. , Pelto, G. , François, Y. , Metellus, E. , & Ferrus, A. (2005). A qualitative study of the patterns of infant feeding and care in the Hinche area of Plateau Central, Haiti. The Food and Nutrition Technical Assistance (FANTA) Project 2005; [Google Scholar]
- Njai, M. , & Dixey, R. (2013). A study investigating infant and young child feeding practices in Foni Kansala district, western region, Gambia. Journal of Clinical Medicine, 5(6), 71–79. [Google Scholar]
- Obermeyer, C. , & Castle, S. (1997). Back to nature: Historical and cross‐cultural perspectives on barriers to optimal breastfeeding. Medical Anthropology, 17, 39–63. [DOI] [PubMed] [Google Scholar]
- Pelto, G. , Armar‐Klemesu, M. , Siekmann, J. , & Schofield, D. (2013). The focused ethnographic study ‘assessing the behavioral and local market environment for improving the diets of infants and young children 6 to 23 month old’ and its use in three countries. Maternal & Child Nutrition, 9(1), 35–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UNICEF . (2016a). Infant and young child feeding global database. https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/
- UNICEF . (2016b). From the first hour of life: Making the case for improved infant and young child feeding everywhere. New York: UNICEF. [Google Scholar]
- Victora, C. G. , Bahl, R. , Barros, A. J. , França, G. V. , Horton, S. , Krasevec, J. , … Group, T. L. B. S. (2016). Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. The Lancet, 387(10017), 475–490. [DOI] [PubMed] [Google Scholar]
- Yimyam, S. , & Morrow, M. (1999). Breastfeeding practices among employed Thai women in Chiang Mai. Journal of Human Lactation, 15(3), 225–232. [DOI] [PubMed] [Google Scholar]
- Zalla, L. (2015). The prevalence and social determinants of exclusive breastfeeding and implications for infant growth in rural Haiti: A mixed‐methods study(Masters of Public Health Thesis). Retrieved from Duke Global Health Institute at Duke University. [Google Scholar]