

Abstract
Background:
Dental caries is a common disease in children, which results in tooth loss if not treated. Children in suburban Nigerian communities have a high unmet treatment need index for caries, due to limited access to dental services.
Objective:
To provide atraumatic restorative treatment (ART) as a field treatment for dental caries and assess the acceptability of this approach to pupils.
Methods:
This is a report of the treatment of dental caries under field conditions among 432 pupils in six primary schools around the Primary Oral Health Clinics (POHC) at Idikan and Igboora, Oyo state, Nigeria. ART restorations were placed on asymptomatic class 1 cavitated carious teeth, were evaluated at six and twelve weeks for intactness and symptoms. Acceptability was assessed by asking the pupils immediately after treatment if they experienced pain/ discomfort while receiving the treatment. Data were analysed using descriptive statistics.
Results:
The mean (SD) age of the participants was 9.2(1.8) years; 222(51.4%) were males. The mean (SD) DMFT/ dmft score were 0.06(0.36) [median (Range): 0.0(6)] and 0.07(0.41) [median (Range): 0.0(4)] respectively. Forty (71.4%) decayed teeth were eligible for ART. At six weeks 27(96.4%) fillings were intact while 1(3.6%) had a defective margin, at twelve weeks 23(82.1%) fillings were retained and 1(3.6%) had dislodged. All participants reported no pain during treatment and found the approach acceptable.
Conclusion:
ART fillings were intact in 27(96.4%) and 23(82.1%) at 6 and 12weeks respectively. The provision of ART within a familiar environment is an acceptable method of caries treatment in underserved schoolchildren.
Keywords: Field treatment, dental caries, Atraumatic restorative treatment.
INTRODUCTION
Dental caries is a multifactorial disease initiated by the bacterial biofilm (dental plaque) that covers the tooth surface.1 It is a dynamic process, with periods of demineralization and remineralization of tooth structure, caused by microbial metabolism at the tooth surface.2 If demineralization exceeds remineralization, a preclinical, subsurface carious lesion becomes a frank clinical cavity characterized by a breakdown of surface enamel and extension of the decay into the dentine.3 This leads to sensitivity and pain on exposure to stimuli such as cold foods and drinks. At this stage of the cavity formation, simple dental fillings would prevent further tooth damage and the need for complex treatment regimen or eventual loss of the affected tooth. Dental caries affects both deciduous and permanent teeth and has a worldwide distribution2. Studies from Nigeria reveal a prevalence between 14% and 46.9%.4,5
Children from suburban communities in Nigeria have been shown to have a high unmet need index for caries.4,6 Untreated dental caries leads to serious conditions such as dentoalveolar and facial space abscesses such as Ludwig's angina. These abscesses when not promptly recognized and treated can be complicated by osteomyelitis, cavernous sinus thrombosis, necrotizing cervico-facial fasciitis and even death.7,8 Therefore, prevention of dental caries is very important, however, early diagnosis and prompt treatment of the lesions are required in order to prevent the aforementioned complications. This can be achieved when patient presents early for dental care and check-ups. But it has been shown that there is a low utilization of dental services among children from sub-urban communities,9,10 attributed to low oral health awareness, high cost of dental services where available and fear of dental treatment.11 These factors amongst others led to the rapid growth and promotion of Atraumatic Restorative Treatment (ART) as a minimal intervention technique for the treatment and prevention of dental caries.12 It involves the use of hand instruments only for the removal of carious lesions, followed by preparation and restoration of the cavity and its adjacent pits and fissures with an adhesive material such as high viscosity Glass Ionomer Cement (GIC).13,14
ART technique, introduced into dentistry in the late 1980s, has been noted to be useful in the treatment and prevention of dental caries in areas where conventional treatment cannot be applied, especially in low socio-economic communities, and areas far from modern dental facilities.14-16 ART approach presents numerous advantages such as no need for local anaesthesia and a dental drill; thus acceptable to children, young adults and patients with dental phobia.17
The field conditions in which ART can be performed include schools, refugee camps, orphanage homes as well as Community Dental Health Outreach (CODEH) programmes. ART carried out within these environments, provides children the opportunity to receive an effective dental treatment which is also affordable. Studies have evaluated ART in different field settings and found to be an acceptable and effective method of treatment of dental caries, with high proportion of retention of the fillings.16,17,18 However, evaluation of this form of secondary prevention of dental caries as one of the major of activities of Community Dentistry unit, Department of Periodontology and Community Dentistry, University of Ibadan is sparse. In addition, documentation on this evaluation is also scarce in many regions of Nigeria. We therefore aimed to descriptively report the provision of ART as a treatment for dental caries and its acceptability among primary school pupils in two suburban communities.
