

Abstract
Small‐quantity, lipid‐based nutrient supplements (SQ‐LNS) show promise to improve the quality of maternal and child diets, particularly during the first 1000 days of life. The potential of SQ‐LNS to impact positively upon nutritional status relies on numerous factors, including complementary dietary intake, disease prevalence and dynamics of household utilization, including sharing practices. Therefore, this study sought to elucidate the patterns and determinants of SQ‐LNS utilization among children 6–23 months and potential sharing practices of other household members prior to intervention development. In Ntchisi, Malawi and Cabo Delgado, Mozambique, both rural, agricultural settings, we conducted two home‐feeding trials of 8 and 6 weeks, respectively, nested within a larger multi‐phase, emergent formative research design. Multiple methods, including in‐depth interviews (n = 38), direct meal observations (n = 80), full‐day child observations (n = 38) and spot checks of SQ‐LNS supply (n = 23), were conducted with households (n = 35 in Malawi; n = 24 in Mozambique). Overall, the SQ‐LNS was utilized contrary to its recommended use, with 50% of households in Malawi reporting running out of stock too early and 87% of households in Mozambique either overusing or underusing the product. Utilization of SQ‐LNS was manifested in four patterns of overuse and two of underuse and was determined by factors at multiple levels of influence. Maternal and child health efforts need to consider the reasons behind choices by households to overuse or underuse SQ‐LNS and design intervention strategies to increase the likelihood of its appropriate utilization.
Keywords: formative research, small‐quantity lipid‐based nutrient supplements (SQ‐LNS), qualitative research, intra‐household sharing practices, infant and young child feeding (IYCF) practices
Introduction
Maternal and child undernutrition is a formidable challenge that affects approximately half of the world's population (Ahmed et al. 2012). As recently as 2011, 165 million children under 5 years (U5) were affected by chronic malnutrition. Micronutrient deficiencies, which underlie many conditions associated with chronic malnutrition, contributed to increased morbidity, mortality and sub‐optimal growth and development (Black et al. 2013). As part of global efforts to address this high burden, the international nutrition community, including both government and non‐government actors, has embraced 13 nutrition‐specific interventions, which if scaled up, are likely to have a substantial and positive impact upon maternal and child nutrition (MCN) (Scaling Up Nutrition, 2014). One of the 13 nutrition interventions that may offer the biggest predicted effect on mortality is the promotion of infant and young child feeding (IYCF) practices (Bhutta et al. 2013; Maternal & Child Study Group 2013).
Promoting healthful IYCF practices in food insecure environments, however, may not be feasible because of lack of household access to promoted foods (Vitta & Dewey 2012). Home fortification – where a specialized nutritious food, such as a micronutrient powder (MNP) or a small‐quantity, lipid‐based nutrient supplement (SQ‐LNS), is added to a complementary food by a caregiver – is a potential component of a larger integrated approach to help improve the diets of infants and young children. As a preventative approach, SQ‐LNS has positively impacted the nutritional status of children under 2 years (U2) (Adu‐Afarwuah et al. 2007; Phuka et al. 2008; Dewey et al. 2009; Siega‐Riz et al. 2014; Hess et al. 2015).
When an SQ‐LNS is added to a complementary food, it increases energy density as well as the micronutrient content of the food (Dewey et al. 2009). Compared with other specialized nutritious foods available to address micronutrient deficiencies, SQ‐LNS offers unique advantages by providing a combination of micronutrients, essential fatty acids and protein in typically just 20‐g servings, making it a cost‐effective option for home fortification of locally available complementary foods without displacing breastmilk (Arimond et al. 2013; Dewey & Arimond 2012; Kumwenda et al. 2014). Further, by providing energy (~110 kcal/day) primarily in the form of lipids and often derived from a peanut base, SQ‐LNS has a sweetened flavour, as well as a semi‐solid consistency that allows caregivers the option to fortify it either into complementary foods or feed it to children directly from the sachet (Arimond et al. 2013). Utilizing SQ‐LNS, however, puts the onus on the caregiver to fortify complementary foods in the household on a consistent basis. As a result, sustained behaviour change of the caregiver (i.e. correctly providing the recommended SQ‐LNS dosage to the intended beneficiary) is a necessary component of a home fortification intervention. While numerous studies in sub‐Saharan Africa have found SQ‐LNS flavour acceptability to be a facilitating factor in behaviour change (Flax et al. 2009; Adu‐Afarwuah et al. 2011; Hess et al. 2011; Parker et al. 2011; Phuka et al. 2011; Tripp et al. 2011; Cohuet et al. 2012; Ickes et al. 2012; Paul et al. 2012; Kodish et al. 2015a), only a limited number has tried to understand other behavioural factors that may facilitate or limit the appropriate household utilization of such a product.
Intra‐household dynamics encompass many phenomena such as cash income control and decision‐making patterns. They also include food sharing practices, which differ by cultural context (Dettwyler 1989), with both positive and negative effects on young children. Researchers have reported that household dynamics are related to food allocation, caring practices and dietary habits (Shankar et al. 1998). Further, some research reports relationships between these behaviours and nutritional outcomes (Gittlesohn et al. 1998). Because family food sharing is commonplace in settings where a large majority of nutrition interventions are being implemented, including sub‐Saharan Africa (Kigutha 1997; Kitanichi 2000), the dynamics of household food utilization need to be understood in order to identify their potential influence on children's nutritional status. Scholars argue that understanding the existing patterns of household food allocation is a necessary prerequisite for determining the effectiveness of specialized nutritious food programmes (Haddad & Kanbur 1992).
Despite the potential for household food sharing practices to limit the nutritional impact of an SQ‐LNS intervention, few in‐depth studies have explored household SQ‐LNS utilization. As part of larger formative research efforts to inform integrated nutrition programmes in Malawi and Mozambique, this study sought to understand SQ‐LNS utilization at household and community levels by answering the following research questions:
To what extent were households using the SQ‐LNS as recommended (one sachet/child aged 6–23 months/day)?
What are the primary patterns of SQ‐LNS utilization by setting?
What are the factors determining patterns of SQ‐LNS utilization?
Because a similar methodological approach was used in each setting, we can draw useful comparisons related to SQ‐LNS utilization from two different cultural contexts.
Key messages.
An SQ‐LNS was not strictly used as recommended in either Malawi or Mozambique during two home‐feeding trials that were part of formative research.
The findings illustrating high rates of non‐compliance with SQ‐LNS instructions contradict much of the literature, which suggests minimal to no sharing of such products.
Understanding intra‐household and inter‐household dynamics in the context of programmes with specialized nutritious foods may help to develop more effective nutrition interventions.
Materials and methods
Study background
As part of global efforts to improve the nutritional status and quality of life of vulnerable populations, the World Food Programme is concurrently supporting the governments of Malawi and Mozambique in two integrated nutrition interventions, which are part of the Scaling Up Nutrition movement. These interventions seek to improve the health and nutritional status of pregnant and lactating women and children 6–23 months. Researchers from the Johns Hopkins Bloomberg School of Public Health conducted formative research for these programmes, and this paper describes findings from that work.
Study settings
Data were collected in two rural field sites from February to May (rainy, lean season) 2013 in Ntchisi District, Malawi and from May to August (dry, post‐harvest season) 2013 in seven districts of Cabo Delgado Province, Mozambique. Populations in both settings have predominantly agricultural livelihoods.
Ntchisi is a culturally homogenous district in the Central Region of Malawi and is home to approximately 250 000 people of Chewa ethnicity. This region has a higher burden of undernutrition than that of the nation with 47.2% stunting, 13.5% underweight and 4.3% wasting among children U5 years (DHS 2010).
