

Abstract
Objectives:
The misuse of prescription drugs in the U.S. is an alarming public health crisis. Prior research at the U.S.-Mexico border has found high rates of prescription drug misuse, but with rates varying significantly across border communities. We aimed to examine a model of permissive climate measures and stress exposures as potential mediators of community differences in prescription drug misuse at the U.S.-Mexico border.
Design:
We analyzed data from the U.S.-Mexico Study of Alcohol and Related Conditions (UMSARC). Household, in-person interviews were conducted with Mexican-origin residents of the Texas border cities Laredo (n=751) and Brownsville/McAllen (n=814). Interviews assessed past-year misuse of any and pain-reliever prescription drugs. Drug availability, neighborhood safety, exposure to violence/crime, and social support were examined as potential mediators. Analyses were stratified by gender and employed regressions and mediation analysis with Mplus.
Results:
The past-year prevalence of any prescription drug misuse in Laredo was 26.3% among women and 24.4% among men, and in Brownsville/McAllen was 12.4% among men, and 6.7% among women. Mediation analysis revealed site effects via some of the hypothesized risk factors for men, but not for women. Specifically, for men, site effects on any and pain reliever prescription drug misuse were partially mediated via high drug availability and low family support.
Conclusions:
Past-year prescription drug misuse was over 3 times the 2015 national prevalence among both men and women in Laredo and calls for immediate attention. Findings regarding the model suggest drug availability and social support may be relevant to understanding community differences in prescription drug misuse among men living at the border, and that additional factors should be investigated to understand misuse among women living at the border.
Keywords: prescription drug misuse, U.S.-Mexico border, Mexican-Americans, mediation modeling
INTRODUCTION
The misuse of prescription drugs in the U.S., including opioid pain relievers, tranquilizers, sedatives, and stimulants (Compton & Volkow, 2006; A. W. Hughes, MR; Lipari, RN; Bose J; Copello, EAP; Kroutil, LA, 2016), is an alarming and escalating public health crisis. The 2015 National Survey on Drug Use and Health (NSDUH) defines prescription drug misuse as “the use of prescription drugs in any way that a doctor did not direct” (A. W. Hughes, MR; Lipari, RN; Bose J; Copello, EAP; Kroutil, LA, 2016). According to the 2015 NSDUH, 18.9 million Americans aged 12 or older engaged in the past-year misuse of prescription drugs, of which 12.5 million had misused pain relievers (A. W. Hughes, MR; Lipari, RN; Bose J; Copello, EAP; Kroutil, LA, 2016). Prescription pain relievers are now one of the most commonly initiated drugs, with approximately 2.1 million initiates per year, second only to marijuana (Center for Behavioral Health Statistics and Quality, 2016; A. W. Hughes, MR; Lipari, RN; Bose J; Copello, EAP; Kroutil, LA, 2016). As the prescription opioid epidemic in the U.S. has made clear, the consequences of prescription drug misuse are severe, including prescription drug dependence (Compton & Volkow, 2006; Saha et al., 2016), drug (Michael, William Klugh, & Gaylord, 2014) and alcohol (Castle, Dong, Haughwout, & White, 2016) interactions, neonatal abstinence syndrome (Creanga et al., 2012); transitions to injection drug use with consequent infections (e.g. – hepatitis C, HIV) (Jones, 2013; Muhuri, 2013; Pollini et al., 2011); falls, and fractures among older adults (Miller, Sturmer, Azrael, Levin, & Solomon, 2011; Rolita, Spegman, Tang, & Cronstein, 2013); cognitive impairment (Tannenbaum, Paquette, Hilmer, Holroyd-Leduc, & Carnahan, 2012); and fatal overdoses (Rudd, Seth, David, & Scholl, 2016).
The phenomenon of “drug tourism”, whereby U.S. residents travel to Mexico to obtain inexpensive prescription medications (de Guzman, Khaleghi, Riffenberg, & Clark, 2007; Rivera, Ortiz, & Cardenas, 2009), enhances access to a variety of prescription drugs for recreational purposes. Drug tourism is prominent at the U.S.-Mexico border, where rates of drug-related violence and unemployment are remarkably high, and which includes some of the poorest counties in the nation (Lee et al., 2013). While immigration from Mexico to the U.S. has declined since the 2007–2009 Great Recession (Gonzalez-Barrera, 2015), the U.S.-Mexico border region also continues to have the highest concentration of Mexican-origin individuals in the United States. Few studies have investigated prescription drug misuse in border communities, especially those comprised largely of Mexican-origin individuals. Given the devastation of the prescription opioid epidemic and the ease of access to prescription drugs at the U.S.-Mexico border, this is an important setting within which to examine prescription drug misuse.
Some studies have already documented the misuse of prescription drugs in US-Mexico border communities. A 2013 study among Latino college students at a U.S. university located on the U.S.-Mexico border reported a lifetime prevalence of 14% for any prescription drug use without a prescription, with opiate analgesics the most commonly reported prescription drug (5.5%) (Cabriales, Cooper, & Taylor, 2013). Another study that examined unintentional drug overdose deaths in New Mexico between 2005 and 2009 observed that deaths that occurred in border counties were more often from prescription opioids compared to off-border deaths (Shah, Lathrop, Flores, & Landen, 2012). These studies from the U.S.-Mexico border focused on special populations (i.e. – college students and overdose deaths) and were thus limited in their applicability to the general population of Mexican-origin people living in the U.S.-Mexico border region. In examining population-based, national U.S. studies, we observe high rates of prescription drug misuse among Latinos. Data from the 2001–2002 National Epidemiologic Survey of Alcohol and Related Conditions (NESARC) showed 3 times higher odds of past year prescription drug misuse among Latino adults aged 65 or older compared to Whites (Moore et al., 2009). Data from the most recent NESARC (2012–2013) among adults aged 18 and above revealed a past-year prevalence of nonmedical prescription opioid use of 4.3% among Whites and 3.3% among Latinos (Saha et al., 2016). More recent data from the 2015 NSDUH show that Latinos and Whites aged 12 or older have comparable rates of past-year pain reliever drug misuse, with Whites at 5.0% vs 4.8% among Latinos (A. Hughes, Williams, M.R., Lipari, R.N., Bose, J., Copello, E.A.P., Kroutil, L.A., 2016).
