

Abstract
Spinal cord injury is a global problem. It is a devastating life altering condition that is associated with permanent disability and reduced life expectancy.
Road traffic accident has been described in global literature as the commonest aetiology and second to it is falls. Identifying these factors have led to development of policies and advocacy to reduce these causes of spinal cord injuries.
We present three cases of spinal cord injuries from unusual aetiologies viz-a-viz an accidental hanging which resulted in a C4 traumatic myelopathy Frankel A in a 30-year old artisan, playful neck manipulation in a 23-year old male student, resulting in Brown-Sequard syndrome, which resolved with non-operative spinal cord injury management protocol over six weeks and a C4 traumatic myelopathy Frankel D with a 50% anterior listhesis of C4 on C5 in a 50-year old man who sustained injuries from a choke hold 10 weeks prior to presentation. He recovered fully on non-operative management and discharged home Frankel E.
Keywords: Spinal cord injury, Browne-Sequard, Frankel
INTRODUCTION
Spinal cord injury (SCI) is a devastating life altering condition, which may be associated with permanent disability and can also lead to decreased life expectancy. It has long been recognized as a key problem in West Africa1.
Several aetiological factors for SCI have been described in the literature. Globally, the most common aetiology for spinal cord injury remains Road traffic accident (R.T.A.), followed by falls2. The 2007 global estimates reports an incidence of 133-226 thousand incident cases from R.T.A. and violence3. This tallies with the findings of the studies that have reported different aetiological factors for spinal cord injury in Nigeria. A 4- year review by Solagberu B.A. with 39 patients, showed R.T.A. as the cause of injury in 67% of the patients, falls in 23%, while misadventure accounted for injuries in 10% of the study group4. This study however did not explain what is classified as misadventure. A larger series spanning a 10-year period between 1997- 2007, with 161 patients also showed 79.7% injuries due to R.T.A., 13.4% of cases due to falls and 10% of cases were due to assault and 1 % not clearly defined.
Though falls and road traffic accidents constitute the main mechanisms for spinal cord injuries, other less prominent mechanisms of spinal cord injuries resulting mainly in incomplete spinal cord injuries also form a group that are of concern. When hanging usually non-judicial, does not result in fatality, it is described as near hanging. Neurologic injuries with a predominance of head injuries, from near hanging have been described mostly amongst prison inmates attempting suicide5. There is an estimated 1348/100,000 population near hanging injuries in the United States population annually6.
The identification of these aetiologies, has provoked an effort towards reduction of road crashes in particular through legislations and advocacy as well as bringing to fore the near hanging injuries which may not be considered when developing laws and protocols for spinal cord injuries.
We present three (3) cases of cervical spinal cord injuries from unusual mechanisms of inadvertent and forceful neck manipulations and an accidental near hanging.
CASE 1.
D.D is a 30-year old artisan who was seen via the Emergency department of the University College Hospital, Ibadan. He presented with features of a C3 traumatic myelopathy Frankel A (Complete SCI) about 8hrs following passenger motor vehicular accident. He was standing at the back of a semi-trailer truck being driven through a bush in south-western Nigeria. His neck was inadvertently trapped by a telephone wire line hanging between two trees in the bush. It was an apparent incomplete hanging with his feet still in contact with the truck. He remained fully conscious but immediately became quadriplegic with no evidence of strangulation.
The C-spine Xray did not show any translation or fractures. (Fig 1). He discharged against medical advice thus precluding evaluation with MRI. There was no improvement in his neurologic status prior to his leaving the hospital.
Fig. 1:

Cervical spine X-ray (Lateral and Open mouth view)
CASE 2
R.A. is a 23-year old, male student of a tertiary institution, in the Southwestern region of Nigeria, who presented to the emergency department, with an 11- hour history of quadriparesis worse on the left side where he was completely plegic. This occurred following a chokehold and a twist to his neck by a friend while they were playing. He developed the symptoms immediately and presented at a private hospital, from where he was referred to us without any neck support.
Examination revealed a young man with normal general examination findings and no features suggestive of brain injury. He had normal muscle bulk and tone. He was plegic in the left hemibody but had M.R.C. grade 4-5 in the right upper and lower limb muscle groups. The deep tendon reflexes were brisk on the left. The sensory level was at C6 with residual sensation to S4/S5. The anal wink and bulbocarvenous reflex were present. We made a clinical diagnosis of C3 traumatic myelopathy, Frankel C.
The cervical spine X-ray showed normal lordosis with no translation (Fig. 2D). The C-spine MRI done about 5days post trauma, revealed cord hyperintensity suggesting cord edema or contusion at C1/C2 (Fig.2A&B) and intradural, extramedullary hypointensity suggestive of a bleed at C7 with mild indentation on the cord anteriorly (Fig. 2C). He was managed non-operatively in a rigid cervical collar and immobilized in bed. He progressively improved and was discharged with power in the left hemibody muscle groups MRC grade 3-5. He is 18 months post trauma and is self-ambulant with full power across all muscle groups.
