

Abstract
Background: Leptomeningeal disease (LMD), also known as neoplastic meningitis, leptomeningeal carcinomatosis, or carcinomatous meningitis, is a rare cancer complication occurring in ~5% of cases and ultimately leads to significant morbidity and mortality. In the modern era, incidence of this condition continues to rise with longer survival of patients with advanced and even metastatic disease due to continued improvements in systemic therapies that are providing prolonged control of distant disease, but with limited effect in the central nervous system (CNS). Typical treatment strategies include optimal systemic therapy for the primary disease, as well as neuroaxis directed therapies, which may include intrathecal chemotherapy (ITC) or radiotherapy (RT).
Methods: A systematic review of radiotherapy for LMD was performed. Medline, EMBASE, and Cochrane databases were searched from 1946 to 2018 for clinical trials, retrospective/prospective reviews, and case series with ≥2 human subjects that used radiation therapy techniques in the treatment of LMD. The outcome measures of interest included: characteristics of trial participants, inclusion/exclusion criteria, study type, number of participants, primary cancer histology, type of intervention for LMD, survival results if reported, length of follow up, and study conclusion.
Results: Of 547 unique citations, 62 studies met the pre-specified eligibility criteria. These studies included 36 retrospective cohorts, 11 prospective series, 12 case series, and a single citation of guidelines, NCDB analysis, and a randomized control trial. Owing to study heterogeneity, meta-analyses of the endpoint data could not be performed.
Conclusions: LMD is a devastating complication of cancer with reported survivals ranging from 2 to 4 months. Based on this systematic review, the recommendation for the treatment of LMD is for multimodality discussion of cases and treatment, including the use of radiotherapy, for LMD. However, with continued advances in systemic therapy as well as imaging advances, the landscape of LMD is evolving rapidly and the role of RT will likely also continue to evolve and advance. There is limited high-quality evidence to guide the optimal use of RT for the treatment of LMD, and there is a great need for prospective, histology specific investigation of the role of radiotherapy for LMD in the era of modern systemic therapies.
Keywords: leptomeningeal disease, leptomeningeal carcinomatosis, radiation, neoplastic meningitis, carcinomatous meningitis, systematic (literature) review
Introduction
Rationale
Leptomeningeal disease (LMD), also known as neoplastic meningitis, leptomeningeal carcinomatosis, or carcinomatous meningitis, is a rare cancer complication in which malignant cells infiltrate the layers of the central nervous system (CNS), known as meninges, and lead to significant morbidity and mortality. This disorder was first diagnosed in 1870, by Eberth et al. and was noted to be a rare complication of malignancy as it was uncommonly diagnosed before death (1). Today, it is known that this condition occurs in ~5% of all cancer patients, presenting most commonly in primary diagnoses of breast cancer (41%), lung cancer (24%), gastrointestinal tract malignancies (13%), and melanoma (12%) (2–4). However, incidence continues to rise with continuous improvements in systemic therapies that allow patients diagnosed with cancer to live longer, as well as improvements in both technology and availability of imaging of the neuroaxis leading to continued increases in the detection and diagnosis of LMD (3).
The anatomy of the neuroaxis consists of the brain and spinal cord, covered by the meninges, which are comprised of dura mater, arachnoid membrane, and pia mater. The leptomeninges refers to the two most inner layers, arachnoid membrane and pia matter, including the subarachnoid space, which separates these two sheets, and is the location of the cerebrospinal fluid (CSF). The CSF is the location of circulating tumor cells in patients with LMD. The pathogenesis of LMD is multifaceted, and can include direct extension from pre-existing CNS tumors or systemic tumors that follow peripheral nerves into the subarachnoid space, as well as infiltration through hematogenous dissemination, or even seeding of the subarachnoid space during surgical procedures (3, 5–8). Once malignant cells gain access to the CSF, they can spread along the meningeal surface by direct extension and be carried by the CSF flow and form new metastatic deposits in other locations.
The clinical presentation of LMD can be widely variable with signs and symptoms of increased intracranial pressure, cranial nerve palsies, radiculopathies, or other focal neurologic deficits, seizures, changes in brain metabolism, or encephalopathy (9–12). A subset of patients present asymptomatic with an incidental imaging finding. Commonly, patients may report a headache or worsening back or radicular pain, as well as signs and symptoms that suggest involvement of multiple anatomic neurologic sites, including: incontinence, lower motor neuron weakness, and sensory abnormalities. In addition to clinical suspicion and signs of LMD on imaging, the most informative diagnostic study is evaluation of the CSF from a lumbar puncture. The opening pressure, cytology, cell count, and measurements of protein and glucose should be performed (13). However, normal lumbar puncture (LP) studies have been reported in 5% of confirmed LMD cases, and, therefore, the requirement of a positive LP is not necessary for diagnosis (14, 15).
Standard treatments for LMD include neuroaxis directed therapies in addition to optimal systemic therapy for the primary and extra-CNS disease. These treatments may include intrathecal chemotherapy (ITC) to target microscopic tumor on the surfaces of the leptomeninges and cells floating in the CSF to prevent further seeding. Radiotherapy (RT) is also commonly used either focally to treat symptomatic sites and areas of bulky disease that will be unlikely to be adequately treated with chemotherapy or in some settings to treat the entire neuroaxis.
Objectives
Regardless of systemic and local control of the primary disease, prognosis in the setting of LMD is very poor, with reported average survivals of ~2–4 months, even with treatment (16–19). There are currently no standardized guidelines for the treatment of LMD, and many clinicians are hesitant to treat patients with clinically advanced neoplastic meningitis given the high risk of toxicity and unknown value of treatment. Furthermore, in the modern era of immunotherapy, it is unclear if the incidence or prevalence of LMD is increasing.
Research Question
Therefore, the objective of this systematic review was to examine the outcomes of the use of RT to treat LMD from any primary cancer histology. We reviewed clinical trials, retrospective reviews, and case series with ≥2 subjects that utilized radiation therapy techniques in the treatment of LMD, and report our findings below.
Methods
Study Design
The present systematic review was designed to evaluate the published evidence underlying the use of RT treatment for LMD.
Participants, Interventions, Comparators
The Population Intervention Comparator Outcome Study (PICOS) design framework was used to structure the research question for the review and the corresponding published data search. The population of interest included patients of any age with a diagnosis of LMD who had RT as a part of their treatment regimen once LMD was diagnosed. No restrictions in terms of age, comorbidities, previous treatment received, or method of diagnosis were used. Patients must have received RT as a part of their LMD treatment, but were allowed to receive any other treatment in addition to RT. All doses, preparations, and frequencies of administration were considered. The primary outcome of interest was overall survival (OS). All study types were permitted, including randomized and non-randomized interventional studies, observational studies, and case series with ≥2 human subjects. Only studies with full articles published in English, or with an English translation were considered.
Systematic Review Protocol
The report documenting our systemic review as prepared in consultation with the Preferred Reporting Items for Systemic Review and Meta-Analysis (PRISMA) statement for systematic review and meta-analyses (20).
Search Strategy
An information specialist (G.P.) designed and executed an electronic data search to seek relevant citations for the present systematic review from Medline (1946-present), EMBASE (1947-present), and Cochrane (all years) databases. The last search was completed on 7/30/2018. The following search terms to search all trials registers and databases were used: randomized controlled trial (RCT), controlled clinical trial, leptomeningeal carcinomatosis, leptomeningeal metastasis, neoplastic meningitis, meningeal metastasis, meningeal carcinomatosis, radiation therapy, radiotherapy, radiation. A full summary of the search strategies used is provided in Supplementary Appendices 1–3.
Data Sources, Studies Sections, and Data Extraction
Stage 1 screening consisted of an independent review of the titles and abstracts by two reviewers (S.B., and C.C.). Discrepancies between studies identified as potentially eligible were reconciled between the two reviewers by consensus. Stage 2 screening consisted of an independent, full-text review of all potentially relevant articles by two reviewers. Data collection of the final articles was performed by reviewer S.B. using a standardized data extraction template. The following information was collected: characteristics of trial participants that had LMD, the trials inclusion/exclusion criteria, study type (retrospective, prospective, randomized controlled trial), number of participants treated with RT for LMD, primary cancer histology, type of intervention, survival results if reported, length of follow up, and study conclusion.
Data Analysis
Due to limitations in the available data, the number of prospective series and randomized controlled trials, and variation in treatments and outcome reporting, it was not possible to perform a detailed meta-analysis. A descriptive approach to summarizing the data was therefore used.
Results
Available Evidence
A consort diagram of the study selection process is shown in Figure 1. The search of Medline, EMBASE, and Cochrane provided a total of 716 citations; 18 additional citations were identified through other sources including Google and Pubmed. After adjusting for duplicates, 547 citations were reviewed, of which 400 studies were discarded for the following reasons: 253 studies did not include the words or variations of the words: “radiation” or “leptomeningeal disease” in the title or abstract, and thus they were deemed unlikely to be the focus of the publications, 2 citations had no traceable abstract or full text available, and 20 manuscripts reported on only 1 patient with LMD treated with RT. Of the remaining citations, 115 citations did not evaluate the use of RT treatment for LMD and 10 citations excluded patients with LMD and therefore, these 125 citations were excluded. An additional 147 full text articles were subsequently reviewed for inclusion. Of these, 85 were excluded for the following reasons: 12 citations did not have a full text available in English or an English translation; four full texts were found to have a single patient treated with RT for their LMD, thus not meeting inclusion criteria; 16 citations did not evaluate the use of RT to treat LMD; four citations excluded patients with LMD from their study; 43 manuscripts did not report the outcomes of patients with LMD treated with RT; and finally, six studies did not include any details of the RT treatment, and were excluded. Therefore, a total of 62 studies met inclusion criteria and were included in the systematic review.