Going beyond the descriptions of prescription drug misuse among racial/ethnic groups noted above, much work has gone into understanding the psychosocial (Cabriales et al., 2013; Wang, Becker, & Fiellin, 2013) and sociodemographic (Havens et al., 2007; Paulozzi & Xi, 2008; Rosenblum et al., 2007; Wang et al., 2013; Wunsch, Nakamoto, Behonick, & Massello, 2009; Young, Havens, & Leukefeld, 2012) correlates of prescription drug misuse and physician’s prescribing drug practices (Curtis et al., 2006; McDonald, Carlson, & Izrael, 2012; Paulozzi, Strickler, Kreiner, & Koris, 2015). However, fewer studies have investigated geographic differences in prescription drug misuse. Of the studies that have focused on this issue, many have examined variation between urban and rural settings (Havens et al., 2007; Rosenblum et al., 2007; Young et al., 2012), where residents often differ on sociodemographic characteristics. A recent analysis of data from the U.S.-Mexico Study of Alcohol and Related Conditions (UMSARC) compared the prevalence of illicit and prescription drug use and misuse on both sides of the U.S.-Mexico border and found marked differences in prescription drug misuse between the two Texas border sites of Laredo and Brownsville/McAllen (Borges et al., 2018). Specifically, a past 12-month prevalence of any prescription drug misuse of 25.4% was found in Laredo compared to 9.4% in Brownsville/McAllen. Moreover, no differences in sociodemographic characteristics were found for men between the two study sites (Zemore et al., 2016). According to the 2013 Census, both Laredo and Brownsville/McAllen are predominantly Mexican-origin (78 to 87%), and in 2013 were located in the top 3 poorest counties in the United States (U.S. Census Bureau, 2013). Taken together, a lack of sociodemographic differences between the populations of Laredo and Brownsville/McAllen suggests that other factors are at play in the marked difference in the prevalence of prescription drug misuse among people of Mexican-origin living in these border communities.
Earlier analysis of the UMSARC data to identify factors explaining the higher prevalence of past-year alcohol use disorder (AUD) in Laredo compared to Brownsville/McAllen found indicators of permissive climate (i.e., permissive drinking norms, high drug availability) and stress exposures (i.e., high exposure to violence/crime, low family support) as partial mediators of the effect of study site on differences in the prevalence of alcohol use disorder (Zemore et al., 2016). Building on this we developed a model to understand variation in prescription drug misuse at the U.S.-Mexico border. This model was informed by Valdez’s theoretical work on drug use among border populations (A. Valdez, 1993), which highlights roles for cultural permissiveness and rampant crime in drug use at the border, and also by a stress-and-coping perspective that acknowledges the potential for perceived stress exposures to increase prescription drug misuse as a coping mechanism (Pearlin, Menaghan, Lieberman, & Mullan, 1981; Pearlin, Schieman, Fazio, & Meersman, 2005). The model proposes that high perceived drug availability as a measure of permissive climate, and low perceived neighborhood safety, exposure to violence/crime, and low family support as measures of perceived stress exposures, can partially explain the differences in prescription drug misuse between Laredo and Brownsville/McAllen (see Figure 1, Conceptual Model). Unlike the previous work noted above, permissive drinking norms were not included in the current model because of its specificity to alcohol use, and perceived neighborhood safety was added to address the postulated influence of stressful environments on prescription drug misuse (Keyes, Cerdá, Brady, Havens, & Galea, 2014). By examining this proposed conceptual model we aim to identify potential drivers of the heterogeneity in prescription drug misuse at the U.S.-Mexico border. Doing so can allow us to understand differences in prescription drug misuse across geographic locations with seemingly similar population characteristics, and apply this understanding to improving efforts to prevent and address prescription drug misuse.
Fig. 1.
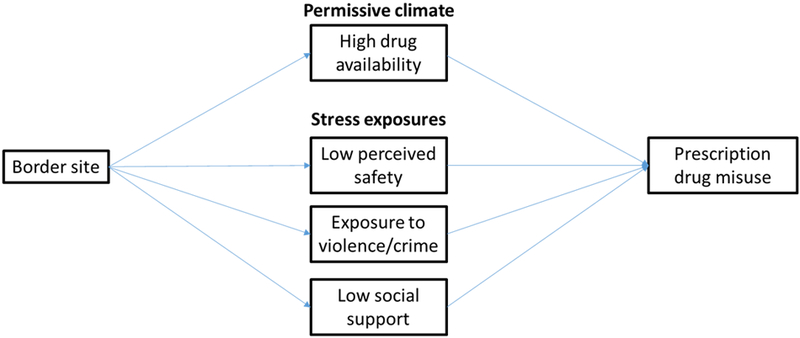
Conceptual model
MATERIALS AND METHODS
Data
Data analyzed here are from the U.S.-Mexico Study of Alcohol and Related Conditions. UMSARC is an epidemiological study conducted among Mexican-origin participants, aged 18–65, living in 2 pairs of sister metropolitan areas (“sister cities”) and 1 adjacent non-border metropolitan area on each side of the Texas-Mexico border (N=4,796). Included in analyses here are data on 751 respondents living in Laredo, Texas and 814 respondents living in Brownsville/McAllen, Texas. Both Laredo and Brownsville/McAllen are medium-sized metropolitan areas, and both are connected via multiple international bridges to their respective Mexican sister cities.
During 2011 to 2013, household in-person interviews were conducted using multistage area-probability sampling with stratification by city. In the U.S., primary sampling units (PSUs) were defined as census block groups with ≥70% Latino population; blocks served as the secondary sampling units (SSUs). Three households per SSU (9 per PSU) were randomly selected and screened for eligible residents (i.e., aged 18 to 65, Mexican origin). Eligible residents were then enumerated and a respondent selected using the last-birthday technique. Interviews were conducted by extensively trained interviewers in English and Spanish, and lasted ~45 minutes. On the U.S. side, the combined cooperation rate was 84% (with a 53% overall response rate; 66% for Laredo, and 45% for Brownsville/McAllen), AAPOR version 4 (The American Association for Public Opinion Research, 2011). For more, see Cherpitel and colleagues (C. J. Cherpitel et al., 2015).
Measures
Indicators of a permissive climate.
Perceived drug availability was assessed with a 2-item scale asking whether the respondent had been approached by someone wishing to sell drugs in the past 30 days, and whether the respondent had seen drug deals in the past 12 months (Pearson r = 0.37).
Perceived stress exposures.
Perceived safety was measured using a 2-item scale assessing perceived safety of walking in the neighborhood during the day and at night (Ruston & Akinrodoye, 2002). The questions were “How safe do you feel walking alone in your neighborhood during the daytime/after dark?”. Exposure to violence/crime was measured using a 7-item scale (Martinez & Richters, 1993; Richters & Martinez, 1992). Respondents were asked whether they had heard gunshots, seen somebody beaten up, seen somebody stabbed, seen somebody shot, seen someone pull a gun on someone else, seen violence related to drug dealing/gangs, or seen somebody arrested in the prior 12 months. Although the original scale includes an eighth item on witnessing drug deals, this item was used to separately assess drug availability (see above; 7-item α = 0.71). Social support was measured using the widely used and well-validated Multidimensional Scale of Perceived Social Support (Zimet, Dahlem, Zimet, & Farley, 1988), which separately measures support from a significant other, family, and friends with 4 items each (α’s = 0.90 to 0.93).
Prescription drug misuse variables.
Prescription drug misuse was assessed with a question asking respondents if they “used prescription drugs that were not prescribed or that were not taken as prescribed” over the previous 12 months, including pain relievers, sedatives, stimulants, and “other” prescription drugs. We constructed a variable indicating “any” prescription drug misuse if the respondent answered “yes” for any of the prescription drug categories. We used any prescription drug misuse and prescription pain reliever misuse as the two main outcome measures.