METHODS
The Primary Oral Health Clinics (POHC) in Idikan and Igboora are dental clinics set up with the aim of providing dental services to the underserved at the grass root level. These clinics are run by the Community Dentistry unit, University College Hospital/ University of Ibadan, undergraduate and postgraduate students are provided with the required skills in these clinics. Therefore, resident doctors at the part one level rotate through the Department of Periodontology and Community Dentistry for a three-month period to further gain experience in clinical and field skills as an addition to their training. The POHC Idikan, is located in an inner city area in Ibadan North East Local Government Area (LGA) and has a population of 15,042 while the POHC Igboora is situated in a rural town in Ibarapa Central LGA of Oyo state with a population of 103, 243.19
Six (6) primary schools within the community of the POHCs were conveniently selected based on their proximity to the POHCS; three from Idikan and three from Igboora. Permission was sought for and obtained from the school authorities to carry out oral health education and oral screening exercise for all the pupils and treatment for pupils with dental caries who met the eligibility criteria. A consent letter to parents/ guardians requesting participation of the children in the oral screening exercise was given to all the pupils. Only pupils who returned a signed consent letter were screened.
During the screening exercise, the pupils were seated comfortably on a chair, in a well lit classroom. Oral examination was performed by the residents using a sterile wooden tongue depressor. The presence of a class 1 carious lesion that was cavitated but asymptomatic and was large enough to admit a small excavator (0.9mm) meant that such teeth could benefit from the placement of ART. Another consent letter explaining in details the treatment protocol including cost of treatment (#500, an equivalent of $1.7) was given to pupils who met the inclusion criteria for ART to give to their parents/ guardians to consent to allow them receive the treatment on a later date. Pupils who had other dental problems such as carious lesions associated with tenderness to percussion or obvious pulpal exposures, gingivitis, fractured teeth, mobile deciduous teeth, interproximal caries or inaccessibility of occlusal caries to hand instruments were given referral letters to the POHCs to obtain treatment. Only pupils who returned signed consent and assented to the treatment received the ART treatment. Those whose parents were not literate had correspondence with the teachers, who further explained to them the details of the treatment approach. The treatment was performed in the school sick bay, school hall or in an ambulance provided by the local government authority (as was the case in Igboora).
The ART approach was carried out by three (3) trained dental resident doctors during a Community Dentistry posting. In each school, a teacher was in attendance during the treatment and younger pupils (Primary 1 and 2) watched older pupils (Primary 3-6) receive treatment as a form of modeling. The socio-demographic characteristics of the pupils such as age, class and gender were noted on a data collection sheet which included; age, class, gender from the participants and caries experience using DMFT/ dmft index. Standard infection control measures were followed, with a facemask, gloves and bib used for each pupil. The ART procedure was done with the pupil lying comfortably on a provided bed/ bench. The operator sat towards the head of the child on a provided plastic chair or bench. Natural light or a headlamp worn by the operator was the source of light used during the procedure. While isolating with cotton rolls, excavation of the carious lesion and shaping of the cavity was done using sterile hand instruments without the use of local anesthesia. The cavity was then irrigated and dried using cotton pellets, this was followed by conditioning for 15-20 seconds with GIC dentine conditioner (Kavitan, Spofa dental, Sybron Dental specialties Markova 238 506 46 Jicin, Czech Republic). Thereafter, the cavity was washed with a wet cotton pellet and then dried with dry cotton pellets. High strength GIC powder and liquid (Kavitan Plus, Spofa dental, Sybron Dental specialties Markova 238 506 46 Jicin, Czech Republic, Batch no 2214954) were mixed to a thick, even consistency according to manufacturer's instructions and placed into the prepared cavity. Petroleum jelly was placed to the gloved finger and then pressure applied on the GIC cement mix before it sets to express some of it to adjacent pits and fissures.12 Excess GIC cement on the occlusal margins of the tooth was removed with a carver. The GIC fillings were checked for high spots by asking the pupils to gently occlude the upper and lower teeth. If a child responded as to biting on a hard object, an articulating paper was placed on the teeth to confirm the high spot which was then removed with a carver. After the GIC filling was adequately placed, the pupils were given post-operative instructions, which included no food or drinks for 30 minutes of placing the filling.