Fig. 2:
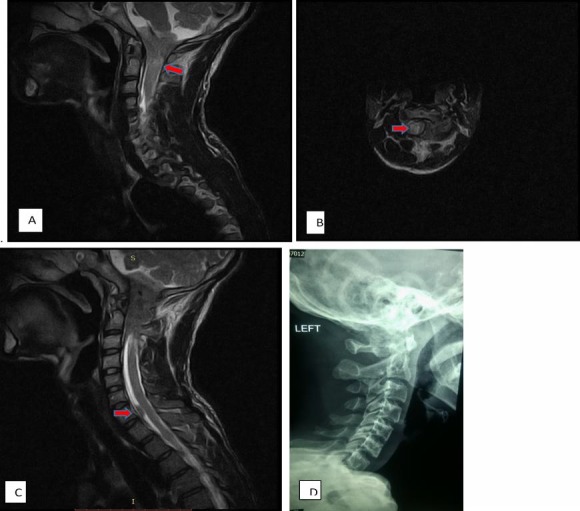
A & B. T2 WI sagittal and axial showing hyperintensity suggestive of cord edema or contusions at C1/ C2 (Red arrows) C. Extramedullary hypointensity suggestive of a bleed at C7 (Red Arrow). D. Lateral Cspine xray showing normal cervical lordosis with no translocation, fractures or subluxation.
CASE 3
A.O. is a 51-year old man who was seen with a 10-week history of neck pain following a choke hold to the neck. There was limitation in neck movement and paraesthesia in the right upper extremity. There was no sphncteric dysfunction nor weakness in any of the limbs. He had defaulted surgery at another facility but presented to us on account of persistent symptoms. He was neurologically well aside from a mild weakness in left shoulder abduction.
The C-Spine X-rays showed 50% anterior subluxation of C4 on C5 with a 60° angulation (Fig 3A). The C-spine MRI revealed a Compression fracture of C5 with 50% anterior subluxation of C4 on C5, moderate cord compression posteriorly, and cord signal intensity change at C3 - C6 (Fig. 3C).
Fig. 3:
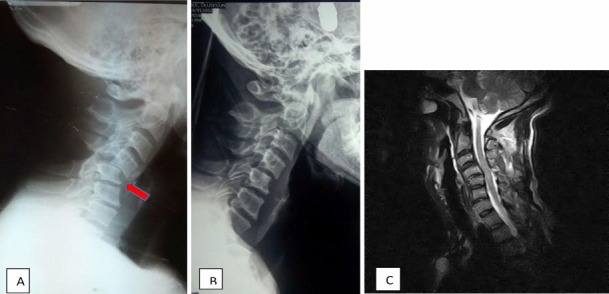
A. Lateral C spine Xray showing 50% anterior subluxation of C4 on C5(Red arrow). B. Post reduction lateral C-spine Xray. The reduction was done with a 40kg weight, after wards the patient was maintained on a 6kg weight for 6weeks. C. T2WI showing evidence of instability at C4/C5 with compression of the cord at the same level and signal cord intensity.
He declined surgery and opted for non-operative care with Gardener- Wells tongs following closed reduction of the subluxed segment (Fig 3B). His pain resolved and he was ambulated after a satisfactory cervical dynamic studies. He remained neurologically intact at discharge.
DISCUSSION
Traumatic spinal cord injury continues to be a major concern globally, due to the associated morbidity, generally affecting the patient's and carer's entire socio-economic life and having a major impact on health care spendings. Whilst there seemingly appear to be a decline in the frequency of road crashes in the developed nations, developing nations such as Nigeria continue to be faced with what appears to be an increase or at best an unchanged prevalence due to the evolution of new aetilogies such as commercial motorcycle accidents and a rather high level of violence predicated on religious, ethnic and political differences.7-10 Thus, reports suggest an increase of SCI in Nigeria in the last decade affecting the young4,11,12. Nigeria has the larger proportion of its populace in the young and middle age group bracket and with an official poverty rate of 57.8% and 70 million people living on less than 1 dollar/ day13. Thus, most of the affected individuals are bread winners of their families resulting in an unquantified economic burden both nationally and for the individual family considering that the average in-hospital cost for non operative care is estimated at $1598.2914 .
One of our three reported cases involving a playful twisting of the neck resulting in a variant of the hemicord (Brown-Sequard) syndrome. This case is peharps comparable to reported cases of spinal cord injury from chiropractic manipulation which may involve a high velocity, low amplitude movement of the neck15. There are few reported cervical cord injuries following chiropractic neck manipulations, including a Brown Sequard syndrome from cord contusion more pronounced on one side or an epidural hematoma16. Our patient had a cord contusion at C1/C2 and a subdural hematoma with the symptomatology being likely secondary to the upper cervical contusion. Brown Sequard syndrome often results from penetrating injury though other causes have also been identified17. We surmise that the progressive neurologic improvement of our patient is likely due to the resolution of the contusion.