Figure 1.

Flow diagram of study selection. N, number of studies; LMD, leptomeningeal disease or other variations of the term; RT, radiation therapy.
Study Selection and Characteristics
The included studies were first categorized according to the primary histology included, and then by the type of study (randomized, observational [retrospective review, prospective review, and case series], guidelines, NCDB analyses, and practice patterns). The results of the following histologies are detailed, below: mixed, breast cancer, non-small cell lung cancer, gastrointestinal (GI) cancer, adult central nervous system (CNS) gliomas, melanoma, leukemia/lymphoma, gynecologic cancer, esthesioneuroblastoma, pediatric CNS disease, and pediatric rhabdomyosarcoma.
Synthesized Findings by Histology
Mixed Histologies
A total of 19 studies reported on patients with LMD from a mix of histologies (Table 1) (15, 17, 21–36, 38). Eighteen of these studies were observational in nature and included patients with breast (n = 375), melanoma (n = 68), lung (n = 469), bladder (n = 2), prostate (n = 1), ovarian (n = 3), solid tumors not otherwise specified (NOS; n = 59), gastrointestinal NOS (n = 12), colon (n = 2), gastric (n = 12), kidney (n = 2), adult brain tumors (n = 51), unknown primary (n = 69), leukemia/lymphoma (n = 111), and pediatric brain tumors (n = 6). The median age of these patients ranged from 13 to 65 years. Patients were treated with any combination of whole brain radiotherapy (WBRT), craniospinal irradiation (CSI), focal brain RT (FBRT; fractionated or stereotactic radiosurgery [SRS]), focal spine radiotherapy (FSRT), intrathecal chemotherapy (ITC), intraventricular radioisotope, systemic chemotherapy (C), and best supportive care (BSC). Reported OS for the cohorts ranged from 1.4 to 10 months. Additionally, Coakham et al. reported their use of I-131 radiolabeled monoclonal antibodies to treat neoplastic meningitis in pediatric and adult patients between 1984 and 1993 and reported a mean survival of 39 months in therapy responders and 4 months in non-responders (35). These results are sufficiently encouraging to stimulate further attempts at cerebrospinal fluid therapy with I-131 monoclonal antibodies; however, since this time, there is very little reported use of this technique in the treatment of LMD in the literature. Overall, the included studies involving mixed histologies leading to LMD reported a variety of conclusions, with an overall consensus that any treatment had a lower risk of death than supportive care alone. Patients who were able to complete a course of WBRT lived longer, and those who received combined modality treatment had the longest survival.
Table 1.
Mixed histologies: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Passarin et al. (21) | Obs | 50 | 2005–2010 | 50 | 48% BSC; 22% C; 6% ITC; 20% RT; 4% combined | 1.4 |
|
| Gani et al. (22) | Obs | 27 | 2004–2010 | 57 | 100% WBRT | 2 |
|
| Brower et al. (23) | Obs | 124 | 1999–2014 | 52 | 47.2% WBRT; 31.4% C; 7.4% ITC | 2.3 |
|
| Clarke et al. (24) | Obs | 187 | 2002–2004 | 56.4 | 55% RT; 29% ITC; 18% C; 21% BSC | 2.4 |
|
| Oechsle et al. (25) | Obs | 135 | 1989–2005 | 54 | 28% C+IT C; 22% ITC; 12% RT + ITC; 7% other; 13% BSC | 2.5 |
|
| Kwon et al. (26) | Obs | 80 | 2004–2011 | 54 | 90% ITC; 70.9% WBRT; 17.5% FSRT | 2.7 |
|
| Hermann et al. (17) | Obs | 16 | 1995–2000 | 46 | 100% CSI | 3 |
|
| Sause et al. (27) | Obs | 26 | 1981–1985 | 54 | IT C + WBRT | 3.1 |
|
| Chamberlain et al. (28) | Obs | 40 | 1986–1995 | 56.5 | 55% WBRT; 17.5% FSRT | 4 |
|
| Herrlinger et al. (29) | Obs | 155 | 1980–2002 | 53 | 10% RT; 32% C; 31% RT+C; 17% BSC | 4.8 |
|
| Wasserstrom et al. (15) | Obs | 90 | 1975–1980 | NR | 73% RT; 100% ITC | 5.8 |
|
| Chamberlain et al. (30) | Obs | 15 | 1987–1994 | 13 | 100% C and ITC; 60% RT | 6 |
|
| Sakaguchi et al. (31) | Obs | 206 | 2000–2015 | 65 | 100% WBRT; 8% surgery | 6 |
|
| Pan et al. (32) | Obs | 59 | 2010–2014 | 55 | 50% ITC+WBRT; 86% WBRT; 34% FSRT; 25% WBRT+FSRT; 71% BSC | 6.5 |
|
| Bokstein et al. (33) | Obs | 104 | 1998 | 52 | 40%WBRT; 12% FSRT; 14% WBRT+FSRT; 6% CSI;4% C | 7 |
|
| Wolf et al. (34) | Obs | 32 | 2013–2015 | 62 | 100% SRS | 10 |
|
| Coakham et al. (35) | Obs | 7 | 1984–1993 | 42 | 100% I-131 MAb | Mean survival responders: 39; non-responders :4 |
|
| Du et al. (36) | Obs | 46 | 2008–2011 | 53 | 26% BSC; 57% C; 47% RT; 11% ITC | 4.4 |
|
| Hyun et al. (37) | NCDB | 519 | 2005–2014 | 56 | 28% BSC; 45% C; 10% RT; 17% C+RT | 5 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT; MAb, monoclonal antibody; Tx, treatment; PS, performance status; dz, disease; SRS, stereotactic radiosurgery; TKI, tyrosine kinase inhibitor.
A National Cancer Database (NCDB) analysis reported the results of patients treated for LMD from any histology from 2005 to 2014. Patients were diagnosed with lung cancer (n = 334), breast cancer (n = 96), GI cancer NOS (n = 39), leukemia/lymphoma (n = 19), and unknown primary (n = 3). Of the cohort, 52 patients were treated with RT alone, 88 patients were treated with RT+C, 232 patients were treated with C alone, and 147 patients were treated with BSC. Of the patient's that received RT, 85% were treated with WBRT, 14% with focal brain RT (FBRT), and 1% with WBRT and focal spine RT (FSRT). Median OS for the entire cohort was 3 months (2.7–3.3 months). Treated patients exhibited a higher median OS compared to BSC; and patients treated with C+RT revealed the highest median OS of 5 months (3.5–6.5 months) followed by patients treated with RT alone who had a median OS of 3 months (1.7–4.3 months). The authors concluded that patients with LMD have poor outcomes overall, but those who had a good performance status and normal CSF levels had a more favorable prognosis upon active treatment (37).
Breast Cancer
Nine studies meeting inclusion criteria included patients with a primary histology of breast cancer (Table 2) (39–48). Of these, 7 studies reported outcomes of observational studies, and a single study reported the results of guideline recommendations, and a randomized controlled trial. The observational studies included a total of 764 patients treated with RT for LMD in sample sizes ranging from 8 to 187 per study. These patients were treated from 1986 to 2015 and ranged in age from 23 to 80 years. Patients were treated with WBRT (n = 243), FSRT (n = 47), C (n = 220), ITC (n = 434), or BSC (n = 20), with multiple patients receiving combinations of these treatments; however, exact numbers were not reported. The OS for patients treated on these studies ranged from 3.8 to 7.5 months. Longer survival was associated with hormone receptor positive tumors, limited prior therapy for systemic disease, and LMD as the site of first metastasis, with mixed conclusions on the impact of improvement when RT is added to C/ITC. A positive correlation was noted between improved quality of life and treatment with RT in the single study that evaluated this endpoint (44). Any treatment was associated with longer survival when compared to BSC alone. Interestingly, a high burden of disease at the time of LMD diagnosis was not found to be associated with worse survival (45). Overall, studies supported inclusion of RT as a part of the multimodality treatment approach in LMD of breast cancer.
Table 2.
Breast cancer: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Boogerd et al. (39) | RCT | 35 | 1991–1998 | 35 | 49% ITC; 46% C; 37% HT; 43% RT | 4.3 for ITC; 7 for no-ITC |
|
| Feyer et al. (40) | G | NA | 1995–2008 | NA | NA | NA |
|
| Le Rhun et al. (41, 42) | Obs | 103 | 2007–2011 | 39 | 100% ITC; 58% C; 17% RT | 3.8 |
|
| Niwinska et al. (43) | Obs | 187 | 1999–2015 | 49 | 68% ITC; 63% WBRT; 14% FSRT | 4 |
|
| Niwinska et al. (44) | Obs | 149 | 1999–2015 | 49 | 52% C; 62% RT; 65% ITC | 4.2 |
|
| Yust-Katz et al. (45) | Obs | 103 | 1995–2011 | 49.2 | 19% BSC; 53% WBRT; 19% FSRT; 36% C; 56% ITC | 4.3 |
|
| Kingston et al. (46) | Obs | 182 | 2004–2014 | 52.5 | 34% WBRT; 25% C; 7.7% ITC | 5.4 |
|
| Yu et al. (47) | Obs | 8 | 1990–1999 | 51.5 | 100% WBRT; 12.5% FSRT; 50% ITC | 5.4 |
|
| Chamberlain et al. (48) | Obs | 32 | 1986–1995 | 49 | 66% RT; 100% ITC | 7.5 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; RCT, randomized controlled trial; G, guidelines; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT; HT, hormonal therapy.