The GIC fillings were reassessed after 24 hours and one week, the schools were revisited and the pupils re-evaluated at six and twelve weeks. The treated teeth were assessed for tenderness to percussion, retention and defective margins. In addition, periodontal complications were assessed using visual and clinical assessment to determine periodontal health status with sterile mouth mirror and caries explorer. Acceptability of the approach was assessed from both pupils and teachers. The pupils were asked for presence of pain/discomfort while receiving treatment and at follow up; willingness to receive a similar procedure in future and recommend same to others. The opinion of the teachers regarding the treatment approach, its cost, convenience and willingness to recommend same to others was also sought.
All data were computed using SPSS version 20 software and descriptive statistics were generated. Means and standard deviation were used to summarize numeric variables such as age and DMFT/dmft scores for permanent and primary teeth respectively. Frequencies and percentages were used for qualitative variables such as gender and status of the ART filling at review.
RESULTS
A total of 432 pupils from the 6 conveniently selected schools who returned a signed consent form were screened. They consisted of 222(51.4%) males and 210(48.6%) females. Their age range was from 5-13 years with a mean (±SD) age of 9.2(±1.8) years. The presence of dental caries was observed among 26(6.0%) pupils, 14(3.2%) males and 12(2.8%) females. The mean DMFT score was 0.06(±0.36) [median (Range): 0.0(6)], while the mean dmft score was 0.07(±0.41) [median (Range): 0.0(4)]. Decayed component accounted for 100% of the DMFT/dmft score as shown in Table 1. There were no filled teeth nor teeth extracted due to caries.
Table 1:
Distribution of dental caries among the participants
| Decayed, missing and filled teeth scores (DMFT/ dmft) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Permanent teeth | Primary teeth | |||||||
| Decayed | Missing | Filled | DMFT | Decayed | missing | filled | dmft | |
| (D) | M | F | (d) | (m) | (f) | |||
| 26 | 0 | 0 | 26 | 30 | 0 | 0 | 30 | |
| Mean (±SD) DMFT: 0.06(±0.36) | Mean (±SD) dmft: 0.07(±0.41) | |||||||
| Median (Range) DMFT: 0.0(6) | Median (Range) dmft: 0.0(4) | |||||||
A total of 56 teeth in the oral cavity of 26 pupils had dental caries of which 30(53.6%) were primary teeth while 26(46.4%) were permanent teeth. Forty (71.4%) of the decayed teeth were non symptomatic and would benefit from placement of an ART restoration while 16(28.6%) were complicated carious lesions that could no longer benefit from ART. Out of the 26 pupils slated for placement of ARTs, 20(76.9%) of them returned the signed consent forms (second consent form given to pupils eligible for treatment to allow for treatment of carious lesions). A total of 28 fillings were placed; 17(60.7%) on primary teeth and 11(39.3%) on permanent teeth.
At six weeks review, 27(96.4%) of the fillings were intact with 1(3.6%) filling having a defective margin, while at twelve weeks, 23(82.1%) of the fillings were still intact (Figures 1 and 2). All 20(100.0%) the pupils who received ARTs reported not having felt pain and they also turned up for the recall visits. They were willing to receive the treatment again if and when necessary, and would recommend similar treatment to others. All the teachers of the visited schools thought the concept was very good and considered the treatment approach convenient as it afforded the children treatment while their parents went about their normal business activities. One of the proprietors/ head teachers hoped the treatment could be carried out free of charge next time. The other 5 considered the treatment cost adequate. All the head teachers were willing to recommend same treatment to others.