Additional variables.
Basic demographic variables included gender, age, marital status, and occupation. Although in prior analysis noted above, SES measures including income, education, and employment status, were not found to vary for men between Laredo and Brownsville/McAllen, differences were not examined for women. Given previous work showing an association between high cross-border mobility and worse alcohol and drug problems (Cherpitel, Ye, Zemore, Bond, & Borges, 2015), we also examined the lifetime frequency of visits to Mexico and any travel to Mexico in the past 12 months. Additionally, we examined age of immigration as previous work has shown it to be associated with alcohol problems and drug use (Cherpitel, Li, Borges, & Zemore, 2017). The age of immigration variable was comprised of the categories “less than 12 years old”, “12–20 years old”, and “21+” and included US born participants in the first category.
Analysis.
Preliminary analyses examined bivariate associations between study site and each outcome using chi-square tests of independence. Specifically, we examined bivariate associations between study site and past 12-month prevalence of any prescription drug misuse and pain reliever drug misuse, separately by gender; to confirm gender differences, we also tested the interaction between gender and site in predicting both outcomes, and stratified analyses by gender when confirmed. We then examined sociodemographic (i.e., age, marital status) and sociocultural (i.e., age of immigration, cross-border mobility) characteristics by study site and both outcomes to contextualize site effects and identify potential confounders. Finally, we examined bivariate associations between measures of the proposed mediators (i.e., permissive climate and stress exposures) and study site and both outcomes. A p-value < 0.05 was used throughout to establish significance.
To test our overall conceptual model we used structural equation modeling (SEM). Modifications to the initial model were informed by preliminary analyses, model fit statistics, modification indices, theory, and plausibility (Byrne, Shavelson, & Muthén, 1989). More specifically, preliminary analyses determined which mediators and covariates to include in the final model based on statistical significance (p<0.05) and directions of associations between the predictor (site) and outcome (prescription drug misuse) variables. Construction of the model based on results from preliminary analyses and the other considerations of fit indices, plausibility, and theory are recommended to ensure the hypothesized model can be adequately tested by the available data (B. O. Muthén, Muthén, & Asparouhov, 2016).
Because the main outcomes (any past 12-month prescription drug misuse and past 12-month prescription pain reliever misuse) were dichotomous (yes vs. no), we used robust weighted least squares (RWLS) estimation. We chose this estimation procedure because it provides fit indices to evaluate model fit, which maximum-likelihood estimation (the second most commonly used estimation for models with a binary outcome after RWLS) does not provide(B. O. Muthén et al., 2016). This is the preferred estimation technique for dichotomous outcomes (Beauducel & Herzberg, 2006). We conducted analyses separately for each outcome.
Statistical mediation was explored using Mplus’ “model indirect” command syntax. This command requests the indirect effects and their standard errors between predictor and outcome variables via a mediator. It allows for the simultaneous modeling of several related regression equations, and can include weighting and clustering variables, and is thus appropriate for multiple mediation modeling with complex survey data. All analyses, with the exception of the SEM, were conducted using Stata version 15 (StataCorp., 2017); the SEM was implemented in Mplus, version 7 (L. Muthén & Muthén, 2013). All analyses accounted for the complex survey designby including both data weighting and clustering variables in the command syntax The weight variable was constructed as a post-stratification sampling weight adjustment for age, sex, and education of the cities sampled, and the clustering variable indicated the primary sampling units based on block group identifiers.
RESULTS
Associations between study site and prescription drug misuse outcomes
Figure 2 shows the prevalence of past 12-month misuse of any prescription drug and past 12-month misuse of prescription pain relievers for each study site by gender. For both measures of prescription drug misuse, Laredo shows statistically significantly higher levels of misuse than Brownsville/McAllen within each gender. The prevalence of past 12-month use of any prescription drug among men was almost twice as high in Laredo compared to Brownsville/McAllen, 24.4% vs. 12.4%. Among women, it was almost 4 times as high, where the prevalence was 26.3% in Laredo compared to 6.7% in Brownsville/McAllen. Similar gender differences were found for past 12-month prescription pain reliever misuse. Logistic regressions for each outcome with gender, site, and their interaction as predictors found a significant interaction effect (p < 0.05; data not shown), confirming these gender differences. We therefore stratified the remaining analyses by gender.
Fig. 2.
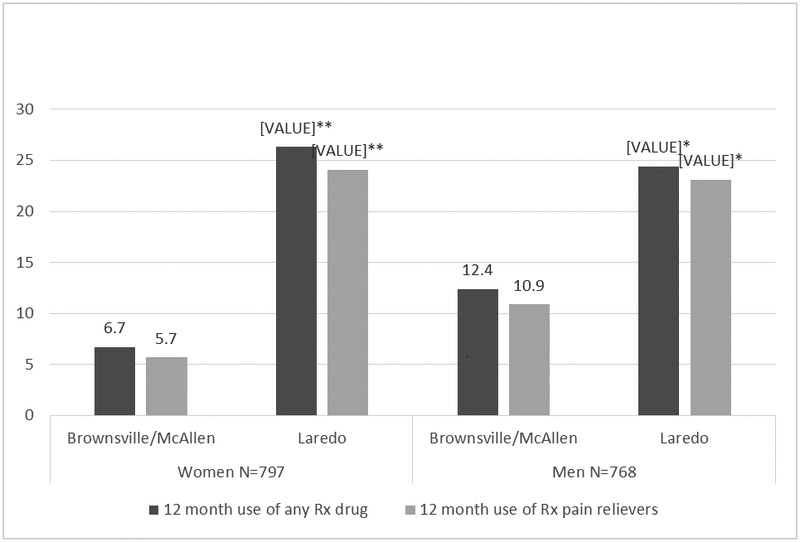
Prevalence rates of prescription drug misuse across study sites by gender
Note: Comparison between Laredo and Brownsville/McAllen
**p<0.000
*p<0.01
Associations between study site and sociodemographic and sociocultural characteristics
Table 1 shows associations between study site and sociodemographic and sociocultural characteristics by gender. Among men there were no differences between Laredo and Brownsville/McAllen on sociodemographic characteristics. On the other hand, among women, residents of Laredo were generally higher on SES measures than residents of Brownsville/McAllen: fewer Laredan women reported incomes less than $15,000 a year, and more had a full-time occupation. Among both men and women in Laredo, a higher proportion immigrated before 12 years of age and had more than 100 visits to Mexico in their lifetime compared to Brownsville/McAllen. No difference was found between Laredo and Brownsville/McAllen for either men or women in the proportion of any past 12-month travel to Mexico.
Table 1.