Feyer et al. published practical guidelines for palliative RT of breast cancer with brain metastases and LMD (40). The guidelines come from the German Society of Radiation Oncology (DEGRO) after performing a comprehensive survey of the literature. For patients with LMD, the group indicates that treatment is mostly indicated for patients with positive cytology in the CSF or with signs or symptoms of neurologic deficits. Treatment may include RT (WBRT or focal RT), C or ITC, or both—with prolongation of survival from several weeks to 4–6 months.
Boogerd et al. published a randomized controlled trial to determine the relevance of ITC for LMD in breast cancer (39). Patients were randomized to ITC (n = 17) or non-ITC treatment (n = 18). Appropriate systemic therapy and RT were given in each group (35% of patients in the ITC arm received focal RT and 2 patients received WBRT; 50% of patients in the non-ITC arm received focal RT, and 4 received WBRT). The authors found that standard systemic chemotherapy with focal RT for LMD is feasible; however, the addition of ITC did not lead to a survival benefit or improved neurological response, and was associated with an increased risk of neurotoxicity.
Non-small Cell Lung Cancer
A total of eight observational studies of 893 patients treated from 1986 to 2014 for LMD from non-small cell lung cancer were included (Table 3) (52–59). Patients were treated with WBRT (n = 389), FSRT (n = 10), C (n = 39), targeted therapy (TT; n = 278), ITC (n = 7), or BSC (n = 31). Overall survival ranged from 3 to 8.7 months for all patients. There were conflicting findings on whether WBRT or tyrosine-kinase inhibitors (TKIs) improved survival for patients; survival was improved for selected patients who received ITC. Similar to other histologies, patients with good performance status at the time of LMD diagnosis had better outcomes.
Table 3.
Non-small cell lung cancer: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Morris et al. (52) | Obs | 125 | 2002–2009 | 59 | 45% WBRT; 6% ITC; 16% C; 15% TT; 30% BSC | 3 |
|
| Kuiper et al. (53) | Obs | 32 | 2000–2014 | 54 | 78% TT; 6% C; 13% C+TT; 34% WBRT; 9% FSRT | 3.1 |
|
| Lee et al. (54) | Obs | 149 | 2001–2009 | 58 | 32% WBRT; 24% C; 13.4% BSC | 3.5 |
|
| Ozdemir et al. (55) | Obs | 51 | 2007–2014 | 53 | 100% WBRT | 3.9 |
|
| Liao et al. (56) | Obs | 212 | 2003–2010 | 56 | 58.5% TT; 60.4% WBRT | 4.5 |
|
| Chamberlain et al. (57) | Obs | 32 | 1986–1996 | 57 | 28% WBRT; 22% FSRT | 5 |
|
| Xu et al. (58) | Obs | 108 | 2006–2013 | 61 | 45% WBRT; 39% TT | 5.3 |
|
| Li et al. (59) | Obs | 184 | 2011 | 57 | 45% TT; 5.5% WBRT; 0.9% C; 38.5% combined tx; 10% BSC | 8.7 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT; TT, targeted therapy.
Gastrointestinal Cancer
Seven observational studies incorporated patients with gastrointestinal (GI) malignancies and LMD (Table 4) (60–66). These studies included 127 patients treated from 1944 to 2010 with the diagnoses of gastric cancer (n = 99), esophageal cancer (n = 7), and GI NOS (n = 21). Patients were treated with RT alone, NOS (n = 30), WBRT (n = 19), FSRT (n = 1), ITC (n = 15), RT + ITC (n = 48), C (n = 8), RT+C (n = 3), or BSC (n = 7). The median OS ranged from 1 to 3 months. From these studies, it was concluded that ITC improved survival on multivariate analysis and cytological negative conversion was predictive of a relatively longer survival; however, there was no clear benefit of the use of RT in patients with LMD from GI malignancies.
Table 4.
Gastrointestinal cancer: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Lee et al. (60) | Obs | 19 | 1992–2002 | 48 | 16% WBRT; 5% FSRT; 5% CSI; 53% ITC | 1 |
|
| Lukas et al. (61) | Obs | 7 | NR | 60 | 14% ITC; 57% WBRT | 1.2 |
|
| Kim et al. (62) | Obs | 5 | 1985–1992 | 43 | 100% WBRT; 40% ITC | 1.4 |
|
| Oh et al. (63) | Obs | 54 | 1994–2007 | 48.5 | 61% ITC, 24% WBRT + ITC; 11% WBRT; 19% C; 13% C+ITC | 1.6 |
|
| Giglio et al. (64) | Obs | 21 | 1944–2002 | NR | 43% RT; 19% ITC; 5% RT+ITC; 5% RT+C; 19% BSC | 1.75 |
|
| Tomita et al. (65) | Obs | 12 | 2002–2009 | 63 | 83% ITC; 58% WBRT | 2 |
|
| Kim et al. (66) | Obs | 9 | 1995–2010 | 53 | 33% BSC; 33% RT; 22% C+RT; 11% ITC | 3 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Adult CNS Gliomas
Seven observational studies incorporated patients with LMD from adult gliomas (Table 5) (67–73). These studies incorporated 101 patients treated between 1978 and 2015, with diagnoses of glioblastoma (GBM, n = 77), World Health Organization (WHO) grade II glioma (n = 1), WHO grade III astrocytoma (n = 14), and oligodendrogliomas (n = 7). Patients were treated with FBRT (n = 5), BSC (n = 5), C (n = 16), C+CSI (n = 4), C+FBRT+FSRT (n = 3), C+FBRT (n = 2), C+ whole spine RT (n = 1), and surgical resection (n = 2). The median OS from the diagnosis of LMD ranged from 2.8 to 10.2 months, with 32 months for oligodendrogliomas NOS. The series that included non-GBM's reported the longer survival outcomes. These studies indicated that patients treated with a combination of C+RT had significantly prolonged survival compared to either therapy alone or BSC. Patients with no symptoms from LMD and better performance status at presentation had longer survival with no difference in outcomes between patients with large volume vs. small volume LMD disease.
Table 5.
Adult CNS gliomas: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Vertosick et al. (67) | Obs | 11 | 1978–1990 | 38.5 | 82% FSRT; 9% FBRT; 9% CSI | 2.8 |
|
| Mandel et al. (68) | Obs | 36 | 2006–2012 | 44 | 14.7% BSC; 6% RT; 47% C; 29% C+RT; 3% surgery | 3.5 |
|
| Cohen et al. (69) | Obs | 3 | 2002 | 37 | 100% RT | 4 |
|
| Burger et al. (70) | Obs | 9 | 2008–2015 | 40.8 | 78% C; 11% WBRT; 44% FSRT; 33% FBRT | 4.3 |
|
| Endo et al. (71) | Obs | 5 | 1997–2001 | 38 | 80% surgery+RT+C; 20% SRS | 7.6 |
|
| Dardis et al. (72) | Obs | 34 | 2003–2013 | 49 | 26% ITC; 44% RT; 62% C; 9% surgery | 10.2 |
|
| Roldan et al. (73) | Obs | 8 | 1991–2009 | 41 | 62.5% BSC; 12.5% RT; 12.5% C; 12.5% C+RT | 32 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Melanoma
Three observational studies reviewed patients with a diagnosis of LMD from melanoma (Table 6) (49–51). These authors reviewed 140 patients treated from 1944 to 2015 treated with FSRT (n = 26), FBRT (n = 2), WBRT (n = 42), FSRT+FBRT (n = 9), C (n = 54), targeted therapy (TT; n = 9), ITC (n = 53), and surgical resection (n = 3); with 9 patients receiving TT+RT treatments. The median OS ranged from 2.3 to 5.2 months with the longest survival seen in the most modern series that included immunotherapy (50). The median OS for the 9 patients treated with TT+RT was 7.2 months. These studies found that survival is improved with the introduction of anti-PD-1 antibodies and BRAF inhibitors, and that multimodality therapy combined with these new techniques may be required to obtain the best control of neurologic symptoms and improve survival. Unfortunately, given the timeline of treatment of patients on these studies, only was study was performed in the modern era of immunotherapy and targeted therapy.
Table 6.
