

Abstract
The objective was to investigate the effects of functional (FT) and traditional (TT) training on trunk muscles maximal isometric strength, rate of force development and endurance with trained elderly women. Forty-five elderly women were directed into three groups: FT (n =1 6), TT (n = 14) and Control (n = 15). The FT (multi-planar, and multi-articular movements) and TT (primarily machine-based resistance exercises) performed mobility, muscle strength and power exercises. Both training groups also performed intermittent cardiometabolic activities. The maximum strength and endurance of the trunk muscles were verified, both at baseline and after 12 weeks of training (3xweek for 50 min each). Data were analyzed using a 2-way ANCOVA with contrast of adjusted mean values. FT significantly increased all variables: maximum trunk flexor strength (p = 0.002, 22%); rate of flexor force development (p = 0.001, 84%); trunk extensors maximal strength (p = 0.003, 17%); trunk extensor rate of force development (p = 0.05, 16%); trunk flexors (p = 0.001, 19%) and extensors (p = 0.017, 13%) endurance compared to baseline. TT showed an increase only in RFD of trunk extensors (p = 0.003, 53%), and flexors (p = 0.033, 42%), and trunk flexors endurance (p = 0.008, 11%). However, there was no statistically significant difference between groups. FT promoted improvement in all variables; strength, endurance and rate of force development of the trunk flexors and extensors of the elderly. On the other hand, TT improved only the rate of force development of trunk flexors and extensors and endurance of the trunk flexors. FT is recommended for elderly women as it improves a broader array of physiological parameters.
Key points.
Both FT and TT can improve trunk flexor and extensor muscle strength and endurance with trained elderly women.
FT provides larger magnitude improvements to a wider variety of physiological measures.
Since FT provides greater training specificity, it is highly recommended for training with elderly women.
Key words: Aging, spine, activities of daily living, exercise
Introduction
The aging process can lead to a reduction in muscle mass and strength (sarcopenia), especially in women aged 60 and older (Hunter et al., 2016; Visser et al., 2005). Resistance training with the goal of increasing strength and endurance is important for the treatment and prevention of many diseases and conditions such as diabetes, dyslipidemia, cardiovascular diseases, and others (Figueiredo et al., 2018). The ubiquitous finding that muscular strength is inversely related to mortality may be related to its role in preventing disability, allowing people to continue performing activities of daily living (ADL) and decreasing the risk for falls and accidents (Willardson and Tudor-Locke, 2005). Garcia-Hermoso and colleagues (2018) in a meta-analysis reported that greater upper- and lower-body muscular strength are associated with a lower risk of mortality in adult population, independent of the age. Hence, research that helps determine the most efficient and effective resistance training modalities are an important contribution to the health of the population.
Trunk muscles are responsible for facilitating the strength transfer between the upper and lower limbs during the execution of complex multi-articular movements (Lehman et al., 2013). Alterations in trunk muscle strength have been investigated to determine their influence for the prevention and treatment of lumbar spine injuries (Fielding et al., 2011) and in the improvement of functional performance with the elderly (Aagaard et al., 2010). The trunk musculature typically undergoes substantial changes with advancing age (Byrne et al., 2016; Fried et al., 2001; Hicks et al., 2012). For example, a significant 26% to 48% decrease in trunk muscle thickness was observed in the elderly population (≥ 75 years old) compared to 30-50 years old adults, impacting the maximum strength of these muscles (Afilalo et al., 2009). Hicks et al. (Hicks et al., 2005) revealed associations between greater trunk muscle fat infiltration and reduced functional capacity and balance in the elderly over 70 years old. In addition, older adults with low pain back (LBP) have a greater average multifidus muscle-to-fat index and smaller cross-sectional area when compared to control participants without LBP (Sions et al., 2017). The literature is consistent in reporting that trunk muscles maximal strength and endurance are associated with improved functional performance (Behm et al., 2009; Maddigan et al., 2014). Therefore, understanding and mediating age-related sarcopenia processes can aid in the formulation of specific training programs for the daily needs of the elderly.