It is interesting that the older patient who had a similar injury as the younger patient albeit in a violent way, presented with significant spinal injuries in a background of spondylotic changes but was neurologically intact. A central cord syndrome would not have been unexpected.
The injury in the second case resulted from an accidental near hanging. There was no fracture or translation of the cervical spine suggesting that the neurological deficit may be from cord transection or significant contusion, which we unfortunately could not confirm with an MRI, due to the patient's decision to discharge against medical advice. Cervical spine injures are not common in near hanging situations5,18 as seen in this patient. However he presented with cervical cord injury which is not a common finding5,18. Though injury from hanging is a combination of axial traction putting the mobile cervical spine at risk and external pressure on the neck, the major mechanism of death in non-judicial hangings has been identified as cerebral ishaemia resulting in anoxic encephalopathy from arterial compression19,20. Vascular occlusion is said to be incomplete or of short duration in near hanging5. Upper cervical spine fractures including, the hangman's fracture have been described following judicial hanging21-23. Our patient's hanging was apparently incomplete thus preventing the typical fractures of skull base and lateral mass of C2 and subsequent instability of C2/C3 leading to instanteneous death which is seen in judicial hangings20,24,25.
Thus, while efforts are continually and rightly directed to the prevention of road crashes which constitute the major cause of SCI, there is a need for increasing enlightement campaigns and social advocacy on the other uncommon aetiologies such as those in our report, which to our knowledge have not been reported in our environment. Awareness of the risks of such dangerous habits such as neck-twisting plays and standing on a moving truck in a show of intrepidity, may have prevented these devastating injury particularly in the first case.
CONCLUSION
We have reported unusual causes of cervical cord injury in our environment which were mainly due to dangerous habits with a resultant significant morbidity in one of the patients while the others progressively regained neurological functions.
REFERENCES
- 1.Owosina FOA. Spine injuries in Nigeria Care Inj Proc. First Int Post-graduate Symp West African Coll Surg. 1977. pp. 100–107.
- 2.Ho C, Wuermser L, Priebe M, Chiodo A. Spinal cord injury medicine. Epidemiology and classification. Arch Phys. 2007. [Accessed July 31, 2016]. http://www.sciencedirect.com/science/article/pii/S00039993060 15577 . [DOI] [PubMed]
- 3.Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord. 2014;52(2):110–116. doi: 10.1038/sc.2012.158. [DOI] [PubMed] [Google Scholar]
- 4.Solagberu BA. Spinal cord injuries in Ilorin, Nigeria. [Accessed July 11, 2016];West Afr J Med. 2002 21(3):230–232. doi: 10.4314/wajm.v21i3.28037. http://www.ncbi.nlm.nih.gov/pubmed/12744575 . [DOI] [PubMed] [Google Scholar]
- 5.Nichols S, McCarthy M, Ekeh A. Outcome of cervical near-hanging injuries. J Trauma. 2009. [Accessed August 31, 2017]. http://journals.lww.com/jtrauma/Abstract/ 2009/01000/Outcome_of_Cer vical_Near_ Hanging_Injuries.22.aspx. [DOI] [PubMed]
- 6.Centers for Disease Control and Prevention. National Center for Injury Prevention and Control. Web-based injury statistics query and reporting system. 2004. http://www.cdc.gov/ncipc/ wisqars/default.htm .