Melanoma: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop With LMD (n) | Treatment Era (years) | Median Age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Chamberlain et al. (49) | Obs | 16 | 1986–1995 | 47 | 44% FSRT; 63% WBRT; 75% C | 4 |
|
| Arasaratnam et al. (50) | Obs | 14 | 2012–2015 | 49.8 | 36% FSRT; 14% SRS; 50% WBRT; 57% TT; 14% surgery; 61% TT+RT | 5.2 |
|
| Harstad et al. (51) | Obs | 110 | 1944–2002 | NR | 56% WBRT; 33% FSRT; 27% WBRT+FSRT; 38% C; 48% ITC | 2.3 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Leukemia/Lymphoma
Two observational series met inclusion criteria and were included in the study (Table 7) (74, 75). A total of 47 patients treated between 1988 and 2016 included diagnoses of chronic lymphocytic leukemia (CLL; n = 3) and diffuse large B-cell lymphoma (DLBCL; n = 44). Patients were treated with FBRT (n = 4), WBRT (n = 42), and CSI (n = 1). The three patients with CLL had an OS of 8 months, 3 months, and still alive at censorship at 6 months. The median OS of the patients with DLBCL was 7 months. These studies indicated that patients with CLL and LMD involvement of their optic nerve had improved survival with focal RT and that RT provides high response rates in DLBCL and can contribute to long-term disease free survival.
Table 7.
Leukemia/Lymphoma: included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Currie et al. (74) | Obs | 3 | 1988 | 63 | 100% FBRT | NR |
|
| Milgrom et al. (75) | Obs | 44 | 2006–2016 | NR | 95% WBRT; 2% CSI; 70% C | 7 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Gynecologic Cancer
Two observational studies included patients with gynecologic cancer leading to a diagnosis of LMD (Table 8) (76, 77). These studies included 15 patients treated between 1996 and 2010 with diagnoses of ovarian cancer (n = 12) and cervical/endometrial cancer (n = 3). Patients were treated with WBRT (n = 8), FBRT (n = 1), FSRT (n = 5), C (n = 1), and BSC (n = 1). The median overall survival was 3.6 months for patients with ovarian cancer, and 2, 4, and 7 months for the three patients with cervical/endometrial cancer. It was concluded that RT can provide a partial or complete response of LMD, although with recurrence likely.
Table 8.
Gynecologic cancer: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Teckie et al. (76) | Obs | 12 | 1996–2010 | 56.1 | 58% WBRT; 8% partial brain RT;17% FSRT; 8% C; 8% BSC | 3.6 |
|
| Asensio et al. (77) | Obs | 3 | 2000 | 63 | 33% ITC; 100% FSRT; 33% WBRT; 33% C | NR |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Esthesioneuroblastoma
One observational study met inclusion criteria and included patients with esthesioneuroblastoma (Table 9) (78). In this study, Chamberlain et al. included 4 patients ranging in age from 47 to 58 years treated in 2002 with FSRT (n = 2), WBRT (n = 3), and C (n = 4). The patients had OS of 4, 11, 12, and 13 months, respectively. The authors concluded that LMD from esthesioneuroblastoma is treatable with acceptable toxicity.
Table 9.
Esthesioneuroblastoma: included studies evaluating the use of RT for LMD.
| Reference | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Chamberlain et al. (78) | Obs | 4 | 2002 | 53 | 50% FSRT; 50% WBRT + ITC | NR |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Pediatric CNS Disease
Three observational studies met inclusion criteria that included pediatric patients with central nervous system (CNS) disease (Table 10) (79–81). These series evaluated 34 patients (ages 1–34) treated from 1977 to 2012 with diagnoses of astrocytoma (n = 6), medulloblastoma (n = 9), ependymoma (n = 3), atypical teratoid rhabdoid tumor (ATRT; n = 4), primitive neuroectodermal tumor (PNET; n = 3), and other (n = 9). Patients received treatment for their LMD with FSRT (n = 28), CSI (n = 6), and FBRT (n = 6). The median OS was not reached in two studies. In patients with astrocytoma receiving FSRT, the median OS was 7 months. In patients with either medulloblastoma, ependymoma, PNET, or other treated with FSRT, the 12 month OS was 68%; patients with PNET had a median OS of 9.2 months. For patients with primary CNS disease, NOS, the mean OS was 25.7 months with salvage CSI. Therefore, these studies revealed that RT in the treatment of LMD is beneficial with minimal toxicity.
Table 10.
Pediatric CNS disease: Included studies evaluating the use of RT for LMD.
| References | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| Kandt et al. (79) | Obs | 6 | 1977–1982 | 9 | 67% FSRT; 17% C; 17% BSC | 7 |
|
| Ray et al. (80) | Obs | 22 | 2004–2012 | 5 | 100% FSRT | NYR |
|
| Wei et al. (81) | Obs | 6 | 2007–2012 | 6.5 | 100% WBRT; 17% CSI; 17% SRS | NR |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT; SRS, stereotactic radiosurgery; NYR, not yet reached; PFS, progression free survival.
Pediatric Rhabdomyosarcoma
One observational series met inclusion criteria and was included with patients with rhabdomyosarcoma and LMD (Table 11) (82). The authors included 13 pediatric patients with LMD (age from 1 to 34 years) treated from 1999 to 2016 with FBRT (n = 1), WBRT (n = 5), CSI (n = 10), C (n = 4), surgery (n = 2). The median OS was 5 months and the study concluded that treatment with CNS directed RT should be considered, however, outcomes were poor.
Table 11.
Pediatric rhabdomyosarcoma: Included studies evaluating the use of RT for LMD.
| Reference | Study type | Study Pop with LMD (n) | Treatment era (years) | Median age, years | Treatment | Median OS (months) | Conclusions |
|---|---|---|---|---|---|---|---|
| De et al. (82) | Obs | 21 | 1999–2016 | 15 | 48% CSI; 14% C; 19% WBRT; 5% ITC; 14% surgery; 5% SRS | 5 |
|
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Ongoing Trials
We performed a search of the ClinicalTrials.gov database to identify any ongoing therapeutic trials utilizing radiotherapy in the treatment of LMD. As of May 2019, we identified 5 ongoing relevant studies (Table 12). One study is using proton radiotherapy alone to the CSI for patients with LMD (84). Three of the trials are evaluating the use of radiotherapy with another drug intervention (pemetrexed, Avelumab, methotrexate, cytarabine) (83, 85, 86). Finally, one trial is evaluating the use of radiation iodine I-131 monoclonal antibody for the treatment of LMD (87).
Table 12.
Ongoing trials: Evaluating the use of RT for LMD.
| References | Study type | Study Pop/Pt treated with RT (n) | Treatment | ClinicalTrials.gov Identifier |
|---|---|---|---|---|
| H. Lee Moffitt Cancer Center (83) | Phase I | LMD | Arm 1: Avelumab + WBRT | NCT03719768 |
| Memorial Sloan Kettering (84) | Single arm, prospective | LMD | Proton CSI | NCT03520504 |
| The First Hospital of Jilin University Changchun, China (85) | Phase I/II | LMD from solid tumors | ITC (pemetrexed)+RT | NCT03507244 |
| The First Hospital of Jilin University Changchun, China (86) | Phase II | LMD from solid tumors | ITC (methotrexate and cytarabine)+RT | NCT03082144 |
| Memorial Sloan Kettering (87) | Phase I | LMD | I-131 monoclonal Ab RT | NCT00089245 |
RT, radiotherapy; LMD, leptomeningeal disease; Pop, population; Obs, observational study; PP, practice patterns; NR, not reported; BSC, best supportive care; C, chemotherapy alone; ITC, intrathecal chemotherapy; WBRT, whole brain radiotherapy; FSRT, spine RT; CSI, craniospinal RT.
Risk of Bias
Due to the small number of randomized trials found, all trials that met eligibility criteria were included.
Discussion
Summary of Main Findings
Leptomeningeal disease is an important, but devastating complication of cancer that leads to significant morbidity and mortality. Since its initial discovery in the 1800s, the incidence of this condition has continued to increase as our methods of diagnosis continue to improve and patients with various cancer histologies are experiencing longer survival, even with metastatic disease. Based on the single histology studies included in this systematic review, the incidence of LMD treated with RT from most common to least common was: lung (n = 893) > breast (n = 799) > melanoma (n = 140) > GI (n = 127) > adult CNS gliomas (n = 106), which is similar to the reported frequencies of the incidence of LMD in all patients, in the literature (2–4). The studies included in this review included patients treated from 1944 to 2015, and all of these studies were included given the small number of studies meeting inclusion criteria in the more modern era. The imaging (or lack thereof) and treatment techniques utilized in the older studies do not reflect how we think about LMD today. Therefore, we have separated these studies into those that included a majority of patients treated with RT prior to the year 2000 and those more modern studies that incorporated a majority of patients treated with RT in the year 2000 and after when evaluating the incidence of LMD treated with RT and the OS seen in these studies, as these outcomes have evolved over time. Prior to the year 2000, the incidence of LMD treated with RT is as follows: melanoma (n = 126) > breast (n = 75) > GI (n = 45) > lung (n = 32) > adult CNS gliomas (n = 16). After the year 2000, the incidence of LMD treated with RT is as follows: lung (n = 861) > breast (n = 724) > adult CNS gliomas (n = 90) > GI (n = 82) > melanoma (n = 14). The median overall survival ranges reported in these studies have also evolved over time, and are demonstrated in Figure 2. Prior to the year 2000, OS in patients with LMD treated with RT increased from shortest to longest in primary histologies of GI (1–1.75 months) < melanoma (2.3–4 months) < lung (5 months) < breast (5.4–7.5 months) < adult CNS gliomas (2.8–7.6 months). After the year 2000, OS increased from shortest to longest in GI (1.2–3 months) < breast (3.8–5.4 months) < melanoma (5.2 months) < lung (3–8.7 months) < adult CNS gliomas (3.5–10.2 months).