The American College of Sports Medicine (ACSM) recommends resistance training to strengthen the trunk muscles. ACSM guidelines support the use of traditional resistance training (TT), characterized as a conservative training method that uses resistance machines with gradual, progressive load increases to prevent or reduce disability in the elderly (Kibler et al., 2006; Shahtahmassebi et al., 2017). However, the training specificity literature has shown that the benefits of TT for improving muscle strength have little transfer to the performance of ADLs in the elderly population (Cadore et al., 2013). Most TT exercises are not multi-articular and multiplanar. But, according to recent studies, these aspects seem fundamental for eliciting greater trunk activation (Kahle and Tevald, 2014; Granacher et al., 2013). This lack of training specficity with TT may contribute to the deficiency of positive trunk muscle training adaptations with TT (Silfies et al., 2015). Furthermore, the possible effects of TT on maximal strength and trunk muscle endurance in the elderly have not been fully investigated.
On the other hand, functional training (FT) has been introduced to the elderly population, combining multi-planar, coordinated and multi-articular movements to improve their functional capacity (Kasukawa et al., 2010). Such training can be organized according to movement patterns such as squat, pushing, pulling and transporting in blocks that stimulate power, speed, stability or maximum strength (Ebenbichler et al., 2001). Therefore, FT seeks to achieve training specificity (Behm and Sale, 1993) by simulating and stimulating relevant actions and components of the elderly’s physical capacity, with direct transfer to the ADLs and involving lower operational cost (Barbado et al., 2016; Behm et al., 2010a; Hicks et al., 2005). Nevertheless, Shahtahmassebi et al. (2017) revealed associations between trunk muscle and functional ability as evaluated with six-minute walk performance, chair stand test, sitting and rising test; and timed up and go test. Thus, improvement of functionality through FT, could possibly improve the strength and endurance of the trunk (Sions et al., 2017).
Considering the importance of the trunk muscles for the physical performance of the elderly and the lack of studies regarding which training allows a greater neuromuscular adaptation of the trunk, the objective of this study was to evaluate the effects of functional and traditional resistance training on the maximal strength, rate of force development and endurance of the trunk muscles in trained elderly women.
Methods
Experimental design
Forty-five elderly women were placed (controlled randomization) into one of two 12 weeks training (3xweek for 50 minutes per session) groups: Functional (FT, n = 16), Traditional (TT, n = 14) or a Control (CG, n = 15). The trunk flexors and extensors strength, rate of force development and endurance were measured before and after training.
Participants
The 45 elderly women were recruited through digital media, posters, and flyers. Initially, 20 women were recruited for the CG in anticipation that the lack of an exercise training protocol would be de-motivating. Five control group participants did drop out. Women older than 60 years old who did not have musculoskeletal or cardiovascular conditions that contraindicated the training and were physically active and independent were included. The exclusion criteria were attendance at less than 85% of the training sessions, two consecutive absences or development of illness during the period of study. After explaining the protocols, they signed a freely informed consent form and this study was approved by the Research Ethics Committee of the Institution (060568/2017).
The participants were organized in ascending order According to their maximum trunk muscle strength. After this initial classification, they were distributed into groups, with each group having a representative sample of the weakest to the strongest. Thus, the participants were randomized by blocks (randomized block type) according to the individual strength capacity in three distinct groups: a) functional resistance training (FT); b) traditional resistance training (TT); and c) control group (CG) (Figure 1).
Figure 1.
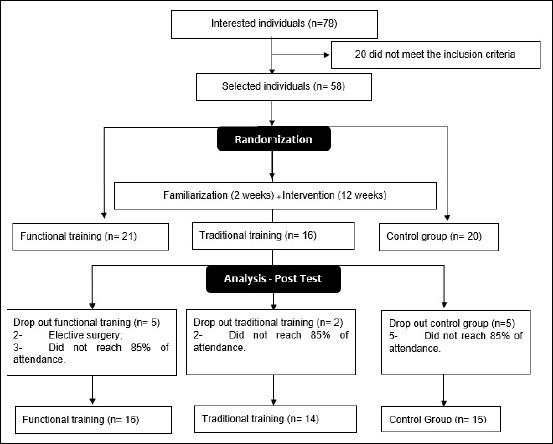
Experimental design.
Data collection procedures
The performance tests were performed on two occasions: before and after the 12 weeks training intervention. The evaluators were blinded regarding the intervention performed by the participants. To minimize the interference between the tests, they were distributed on two consecutive days. On the first day, maximum strength tests were applied and on the second day, the endurance tests were applied. For all performance tests, participants were verbally motivated to achieve their best performance.
For the anthropometric measures, the body mass (kg) was determined by an electronic scale (Welmy, R-110, São Paulo, Brazil) with an accuracy of 0.01 kg, and their height was determined by a stadiometer (Sanny®, ES2030, Araraquara, São Paulo, Brazil) with an accuracy of 0.1 cm.