Sociodemographic & sociocultural characteristics by study site by gender
| Women n=797 | Men n=768 | |||
|---|---|---|---|---|
| Sociodemographic characteristics | Laredo | Brownsville/McAllen | Laredo | Brownsville/McAllen |
| n=389 | n=408 | n=362 | n=406 | |
| n (%) | n (%) | n (%) | n (%) | |
| Age in years, mean (SE) | 39.2 (0.44) | 38.3 (0.63) | 37.4 (0.46) | 38.5 (0.71) |
| Highest education completed | ||||
| Some high school | 129 (36.1) | 162 (41.8) | 138 (37.8) | 124 (29.8) |
| High school/some college | 190 (38.8) | 161 (31.4) | 171 (40.1) | 212 (45.0) |
| College/graduate school | 70 (25.1) | 83 (26.8) | 53 (22.1) | 70 (25.3) |
| Income | ||||
| <15,000/year | 100 (27.3) | 162 (41.3)*** | 83 (21.4) | 109 (25.6) |
| $15,001 to $30,000 | 126 (32.1) | 92 (24.5) | 116 (31.5) | 109 (26.8) |
| $30,001 to $60,000 | 94 (26.7) | 73 (22.0) | 95 (28.3) | 106 (30.3) |
| $60,001 plus | 43 (13.9) | 41 (12.2) | 45 (18.9) | 52 (17.4) |
| Employment | ||||
| Employed | 251 (65.8) | 208 (52.3)*** | 278 (76.5) | 301 (75.5) |
| Unemployed | 28 (5.1) | 54 (15.0) | 35 (9.0) | 48 (9.7) |
| Other | 110 (29.2) | 146 (32.8) | 49 (14.5) | 57 (14.9) |
| Occupation | ||||
| Full time occupation | 156 (41.5) | 122 (30.6)*** | 187 (55.3) | 215 (52.4) |
| Part time or seasonal | 91 (23.5) | 86 (21.7) | 89 (20.7) | 83 (22.2) |
| Other | 142 (35.0) | 200 (47.8) | 86 (24.0) | 108 (25.4) |
| Marital Status | ||||
| Never married | 95 (23.4) | 116 (26.1) | 125 (30.8) | 118 (28.3) |
| Married/living with partner | 213 (58.3) | 204 (51.5) | 192 (57.1) | 237 (61.6) |
| Separated/divorced/widowed | 81 (18.3) | 88 (22.4) | 45 (12.1) | 51 (10.1) |
| Age of immigration | ||||
| <12 years old | 312 (74.2) | 276 (66.0)** | 301 (81.8) | 311 (72.1)*** |
| 12-20 years old | 36 (12.3) | 74 (19.4) | 34 (11.2) | 46 (11.4) |
| 21+ years old | 40 (13.5) | 57 (14.7) | 26 (7.0) | 49 (16.5) |
| Lifetime travel to Mexico | ||||
| Never visited Mexico | 37 (9.0) | 13 (2.4) | 43 (12.4) | 13 (3.2) |
| Been to Mexico <100 times | 136 (34.0) | 206 (48.5) | 121 (31.9) | 214 (48.6) |
| Been to Mexico >100 times | 214 (57.0) | 185 (49.1)*** | 195 (55.7) | 179 (48.2)*** |
| Any past 12 mo. travel to Mexico | 140 (39.8) | 180 (46.2) | 124 (33.6) | 140 (40.1) |
p≤0.001,
p≤0.01,
p≤0.05
Associations between study site and potential mediators
Table 2 shows the associations between study site and the potential mediators of permissive climate and stress exposures by gender. Among both men and women, perceived drug availability and exposure to violence/crime were higher in Laredo compared to Brownsville/McAllen, and perceived safety was lower in Laredo than in Brownsville/McAllen. Measures of social support differed for men and women and across study site; among both men and women, support from a friend was higher in Laredo than Brownsville/McAllen. However, support from a significant other and from family did not differ statistically among women across study site, whereas among men support from a significant other and from family were significantly lower in Laredo compared to Brownsville/McAllen.
Table 2.
Associations between study site and potential mediators by gender
| Women n=797 | Men n=768 | |||
|---|---|---|---|---|
| Risk factors mean(SE) |
Laredo N=389 |
Brownsville/McAllen N=408 |
Laredo N=362 |
Brownsville/McAllen N=406 |
| Permissive climate | ||||
| Perceived drug availability | 0.14 (0.01) | 0.07 (0.01)*** | 0.27 (0.01) | 0.10 (0.01)*** |
| Perceived safety | 3.1 (0.04) | 3.2 (0.05)** | 3.3 (0.03) | 3.7 (0.04)*** |
| Stress exposures | ||||
| Exposure to violence/crime Social support | 0.20 (0.01) | 0.09 (0.01)*** | 0.26 (0.01) | 0.11 (0.01)*** |
| Significant other support | 4.5 (0.03) | 4.6 (0.04) | 4.3 (0.03) | 4.5 (0.04)*** |
| Family support | 4.5 (0.03) | 4.5 (0.04) | 4.2 (0.03) | 4.5 (0.04)*** |
| Friend support | 4.3 (0.03) | 4.1 (0.05)** | 4.0 (0.03) | 3.8 (0.06)* |
p≤0.001,
p≤0.01,
p≤0.05
Associations between potential mediators and prescription drug misuse outcomes
Table 3 shows the associations between each outcome and measures of permissive climate and stress exposures. Among both men and women, a higher level of perceived drug availability was associated with both outcomes. Among men, a lower level of perceived safety was associated with both outcomes, whereas among women it was only associated with any past-12 month prescription drug misuse. A higher level of being exposed to violence or crime was significantly associated with both outcomes among women, whereas among men it was associated with any prescription drug use only. Lower levels of all forms of social support, that is, from a significant other, family member, and friend, were associated with both outcomes among men. Among women, lower levels of support only from a significant other and family were associated with both outcomes.
Table 3.