Figure 2.
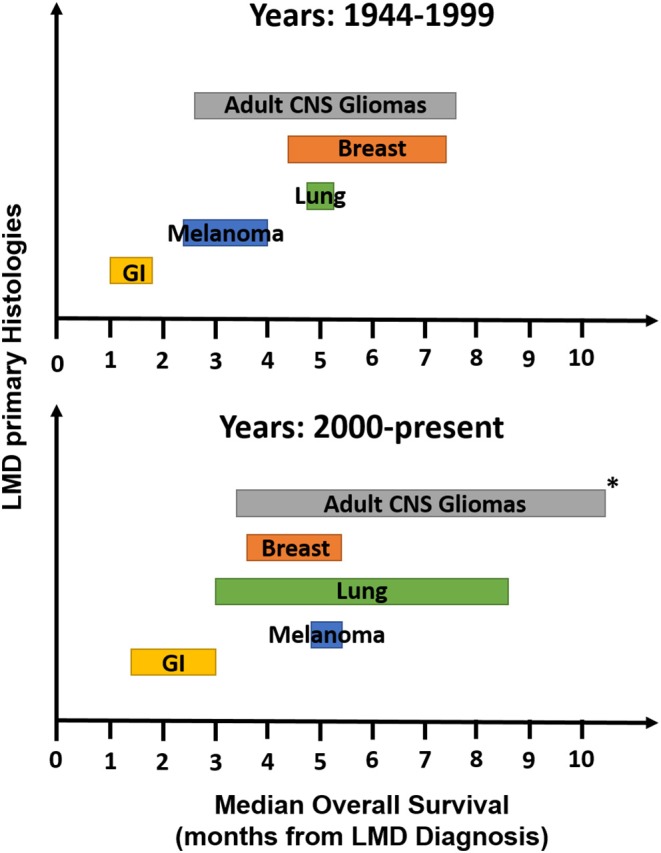
Median OS ranges from observational studies meeting inclusion criteria for the most common histologies of LMD. OS, overall survival; LMD, leptomeningeal disease. *Excluding trial by Roldan et al. (73) which included only patients with oligodendrogliomas and reported an OS of 32 months.
The optimal management of this condition remains unknown, with limited data to guide standard of care treatment. Current management approaches include a range of treatments including systemic therapy (intravenous or intrathecal), targeted therapy, focal or non-focal radiotherapy, and supportive care. A recent survey study of oncologists across Europe evaluated their diagnosis and treatment patterns for patients with LMD from solid tumors. A total of 115 physicians submitted responses (19% radiation oncologists, 23% medical oncologists, 34% neuro-oncologists, and 10% neurosurgeons) reporting that only 31.5% always administer systemic treatment when feasible, 15.5% felt that WBRT should always be performed, while 73% of medical oncologists, 56% of neuro-oncologists, 50% of radiation oncologists, and 39% of neurosurgeons felt that WBRT should be offered in the setting multifocal nodular disease only. A total of 73% of respondents declared that focal RT should only be performed in cases of neurologic symptoms only when they could be linked to an MRI abnormality and not for neurological signs or symptoms alone (88). This wide range in practice patterns highlights the need for more formal guidelines and recommendations for the treatment of LMD.
Recent developments, to assist in the standardization of diagnosis of LMD, were performed by an international panel of experts from the United States and Europe, termed the RANO group. This group recently published their results of using an MRI scorecard to assess response to treatment in patients with leptomeningeal disease. Unfortunately, after MRIs of 22 patients with LMD were scored by neuro-oncologists and neuroradiologists, many raters experienced difficulty with the instructions of the scorecard and no acceptable alpha concordance coefficient was obtained. The authors are currently working on a more simplified scorecard that will require validation, but will be a great step forward in the standardization of this disease process, hopefully leading to more comparable trials in the future (89).
The National Comprehensive Cancer Network (NCCN) has recently incorporated risk stratification and guidelines for the treatment of LMD (90). Patients with LMD can be defined as Good Risk if they have all of the following characteristics: Karnofsky Performance Status (KPS) ≥60, no major neurologic deficits, minimal systemic disease, and if they have a reasonable systemic treatment options should they need them. Patients in this category are typically diagnosed with LMD based on routine imaging and are being evaluated on an outpatient basis. Ultimately, the level of aggressiveness of the treatment provided should include a discussion with the patient and their wishes. RT is typically included in the multimodal treatment of patients with Good Risk LMD. In contrast to Good Risk LMD, patients with LMD can be defined as Poor Risk if they have any of the following characteristics: KPS <60, multiple, serious, or major neurologic deficits, extensive systemic disease with few treatment options, bulky central nervous system (CNS) disease, or encephalopathy. Some exceptions to these symptoms, where a patient may still be considered for a more aggressive treatment course, include patients with exceptionally chemosensitive tumors (e.g., small cell lung cancer, lymphoma).
Traditionally, radiotherapy has been recommended for patients with symptomatic disease or bulky metastatic disease, regardless of clinical symptoms (4, 13, 15, 89–91). To date, there is no level I evidence available on the use of RT for LMD, as the only randomized controlled trial included in this systematic review sought to evaluate the use of ITC in patients with LMD from breast cancer (39). However, a large majority (69%) of the observational studies found an improvement or likely improvement in OS with the addition of RT to the treatment regimen of LMD of those studies that commented on the influence of a single or combined treatment regimen on survival (n = 18/26 studies).
To the best of our knowledge, this is the first systemic review that has attempted to assimilate the reported data for the use of radiotherapy in the treatment of LMD across a range histologies. In our own clinical experience, radiotherapy for the treatment of LMD is consistently considered and discussed in the multidisciplinary setting. The treatment of RT is often recommended for patients with bulky disease seen on imaging or causing symptoms to prevent further neurologic compromise, or for asymptomatic patients with LMD seen on MRI who have well-controlled extracranial disease.
The results of our review indicate that for the majority of studies, any treatment was felt to be superior to best supportive care in the management of LMD, but this may reflect a selection bias of patients with better prognosis and performance status to receive treatment. The use of RT monotherapy was found to be beneficial in patients with LMD from pediatric CNS gliomas, leukemia/lymphoma, gynecologic, esthesioneuroblastoma, and pediatric rhabdomyosarcoma histologies. For patients with LMD from breast cancer, melanoma and adult CNS cancer, multimodality therapy, including the use of radiotherapy, was found to be most beneficial. In terms of prognostic factors, MVA across the included series in this systematic review consistently revealed that a good performance status at the time of diagnosis of LMD and normal CSF flow predicted for improved survival. In patients with breast cancer, hormone receptor positive disease, limited prior systemic therapy exposure, and LMD as the first site of metastases additionally predicted for improved survival.
Due to the vast clinical and methodologic differences between the included studies, a meta-analysis could not be performed to identify the optimal treatments for patients with LMD. Most studies only reported whether RT was used or not, and what type of RT was used (WBRT, focal brain/spine RT, etc.) with a complete lack of details about RT dose, fields, or timing. Additionally, the role of targeted therapies and immunotherapy has greatly increased in the treatment of LMD in the past decade (91). For example, for NSCLC with LMD, current therapies target epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangement via tyrosine kinase inhibitors (TKIs); in breast cancer, HER2 positive disease may be targeted via an intrathecal injection; and finally, melanoma with BRAF V600E mutations may also be treated with targeted therapies. Given that the included studies only included patients treated through 2015, the role and impact of targeted therapies is not reflected in this systematic review. It will be imperative to re-evaluate the use of RT, paying special attention to the dose of RT, RT fields, and timing of RT, in conjunction with these targeted and immunotherapies, in future studies.
Additionally, new classifications of LMD are being reported that may influence survival outcomes and help aid in the most optimal therapy selection. A recent report by Prabhu et al. categorized the LMD pattern of their postoperative stereotactic radiosurgery cohort as nodular or the more classical “sugarcoating” pattern. (92) The authors found that nodular LMD was less likely to be symptomatic and had better OS outcomes. Furthermore, when the patients with nodular LMD were treated with focal RT, as opposed to WBRT, they had a higher risk of second LMD recurrence, but no detriment in OS, providing a reasonable, less toxic, treatment strategy for these patients. Unfortunately, LMD was not subclassified in the articles included in this review. Future studies should consider further subclassification of this heterogeneous disease.
Limitations
In conducting this systematic review, it became very apparent that there is a paucity of prospective, interventional studies in the treatment of LMD, particularly for the use of radiotherapy for the treatment of LMD. The single RCT that met inclusion criteria was a randomized trial evaluating intraventricular chemotherapy for LMD that also reported that the use of RT with systemic chemotherapy was feasible in this population (39).