Cabo Delgado is the northernmost province of Mozambique with a composite of different cultural groups, including 312 Macua, 32 Mwani and 13 Maconde villages in the intervention area (Kodish et al. [2015b] Formative research to inform a government of Mozambique nutrition intervention in Cabo Delgado province, unpublished observations). Among children U5 years, this province has the highest stunting prevalence (52.7%) in the country and an underweight prevalence (20.6%) that remains higher than that of the nation (14.9%) (DHS 2011).
General formative research design
This formative research design was emergent with an iterative, three‐phase data collection process that drew from a Rapid Assessment Procedures (RAP) approach (Scrimshaw & Hurtado 1987; Gittelsohn et al. 1998; Gittelsohn & Kodish [2011] Rapid Assessment Procedures [RAP] to develop and evaluate specialized food commodity programs: applying qualitative research skills v3.5, unpublished observations). The overarching formative research design, breadth of methods used and scope of data collected are described in detail elsewhere (Kodish et al. 2015a,b).
Research design to understand household LNS utilization
In each setting, a home‐feeding trial with SQ‐LNS was part of formative research. Trial designs varied slightly based on time availability, budgetary parameters and methodological changes made from one setting to the other based on findings from Malawi where the first trial occurred. For example, the trial period was 2 weeks shorter in Mozambique, but a new method was added to better understand SQ‐LNS utilization. In Malawi and Mozambique, the trials lasted 8 and 6 weeks, respectively, and multiple methods were used to understand household LNS utilization.
At the onset of the home‐feeding trials, the research team members supplied households with a full supply of SQ‐LNS to last the trial duration (56 sachets in Malawi and 42 sachets in Mozambique). Caregivers were given the product for consumption by their children aged 6–23 months. At distribution, they were also provided basic oral instructions on appropriate SQ‐LNS use, including information about dose (e.g. one sachet/child/day), ways to fortify local foods (e.g. mix it into porridge after the cooking process) and instructions not to share the product with non‐beneficiaries. The trials were not accompanied by other behaviour change communications.
To understand utilization, in‐depth interviews were conducted with a sub‐set of participating caregivers during the trials. Repeated direct meal observations and full‐day child observations were carried out among another sub‐set of households. Finally, in Mozambique but not Malawi, unannounced spot checks of SQ‐LNS availability at random times were conducted to compare the number of sachets in any one household to the number of sachets that should have remained available based on recommended use of the product.
Overall sampling strategy
We used a two‐tiered sampling strategy to recruit participants, by firstly identifying specific villages. In Malawi, the district nutritionist helped identify villages in each traditional authority (geographic area within a district) that would provide a geographically representative sample from Ntchisi District. In Mozambique, the government nutrition staff working with our data collection team identified villages that would provide a culturally representative sample of households. We then gained permission from community leaders to work in those areas.
The community leaders, working with the community health workers, then secondly identified households that had caregivers with children aged 6–23 months to participate in the home‐feeding trials. We recruited individuals using both criterion‐based and stratified purposeful sampling (Miles & Huberman 1994). Participants of differing geographic locations, cultural groups, genders, age groups and number of children were included (Sandelowski 2000; Patton 2002).
Data collection team
Data collectors underwent approximately 40 h of qualitative research theory and methods training prior to fieldwork. In Malawi, all five team members held university degrees and were bilingual in Chichewa and English. The seven Mozambique team members held a mixture of secondary school and university degrees. They were native Portuguese speakers who also spoke either Macua or Kimwani languages fluently.
Data collection
Home‐feeding trials with SQ‐LNS
The SQ‐LNS was distributed to 35 households [five households in each of the seven traditional authorities (geographic areas)] as part of an 8‐week, home‐feeding trial in Malawi and 24 households for a 6‐week trial in Mozambique. An equal number of children (n = 8) in each age stratum (6–12 months; 12–18 months; 18–23 months.) from two cultural groups (n = 12 Macua; n = 12 Mwani) was enrolled in Mozambique.
Table 1 outlines the methods and samples sizes of data collection within the trials by country setting.
Table 1.
Overview of data collection methods used to understand small‐quantity, lipid‐based nutrient supplement utilization
| Data collection methods | Description of application in this study | Malawi households (n = 35) | Mozambique households (n = 24)† |
|---|---|---|---|
| In‐depth interviews | Semi‐structured interviews with caregivers who participated in the home‐feeding trial with LNS | n = 13 | n = 18 |
| Direct observations | Midday and evening household meal observations using an observation guide to record events of food preparation, household feeding practices, food allocation and LNS utilization | n = 55‡ | n = 23 |
| Structured spot checks§ | Structured observations to compare the number of LNS sachets in the household to the number of sachets that should have remained available based on the product distribution cycle | — | n = 23 |
| Full‐day child observations | Direct observations during which a child 6–23 months are monitored throughout the entire day to record his/her eating behaviours | n = 21¶ | n = 24¶ |
Half of this sample (n = 12) was Macua and half was Mwani (n = 12).
The same 19 households were each observed on three different days; two observations were missed because of impassable road conditions.
Specific to Mozambique study arm.
The same 7 and 12 children in Malawi and Mozambique, respectively, were each observed on three different days.
Continuous monitoring observations
Full‐day, continuous monitoring observations (8 am–sundown) of children 6–23 months (n = 7) were conducted at three different time points over 12 weeks in Malawi. These same type of observations (n = 12) were conducted at two different time points over 8 weeks in Mozambique.
Direct meal observations
Direct observations of household midday and evening meals (n = 19) were conducted on three different days in Malawi. In Mozambique, one episode of direct meal observations (n = 23) was conducted.
Both continuous monitoring and direct meal observations were event‐sampled and time‐sampled. For event sampling, observers recorded every event of a behaviour related to the research questions. Observers gave priority to behaviours of children 6–23 months, but those of other household members were also recorded, especially when the SQ‐LNS was involved. For time sampling, recording of behaviours that remained constant (e.g. boiling water) over time were conducted a minimum of once per 5 min. Observations were largely performed in the household but also extended to the larger community when children 6–23 months would play with other children or go somewhere with their caregiver (e.g. harvesting crops).
Observation forms were used for recordings. Both qualitative (descriptive data related to types of food shared, requests for food from others and food sharing practices) and quantitative (frequencies of giving or receiving food and general food quantities) information were recorded on the forms. Specifically, each recording included the time and duration of the behaviour, the actors involved in the behaviour, the description of the behaviour, the name of the food/drink involved and the food/drink quantity.
In‐depth interviews
Interviews were conducted with male and female caregivers whose households had taken part in the home‐feeding trial. Interviewers used semi‐structured interview guides to cover the following topical areas: (1) young child food challenges; (2) caregiver experiences using SQ‐LNS during the feeding trial; (3) barriers and facilitating factors to appropriate SQ‐LNS usage; (4) issues of product acceptability; (5) reported sharing practices and associated coping mechanisms; and (6) suggestions for promoting SQ‐LNS, including recommended messages. All interviews were digitally recorded in local languages, and descriptive field notes were taken after each interview (Bernard 2006). Final sample sizes were determined based on the amount of data needed to reach data saturation – the point at which additional data collection no longer generated new understanding (Glaser & Strauss 1967; Morgan 1997).
Spot checks
Households (n = 23; one household did not agree to the spot check) in Mozambique underwent one unannounced spot check, a form of direct observation of SQ‐LNS availability at a randomly chosen time during the trial (Paolisso & Regmi 1992) for comparison against the amount of SQ‐LNS that should have been still available considering the distribution cycle of the product.