Associations between potential mediators and prescription drug outcomes by gender
| Women n=797 | Men n=768 | |||||||
|---|---|---|---|---|---|---|---|---|
| Potential mediators | Pain reliever | Any Rx | Pain reliever | Any Rx | ||||
| Mean (SE) | No n=683 | Yes n=114 | No n=667 | Yes n=130 | No n=637 | Yes n=131 | No n=625 | Yes n=143 |
| Permissive climate | ||||||||
| Perceived drug availability | 0.09 (0.01) | 0.16 (0.02)*** | 0.09 (0.01) | 0.16 (0.02)*** | 0.17 (0.01) | 0.26 (0.02)*** | 0.17 (0.01) | 0.26 (0.02)*** |
| Perceived safety | 3.17 (0.04) | 3.04 (0.06) | 3.18 (0.04) | 2.99 (0.06)** | 3.52 (0.03) | 3.34 (0.07)** | 3.52 (0.03) | 3.35 (0.07)** |
| Stress exposures | ||||||||
| Exposure to violence/crime Social support | 0.12 (0.01) | 0.22 (0.02)*** | 0.12 (0.01) | 0.21 (0.02)*** | 018 (0.01) | 021 (0.02) | 0.18 (0.01) | 0.21 (0.02)* |
| Significant other support | 4.59 (0.02) | 4.44 (0.07)* | 4.59 (0.02) | 4.44 (0.07)* | 4.48 (0.03) | 4.22 (0.06)*** | 4.48 (0.03) | 4.23 (0.06)*** |
| Family support | 4.53 (0.02) | 4.32 (0.07)** | 4.53 (0.02) | 4.33 (0.07)** | 4.45 (0.03) | 4.06 (0.05)*** | 4.45 (0.03) | 4.09 (0.05)*** |
| Friend support | 4.19 (0.03) | 4.18 (0.07) | 4.18 (0.03) | 4.20 (0.06) | 3.94 (0.04) | 3.70 (0.05)*** | 3.94 (0.05) | 3.75 (0.05)** |
p≤0.001,
p≤0.01,
p≤0.05
Test of the conceptual model
Based on the results of the preliminary analyses described above, we used structural equation modeling to test our conceptual model for each prescription drug misuse outcome, separately for women and men. We excluded potential mediators that did not differ by site as expected or were not strongly associated with both site and prescription drug misuse outcomes, which were perceived safety and the social support variables for women, and exposure to violence/crime for men. Additionally for women we excluded income as a covariate because it was associated with site and the outcomes in different directions, and age of immigration because it was not associated with either of the outcomes. For men, we limited the social support variables to family support because it was the most strongly associated with outcomes of the three social support variables. In the final models for women, for both outcomes, we examined drug availability and exposure to violence/crime as potential mediators controlling for education; the model for pain reliever drug misuse also controlled for lifetime travel to Mexico. For men, the models for both outcomes examined drug availability, perceived safety, and family support as potential mediators controlling for education, occupation, marital status, and age of immigration.
Figure 3 shows the final model for any prescription drug misuse for men adjusting for demographic variables (and trimming). This model achieved acceptable model fit (see Figure 3 legend) and supported parts of the hypothesized model. Indirect effects from site to any prescription drug misuse were statistically significant for perceived drug availability (p=0.034) and family support (p=0.032), but not for perceived safety (p=0.563). The model for pain reliever misuse likewise achieved acceptable model fit. Our hypothesized pathways were supported only insofar as indirect effects from site to pain reliever misuse were statistically significant for family support (p=0.022); indirect effects were not statistically significant for perceived safety (p=0.506), and only approached statistical significance for high perceived drug availability (p=0.069).
Fig. 3.
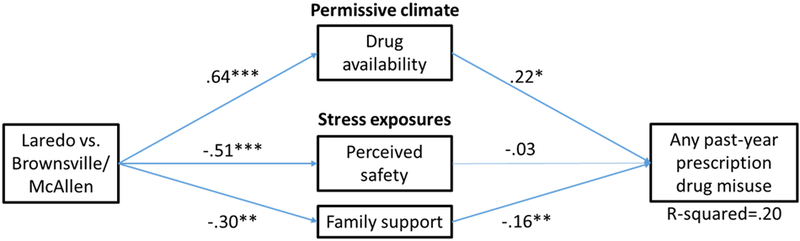
Adjusted structural equation model of site effects on any prescription drug misuse among men only. Notes. ***p<0.001, **p<0.01, *p<0.05. Significant pathways bolded. Model fit statistics: χ2(df=9, N=767)=10.5, p=0.31, comparative fit index (CFI) = 0.99, Tucker Lewis Index (TLI) = 0.95, root mean square error of approximation (RMSEA) = 0.02 (0.00,0.045). Each pathway adjusted for education, occupation, marital status, and age of immigration; non-significant covariates trimmed.
The models for both prescription drug misuse outcomes among women did not support the hypothesized model whereby the effects of site on prescription drug misuse were mediated by drug availability and exposure to violence/crime. While the models for both outcomes achieved acceptable model fit indicating that the models were able to adequately represent the data, the specific indirect effects between the main predictor (site) via the mediators on the outcomes were not statistically significant. This occurred even though the individual paths between predictor and mediator, and mediator and outcome were statistically significant, as suggested by preliminary analyses, but the test for significance over both paths was not. Specifically, for any prescription drug misuse, the indirect effects via high perceived drug availability and exposure to violence were not statistically significant (p= 0.293 and p=0.731, respectively). Similarly, indirect effects via high perceived drug availability and exposure to violence were not statistically significant for pain reliever drug misuse (p= 0.337 and p=0.839, respectively).
DISCUSSION
This analysis aimed to describe differences in prescription drug misuse across US-Mexico border sites by gender and to identify factors that could partially explain the marked difference in prescription drug misuse between those sites. We tested a conceptual model suggesting permissive climate and stress exposures link study site to the higher prevalence of prescription drug misuse in Laredo compared to Brownsville/McAllen, separately for men and women. For men, we observed partial support for the model, where indirect effects were significant for perceived drug availability and family support for any past-year prescription drug misuse. For any pain reliever misuse among men, a significant indirect effect via family support only was found. We found that this model did not hold among women for either past-year misuse of any prescription drug or pain relievers, as no significant indirect effects via any of the proposed mediators were observed. However, a main effect of site on prescription drug misuse outcomes was observed for both men and women.
A higher prevalence of prescription drug misuse among both men and women in Laredo compared to Brownsville/McAllen extends previous work that did not disaggregate by gender and showed a higher prevalence of prescription drug misuse among Laredo’s total population (Borges et al., 2018). Interestingly, this finding is in contrast to other work showing no differences in AUD among women between Laredo and Brownsville/McAllen, but indeed showing higher rates of AUD in Laredo among men (Zemore et al., 2016). This contrast was surprising given that heavy alcohol use and drug use are frequently co-occurring and often have similar risk factors. Further, prescription drug misuse among women was 4 times higher in Laredo compared to Brownsville/McAllen while only 2 times higher among men. This suggests that Laredo’s environment has a stronger effect on prescription drug misuse among women than men when compared to Brownsville/McAllen. Aspects of Laredo’s environment, such as access to prescription drugs or social norms towards prescription drug use and misuse, may be differentially impacting men and women. It is worth noting that the UMSARC definition of prescription drug misuse included the use of prescription drugs that were “not prescribed”. Given the phenomenon of “drug tourism” at the border, it is possible that this measure is capturing the purchase of prescription drugs in Mexico without a prescription; perhaps by chronically ill, uninsured individuals for medications previously recommended by a physician (Homedes, 2013). However, pain relievers were the most commonly misused prescription drug in this sample (data not shown), suggesting pain reliever misuse is driving the high rate of any prescription drug misuse, which is cause for concern given the highly additive quality of these drugs. Overall, the observation that over a quarter of women and nearly a quarter of men in Laredo misused prescription drugs in the past year, which is over 3 times higher than the national prevalence (7.1%), underscores the dire need for work in this area to address the current high levels of prescription drug misuse and to prevent misuse from occurring.