Conclusions
In conclusion, LMD is a devastating complication of cancer with reported survivals from the time of diagnosis ranging from 2 to 4 months in prior literature (16–19), and 1–32 months in our review, depending on the primary histology. Based on this systematic review, the recommendation for the treatment of LMD is for multimodality discussion of cases and treatment, including the use of radiotherapy, for LMD. However, with continued advances in systemic therapy including targeted therapy and immunotherapy as well as imaging advances, the landscape of metastatic disease and LMD is evolving rapidly. Within this changing environment, the role of RT will likely also continue to evolve and advance. As this systematic review highlights, there is limited high-quality evidence to guide the optimal use of radiotherapy for the treatment of LMD, and there is a great need for prospective, histology specific investigation of the role of radiotherapy for LMD in the era of modern systemic therapies.
Author Contributions
SB and CC reviewed the articles included in this systematic review. CC developed the concept of the review and reviewed the manuscript. SB wrote the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Gregory Pratt of the Research Medical Library, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.01224/full#supplementary-material
References
- 1.Eberth CJ. Zur Entwicklung des Epitheliomas (Cholesteatomas) dur Pia under der Lungs. Virchow's Arch. (1870) 49:51–63. 10.1007/BF02214196 [DOI] [Google Scholar]
- 2.Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, et al. Harrison's Principles of Internal Medicine. 17th ed New York, NY: McGraw Hill; (2008). [Google Scholar]
- 3.Nugent JL, Bunn PA, Jr, Matthews MJ, Ihde DC, Cohen MH, Gazdar A, et al. CNS metastases in small cell bronchogenic carcinoma: increasing frequency and changing pattern with lengthening survival. Cancer. (1979) 44:1885–93. [DOI] [PubMed] [Google Scholar]
- 4.Shapiro WR, Posner JB, Ushio Y, Chemik NL, Young DF. Treatment of meningeal neoplasms. Cancer Treat Rep. (1977) 61:733–43. [PubMed] [Google Scholar]
- 5.Aroney RS, Dalley DN, Chan WK, Bell DR, Levi JA. Meningeal carcinomatosis in small cell carcinoma of the lung. Am J Med. (1981) 71:26–32. 10.1016/0002-9343(81)90254-0 [DOI] [PubMed] [Google Scholar]
- 6.Glass JP, Melamed M, Chernik NL, Posner JB. Malignant cells in cerebrospinal fluid (CSF): the meaning of a positive CSF cytology. Neurology. (1979) 29:1369–75. 10.1212/WNL.29.10.1369 [DOI] [PubMed] [Google Scholar]
- 7.Price RA, Johnson WW. The central nervous system in childhood leukemia. I. The arachnoid. Cancer. (1973) 31:520–33. [DOI] [PubMed] [Google Scholar]
- 8.Rosen ST, Aisner J, Makuch RW, Matthews MJ, Ihde DC, Whitacre M, et al. Carcinomatous leptomeningitis in small cell lung cancer: a clinicopathologic review of the National Cancer Institute experience. Medicine. (1982) 61:45–53. 10.1097/00005792-198201000-00005 [DOI] [PubMed] [Google Scholar]
- 9.Balm M, Hammack J. Leptomeningeal carcinomatosis. Presenting features and prognostic factors. Arch Neurol. (1996) 53:626–32. 10.1001/archneur.1996.00550070064013 [DOI] [PubMed] [Google Scholar]
- 10.Chamberlain MC. Carcinomatous meningitis. Arch Neurol. (1997) 54:16–7. 10.1001/archneur.1997.00550130008003 [DOI] [PubMed] [Google Scholar]
- 11.DeAngelis LM. Current diagnosis and treatment of leptomeningeal metastasis. J Neurooncol. (1998) 38:245–52. [DOI] [PubMed] [Google Scholar]
- 12.Jayson GC, Howell A. Carcinomatous meningitis in solid tumours. Ann Oncol. (1996) 7:773–86. 10.1093/oxfordjournals.annonc.a010755 [DOI] [PubMed] [Google Scholar]
- 13.Kaplan JG, DeSouza TG, Farkash A, Shafran B, Pack D, Rehman F, et al. Leptomeningeal metastases: comparison of clinical features and laboratory data of solid tumors, lymphomas and leukemias. J Neurooncol. (1990) 9:225–9. 10.1007/BF02341153 [DOI] [PubMed] [Google Scholar]
- 14.Reuler JB, Meier D. Leptomeningeal carcinomatosis with normal CSF features. Arch Intern Med. (1979) 139:237–8. 10.1001/archinte.139.2.237 [DOI] [PubMed] [Google Scholar]
- 15.Wasserstrom WR, Glass JP, Posner JB. Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer. (1982) 49:759–72. [DOI] [PubMed] [Google Scholar]
- 16.Chamberlain MC, Glantz M, Groves MD, Wilson WH. Diagnostic tools for neoplastic meningitis: detecting disease, identifying patient risk, and determining benefit of treatment. Semin Oncol. (2009) 36(4 Suppl 2): S35–45. 10.1053/j.seminoncol.2009.05.005 [DOI] [PubMed] [Google Scholar]
- 17.Hermann B, Hultenschmidt B, Sautter-Bihl ML. Radiotherapy of the neuroaxis for palliative treatment of leptomeningeal carcinomatosis. Strahlenther Onkol. (2001) 177:195–9. 10.1007/PL00002398 [DOI] [PubMed] [Google Scholar]
- 18.Hitchins RN, Bell DR, Woods RL, Levi JA. A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. J Clin Oncol. (1987) 5:1655–62. 10.1200/JCO.1987.5.10.1655 [DOI] [PubMed] [Google Scholar]
- 19.Waki F, Ando M, Takashima A, Yonemori K, Nokihara H, Miyake M, et al. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J Neurooncol. (2009) 93:205–12. 10.1007/s11060-008-9758-3 [DOI] [PubMed] [Google Scholar]
- 20.Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. (2009) 62:1006–12. 10.1016/j.jclinepi.2009.06.005 [DOI] [PubMed] [Google Scholar]
- 21.Passarin MG, Sava T, Furlanetto J, Molino A, Nortilli R, Musso AM, et al. Leptomeningeal metastasis from solid tumors: a diagnostic and therapeutic challenge. Neurol Sci. (2015) 36:117–23. 10.1007/s10072-014-1881-7 [DOI] [PubMed] [Google Scholar]
- 22.Gani C, Muller AC, Eckert F, Schroeder C, Bender B, Pantazis G, et al. Outcome after whole brain radiotherapy alone in intracranial leptomeningeal carcinomatosis from solid tumors. Strahlentherapie und Onkol. (2012) 188:148–53. 10.1007/s00066-011-0025-8 [DOI] [PubMed] [Google Scholar]
- 23.Brower JV, Saha S, Rosenberg SA, Hullett CR, Ian Robins H. Management of leptomeningeal metastases: prognostic factors and associated outcomes. J Clin Neurosci. (2016) 27:130–7. 10.1016/j.jocn.2015.11.012 [DOI] [PubMed] [Google Scholar]
- 24.Clarke JL, Perez HR, Jacks LM, Panageas KS, Deangelis LM. Leptomeningeal metastases in the MRI era. Neurology. (2010) 74:1449–54. 10.1212/WNL.0b013e3181dc1a69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oechsle K, Lange-Brock V, Kruell A, Bokemeyer C, de Wit M. Prognostic factors and treatment options in patients with leptomeningeal metastases of different primary tumors: a retrospective analysis. J Cancer Res Clin Oncol. (2010) 136:1729–35. 10.1007/s00432-010-0831-x [DOI] [PubMed] [Google Scholar]
- 26.Kwon J, Chie EK, Kim K, Kim HJ, Wu HG, Kim IH, et al. Impact of multimodality approach for patients with leptomeningeal metastases from solid tumors. J Korean Med Sci. (2014) 29:1094–101. 10.3346/jkms.2014.29.8.1094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sause WT, Crowley J, Eyre HJ, Rivkin SE, Pugh RP, Quagliana JM, et al. Whole brain irradiation and intrathecal methotrexate in the treatment of solid tumor leptomeningeal metastases–a Southwest Oncology Group study. J Neuro Oncol. (1988) 6:107–12. 10.1007/BF02327385 [DOI] [PubMed] [Google Scholar]
- 28.Chamberlain MC, Kormanik PA. Prognostic significance of coexistent bulky metastatic central nervous system disease in patients with leptomeningeal metastases. Arch Neurol. (1997) 54:1364–8. 10.1001/archneur.1997.00550230037013 [DOI] [PubMed] [Google Scholar]
- 29.Herrlinger U, Forschler H, Kuker W, Meyermann R, Bamberg M, Dichgans J, et al. Leptomeningeal metastasis: survival and prognostic factors in 155 patients. J Neurol Sci. (2004) 223:167–78. 10.1016/j.jns.2004.05.008 [DOI] [PubMed] [Google Scholar]
- 30.Chamberlain MC. Pediatric leptomeningeal metastases: outcome following combined therapy. J Child Neurol. (1997) 12:53–9. 10.1177/088307389701200109 [DOI] [PubMed] [Google Scholar]