Data analysis
Direct observation data
Descriptions of behaviours and observation field notes were aggregated in local languages and translated into English. These data were then analysed by the research team using Atlas.ti v7.0 computer software (Scientific Software Development, Berlin) in order to first explore emergent themes in relation to patterns of SQ‐LNS utilization, taking an inductive approach to the textual analysis (Glaser & Strauss 1967; Strauss & Corbin 1990). Then, once salient themes of SQ‐LNS utilization were identified, we sought to understand them in relation to one another by making comparisons based on frequency of occurrence, cultural context, phase of research and household characteristics. Memos were taken throughout this process in order to make connections between emergent themes and crystallize meanings in the data (Charmaz 2006). Findings were then incorporated into semi‐structured interview guides for triangulation of results during interviews with caregivers.
In‐depth interview data
The research team translated and transcribed data from the digital recordings verbatim, maintaining key terms and phrases in the local language (Morris et al. 1999). In Mozambique, a randomly chosen sub‐set (25%) of the total sample was also back‐translated from English into Portuguese and into local languages, and checked for accuracy.
Atlas.ti v7.0 (Scientific Software Development, Berlin) was used for coding and analysis of the transcripts. The data were coded throughout each week of the study shortly after transcriptions become available using a codebook. Within Atlas.ti v7.0, the textual data were inductively analysed drawing from aspects of Grounded Theory (Charmaz 2006). The process began with line‐by‐line coding until strong analytic directions were identified. The codes are labels for assigning units of meaning to the data compiled during the study and which were then used to retrieve and organize data related to specific research questions (Miles & Huberman 1994).
Focused coding was then applied to the data set to synthesize and reference larger segments of text. Constant comparisons were made throughout the coding process in order to make comparisons at each level of analytic work (Glaser & Strauss 1967). Throughout the coding process, the investigator composed analytic notes to draw comparisons between and among codes, categories and quotations from text (Charmaz 2006).
Spot check data
Spot check data were tallied, and simple frequencies were created based on SQ‐LNS supply in comparison to schedules outlining the distribution cycle. Comparisons were made between groups of households based on geographic location, cultural group and age group of household child.
Ethical approvals
The study protocols were approved by the Malawi National Health Sciences Research Committee and the National Bioethics Committee for Health in the Mozambique Ministry of Health, as well as the Johns Hopkins Bloomberg School of Public Health Institutional Review Board. Adult participants gave informed oral consent and provided assent for their children.
Results
Household utilization of the SQ‐LNS
Mozambique
Of the 23 households that consented to a random spot check of SQ‐LNS stock, 17 of them were in short supply (too few sachets remaining considering the number of days left in the distribution cycle) (73.9%), three had excess supply (too many sachets remaining considering the number of days left in the distribution cycle) (13.0%) and three had an adequate supply (the same number of sachets remaining as the number of days left in the distribution cycle) (13.0%). No noticeable differences in supply levels existed by cultural group or age range of the beneficiary child (Table 2). Further, supply levels were not affected by geographic area (coastal vs. inland) of the household (Table 3). From the first to third weeks of the spot checks, the percentage of households that ran out of SQ‐LNS stock increased from 44.4% to 57.1%.
Table 2.
Data from spots checks (n = 23 households) of small‐quantity, lipid‐based nutrient supplement supply in Mozambique during the home‐feeding trial by cultural group and household child age group
| Cultural group | Household child age group | Total households (n = 23) | ||
|---|---|---|---|---|
| 6–12 months | 12–18 months | 18–23 months | ||
| Mwani (n = 12) | 1/4 (25%) | 0/4 (0%) | 1/4 (25%) | 2/12 (16.7%) |
| Macua (n = 11) | 1/4 (25%) | 0/3 (0%) | 0/4 (0%) | 1/11 (0.09%) |
| Total households (n = 23) | 2/8 (25%) | 0/7 (0%) | 1/8 (12.5%) | 3/23 (13.0%) |
Fractions indicate the number of households with the correct number of small‐quantity, lipid‐based nutrient supplement sachets based on the distribution cycle divided by the total number of households.
Table 3.
Comparison of small‐quantity, lipid‐based nutrient supplement supply level between Mwani and Macua households of Mozambique
| Supply level† | Mwani | Macua | Total |
|---|---|---|---|
| Under supply | 10 | 7 | 17 |
| Over supply | 2 | 1 | 3 |
| Adequate supply | 2 | 1 | 3 |
Undersupply indicates a short supply of small‐quantity, lipid‐based nutrient supplement (SQ‐LNS) sachets in household; oversupply indicates an excess supply of SQ‐LNS sachets in household; and adequate supply indicates the correct number of sachets remaining in household compared with the number that should be remaining based on the distribution cycle.
The research team conducted full‐day observations in a total of 12 households during the first round of data collection. Caregivers in only 3 of the 12 (25.0%) households provided the SQ‐LNS as recommended to beneficiary children. In 6 of the 12 (50.0%) observations, no SQ‐LNS was provided throughout the day. Of the six events of provision of SQ‐LNS, three included the caregiver or another child also eating at least some of it (50.0%). During the second round of full‐day child observations, 4 out of 12 households (33.0%) used the product as recommended. In 7 of the 12 households (58.3%), observers did not observe the provision of the SQ‐LNS from 8 am until sundown. And 1 of the 12 (8.3%) observations did reveal utilization of the product in the household, but sharing of it occurred among other children.
Data from in‐depth interviews and field notes from direct observations reveal that caregivers did not provide the SQ‐LNS in most cases during the full‐day observations because they ran out of supply too early.
‘I did not see the child eat LNS in this household and according to the next round of distribution there should be 4 sachets left. The caregiver explained that the product ran out early because she gave more than one product to the child at times, such as when the child cried, or even on some days the parents ate some of it. There was also a case of the product being taken from the household. It was taken by the older sister’.
‐Data collector, field notes from direct observation
This finding is corroborated by the spot check data outlined in Table 2 that describe 73% of households without adequate supply of the product during the second half of the home trial.
Malawi
When asked whether 28 sachets was a sufficient supply for 28 days, 50% of the respondents responded affirmatively. One caregiver explained, ‘…the sachets weren't enough for 28 days, for only 20 days…’ describing her own situation; another person admitted, ‘there were not enough because I gave two sachets to my cousin’. Another caregiver was reluctant to talk about her own household and instead pointed to the short supply another household was facing.
‘OK, right now the other household who was given LNS says that it already finished and the owners are saying that they gave it to other children at some point but they also say that the beneficiary child sometimes took it without permission’.
‐Male caregiver of child 12 months, In‐depth interview in Malawi
Even for those caregivers who reported an adequate supply of the product, maintaining the recommended use of the product was not easy, as one caregiver explained, ‘They lasted 28 days as well…but to tell you the truth for them to reach 28 days it was hard…’ Data collectors observed more episodes of SQ‐LNS sharing over time from phase 1 to phase 3. Myriad interrelated factors determined the ease or difficulty of appropriate SQ‐LNS usage in Malawi (Table 4), including seasonal influences on household food security.
Table 4.
Factors influencing small‐quantity, lipid‐based nutrient supplement (SQ‐LNS) usage by household characteristics and dynamics in Malawi
| Factor | Explanation of influence on SQ‐LNS usage during home‐feeding trial |
|---|---|
| Perception of SQ‐LNS | Interview data indicate that community members perceived the SQ‐LNS in the same food grouping as other cereal‐based staple foods commonly shared in this setting. It was considered to be an ‘energy‐giving food’, similar in classification to nsima, which is a commonly shared, maize‐based staple food in Ntchisi. |
| Caregiver feeding style of child 6–23 months | Caregivers who more responsively fed their children aged 6–23 months were observed to share less often than those caregivers using a laissez‐faire style, with little attention to protect the beneficiary child from older children's attempts to share during feeding episodes. |
| Ease of product storage for caregivers | Households with storage challenges (e.g. lack of locked storage space) reported more difficulty keeping SQ‐LNS away from older children, particularly when caregivers had to travel away from the household for agricultural activities during the day. |
| Appetite of beneficiary child 6–23 months | Children aged 6–23 months, whose caregivers reported having good appetites to finish their entire meal portions, did not often leave leftovers of SQ‐LNS or the fortified vehicle food to be consumed by other household members. |
| Number of children in a household | Observation data, including data collector field notes, suggest that caregivers of households with a greater number of children faced more pressure to share than those households with just one child. |
| Varying levels of social support | Social support was an important facilitating factor. Other household members, especially husbands and adolescents, provided reminders and gave encouragement to caregivers to use SQ‐LNS. They also helped with feeding. Health workers reportedly provided follow‐up directions and answered questions/concerns about SQ‐LNS usage, as well as gave additional motivation to caregivers while making routine household health visits. |
Household food shortages during the lean season are not uncommon in Malawi. Such a circumstance was an underlying cause of SQ‐LNS sharing, as one caregiver explained, ‘During the rainy season, a lot of people will share food with others because it is the time that food is scarce’. Food sharing varies by type and frequency during different times of the year and caregivers expect that SQ‐LNS sharing will do so as well. This finding is supported by self‐reported food sharing practices in relation to seasonal food shortages.