The proposed model was partially supported among men in this sample, insofar as drug availability and family support showed significant indirect effects for any prescription drug misuse. Keyes et al postulated drug availability and social network connections as important factors at the macro and local context level, respectively, to consider when trying to understand urban-rural differences in prescription drug misuse (Keyes et al., 2014), and these factors were borne out in this analysis. While our measure of drug availability did not specify prescription drugs, it may be an indicator of ease of access to prescription drugs outside the pharmacy, and/or an indicator of polydrug use among those misusing prescription drugs. Indeed, among men in Laredo who reported past-year prescription drug misuse, 29.4% also reported using 2 or more illicit drugs in the past 12 months. Findings for low family support are consistent with those of our previous work, which identified low family support as a risk factor for AUD among men in Laredo. That family support was a factor in prescription drug misuse use and AUD for Mexican-origin men may be related to the salience of the concept of familia in Mexican culture (Zinn, 1982). Further work is needed to understand why men in Laredo may be experiencing low family support and how it is associated with prescription drug misuse. Providing services to promote community and a sense of belonging among Mexican-origin men living in Laredo may be an important component of interventions to reduce and prevent prescription drug misuse in this area.
Our model to explain the variation in prescription drug misuse did not hold among women, and this suggests other risk factors are at play in the higher prevalence of prescription drug misuse among women in Laredo compared to women in Brownsville/McAllen. However, while the risk factors we examined might not be relevant for explaining site differences in prescription drug misuse among women, they may be relevant for understanding prescription drug misuse generally among Mexican-American women in this region. For example, we observed a significant association between a lower level of social support from a significant other/family member and prescription drug misuse among women, and future work may want to consider social support in their models.
For Laredan women, prescription drug misuse may be a coping strategy for traumas more often experienced by women than men, such as domestic violence. In Laredo, recorded homicides in recent years were overwhelmingly domestic violence related, and securing funding for domestic violence prevention programs was part of the city’s 2017 legislative agenda (Laredo, 2017). Other contextual factors not investigated in this study may also be pertinent to the high prevalence of prescription drug misuse among Lareden women, such as how and where prescription drugs are being procured. The UMSARC survey asked about reasons for traveling to Mexico in the past year, with a significantly higher proportion of women in Laredo vs. Brownsville/McAllen reporting that they did so to purchase over-the-counter and prescription medications (data not shown). However, the cell sizes were very small so this observation should be noted with caution. Given the very high rate of prescription drug misuse among Lareden women, further work is required to identify associated factors that can inform efforts to address the alarmingly high rate of misuse.
There are notable limitations associated with the current study that warrant mention and suggest caution when interpreting the above results. First, UMSARC collected data in Texas only. As defined by the U.S.-Mexico Border Health Association, the U.S.-Mexico border region stretches across approximately 2,000 miles over 4 U.S. states and includes 25 counties (Driessen & de Cosío, 1995). Therefore, the extent to which the differences in prescription drug misuse between Laredo and Brownsville/McAllen would be observed between other parts of the U.S.-Mexico border cannot be determined from the current data. It may be that Laredo is a unique case in the region for high prescription drug misuse, or that Brownsville/McAllen is a uniquely low risk area for prescription drug misuse. Relatedly, the results we obtained regarding the examined risk factors may not be generalizable to the U.S.-Mexico border area as a whole. Second, the UMSARC is a cross-sectional study and we can therefore not make any causal inferences regarding the relationship between the examined risk factors and prescription drug misuse. Third, we did not query participants about the circumstances of their prescription drug misuse, such as why they initially started using prescription drugs, and the length and severity of their misuse. Further, the overlap and extent to which residents of the U.S. Mexico border region are procuring prescription drugs on the black market in the U.S., at American pharmacies, or at Mexican pharmacies should be investigated to develop targeted interventions, particularly in light of historical loopholes in U.S. Customs laws (A. Valdez, Sifaneck, S.J., 1997). Similarly, we did not assess whether or not participants who were immigrants had legal status, which could have limited the identification of factors associated with site differences in prescription drug-misuse given findings that undocumented immigration is associated with reductions in drug and alcohol problems (Light, Miller, & Kelly, 2017). Finally, this study also did not measure variables at the community level that could have provided less subjective measures of perceived drug availability and perceived safety, such as local police department reports of drug-related crimes. Results may differ with these more objective, community level measures, which should be included in future research.
In conclusion, this study presents evidence showing heterogeneity at the U.S.-Mexico border in prescription drug misuse for both men and women, and the potential for drug availability and low social support to contribute to the high level of prescription drug misuse among men in Laredo and potentially other border hotspots for drug misuse. This work provides further support for differences in substance misuse among demographically similar border communities, and calls for action to address the high level of prescription drug misuse in Laredo and to examine whether there are other hotspots for prescription drug problems along the border. Additional research is needed to investigate macro-level factors related to prescription drug misuse, such as how and where prescription drugs are procured, and local-level factors, such community norms around prescription drug use. This work serves as preliminary evidence to support future work on prescription drug misuse in communities at the U.S.-Mexico border in an effort to help halt and reverse the crisis of prescription drug misuse in all segments of American society.