- 31.Sakaguchi M, Maebayashi T, Aizawa T, Ishibashi N, Saito T. Patient outcomes of whole brain radiotherapy for brain metastases versus leptomeningeal metastases: a retrospective study. Asia-Pacific J Clin Oncol. (2017) 13:e449–57. 10.1111/ajco.12597 [DOI] [PubMed] [Google Scholar]
- 32.Pan Z, Yang G, He H, Zhao G, Yuan T, Li Y, et al. Concurrent radiotherapy and intrathecal methotrexate for treating leptomeningeal metastasis from solid tumors with adverse prognostic factors: A prospective and single-arm study. Int J Cancer. (2016) 139:1864–72. 10.1002/ijc.30214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bokstein F, Lossos A, Siegal T. Leptomeningeal metastases from solid tumors: a comparison of two prospective series treated with and without intra-cerebrospinal fluid chemotherapy. Cancer. (1998) 82:1756–63. [PubMed] [Google Scholar]
- 34.Wolf A, Donahue B, Silverman JS, Chachoua A, Lee JK, Kondziolka D. Stereotactic radiosurgery for focal leptomeningeal disease in patients with brain metastases. J Neuro Oncol. (2017) 134:139–43. 10.1007/s11060-017-2497-6 [DOI] [PubMed] [Google Scholar]
- 35.Coakham HB, Kemshead JT. Treatment of neoplastic meningitis by targeted radiation using (131)I-radiolabelled monoclonal antibodies. Results of responses and long term follow-up in 40 patients. J Neuro Oncol. (1998) 38:225–32. 10.1023/A:1005996606073 [DOI] [PubMed] [Google Scholar]
- 36.Du C, Hong R, Shi Y, Yu X, Wang J. Leptomeningeal metastasis from solid tumors: a single center experience in Chinese patients. J Neuro Oncol. (2013) 115:285–91. 10.1007/s11060-013-1228-x [DOI] [PubMed] [Google Scholar]
- 37.Hyun JW, Jeong IH, Joung A, Cho HJ, Kim SH, Kim HJ. Leptomeningeal metastasis: clinical experience of 519 cases. Eur J Cancer. (2016) 56:107–14. 10.1016/j.ejca.2015.12.021 [DOI] [PubMed] [Google Scholar]
- 38.Chamberlain MC, Kormanik PA. Prognostic significance of 111indium-DTPA CSF flow studies in leptomeningeal metastases. Neurology. (1996) 46:1674–7. 10.1212/WNL.46.6.1674 [DOI] [PubMed] [Google Scholar]
- 39.Boogerd W, van den Bent MJ, Koehler PJ, Heimans JJ, van der Sande JJ, Aaronson NK, et al. The relevance of intraventricular chemotherapy for leptomeningeal metastasis in breast cancer: a randomised study. Eur J Cancer. (2004) 40:2726–33. 10.1016/j.ejca.2004.08.012 [DOI] [PubMed] [Google Scholar]
- 40.Feyer P, Sautter-Bihl ML, Budach W, Dunst J, Haase W, Harms W, et al. DEGRO Practical Guidelines for palliative radiotherapy of breast cancer patients: brain metastases and leptomeningeal carcinomatosis. Strahlenther Onkol. (2010) 186:63–9. 10.1007/s00066-010-2100-y [DOI] [PubMed] [Google Scholar]
- 41.Le Rhun E, Taillibert S, Zairi F, Pannier D, Boulanger T, Andre C, et al. Prolonged survival of patients with breast cancer-related leptomeningeal metastases. Anticancer Res. (2013) 33:2057–63. [PubMed] [Google Scholar]
- 42.Le Rhun E, Taillibert S, Zairi F, Kotecki N, Devos P, Mailliez A, et al. A retrospective case series of 103 consecutive patients with leptomeningeal metastasis and breast cancer. J Neuro Oncol. (2013) 113:83–92. 10.1007/s11060-013-1092-8 [DOI] [PubMed] [Google Scholar]
- 43.Niwinska A, Pogoda K, Michalski W, Kunkiel M, Jagiello-Gruszfeld A. Determinants of prolonged survival for breast cancer patient groups with leptomeningeal metastasis (LM). J Neuro Oncol. (2018) 138:191–8. 10.1007/s11060-018-2790-z [DOI] [PubMed] [Google Scholar]
- 44.Niwinska A, Rudnicka H, Murawska M. Breast cancer leptomeningeal metastasis: the results of combined treatment and the comparison of methotrexate and liposomal cytarabine as intra-cerebrospinal fluid chemotherapy. Clin Breast Cancer. (2015) 15:66–72. 10.1016/j.clbc.2014.07.004 [DOI] [PubMed] [Google Scholar]
- 45.Yust-Katz S, Garciarena P, Liu D, Yuan Y, Ibrahim N, Yerushalmi R, et al. Breast cancer and leptomeningeal disease (LMD): hormone receptor status influences time to development of LMD and survival from LMD diagnosis. J Neurooncol. (2013) 114:229–35. 10.1007/s11060-013-1175-6 [DOI] [PubMed] [Google Scholar]
- 46.Kingston B, Kayhanian H, Brooks C, Cox N, Chaabouni N, Redana S, et al. Treatment and prognosis of leptomeningeal disease secondary to metastatic breast cancer: a single-centre experience. Breast. (2017) 36:54–9. 10.1016/j.breast.2017.07.015 [DOI] [PubMed] [Google Scholar]
- 47.Yu H, Mitsumori M, Nagata Y, Katakura Y, Kokubo M, Oya N, et al. Meningeal carcinomatosis in patients with breast cancer: report of 8 patients. Breast Cancer. (2001) 8:74–8. 10.1007/BF02967482 [DOI] [PubMed] [Google Scholar]
- 48.Chamberlain MC, Kormanik PR. Carcinomatous meningitis secondary to breast cancer: predictors of response to combined modality therapy. J Neuro Oncol. (1997) 35:55–64. 10.1023/A:1005803918194 [DOI] [PubMed] [Google Scholar]
- 49.Chamberlain M, Kormanik P. Leptomeningeal metastases due to melanoma. Int J Oncol. (1996) 9:505–10. 10.3892/ijo.9.3.505 [DOI] [PubMed] [Google Scholar]
- 50.Arasaratnam M, Hong A, Shivalingam B, Wheeler H, Guminksi AD, Long GV, et al. Leptomeningeal melanoma-A case series in the era of modern systemic therapy. Pigment Cell Melanoma Res. (2018) 31:120–4. 10.1111/pcmr.12652 [DOI] [PubMed] [Google Scholar]
- 51.Harstad L, Hess KR, Groves MD. Prognostic factors and outcomes in patients with leptomeningeal melanomatosis. Neuro Oncol. (2008) 10:1010–8. 10.1215/15228517-2008-062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Morris PG, Reiner AS, Szenberg OR, Clarke JL, Panageas KS, Perez HR, et al. Leptomeningeal metastasis from non-small cell lung cancer: survival and the impact of whole brain radiotherapy. J Thorac Oncol. (2012) 7:382–5. 10.1097/JTO.0b013e3182398e4f [DOI] [PubMed] [Google Scholar]
- 53.Kuiper JL, Hendriks LE, van der Wekken AJ, de Langen AJ, Bahce I, Thunnissen E, et al. Treatment and survival of patients with EGFR-mutated non-small cell lung cancer and leptomeningeal metastasis: a retrospective cohort analysis. Lung Cancer. (2015) 89:255–61. 10.1016/j.lungcan.2015.05.023 [DOI] [PubMed] [Google Scholar]
- 54.Lee SJ, Lee JI, Nam DH, Ahn YC, Han JH, Sun JM, et al. Leptomeningeal carcinomatosis in non-small-cell lung cancer patients: impact on survival and correlated prognostic factors. J Thorac Oncol. (2013) 8:185–91. 10.1097/JTO.0b013e3182773f21 [DOI] [PubMed] [Google Scholar]
- 55.Ozdemir Y, Yildirim BA, Topkan E. Whole brain radiotherapy in management of non-small-cell lung carcinoma associated leptomeningeal carcinomatosis: evaluation of prognostic factors. J Neurooncol. (2016) 129:329–35. 10.1007/s11060-016-2179-9 [DOI] [PubMed] [Google Scholar]
- 56.Liao BC, Lee JH, Lin CC, Chen YF, Chang CH, Ho CC, et al. Epidermal growth factor receptor tyrosine kinase inhibitors for non-small-cell lung cancer patients with leptomeningeal carcinomatosis. J Thorac Oncol. (2015) 10:1754–61. 10.1097/JTO.0000000000000669 [DOI] [PubMed] [Google Scholar]
- 57.Chamberlain MC, Kormanik P. Carcinoma meningitis secondary to non-small cell lung cancer: combined modality therapy. Arch Neurol. (1998) 55:506–12. 10.1001/archneur.55.4.506 [DOI] [PubMed] [Google Scholar]
- 58.Xu Q, Chen X, Qian D, Wang Y, Meng S, Liu H, et al. Treatment and prognostic analysis of patients with leptomeningeal metastases from non-small cell lung cancer. Thorac Cancer. (2015) 6:407–12. 10.1111/1759-7714.12188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Li YS, Jiang BY, Yang JJ, Tu HY, Zhou Q, Guo WB, et al. Leptomeningeal metastases in patients with NSCLC with EGFR mutations. J Thorac Oncol. (2016) 11:1962–9. 10.1016/j.jtho.2016.06.029 [DOI] [PubMed] [Google Scholar]
- 60.Lee JL, Kang YK, Kim TW, Chang HM, Lee GW, Ryu MH, et al. Leptomeningeal carcinomatosis in gastric cancer. J Neurooncol. (2004) 66:167–74. 10.1023/B:NEON.0000013462.43156.f4 [DOI] [PubMed] [Google Scholar]