Common patterns of SQ‐LNS utilization
Product overuse
There were six primary ways that households used the SQ‐LNS contrary to its intended use. Four thematic areas emerged related to overuse and two associated with underuse. Overall, SQ‐LNS overuse was substantially more frequent than underuse.
Caregiver consumption of product
Most caregivers were observed tasting or consuming the product during feeding episodes. It was perceived to be both a novelty and very tasty. Consumption was performed directly from the sachets during feeding or when children would not finish their food and leftovers remained. Caregivers report that having leftovers is a common occurrence because preparing just the right amount of food for a child 6–23 months is difficult.
‘Sharing was happening, I cannot lie. Sometimes when I cook porridge for the child and I give it (SQ‐LNS) to the child, the child won't finish the porridge and I would finish it…so that's how sharing was happening. Sometimes when giving her it (SQ‐LNS) directly she would leave some in the packet and I would finish it for her’.
Female caregiver of child 11 months, Interview in Malawi
In other situations, however, caregivers explain that they keep leftovers to provide to the child, either later that day or the following day. They discuss the importance of hygiene when they have to store the leftover food for later and suggested that SQ‐LNS sachets should be re‐sealable for future use. This practice was also linked to the season in which the product was being introduced, as the same caregiver explained.
‘What happens is that when we prepare porridge for the child and we put the product in the porridge, after the child has eaten, if I (the parent) is also hungry, then I will also eat some of the porridge, so this is how sharing will occur in the lean season’.
Female caregiver of child 11 months, Interview in Malawi
Field notes from observations in Mozambique reveal conversations with mothers that underscore caregiver consumption as a salient barrier to appropriate SQ‐LNS utilization.
‘With regard to the provision of the SQ‐LNS in this household, there is not one sachet left…the provision of it ran out early, which suggests that the product was shared excessively…according to household members during discussion in the field…each member of the home removed for themselves a packet of the product each morning’.
Data Collector, Observation field notes in Mozambique
Data collection did not reveal any caregiver or household strategies to mitigate this form of product sharing, but did so for other sharing patterns described below (Table 5).
Table 5.
Coping mechanisms employed by caregivers to use small‐quantity, lipid‐based nutrient supplement (SQ‐LNS) as indicated
| Patterns of SQ‐LNS utilization | Caregiver coping mechanisms |
|---|---|
| OVERUSE | |
| Caregiver consumption of SQ‐LNS | • None reported or observed |
| Sharing SQ‐LNS with children older than 2 years |
• Preparing extra food for older children • Feeding the SQ‐LNS to child 6–23 months in private |
| Children older than 2 years taking SQ‐LNS from household |
• Moving hiding place of SQ‐LNS frequently • Hanging SQ‐LNS out of reach with a cloth or capulana † • Storing SQ‐LNS in a neighbour's house • Securing SQ‐LNS in a padlocked bedroom |
| Daily provision of >1 sachet to child 6–23 months |
• Adding sugar to porridge of child 6–23 months to replicate the sweet flavour of SQ‐LNS • Making extra meals for the child 6–23 months |
| UNDERUSE | |
| Forgetting to provide SQ‐LNS | • Getting reminders from household members |
| Not being permitted to give SQ‐LNS by husbands | • None reported or observed |
A capulana is a sarong worn by women primarily in Mozambique.
Caregiver sharing of SQ‐LNS with children >2 years of age
Caregivers in both settings shared the SQ‐LNS with non‐beneficiary children. Children U5 years were observed to be in proximity to meal preparation and feeding of children 6–23 months and made repeated efforts to consume the SQ‐LNS in such situations. Non‐beneficiary, older children were observed both repeatedly asking and crying for the product during serving.
‘…I have two children and one of them did not receive the product because he is over two years old. On the days that there was no food in the house, of course the product was used to feed both of the two children because it would be illogical having one child served food while the other is starving. As a mother, I prefer to serve a little portion of food for each child’.
Mwani Female Caregiver, Interview in Mozambique
Children in these settings who are closer to 2 years than to 6 months were observed having more freedom to walk around their communities independently and thus experienced more pressure from other children to share the SQ‐LNS. Older children (e.g. 3–8 years) were observed living, eating and playing together throughout the day. Village life is largely communal and interdependent in Chewa, Macua and Mwani communities, creating environments where sharing of the SQ‐LNS with non‐beneficiary, non‐household children was difficult to avoid for households that view food sharing as a core cultural value.
‘It will be very hard to be indifferent if I see a child crying for the product. I am a mother and I feel like a mother. I can prohibit my older children perhaps but I will be heartbroken if I see younger children from the neighboring house crying for the product. I do not know if the best way is to hide this product and to feed my children inside the house…I don't know. This is difficult’.
Mwani Female Caregiver, Interview in Mozambique
Some caregivers found success by feeding the SQ‐LNS in privacy. One Mozambique caregiver explained, ‘I always fed her (beneficiary) the product (SQ‐LNS) when other kids were absent and this (strategy) seemed to work.’ Caregivers who responsively fed their young children the SQ‐LNS, rather than leaving them to eat it on their own, more successfully avoided sharing it. Also, caregivers who made food for the older children to eat when the child 6–23 months was consuming the product faced less pressure to share. However, household food shortages made such a coping strategy not feasible for many households, especially in Malawi where data were collected during the lean season.
Children >2 years taking SQ‐LNS from households
Dwellings in villages of both settings generally lack the safe storage spaces necessary to keep children away from valuable household items. Theft is sometimes an issue in villages, as one caregiver in Malawi explained, ‘People steal in this community, they steal a lot, they steal things like chickens, goats, cows, even furniture and things in the house…they can enter the house and steal things’. Coupled with incidents of theft, a lack of safe storage was a challenge for caregivers trying to ration the SQ‐LNS provision.
‘I kept it (SQ‐LNS) in a bucket…but the other children would spy on me when I went to store it and I believe they stole some of it while I was on the farm, because when I came back I did not find all of the packets as I had left them’.
Macua Female Caregiver, Interview in Mozambique
Caregivers used a few different strategies to overcome this challenge: (1) moving the hiding place of the product every few days; (2) wrapping the product in a traditional cloth sarong or bag and hanging it out of the reach of children; (3) keeping the product in a padlocked bedroom; and (4) storing the product in a neighbour's house where no children lived.
Daily provision of >1 SQ‐LNS sachet to the child 6–23 months
Providing more than one SQ‐LNS sachet per child 6–23 months per day was more commonly observed in Mozambique than in Malawi. This overconsumption was a result of beneficiaries asking for more of the product throughout the day and the caregivers succumbing to those demands.
‘The child would sometimes insist on eating another packet immediately after finishing the first…and because the product is good (nutritious), I would serve another sachet, despite your team having told me that I shouldn't give more than one packet per day’.