REFERENCES
- Beauducel Andre, & Herzberg Philipp Yorck. (2006). On the Performance of Maximum Likelihood Versus Means and Variance Adjusted Weighted Least Squares Estimation in CFA. Structural Equation Modeling: A Multidisciplinary Journal, 13(2), 186–203. doi: 10.1207/s15328007sem1302_2 [DOI] [Google Scholar]
- Borges Guilherme, Zemore Sarah E, Orozco Ricardo, Cherpitel Cheryl J, Martínez Priscilla, & Wallisch Lynn. (2018). Drug use on both sides of the US-Mexico border. 2018, 60(4, jul-ago), 11. doi: 10.21149/8603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byrne Barbara M., Shavelson Richard J., & Muthén Bengt. (1989). Testing for the equivalence of factor covariance and mean structures: the issue of partial measurement invariance. Psychological Bulletin, 105(3), 456–466. doi: 10.1037/0033-2909.105.3.456 [DOI] [Google Scholar]
- Cabriales JA, Cooper TV, & Taylor T (2013). Prescription drug misuse, illicit drug use, and their potential risk and protective correlates in a Hispanic college student sample. Exp Clin Psychopharmacol, 21(3), 235–244. doi: 10.1037/a0031973 [DOI] [PubMed] [Google Scholar]
- Castle IJ, Dong C, Haughwout SP, & White AM (2016). Emergency Department Visits for Adverse Drug Reactions Involving Alcohol: United States, 2005 to 2011. Alcohol Clin Exp Res, 40(9), 1913–1925. doi: 10.1111/acer.13167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Center for Behavioral Health Statistics and Quality. (2016). Key substance use and mental health indidcators in the United States: Results from the 2015 National Survey on Drug Use and Health. (HHS Publication No. SMA 16–4984). Retrieved from http://www.samhsa.gov/data/
- Cherpitel CJ, Ye Y, Bond J, Zemore SE, Borges G, & Greenfield TK (2015). Border effects on DSM-5 alcohol use disorders on both sides of the U.S.-Mexico border. Drug Alcohol Depend, 148, 172–179. doi: 10.1016/j.drugalcdep.2015.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cherpitel Cheryl J., Li Libo, Borges Guilherme, & Zemore Sarah E. (2017). Age at immigration and substance use and problems among males and females at the U.S.–Mexico border. Journal of Studies on Alcohol and Drugs, 78(6), 827–834. doi: 10.15288/jsad.2017.78.827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cherpitel Cheryl J., Ye Yu, Zemore Sarah E., Bond Jason, & Borges Guilherme. (2015). The effect of cross-border mobility on alcohol and drug use among Mexican-American residents living at the U.S.-Mexico border. Addictive Behaviors, 50, 28–33. doi: 10.1016/j.addbeh.2015.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton WM, & Volkow ND (2006). Major increases in opioid analgesic abuse in the United States: concerns and strategies. Drug Alcohol Depend, 81(2), 103–107. doi: 10.1016/j.drugalcdep.2005.05.009 [DOI] [PubMed] [Google Scholar]
- Creanga AA, Sabel JC, Ko JY, Wasserman CR, Shapiro-Mendoza CK, Taylor P, . . . Paulozzi LJ (2012). Maternal drug use and its effect on neonates: a population-based study in Washington State. Obstet Gynecol, 119(5), 924–933. doi: 10.1097/AOG.0b013e31824ea276 [DOI] [PubMed] [Google Scholar]
- Curtis Lesley H., Stoddard Jennifer, Radeva Jasmina I., Hutchison Steve, Dans Peter E., Wright Alan, . . . Schulman Kevin A. (2006). Geographic Variation in the Prescription of Schedule II Opioid Analgesics among Outpatients in the United States. Health Services Research, 41(3 Pt 1), 837–855. doi: 10.1111/j.1475-6773.2006.00511.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Guzman GC, Khaleghi M, Riffenberg RH, & Clark RF (2007). A survey of the use of foreign-purchased medications in a border community emergency department patient population. J Emerg Med, 33(2), 213–221. doi: 10.1016/j.jemermed.2007.02.019 [DOI] [PubMed] [Google Scholar]
- Driessen M, & de Cosío Federico Gerardo. (1995). Future Directions: Substance Abuse in the U.S.–Mexico Border Region, 1–68. Final Report submitted to the Center for Substance Abuse Prevention. El Paso, TX. [Google Scholar]
- Gonzalez-Barrera Ana. (2015). More Mexicans Leaving Than Coming to the U.S . In. Washington, DC: Pew Research Center. [Google Scholar]
- Havens JR, Oser CB, Leukefeld CG, Webster JM, Martin SS, O’Connell DJ, . . . Inciardi JA (2007). Differences in prevalence of prescription opiate misuse among rural and urban probationers. Am J Drug Alcohol Abuse, 33(2), 309–317. doi: 10.1080/00952990601175078 [DOI] [PubMed] [Google Scholar]
- Homedes N, Ugalde A . (2013). Mexican pharmacies: benefits and risks for border residents in the United States of America and Mexico. Pan American Journal of Public Health, 33(3), 196–204. [DOI] [PubMed] [Google Scholar]
- Hughes A; Williams MR; Lipari RN; Bose J; Copello EAP; Kroutil LA. (2016). Prescription Drug Use and Misuse in the United States: Results from the 2015 National Survey on Drug Use and Health. Retrieved from https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR2-2015/NSDUH-FFR2-2015.pdf
- Jones CM (2013). Heroin use and heroin use risk behaviors among nonmedical users of prescription opioid pain relievers - United States, 2002–2004 and 2008–2010. Drug Alcohol Depend, 132(1–2), 95–100. doi: 10.1016/j.drugalcdep.2013.01.007 [DOI] [PubMed] [Google Scholar]
- Keyes Katherine M., Cerdá Magdalena, Brady Joanne E., Havens Jennifer R., & Galea Sandro. (2014). Understanding the Rural–Urban Differences in Nonmedical Prescription Opioid Use and Abuse in the United States. American Journal of Public Health, 104(2), e52–e59. doi: 10.2105/ajph.2013.301709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laredo, City of. (2017). Homeland Security, Domestic Violence Prevention. Retrieved from http://www.ci.laredo.tx.us/cmo/CASS/Pres_Fed/2017/domestic.html [Google Scholar]
- Lee Erik, Wilson Christopher E., Lara-Valencia Francisco, de la Parra Carlos A., Schoik Van, Rick Patron-Soberano, Kristofer, . . . Selee Andrew. (2013). The State of the Border Report: A comprehensive analysis of the U.S.-Mexico Border [Accessed: 2014-09-04. Archived by WebCite® at http://www.webcitation.org/6SLFr9GwU]. Retrieved from Washington, DC: http://www.wilsoncenter.org/sites/default/files/mexico_state_of_border_0.pdf [Google Scholar]
- Light Michael T., Miller Ty, & Kelly Brian C. (2017). Undocumented Immigration, Drug Problems, and Driving Under the Influence in the United States, 1990–2014. American Journal of Public Health, 107(9), 1448–1454. doi: 10.2105/ajph.2017.303884 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martinez Pedro, & Richters John E. (1993). The Nimh Community Violence Project: II. Children’s Distress Symptoms Associated with Violence Exposure. Psychiatry, 56(1), 22–35. doi: 10.1080/00332747.1993.11024618 [DOI] [PubMed] [Google Scholar]
- McDonald Douglas C., Carlson Kenneth, & Izrael David. (2012). Geographic Variation in Opioid Prescribing in the U.S. The journal of pain : official journal of the American Pain Society, 13(10), 988–996. doi: 10.1016/j.jpain.2012.07.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jann Michael, Kennedy William Klugh, & Lopez Gaylord. (2014). Benzodiazepines: A Major Component in Unintentional Prescription Drug Overdoses With Opioid Analgesics. Journal of Pharmacy Practice, 27(1), 5–16. doi: 10.1177/0897190013515001 [DOI] [PubMed] [Google Scholar]