- 61.Lukas RV, Mata-Machado NA, Nicholas MK, Salgia R, Antic T, Villaflor VM. Leptomeningeal carcinomatosis in esophageal cancer: a case series and systematic review of the literature. Dis Esophagus. (2015) 28:772–81. 10.1111/dote.12276 [DOI] [PubMed] [Google Scholar]
- 62.Kim M. Intracranial involvement by metastatic advanced gastric carcinoma. J Neurooncol. (1999) 43:59–62. [DOI] [PubMed] [Google Scholar]
- 63.Oh SY, Lee SJ, Lee J, Lee S, Kim SH, Kwon HC, et al. Gastric leptomeningeal carcinomatosis: multi-center retrospective analysis of 54 cases. World J Gastroenterol. (2009) 15:5086–90. 10.3748/wjg.15.5086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Giglio P, Weinberg JS, Forman AD, Wolff R, Groves MD. Neoplastic meningitis in patients with adenocarcinoma of the gastrointestinal tract. Cancer. (2005) 103:2355–62. 10.1002/cncr.21082 [DOI] [PubMed] [Google Scholar]
- 65.Tomita H, Yasui H, Boku N, Nakasu Y, Mitsuya K, Onozawa Y, et al. Leptomeningeal carcinomatosis associated with gastric cancer. Int J Clin Oncol. (2012) 17:361–6. 10.1007/s10147-011-0301-8 [DOI] [PubMed] [Google Scholar]
- 66.Kim NH, Kim JH, Chin HM, Jun KH. Leptomeningeal carcinomatosis from gastric cancer: single institute retrospective analysis of 9 cases. Ann Surg Treat Res. (2014) 86:16–21. 10.4174/astr.2014.86.1.16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Vertosick FT, Jr, Selker RG. Brain stem and spinal metastases of supratentorial glioblastoma multiforme: a clinical series. Neurosurgery. (1990) 27:516–21; discussion 521–2. 10.1227/00006123-199010000-00002 [DOI] [PubMed] [Google Scholar]
- 68.Mandel JJ, Yust-Katz S, Cachia D, Wu J, Liu D, de Groot JF, et al. Leptomeningeal dissemination in glioblastoma; an inspection of risk factors, treatment, and outcomes at a single institution. J Neurooncol. (2014) 120:597–605. 10.1007/s11060-014-1592-1 [DOI] [PubMed] [Google Scholar]
- 69.Cohen ZR, Hassenbusch SJ, Maor MH, Pfeffer RM, Ram Z. Intractable vomiting from glioblastoma metastatic to the fourth ventricle: three case studies. Neuro Oncol. (2002) 4:129–33. 10.1215/S1522851701000539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Burger MC, Zeiner PS, Jahnke K, Wagner M, Mittelbronn M, Steinbach JP. Addition of anti-angiogenetic therapy with bevacizumab to chemo- and radiotherapy for leptomeningeal metastases in primary brain tumors. PLoS ONE. (2016) 11:e0155315. 10.1371/journal.pone.0155315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Endo H, Kumabe T, Jokura H, Shirane R, Ariga H, Takai Y, et al. Leptomeningeal dissemination of cerebellar malignant astrocytomas. J Neurooncol. (2003) 63:191–9. 10.1023/a:1023983518341 [DOI] [PubMed] [Google Scholar]
- 72.Dardis C, Milton K, Ashby L, Shapiro W. Leptomeningeal metastases in high-grade adult glioma: development, diagnosis, management, and outcomes in a series of 34 patients. Front Neurol. (2014) 5:220. 10.3389/fneur.2014.00220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Roldan G, Chan J, Eliasziw M, Cairncross JG, Forsyth PA. Leptomeningeal disease in oligodendroglial tumors: a population-based study. J Neurooncol. (2011) 104:811–5. 10.1007/s11060-011-0551-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Currie JN, Lessell S, Lessell IM, Weiss JS, Albert DM, Benson EM. Optic neuropathy in chronic lymphocytic leukemia. Arch Ophthalmol. (1988) 106:654–60. 10.1001/archopht.1988.01060130708030 [DOI] [PubMed] [Google Scholar]
- 75.Milgrom SA, Pinnix CC, Chi TL, Vu TH, Gunther JR, Sheu T, et al. Radiation Therapy as an Effective Salvage Strategy for Secondary CNS Lymphoma. Int J Radiat Oncol Biol Phys. (2018) 100:1146–54. 10.1016/j.ijrobp.2018.01.003 [DOI] [PubMed] [Google Scholar]
- 76.Teckie S, Makker V, Tabar V, Alektiar K, Aghajanian C, Hensley M, et al. Radiation therapy for epithelial ovarian cancer brain metastases: clinical outcomes and predictors of survival. Radiat Oncol. (2013) 8:36. 10.1186/1748-717X-8-36 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Asensio N, Luis A, Costa I, Oliveira J, Vaz F. Meningeal carcinomatosis and uterine carcinoma: three different clinical settings and review of the literature. Int J Gynecol Cancer. (2009) 19:168–72. 10.1111/IGC.0b013e31819a1e1a [DOI] [PubMed] [Google Scholar]
- 78.Chamberlain MC. Treatment of intracranial metastatic esthesioneuroblastoma. Cancer. (2002) 95:243–8. 10.1002/cncr.10679 [DOI] [PubMed] [Google Scholar]
- 79.Kandt RS, Shinnar S, D'Souza BJ, Singer HS, Wharam MD, Gupta PK. Cerebrospinal metastases in malignant childhood astrocytomas. J Neurooncol. (1984) 2:123–8. 10.1007/BF00177897 [DOI] [PubMed] [Google Scholar]
- 80.Ray GL, Buchsbaum JC, McMullen KP, Simoneaux RV, Hines M, Douglas JG, et al. Definitive treatment of leptomeningeal spinal metastases in children. Pediatr Blood Cancer. (2013) 60:1839–41. 10.1002/pbc.24659 [DOI] [PubMed] [Google Scholar]
- 81.Wei RL, Nguyen ST, Yang JN, Wolff J, Mahajan A. Salvage craniospinal irradiation with an intensity modulated radiotherapy technique for patients with disseminated neuraxis disease. Pract Radiat Oncol. (2012) 2:e69–75. 10.1016/j.prro.2012.01.004 [DOI] [PubMed] [Google Scholar]
- 82.De B, Kinnaman MD, Wexler LH, Kramer K, Wolden SL. Central nervous system relapse of rhabdomyosarcoma. Pediatr Blood Cancer. (2018) 65:26710. 10.1002/pbc.26710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.H. Lee Moffitt Cancer Center Avelumab with Radiotherapy in Patients with Leptomeningeal Disease. (2019) ClinicalTrials.gov Identifier: NCT03719768. (cited January 5, 2019).
- 84.Memorial Sloan Kettering Study of Proton Radiation to the Brain and Spinal Cord for Patients with Leptomeningeal Metastases. (2019) ClinicalTrials.gov Identifier: NCT03520504. (cited 2019 5/1/19).
- 85.The First Hospital of Jilin University Changchun China Concurrent Intrathecal-Pemetrexed and Involved Field Radiotherpy for Leptomeningeal Metastasis from Solid Tumors. (2019) ClinicalTrials.gov Identifier: NCT03507244. (cited January 5, 2019).
- 86.The First Hospital of Jilin University Changchun China Concurrent Involved Field Radiotherapy and Intrathecal Chemotherapy for Leptomningeal Metastases from Solid Tumors. (2019) ClinicalTrials.gov Identifier: NCT03082144. (cited January 5, 2019).
- 87.Kettering MS. Radiolabeled Monoclonal Antibody Therapy in Treating Patients With Refractory, Recurrent, or Advanced CNS or Leptomeningeal Cancer. (2019) ClinicalTrials.gov Identifier: NCT00089245 (cited January 5, 2019).
- 88.Le Rhun E, Ruda R, Devos P, Hoang-Xuan K, Brandsma D, Perez Segura P, et al. Diagnosis and treatment patterns for patients with leptomeningeal metastasis from solid tumors across Europe. J Neuro Oncol. (2017) 133:419–27. 10.1007/s11060-017-2452-6 [DOI] [PubMed] [Google Scholar]
- 89.Le Rhun E, Devos P, Boulanger T, Smits M, Brandsma D, Ruda R, et al. The RANO Leptomeningeal Metastasis Group proposal to assess response to treatment: lack of feasibility and clinical utility and a revised proposal. Neuro Oncol. (2019) 21:648–58. 10.1093/neuonc/noz024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.National Comprehensive Cancer Network Central Nervous System Cancers. (2019). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/cns.pdf (cited July, 2019).
- 91.Thomas KH, Ramirez RA. Leptomeningeal disease and the evolving role of molecular targeted therapy and immunotherapy. Ochsner J. (2017) 17:362–78. [PMC free article] [PubMed] [Google Scholar]
- 92.Prabhu RS, Turner BE, Asher AL, Marcrom SR, Fiveash JB, Foreman PM, et al. A Multi-Institutional analysis of presentation and outcomes for leptomeningeal disease recurrence after surgical resection and radiosurgery for brain metastases. Neuro Oncol. (2019) 21:noz049 10.1093/neuonc/noz049 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.