Macua Female Caregiver, Interview in Mozambique
In some instances, beneficiary children demanded to have as much of the product as possible. One mother said, ‘My son ate two, three and four sachets per day. When I refused to give him more, he even would hit me.’ Some caregivers prepared extra meals when children demanded more of the SQ‐LNS. Others found success using sugar to fortify porridge, leading the child 6–23 months into thinking that the product had been added to the porridge.
Product underuse
Forgetting to give SQ‐LNS to the beneficiary child
Forgetting to provide the SQ‐LNS proved to be a challenge for mothers when they had to travel outside of their community and would forget to pack the product. Maternal caregivers indicated that getting reminders from other household members was helpful in ensuring that they would not forget to give the product to their children 6–23 months on a daily basis. A lack of paternal caregiver support in IYCF was a barrier to appropriate product usage.
‘The caregiver did not give the child the product for a few days and because of this there were 22 instead of 14 sachets left during the spot check. According to her account, when she goes to the farm, she asks her husband to feed the child the product, which he never does’.
Data Collector, Direct Observation Field Notes in Mozambique
Two solutions to this issue offered by community members were ‘sensitizing parents together’ and ‘workshops for dads’.
Not being permitted to give SQ‐LNS by husband
In Mozambique specifically, caregivers who were not providing the SQ‐LNS to the beneficiary children reported that they did not do so because they were not given permission by their husbands. This finding emerged only among some Mwani families that practice Islam. Interview data revealed that female caregivers in these households required the permission of their husbands prior to introducing a new behaviour or product, and in such cases that support was not received largely because of lack of information related to whether the SQ‐LNS was halal. When discussing the SQ‐LNS packaging, one Mwani caregiver emphasized this point by saying, ‘You need to add the word halal because there are Macuas who are also Muslims (in this area)’. Suggesting that not only her community but others would prefer a product that is culturally appropriate.
Discussion
Overall, it was common that the SQ‐LNS was not strictly used according to the instructions that included provision of one complete sachet per day, per child aged 6–23 months. There were many incidents of other children and caregivers consuming the product, as well as lack of daily provision per recommended usage. We observed high rates of sharing within and between households. Patterns of household SQ‐LNS utilization were very similar in Malawi and Mozambique where interdependent cultural contexts are defined by a fundamental relatedness of individuals, attending to others and living harmoniously (Markus & Kitayama 1991). Such a core cultural value has been found elsewhere to also drive key socio‐cultural practices, including household food sharing patterns (Speth 1990; Gittelsohn 1991) and nutrition supplement utilization (Bonvecchio et al. 2007). Consider the excerpt from a caregiver quote provided earlier in this paper in relation to SQ‐LNS utilization: ‘Sharing is happening…I cannot lie’. This statement underscores the strength of interdependence as an underlying social value in Malawi, bringing to light the potential challenges and consequences of targeted nutrition programmes in similar contexts, including specialized nutritious food sharing (Marchione 2005).
Despite this underlying cultural similarity in Malawi and Mozambique, setting‐specific findings emerged as well, indicating some variability by cultural context stemming from religious practices, varying levels of trust toward local development organizations as well as seasonal influences on household food access and availability. Data reveal that SQ‐LNS utilization was determined by factors at multiple levels, governed by caregiver decision‐making in line with core cultural values and as coping mechanisms in light of household food insecurity, rather than a mere disregard for programme guidelines. Fig. 1 illustrates the salient patterns of SQ‐LNS utilization, including the immediate and underlying behavioural factors at multiple levels organized through the lens of a socio‐ecological framework (McLeroy et al. 1988).
Figure 1.
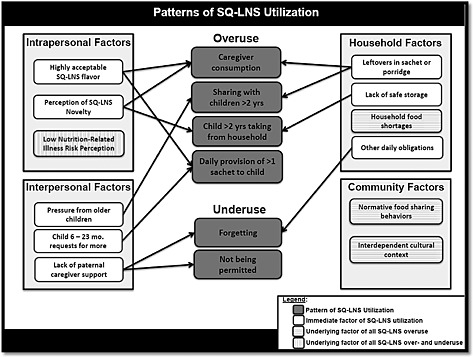
Multi‐level factors and their influence on small‐quantity, lipid‐based nutrient supplement (SQ‐LNS) utilization patterns in Malawi and Mozambique
These findings indicate that the large majority of intended beneficiaries were not receiving the recommended quantity of the SQ‐LNS throughout much of the study duration. These findings may help to, at least partially, explain why the specialized nutritious food, which theoretically offers a viable option for preventing chronic malnutrition, has shown only modest improvements in linear growth of children 6–23 months in efficacy trials (Adu‐Afarwuah et al. 2007; Phuka et al. 2008; Dewey et al. 2009). After all, 87.0% of the Mozambican households in the current investigation did not use the SQ‐LNS as recommended, with numerous manifestations of allocation to non‐beneficiaries. If other studies in comparable contexts have similar utilization patterns, then the limited impacts of such products on nutritional status should not be surprising. A number of efficacy trials are currently underway globally to determine to what extent SQ‐LNS may impact upon child undernutrition in different contexts (Arimond et al. 2013). Assessments of household SQ‐LNS utilization should complement the methods of those trials to understand to what extent, if any, it may be determining nutritional impacts.
Our findings contradict much of the already‐established research on the topic that has indicated only minimal SQ‐LNS sharing during prevention‐focused interventions. The majority of previous work in this area has sought to understand SQ‐LNS sharing practices using questionnaires, focus group discussions or interviews (Parker et al. 2011; Phuka et al. 2011; Cohuet et al. 2012; Ickes et al. 2012; Ashorn et al. 2015) and self‐reporting methods, which likely underestimate the amount of sharing that occurs. In a study in Niger by Cohuet et al. (2012) and another in Malawi by Phuka et al. (2011) that relied exclusively on self‐report, results suggest that sharing of SQ‐LNS occurred but only minimally at 23.7% and 20.4% of the time, respectively. In Burkina Faso, researchers found a 97(± 6)% self‐reported adherence to an SQ‐LNS, but direct observation data indicated that only 63 and 54% of children 11 and 16 months, respectively, received the product (Abbeddou et al. 2014). Studies by Parker et al. (2011) in Malawi and Ickes et al. (2012) in Uganda acknowledged that sharing of SQ‐LNS occurred but they did not quantify the practice to understand its magnitude. Such self‐reported findings should be taken with caution, however, as caregivers are not always present during children's meals or in cases when children share food or take it from other households. Caregivers frequently do not accurately observe what portion of food their child ate (Shankar et al. 2001) or shared. Thus, caregivers' dietary recall and self‐report of SQ‐LNS sharing practices among young children may be based on limited knowledge.
Other studies have tried to overcome this methodological shortcoming by incorporating mealtime observations into monitoring of SQ‐LNS utilization. Tripp and colleagues (2011) used both self‐report and household meal observations in Niger to capture sharing practices. They found similar results to those of the self‐report studies and concluded that among their sample, ‘most women did not share’ because only 5/80 mothers reported giving the product away to non‐beneficiaries. Their direct observation data revealed that despite pressure to share, the participants of their study largely refrained from doing so. Similarly, Flax and colleagues (2010) in Malawi using single‐day observations (6:30 am–5:30 pm) of enrolled children found that sharing of SQ‐LNS occurred only 5% of the time (4/75 observations) without any change in child weight‐for‐age z‐score.