- 7.Malomo T, Oyemolade T, Adeleye A. Determinants of timing of presentation of neurotrauma patients to a neurosurgical center in a developing country. J Neurosci Rural Pract. 2018; 9(4):545. doi: 10.4103/jnrp.jnrp_502_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Adejugbagbe AM, Fatiregun AA, Rukewe A, Alonge T. Epidemiology of road traffic crashes among long distance drivers in Ibadan, Nigeria. Afr Health Sci. 2015;15(2):480–488. doi: 10.4314/ahs.v15i2.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ibrahim NA, Ajani AWO, Mustafa IA, et al. Road Traffic Injury in Lagos, Nigeria: Assessing Prehospital Care. Prehosp Disaster Med. 2017;32(4):424–430. doi: 10.1017/S1049023X17006410. [DOI] [PubMed] [Google Scholar]
- 10.Adeolu AA, Abiona TC, Komolafe EO, et al. Epidemiology of neurotrauma in Ife-Ijesha zone of Nigeria. World Neurosurg. 2013;80(3-4):251–254. doi: 10.1016/j.wneu.2012.11.063. [DOI] [PubMed] [Google Scholar]
- 11.Kawu A. Pattern and presentation of spine trauma in Gwagwalada Abuja, Nigeria. Niger J Clin Pract. 2012. [Accessed November 1, 2016]. http://www.ajol.info/index.php/njcp/ article/view/75786 . [DOI] [PubMed]
- 12.Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO. Profile of spinal injuries in Lagos, Nigeria. Spinal Cord. 2009;47(2):134–137. doi: 10.1038/sc.2008.93. [DOI] [PubMed] [Google Scholar]
- 13.Swende T, Sokpo J, Tamen F. Globalization and health: a critical appraisal. Niger J Med. 2008. [Accessed August 31, 2017]. https:/ /www.researchgate.net/profileTerr umun_ Swende/publication/23155702_Globalization _and_Health_A_Critical_Appraisal/links/ 564136d208aeacfd893647dc.pdf . [DOI] [PubMed]
- 14.Kawu AA, Olawepo A, Salami AOO, et al. A cost analysis of conservative management of spinal cord-injured patients in Nigeria. Spinal Cord. 2011;49(11):1134–1137. doi: 10.1038/sc.2011.69. [DOI] [PubMed] [Google Scholar]
- 15.Chakraverty J, Curtis O, Hughes T. Spinal cord injury following chiropractic manipulation to the neck. Acta. 2011. [Accessed August 31, 2017]. http://journals.sagepub.com/doi/abs/10.1258/ar.2011.110281 . [DOI] [PubMed]
- 16.Lipper M, Goldstein J. Brown-S quard syndrome of the cervical spinal cord after chiropractic manipulation. Am J. 1998. [Accessed August 31, 2017]. http://www.ajnr.org/content/ajnr/19/7/1349.full.pdf . [PMC free article] [PubMed]
- 17.Roth EJ, Park T, Pang T, et al. [Accessed September 21, 2017];Fcrr aplegia Traumatic Cervical Brown-Sequard and Brown-Sequard-plus Syndromes: The Spectrum of Presentations and Outcomes. 1991 29:582–589. doi: 10.1038/sc.1991.86. https://s3.amazonaws.com/academia.edu. documents/41942632Traumatic_cer vical_ BrownSequard_and_Bro20160203-1820813iiux6. pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53 UL3AExpires=1506010819&Signature= DutJnQYq65PtdJpDvZyHNLqkt5w%3D&responsecontentdisposition= inline%3Bfilename%3D Traumatic_cer vical_Brown-Sequard_and_ Bro.pdf . [DOI] [PubMed] [Google Scholar]
- 18.Adams N. Near hanging. Emerg Med Australas. 1999. [AccessedSeptember 1, 2017]. http://onlinelibrary.wiley.com/doi/10.1046/j.1442-2026.1999.00314.x/full .
- 19.Iserson K. Strangulation: a review of ligature, manual, and postural neck compression injuries. Ann Emerg Med. 1984. [Accessed September 21, 2017]. http://www.sciencedirect.com/science/article/pii/S0196064484806095 . [DOI] [PubMed]
- 20.Krol L, Wolfe R. The emergency department management of near-hanging victims. J Emerg Med. 1994. [Accessed September 1, 2017]. http://www.sciencedirect.com/science/article/pii/0736467994902682 . [DOI] [PubMed]
- 21.Schneider R, Livingston K, Cave A. Hangman s fracture of the cervical spine. Neurosurg. 1965. [AccessedAugust 31, 2017]. h t t p : / / t h e j n s . o r g / d o i / a b s / 1 0 . 3 1 7 1 / jns.1965.22.2.0141 . [DOI] [PubMed]
- 22.Effendi B, Roy D, Cornish B, Dussault R. Fractures of the ring of the axis. A classification based on the analysis of 131 cases. Bone Jt. 1981. [Accessed August 31, 2017]. http://bjj.boneandjoint.org.uk/content/63-B/3/319.short . [DOI] [PubMed]
- 23.Wallace S, Cohen W, Stern E, Reay D. Judicial hanging: postmortem radiographic, CT, and MR imaging features with autopsy confirmation. Radiology. 1994. [Accessed August 31, 2017]. http://pubs.rsna.org/doi/abs/10.1148/radiology.193.1.8090904 . [DOI] [PubMed]
- 24.James R, Nasmyth-Jones R. The occurrence of cervical fractures in victims of judicial hanging. Forensic Sci Int. 1992. [Accessed September 1, 2017.]. http://www.sciencedirect.com/science/article/pii/0379073892900839 . [DOI] [PubMed]
- 25.Penney D, Stewart A, Parr M. Prognostic outcome indicators following hanging injuries. Resuscitation. 2002. [Accessed September 1, 2017.]. http://www.sciencedirect.com/science/article/pii/S0300957202000503. [DOI] [PubMed]