- Miller M, Sturmer T, Azrael D, Levin R, & Solomon DH (2011). Opioid analgesics and the risk of fractures in older adults with arthritis. J Am Geriatr Soc, 59(3), 430–438. doi: 10.1111/j.1532-5415.2011.03318.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore AA, Karno MP, Grella CE, Lin JC, Warda U, Liao DH, & Hu P (2009). Alcohol, tobacco, and nonmedical drug use in older U.S. Adults: data from the 2001/02 national epidemiologic survey of alcohol and related conditions. J Am Geriatr Soc, 57(12), 2275–2281. doi: 10.1111/j.1532-5415.2009.02554.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muhuri PK; Gfoerere JC; Davis MC. (2013). Associations on Nonmedical Pain Reliver Usse and Inititation of Heroin Use in the Unites States. Retrieved from Rockville, MD. [Google Scholar]
- Muthén BO, Muthén LK, & Asparouhov T (2016). Regression and Mediation Analysis Using Mplus: Muthén & Muthén. [Google Scholar]
- Muthén Linda, & Muthén Bengt. (2013). Mplus User’s Guide, Version 7. Los Angeles: Muthén & Muthén. [Google Scholar]
- Paulozzi LJ, Strickler GK, Kreiner PW, & Koris CM (2015). Controlled Substance Prescribing Patterns--Prescription Behavior Surveillance System, Eight States, 2013. MMWR Surveill Summ, 64(9), 1–14. doi: 10.15585/mmwr.ss6409a1 [DOI] [PubMed] [Google Scholar]
- Paulozzi LJ, & Xi Y (2008). Recent changes in drug poisoning mortality in the United States by urban-rural status and by drug type. Pharmacoepidemiol Drug Saf, 17(10), 997–1005. doi: 10.1002/pds.1626 [DOI] [PubMed] [Google Scholar]
- Pearlin Leonard I., Menaghan Elizabeth G., Lieberman Morton A., & Mullan Joseph T. (1981). The stress process. Journal of Health and Social Behavior, 22(4), 337–356. [PubMed] [Google Scholar]
- Pearlin Leonard I., Schieman Scott, Fazio Elena M., & Meersman Stephan C. (2005). Stress, health, and the life course: some conceptual perspectives. Journal of Health and Social Behavior, 46(2), 205–219. [DOI] [PubMed] [Google Scholar]
- Pollini RA, Banta-Green CJ, Cuevas-Mota J, Metzner M, Teshale E, & Garfein RS (2011). Problematic use of prescription-type opioids prior to heroin use among young heroin injectors. Subst Abuse Rehabil, 2(1), 173–180. doi: 10.2147/sar.s24800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richters JE, & Martinez P (1992). Things I have seen and heard: measures for assessment of functioning & outcomes in longitudinal research on child abuse. [Google Scholar]
- Rivera JO, Ortiz M, & Cardenas V (2009). Cross-border purchase of medications and health care in a sample of residents of El Paso, Texas, and Ciudad Juarez, Mexico. J Natl Med Assoc, 101(2), 167–173. [DOI] [PubMed] [Google Scholar]
- Rolita L, Spegman A, Tang X, & Cronstein BN (2013). Greater number of narcotic analgesic prescriptions for osteoarthritis is associated with falls and fractures in elderly adults. J Am Geriatr Soc, 61(3), 335–340. doi: 10.1111/jgs.12148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenblum A, Parrino M, Schnoll SH, Fong C, Maxwell C, Cleland CM, . . . Haddox JD (2007). Prescription opioid abuse among enrollees into methadone maintenance treatment. Drug Alcohol Depend, 90(1), 64–71. doi: 10.1016/j.drugalcdep.2007.02.012 [DOI] [PubMed] [Google Scholar]
- Rudd RA, Seth P, David F, & Scholl L (2016). Increases in Drug and Opioid-Involved Overdose Deaths - United States, 2010–2015. MMWR Morb Mortal Wkly Rep, 65(5051), 1445–1452. doi: 10.15585/mmwr.mm655051e1 [DOI] [PubMed] [Google Scholar]
- Ruston Dave, & Akinrodoye Lola. (2002). Social Capital Question Bank June 2002: Questions from Social Capital surveys included in the Social Capital Survey Matrix 2002 [www.statistics.gov.uk/about_ns/social_capital/downloads/Social_Capital_Question_Bank.pdf, accessed 012907]. Retrieved from www.statistics.gov.uk/about_ns/social_capital/downloads/Social_Capital_Question_Bank.pdf
- Saha TD, Kerridge BT, Goldstein RB, Chou SP, Zhang H, Jung J, . . . Grant BF (2016). Nonmedical Prescription Opioid Use and DSM-5 Nonmedical Prescription Opioid Use Disorder in the United States. J Clin Psychiatry, 77(6), 772–780. doi: 10.4088/JCP.15m10386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shah NG, Lathrop SL, Flores JE, & Landen MG (2012). The influence of living along the U.S.-Mexico border on unintentional drug overdose death, New Mexico (USA), 2005–2009. Drug Alcohol Depend, 125(1–2), 19–26. doi: 10.1016/j.drugalcdep.2012.02.023 [DOI] [PubMed] [Google Scholar]
- StataCorp. (2017). Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC. [Google Scholar]
- Tannenbaum Cara, Paquette Amélie, Hilmer Sarah, Holroyd-Leduc Jayna, & Carnahan Ryan. (2012). A Systematic Review of Amnestic and Non-Amnestic Mild Cognitive Impairment Induced by Anticholinergic, Antihistamine, GABAergic and Opioid Drugs. Drugs & Aging, 29(8), 639–658. doi: 10.1007/BF03262280 [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. (2013). USA QuickFacts [Accessed: 2013-07-11. Archived by WebCite® at http://www.webcitation.org/6I2c4494W]. Retrieved from Washington, DC: http://quickfacts.census.gov/qfd/states/00000.html [Google Scholar]
- Valdez A, Sifaneck SJ (1997). Drug Tourists and Drug Policy on the U.S.-Mexican Border: An Ethnographic Investigation of the Acquisition of Prescription Drugs. Journal of Drug Issues, 27(4), 879–898. [Google Scholar]
- Valdez Avelardo. (1993). Persistent poverty, crime, and drugs: U.S.–Mexican border region. In Moore Joan & Pinderhughes Raquel (Eds.), In the Barrios. Latinos and the underclass debate (pp. 173–194). New York, NY: Russell Sage Foundation. [Google Scholar]
- Wang KH, Becker WC, & Fiellin DA (2013). Prevalence and correlates for nonmedical use of prescription opioids among urban and rural residents. Drug Alcohol Depend, 127(1–3), 156–162. doi: 10.1016/j.drugalcdep.2012.06.027 [DOI] [PubMed] [Google Scholar]
- Wunsch MJ, Nakamoto K, Behonick G, & Massello W (2009). Opioid deaths in rural Virginia: a description of the high prevalence of accidental fatalities involving prescribed medications. Am J Addict, 18(1), 5–14. doi: 10.1080/10550490802544938 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young AM, Havens JR, & Leukefeld CG (2012). A comparison of rural and urban nonmedical prescription opioid users’ lifetime and recent drug use. Am J Drug Alcohol Abuse, 38(3), 220–227. doi: 10.3109/00952990.2011.643971 [DOI] [PubMed] [Google Scholar]
- Zemore SE, Cherpitel CJ, Ye Y, Borges G, Li L, & Wallisch LS (2016). Factors Explaining Variation in Alcohol Use Disorder Prevalence Across Border and Nonborder Communities in Texas. Alcohol Clin Exp Res, 40(8), 1707–1716. doi: 10.1111/acer.13124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimet Gregory D., Dahlem Nancy W., Zimet Sara G., & Farley Gordon K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. [DOI] [PubMed] [Google Scholar]
- Zinn Maxine Baca. (1982). FAMILISM AMONG CHICANOS: A THEORETICAL REVIEW. Humboldt Journal of Social Relations, 10(1), 224–238. [Google Scholar]