Methodological differences between our study and other studies may help to explain the discrepant findings. Unlike other small home‐feeding trials, which were shorter in duration and reported minimal sharing (e.g. 2 weeks in Malawi: Phuka et al. 2011; 4 weeks in Niger: Tripp et al. 2011), our research time frames were 8 and 6 weeks long. With repeated direct observations over time, our study was able to illustrate increased allocation to non‐beneficiaries during later direct observations compared with those conducted earlier in the home trial, an indication of either more natural behaviour (i.e. less reactivity) occurring or increased sharing over time. Behavioural research on other health‐seeking behaviours illustrates that engaging in sustained, positive health‐seeking behaviour change is difficult over longer periods of time when a person's environment is often filled with cues (e.g. seeing other non‐beneficiary children crying for SQ‐LNS) for falling back on comfortable, normative behaviour (Prochashka et al. 1994). For example, Allen (2002) explained that the lack of programmatic success with iron supplement compliance can be attributed to the need for those supplements to be taken daily and over long periods of time. Similarly then with an SQ‐LNS, which is currently recommended to be consumed daily for a period of 18 months, shorter household trials may indicate less sharing but be less reflective of the reality within a full‐length intervention aimed at prevention of stunting.
Also, the logistics of our trials may uniquely have contributed to the high rates of sharing. Because of limited capacity, our studies distributed one initial batch of SQ‐LNS to households (56 sachets in Malawi; 42 sachets in Mozambique) only at the onset of the trial, leaving ample time for various forms of usage throughout the study periods. To be sure, our results indicate that nearly all households ran out of product supply too early. This finding is similar to that of studies in Malawi (Flax et al. 2010) and Guatemala (Davis et al. 2014), where SQ‐LNS supplies also ran out early because of sharing, albeit less extensively. More frequent distributions of the SQ‐LNS (e.g. every 1 or 2 weeks) would reduce the amount of time and product available for allocation to non‐beneficiaries, a strategy that has been used to improve adherence in other nutrition programmes (Inayati et al. 2012). However, Ntchisi and Cabo Delgado cover large geographic areas with long distances and weak transportation infrastructures connecting villages. Ensuring a reliable supply chain and logistics necessary for frequent product distribution may prove difficult, especially during a rainy season.
This investigation is one of the first to triangulate multiple methods for understanding patterns of household SQ‐LNS utilization in extended home‐feeding trials as part of nutrition intervention formative research. Thus, our findings of extensive SQ‐LNS sharing may due to the utilization of the most appropriate methods for capturing the behaviour in question. This study was able to both document the amount and types of sharing through unannounced spot checks and full‐day observations, as well as to contextualize its occurrence through observation field notes and in‐depth interviews. It also used several rounds of full‐day observations to understand SQ‐LNS utilization. Other studies used either a single full day of meal observations (Flax et al. 2010; Abbeddou et al. 2015) or multiple days of individual meal observations or feeding episodes (Tripp et al. 2011; Davis et al. 2014), research designs that potentially yielded different results from those in this study.
This work had its limitations. First, it was conducted during only one season of the year in each setting. Findings are likely season‐specific and should not be extrapolated to other seasons as food availability differs from season to season in these contexts and may impact upon household SQ‐LNS utilization. Also, it is likely that behaviours were impacted by the presence of observers. However, this study employed multiple rounds of repeated observations to reduce reactivity and understand more natural behaviours related to our research questions (Gittelsohn et al. 1997).
While cultural contexts differ and practices may somewhat vary by setting, this formative research suggests that for SQ‐LNS to have its desired effect within the context of a prevention‐focused nutrition intervention, the barrier of product sharing may be formidable. Using the sociocultural information generated from the larger formative research efforts within which these home‐feeding trials were nested (Kodish et al. 2015a,b) culturally appropriate and targeted BCC should be developed as a core component of programming (Kreuter et al. 2003; Fabrizio et al. 2014). After all, culture and health‐related practices are inextricably linked (Napier et al. 2014). Because SQ‐LNS programmes are relatively new, they might benefit from drawing from the experiences of MNP interventions which, to date, have been implemented in more settings globally with many programmatic lessons learned (Kodish et al. 2011; Rah et al. 2012; De‐Regil et al. 2013; Jefferds et al. 2013). In the short term, other studies that are utilizing SQ‐LNS as a preventative measure for children aged 6–23 months should use rigorous methodology to understand household utilization, as well as document the impact of BCC on those practices within the context of interventions (HF‐TAG 2013). In the long term, the international nutrition community needs to continue to research and develop community‐led strategies for improving the nutritional status of vulnerable populations with a focus on intervention implementation across the life cycle from adolescence through until childhood (Bhutta et al. 2013).
Acknowledgements
We would first like to thank the communities in each setting for participating in this study. We also sincerely acknowledge our hardworking data collection teams. The team in Malawi comprised Yamikani Kunashe, Evelyne Kamwendo, Ndapile Bwanausi, Chifundo Nsanjama and Eric Maonga. The team in Mozambique included Afonso Campos, Vasco Buanausse, Adriano Antonio, Dionisia Mucussete, Gustave Ndagijimana, Carolina Cardoso, Adao Eduardo, Abdul Faque, Focas Malimbili and Amido Ussene. We are grateful to the many WFP country and headquarters office staff members who supported this project in a variety of invaluable ways, the Children's Investment Fund Foundation (CIFF), which funded this work, and the governments of Malawi and Mozambique for their support.
Source of funding
This study was funded by the Children's Investment Fund Foundation (CIFF).
Conflict of interest
The authors declare that they have no conflicts of interest.
Contributions
SK developed the research protocol, led data collection and analysis in the field, and drafted the manuscript. NJA, MNH, and FD provided peer review throughout the data collection and analysis periods, as well as offered critical feedback during manuscript preparation. JG was the principal investigator and provided guidance, feedback and critical review at each stage of this study.
Kodish S. R., Aburto N. J., Nseluke Hambayi M., Dibari F., and Gittelsohn J. (2017) Patterns and determinants of small‐quantity LNS utilization in rural Malawi and Mozambique: considerations for interventions with specialized nutritious foods, Maternal & Child Nutrition, 13, e12234. doi: 10.1111/mcn.12234.
Footnotes
The small‐quantity LNS used for this research was Nutributter® (20 g), made by Nutriset (Maulanay, France). Each reference to ‘SQ‐LNS’ hereafter refers to this particular small‐quantity, 20‐g product unless otherwise specified.