Fig. 1:
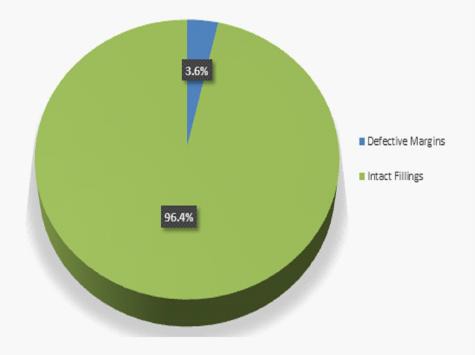
Distribution of GIC fillings of participants retained at 6 weeks
Fig. 2:
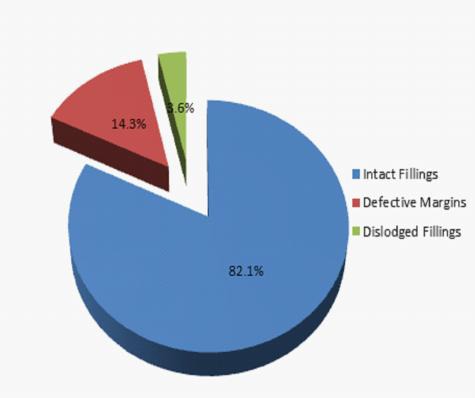
Distribution of GIC fillings of participants at 12 weeks
DISCUSSION
The prevalence of dental caries seen among the pupils during this exercise was lower (13.9%) than that reported among children in another suburban area in south west Nigeria.7 The limited number of pupils involved in this report may be responsible for this, as only schools within the locality of the Primary Oral Health Center were visited by the dentists. There was an almost even distribution of the carious lesions among male and female pupils and this is similar to findings from earlier studies.6
The decayed (D/d) component of the DMFT/dmft index was similar to findings from other studies conducted in Nigeria.8,20 further confirming a high treatment need index for dental caries among children in this environment. It also reflects poor utilization of oral health care services despite the presence of a primary oral health care facility within the locality. Factors responsible for this may include low priority placed on oral health as well as low level of oral health awareness.11 The effort of the Community Dentistry unit to take oral health care to the door steps of people is a giant step to reduce the high unmet need that exists among the populace.
Findings from this report indicate that the percentage of GIC fillings retained, though evaluated on a short term, is comparable to that observed in a short term study carried out in field conditions in rural Turkey.21 In that study, 89.8% of GIC fillings remained intact after 6 months, while in our finding, 82% of GIC fillings were intact at the end of 3 months. This value is also similar to that reported by Ibiyemi et al in an earlier study22 but unlike this report, the study by Ibiyemi et al was carried out within a clinic setting and observation was for much longer. We recommend further studies on long term success of this treatment in field conditions.
The ART treatment approach was acceptable to the pupils and is similar to what was reported in another school in a study carried out among Chinese primary school pupils23. The positive response of the participants may be due to the fact that the treatment given to the pupils was carried out within a familiar zone, which is less threatening compared to the unfamiliar environment of a dental clinic. Also the absence of pain during treatment may have contributed to their favorable response.
The teachers also found the treatment approach acceptable and convenient similar to that reported in a study23. Treating children within the school environment prevents loss of man hours that occurs when parents take children for treatment at the regular dental clinic. Furthermore, the average fee for such treatment at the government dental clinic is about ₦3000 and excludes cost of transportation to the clinic as well as registration fees. Thus, the cost of treatment at ₦500 (an equivalent of $1.7) is highly subsidized and therefore attractive to the teachers who most often are also parents. The request by one proprietor to have the treatment carried out at no extra cost to the pupils/parents suggests that efforts from government agencies and donor agencies can be harnessed to incorporate school dental health and treatments into the current school curriculum for improved general and oral health of the Nigerian child.
ART placed in a field condition can serve as a means of treatment and prevention of dental caries among children in underserved communities. Literature on ART use in field conditions is scarce in this environment, so adequate comparison with other studies could not be done. With increase in its use under similar situations, studies with larger number of participants and longer observation periods may be necessary to validate the retention of ART placed under field conditions.
CONCLUSION
ART provided for primary school pupils under field conditions remained intact in 27(96.4%) of the pupils at 6 weeks and 23(82.1%) at 12 weeks. The approach was acceptable to the pupils who received the treatment, their teachers also found the method of treatment satisfactory.
REFERENCES
- 1.Frazao P. Epidemiology of dental caries: when structure and context matter. Braz Oral Res. 2012;26.Spec(1):108–114. doi: 10.1590/s1806-83242012000700016. [DOI] [PubMed] [Google Scholar]
- 2.Parker E, Jamieson L, Broughton J, Albino J, Lawrence H, Roberts-Thomson K. The oral health of indigenous children: A review of four nations. J Paediatr Child Health. 2010;46:483–486. doi: 10.1111/j.1440-1754.2010.01847.x. [DOI] [PubMed] [Google Scholar]
- 3.Moreira R. Virdi PM, editor. Epidemiology of dental caries in the world, oral health care - Pediatric, Research, Epidemiology and Clinical Practices. 2012.
- 4.Oziegbe EO, Esan TA. Prevalence and clinical consequences of untreated dental caries using PUFA index in suburban Nigerian school children. Eur Arch Paediatr Dent. 2013;14(4):227–231. doi: 10.1007/s40368-013-0052-5. [DOI] [PubMed] [Google Scholar]
- 5.Popoola BO, Denloye OO, Iyun OI. Influence of parental socioeconomic status on caries prevalence among children seen at the University College Hospital, Ibadan. Ann Ibadan Postgrad Med. 2013;11(2):81–86. [PMC free article] [PubMed] [Google Scholar]
- 6.Denloye O, Ajayi D, Bankole O. A study of dental caries prevalence in 12-14 year old school children in Ibadan, Nigeria. Pediatr Dent J. 2005;15(2):147–151. [Google Scholar]
- 7.Adekoya-Sofowora CA, Nasir WO, Oginni AO, Taiwo M. Dental caries in 12-year-old suburban Nigerian school children. Afr Health Sci. 2006;6(3):145–150. doi: 10.5555/afhs.2006.6.3.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Okoye L, Ekwueme O. Prevalence of dental caries in a Nigerian rural community: a preliminary local sur vey. Ann Med Health Sci Res. 2011;1(2):187–195. [PMC free article] [PubMed] [Google Scholar]
- 9.Akpata E. Textbook of Operative dentistry. 1st ed. Class Publishing; London: 1997. [Google Scholar]
- 10.Azodo CC, Chukwumah NM, Ezeja EB. Dentoalveolar abscess among children attending a dental clinic in Nigeria. Odontostomatol Trop. 2012;35(139):41–46. [PubMed] [Google Scholar]
- 11.Sofola O. Implication of low oral health awareness in Nigeria. Niger Med J. 2010;51(3):131–133. [Google Scholar]
- 12.Holmgren CJ, Roux D, Domejean S. Minimal inter vention dentistr y Part 5: Atraumatic restorative treatment (ART) a minimum intervention and minimally invasive approach for the management of dental caries. Br Dent J. 2013;214(1):11–8. doi: 10.1038/sj.bdj.2012.1175. [DOI] [PubMed] [Google Scholar]
- 13.Frencken JE, Leal SC. The correct use of the ART approach. J Appl Oral Sci. 2010;18(1):1–4. doi: 10.1590/S1678-77572010000100002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic restorative treatment (ART): Rationale, technique, and development. J Public Health Dent. 1996;56(3):135–140. doi: 10.1111/j.1752-7325.1996.tb02423.x. [DOI] [PubMed] [Google Scholar]
- 15.Mjor IA, Gordan V V. A review of atraumatic restorative treatment (ART) Int Dent J. 1999;49(3):127–131. doi: 10.1002/j.1875-595x.1999.tb00896.x. [DOI] [PubMed] [Google Scholar]
- 16.Smales RJ, Hak-Kong Y. The atraumatic restorative treatment (ART) approach for the management of dental caries. Quintessence Int. 2002;33(6):427–432. [PubMed] [Google Scholar]
- 17.Holmgren CJ, Lo ECM, Hu D. Glass ionomer ART sealants in Chinese school children—6-year results. J Dent. 2013;41(9):764–770. doi: 10.1016/j.jdent.2013.06.013. [DOI] [PubMed] [Google Scholar]
- 18.Frencken JE, Makoni F, Sithole WD. ART restorations and glass ionomer sealants in Zimbabwe: survival after 3 years. Community Dent Oral Epidemiol. 1998;26(6):372–381. doi: 10.1111/j.1600-0528.1998.tb01975.x. [DOI] [PubMed] [Google Scholar]
- 19.Nigeria Populations Commission. Population and Housing Census Priority Table Volume III. Abuja; 2010. 2006 .
- 20.Agbelusi GA, Jeboda SO. Oral health status of 12-year-old Nigerian children. West Afr J Med. 2006;25(3):195–198. doi: 10.4314/wajm.v25i3.28277. [DOI] [PubMed] [Google Scholar]
- 21.Dülgergil ÇT, Soyman M, Civelek A. Atraumatic restorative treatment with resin-modified glass ionomer material: Short-term results of a pilot study. Med Princ Pr. 2005;14:277–280. doi: 10.1159/000085750. [DOI] [PubMed] [Google Scholar]
- 22.Ibiyemi O, Bankole OO, Oke GA. Survival rates of two atraumatic restorative treatment (ART) types in occlusal carious permanent teeth after two years. Afr J Med Med Sci. 2011 Jun;40(2):127–134. [PubMed] [Google Scholar]
- 23.Lo EC, Holmgren CJ. Provision of atraumatic restorative treatment (ART) restorations to Chinese pre-school children - a 30-month evaluation. Int J Paediatr Dent. 2001;11(1):3–10. doi: 10.1046/j.1365-263x.2001.00232.x. [DOI] [PubMed] [Google Scholar]