References
- Abbeddou S., Hess S.Y., Yakes J.E., Somé J.W., Vosti S.A., Guissou R.M. et al. (2015) Comparison of methods to assess adherence to small‐quantity lipid‐based nutrient supplements (SQ‐LNS) and dispersible tablets among young Burkinabé children participating in a community‐based intervention trial. Maternal & Child Nutrition. DOI: 10.1111/mcn.12162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adu‐Afarwuah S., Lartey A., Brown K.H., Zlotkin S., Briend A. & Dewey K.G. (2007) Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghana: effects on growth and motor development. American Journal of Clinical Nutrition 86, 412–420. [DOI] [PubMed] [Google Scholar]
- Adu‐Afarwuah S., Lartey A., Zeilani M. & Dewey K.G. (2011) Acceptability of lipid‐based nutrient supplements (LNS) among Ghanaian infants and pregnant or lactating women. Maternal & Child Nutrition 7, 344–356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed T., Hossain M. & Sanin K.I. (2012) Global burden of maternal and child undernutrition and micronutrient deficiencies. Annals of Nutrition & Metabolism 61 (Suppl.1), 8–17. [DOI] [PubMed] [Google Scholar]
- Allen L.H. (2002) Iron supplements: scientific issues concerning efficacy and implications for research and programs. The Journal of Nutrition 132 (4), 813S–819S. [DOI] [PubMed] [Google Scholar]
- Arimond M., Zeilani M., Jungjohann S., Brown K.H., Ashorn P., Allen L.H. et al. (2013) Considerations in developing lipid‐based nutrient supplements for prevention of undernutrition: experience from the International Lipid‐Based Nutrient Supplements (iLiNS) Project. Maternal & Child Nutrition, 1–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashorn U., Alho L., Arimond M., Dewey K.G., Maleta K., Phiri N. et al. (2015) Malawian mothers consider lipid‐based nutrient supplements acceptable for children throughout a 1‐year intervention, but deviation from user recommendations is common. Journal of Nutrition. DOI: 10.3945/jn.114.209593. [DOI] [PubMed] [Google Scholar]
- Bernard H.R. (2006) Research Methods in Anthropology, 2nd edn. Sage Publications, Inc.: Thousand Oaks, CA. [Google Scholar]
- Bhutta Z.A., Das J.K., Rizvi A., Gaffey M.F., Walker N., Horton S. et al. (2013) Evidence‐based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet 382, 452–477. [DOI] [PubMed] [Google Scholar]
- Black R.E., Victoria C.G., Walker S.P., Bhutta Z.A., Christian P., de Onis M. et al. (2013) Maternal and child undernutrition and overweight in low‐income and middle‐income countries. Lancet 382, 427–451. [DOI] [PubMed] [Google Scholar]
- Bonvecchio, A. , Pelto, G.H. , Escalante, E. , Monterrubio, E. , Habicht, J.P. , Nava, F. et al. (2007) Maternal knowledge and use of a micronutrient supplement was improved with a programmatically feasible intervention in Mexico. The Journal of Nutrition 137 (2), 440–446. [DOI] [PubMed] [Google Scholar]
- Charmaz K. (2006) Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. Sage Publications: London. [Google Scholar]
- Cohuet S., Marquer C., Shepherd S., Captier V., Langendorf C., Ale F. et al. (2012) Intra‐household use and acceptability of ready‐to‐use‐supplementary‐foods distributed in Niger between July and December 2010. Appetite 59, 698–705. [DOI] [PubMed] [Google Scholar]
- Davis T.E., Fischer E.F., Rohloff P.J. & Heimburger D.C. (2014) Chronic malnutrition, breastfeeding, and ready to use supplementary food in a Guatemalan Maya town. Human Organization 73, 72–81. [Google Scholar]
- Dettwyler K.A. (1989) Styles of infant feeding: parental/caretaker control of food consumption in young children. American Anthropology 9, 696–703. [Google Scholar]
- Dewey K.G. & Arimond M. (2012) Lipid‐based nutrient supplements: how can they combat child malnutrition? PLoS Medicine. DOI: 10.1371/journal.pmed.1001314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dewey K.G., Yang Z. & Boy E. (2009) Systematic review and meta‐analysis of home fortification of complementary foods. Maternal & Child Nutrition 5, 283–321. [Google Scholar]
- Demographic and Health Survey [DHS] (2010) Malawi Demographic and Health Survey. [Online] Available at: http://dhsprogram.com/pubs/pdf/FR247/FR247.pdf (Accessed 13 June 2014).
- Demographic Health Survey [DHS] (2011) Mozambique DHS—final report (Portuguese). [Online] Available at: http://www.measuredhs.com/publications/publication-FR266-DHS-Final-Reports.cfm (Accessed 1 May 2014).
- De‐Regil L.M., Suchdev P.S., Vist G.E., Walleser S. & Pena‐Rosas J.P. (2013) Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age (review). Evidence‐Based Child Health: A Cochrane Review Journal 8 (1), 112–201. [DOI] [PubMed] [Google Scholar]
- Fabrizio C.S., van Liere M. & Pelto G. (2014) Identifying determinants of effective complementary feeding behavior change interventions in developing countries. Maternal & Child Nutrition 10, 575–592. DOI: 10.1111/mcn.12119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flax V.L., Thakwalakwa C., Phuka J., Ashorn U., Cheung Y.B., Maleta K. et al. (2009) Malawian mothers' attitudes towards the use of two supplementary food for moderately malnourished children. Appetite 53, 195–202. [DOI] [PubMed] [Google Scholar]
- Flax V.L., Phuka J., Cheung Y.B., Ashorn U., Maleta K. & Ashorn P. (2010) Feeding patterns and behaviors during home supplementation of underweight Malawian children with lipid‐based nutrient supplements or corn‐soy blend. Appetite 54, 504–511. [DOI] [PubMed] [Google Scholar]
- Gittelsohn J. (1991) Opening the box: intrahousehold food distribution in rural Nepal. Social Science & Medicine 33 (10), 1141–1154. DOI: 10.1016/0277-9536(91)90230-A. [DOI] [PubMed] [Google Scholar]
- Gittelsohn J., Shankar A.V., Ram R., Gnywali T. & West K.P. (1997) Estimating reactivity and its effects in direct observation studies of health behavior. Human Organization 56 (2), 182–189. [Google Scholar]
- Gittelsohn J., Shankar A.V., West K.P., Faruque F., Gnywali T. & Pradhan E.K. (1998) Child feeding and care behaviors are associated with xeropthalmia in rural Nepalese households. Social Science and Medicine 47 (4), 477–486. [DOI] [PubMed] [Google Scholar]
- Glaser B. & Strauss A. (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research. New York, NY: Aldine de Gruyter. [Google Scholar]
- Haddad L. & Kanbur R. (1992) The value of intra‐household survey data for age‐based nutritional targeting. Annales d'Economie et de Statistique 29, 65–81. [Google Scholar]
- Hess S.Y., Bado L., Aaron G.J., Ouedraogo J.B., Zeilani M. & Brown K.H. (2011) Acceptability of zinc‐fortified, lipid‐based nutrient supplements (LNS) prepared for young children in Burkina Faso. Maternal & Child Nutrition 7, 357–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hess S.Y., Abbeddou S., Jimenez E.Y., Somé J.W., Vosti S.A., Ouédraogo Z.P. et al. (2015) Small‐quantity lipid‐based nutrient supplements, regardless of their zinc content, increase growth and reduce the prevalence of stunting and wasting in young Burkinabe children: a cluster‐randomized trial. PLoS ONE 10 (3). DOI: 10.1371/journal.pone.0122242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Home Fortification Technical Advisory Group (HF‐TAG) (2013) Monitoring manual for developing and implementing monitoring systems for home fortification interventions. HF‐TAG: Geneva. [Google Scholar]
- Ickes S.B., Jilcott S.B., Myhre J.A., Adair L.S., Thirumurthy H., Handa S. et al. (2012) Examination of facilitators and barriers to home‐based supplemental feeding with ready‐to‐use‐food for underweight children in western Uganda. Maternal & Child Nutrition 8, 115–129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inayati D.A., Scherbaum V., Purwestri R.C., Wirawan N.N., Suryantan J., Hartono S. et al. (2012) Combined intensive nutrition education and micronutrient powder supplementation improved nutritional status of mildly wasted children on Nias Island, Indonesia. Asia Pacific Journal of Nutrition 21 (3), 361–373. [PubMed] [Google Scholar]
- Jefferds M.E., Irizarry L., Timmer A. & Tripp K. (2013) UNICEF–CDC global assessment of home fortification interventions 2011: current status, new directions, and implications for policy and programmatic guidance. Food and Nutrition Bulletin 34 (4), 434–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kigutha H.N. (1997) Assessment of dietary intake in rural communities in Africa: experiences in Kenya. American Journal of Clinical Nutrition 65, 1168–1172. [DOI] [PubMed] [Google Scholar]
- Kitanichi K. (2000) The Aka and Baka: food sharing among two central Africa hunter‐gatherers [Online]. Senri Ethnological Studies 53, 149–169. Available at: http://camel.minpaku.ac.jp/dspace/bitstream/10502/907/1/SES53_008.pdf (Accessed 5 June 2014) [Google Scholar]
- Kodish S., Aburto N., Nseluke H.M., Kennedy C. & Gittelsohn J. (2015a) Identifying the sociocultural barriers and facilitating factors to nutrition‐related behavior change: formative research for a stunting prevention program in Ntchisi, Malawi. Food and Nutrition Bulletin 36 (2), 138–153. [DOI] [PubMed] [Google Scholar]
- Kodish S., Aburto N., Dibari F., Brieger W., Agostinho S.P. & Gittelsohn J. (2015b) Informing a behavior change communication strategy: formative research findings from the scaling up nutrition (SUN) movement in Mozambique. Food and Nutrition Bulletin 36 (3), 354–370. [DOI] [PubMed] [Google Scholar]
- Kodish S., Rah J.H., Kraemer K., de Pee S. & Gittelsohn J. (2011) Understanding low usage of micronutrient powder in the Kakuma Refugee Camp, Kenya: findings from a qualitative study. Food and Nutrition Bulletin 32 (3), 292–303. [DOI] [PubMed] [Google Scholar]
- Kreuter M.W., Lukwago S.N., Bucholtz D.C., Clark E.M. & Sanders‐Thompson V. (2003) Achieving cultural appropriateness in health promotion programs: targeted and tailored approaches. Health Education & Behavior 30 (2), 133–146. [DOI] [PubMed] [Google Scholar]
- Kumwenda C., Dewey K.G., Hemsworth J., Ashorn P., Maleta K. & Haskell M.J. (2014) Lipid‐based nutrient supplements do not decrease breast milk intake of Malawian infants. The American Journal of Clinical Nutrition 99 (3), 617–623. [DOI] [PubMed] [Google Scholar]
- Marchione T.J. (2005) Interactions with the recipient community in targeted food and nutrition programs. The Journal of Nutrition 135 (4), 886–889. [DOI] [PubMed] [Google Scholar]
- Markus H.R., Kitayama S. (1991) Culture and the self: Implications for cognition, emotion, and motivation. Psychological review 98 (2), 224. [Google Scholar]
- Markus H.R. & Kitayama S. (2003) Culture, self, and the reality of the social. Psychological Inquiry 14 (3–4), 277–283. [Google Scholar]
- Maternal and Child Nutrition Study Group (2013) Maternal and child nutrition: building momentum for impact. Lancet 382, 372–375. [DOI] [PubMed] [Google Scholar]
- McLeroy K.R., Bibeau D., Steckler A. & Glanz K. (1988) An ecological perspective on health promotion programs. Health Education & Behavior 15 (4), 351–377. [DOI] [PubMed] [Google Scholar]
- Miles M.B. & Huberman A.M. (1994) Qualitative Data Analysis, 2nd edn. Sage Publications: Thousand Oaks, CA. [Google Scholar]
- Morgan D. (1997) Focus Groups as Qualitative Research, 2nd edn. Sage Publications: Thousand Oaks, CA. [Google Scholar]
- Morris M.W., Lueng K., Ames D. & Lickel B. (1999) Views from inside and outside: integrating emic and etic insights about culture and justice judgment. Academy of Management Review 24 (4), 781–796. [Google Scholar]
- Napier, A.D. , Ancarno, C. , Butler, B. , Calabrese, J. , Chater, A. , Chatterjee, H. et al. (2014) Culture and health. The Lancet 384 (9954), 1607–1639. [DOI] [PubMed] [Google Scholar]
- Paolisso M. & Regmi C.S. (1992) Gender and the Commercialization of Subsistence Agriculture in Nepal. International Center for Research on Women and New ERA: Washington, D.C. & Kathmandu, Nepal. [Google Scholar]
- Parker M.E., Bentley M.E., Chasela C., Adair L., Piwoz E.G., Jamieson D.J. et al. (2011) The acceptance and feasibility of replacement feeding at 6 months as an HIV prevention method in Lilongwe, Malawi: results from the BAN study. AIDS Education and Prevention 23 (3), 281–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton M.Q. (2002) Qualitative Evaluation and Research Methods, 3rd edn. Sage Publications: Thousand Oaks, CA. [Google Scholar]
- Paul K.H., Muti M., Chasekwa B., Mbuya M.N., Madzima R.C., Humphrey J.H. et al. (2012) Complementary feeding messages that target cultural barriers enhance both the use of lipid‐based nutrient supplements and underlying feeding practices to improve infant diets in rural Zimbabwe. Maternal and Child Nutrition 8, 225–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phuka J., Maleta K., Thakwalakwa C., Cheung Y.B., Briend A., Manary M.J. et al. (2008) Complementary feeding with fortified spread and incidence of severe stunting in 6‐ to 18‐month‐old rural Malawians. Archives of Pediatrics and Adolescent Medicine 162, 619–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phuka J., Ashorn U., Ashorn P., Zeilani M., Cheung Y.B., Dewey K.G. et al. (2011) Acceptability of three novel lipid‐based nutrient supplements among Malawian infants and their caregivers. Maternal and Child Nutrition 7, 368–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prochaska J.O., Redding C.A., Harlow L.L., Rossi J.S. & Velicer W.F. (1994) The transtheoretical model of change and HIV prevention: a review. Healthy Education Quarterly 21 (4), 471–486. [DOI] [PubMed] [Google Scholar]
- Rah J.H., De Pee S., Kraemer K., Bloem M.W., Spiegel P., Wilkinson C. et al. (2012) Program experience with micronutrient powders and current evidence. Journal of Nutrition 142 (1), 191S–196S. [DOI] [PubMed] [Google Scholar]
- Sandelowski M. (2000) Combining qualitative and quantitative sampling, data collection, and analysis techniques in mixed‐method studies. Research in Nursing & Health 23, 246–255. [DOI] [PubMed] [Google Scholar]
- Scaling up Nutrition [SUN] . A framework for action (2014). [Online] Available at: http://scalingupnutrition.org/sun-countries (Accessed 5 April 2014).
- Scrimshaw S.C.M. & Hurtado E. (1987) Rapid Assessment Procedures for Nutrition and Primary Health Care: Anthropological Approaches to Improving Programme Effectiveness. UNU Press: Tokyo. [Google Scholar]
- Shankar A.V., Gittelsohn J., Stalling R., West K.P., Gynwali T., Dhungel C. et al. (2001) Comparison of visual estimates of children's portion sizes under both shared‐plate and individual‐plate conditions. Journal of American Dietary Association 101 (1), 47–52. [DOI] [PubMed] [Google Scholar]
- Shankar A.V., Gittelsohn J., West K.P., Stalling R., Gnywali T. & Faruque F. (1998) Eating from a shared plate affects food consumption in vitamin A‐deficient Nepali children. Journal of Nutrition 128 (7), 1127–1133. [DOI] [PubMed] [Google Scholar]
- Siega‐Riz A.M., Estrada Del Campo Y., Kinlaw A., Reinhart G.A., Allen L.H., Shahab‐Ferdows S. et al. (2014) Effect of supplementation with a lipid‐based nutrient supplement on the micronutrient status of children aged 6–18 months living in the rural region of Intibucá, Honduras. Paediatric and Perinatal Epidemiology 28 (3), 245–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Speth J.D. (1990) Seasonality, resource stress, and food sharing in so‐called “egalitarian” foraging societies. Journal of Anthropological Archaeology 9 (2), 148–188. [Google Scholar]
- Strauss A. & Corbin J. (1990) Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Sage Publications, Inc: Newbury Park. [Google Scholar]
- Tripp K., Perrine C.G., de Campos P., Knieriemen M., Hartz R., Ali F. et al. (2011) Formative research for the development of a market‐based home fortification programme for young children in Niger. Maternal & Child Nutrition 7 (3), 82–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vitta B. & Dewey K.G. (2012) Identifying Micronutrient Gaps in the Diets of Breastfed 6–11‐Month‐old Infants in Bangladesh, Ethiopia, and Viet Nam Using Linear Programming. Alive & Thrive: Washington, DC. [Google Scholar]