Participants sat on a stable wooden seat (Figures 2 and 3) when testing the maximum strength of the trunk flexor and extensor muscles. This seat allowed adjustable support for the hips and the lower limbs according to each individual height. Pelvic positioning instructions were followed according to Sutarno et al. (Sutarno and McGill, 1995). To ensure the activation of only the trunk muscles, the participants were asked to have their knees flexed at 90°, with a slight anterior tilt of the pelvis to avoid a compensatory activation of the lower limbs and with the legs fixed to the seat with a velcro strap (Cadore et al., 2013; Garcia-Hermoso et al., 2018). To measure the strength and rate of force development of the trunk extensors, the participants were positioned with the trunk at a 0° flexion and the load cell fixed to the wall with adjustable tension and connected to the participant by a Velcro strap positioned at the level of the xiphoid process. For the strength of the trunk flexors, the same positioning of the trunk and Velcro strap was maintained, however, the load cell was fixed to the wall behind the participant. In both actions, a maximal isometric contraction of the trunk muscles was requested of the participants. From this position, the muscle strength of the trunk extensors and flexors were measured by a digital load cell (Ktoyo, 333 A, Hown Dong, South Korea), connected to the Muscle Lab system (Ergotest Innovation, Porsgrunn, Norway), which provides a value in Newton (N), and the Strength Development Rate (SDR) in Newtons/seconds.
Figure 2.

Experimental testing device.
Figure 3.
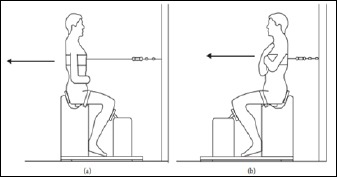
Schematic of trunk extensors and flexors testing device.
The participants initially performed a maximal repetition for familiarization to evaluate the maximum strength in both muscle groups, followed by three maximal, five second contractions and the highest value was used for analysis. The recovery intervals between the maximal repetitions were 15 seconds and the evaluators issued the following verbal commands in all the attempts: “prepare” (individual positioning); and “go, strength, strength, strength” (performing the test), “relax” (end of the test), with a smooth and continuous execution (Kasukawa et al., 2010).
The trunk muscles endurance was evaluated with the protocol proposed by McGill (1999). A timer (Technos, YP2151 / 8P, Rio de Janeiro, Brazil) was used to measure the maximum duration (time) the participants were able to maintain each isometric position and a five-minute recovery interval between each test was determined. For the evaluation of the trunk flexors, the participants were instructed to remain in the seated position with their backs resting on a wooden wedge with a 60° angle from the ground. Both the knees and hips were flexed 90°, the arms were crossed in front of the chest, hands on the opposite shoulder and the feet were fixed by an evaluator. They were instructed to maintain the initial posture while the wedge was withdrawn at 10 cm from that posture assessed in the posterior direction. The end of the test was determined when the upper trunk was unable to maintain the angle of 60°.
For the trunk extensors endurance, the participants were positioned with the hip and lower limbs on the edge of a stretcher and with their arms crossed in front of the chest, and the spine remaining erect. Pelvis, knees, and hip were secured with three Velcro straps to keep the participant secure. For the beginning of the test, the command was given to maintain the horizontal position of the trunk as long as possible and it was completed when the participant could not maintain the position. Prior published assessments from this laboratory have shown very high and high reliability scores for both trunk extensor (0.98) and flexor (0.86) strength in elderly women (Mesquita et al. 2019).
Training protocol
The familiarization and training intervention lasted 14 weeks. After the initial assessments, all participants went through two weeks of familiarization, where 50% of the training volume planned for the first session was applied. Then, they completed 36 progressive training sessions over 12 weeks. The three groups performed the training three times a week, lasting 50 minutes per session with 48-hour recovery interval between sessions. For the TT and FT groups, the OMNI-GSE scale was additionally used to control and normalize the overall effort perception of training between the groups at the end of each exercise block (Behm et al., 2009). For both groups, a range between 6 and 9 (moderate to intense) was established in the effort perception scale.
Functional training: The participants performed exercises with greater freedom of movement and specific to the physical needs of their daily life. Each session was divided into four blocks: Block 1 involved 5 minutes of dynamic mobility exercises of the cervical, glenohumeral, thoracic, hip joint complexes and ankle and general warming exercises that included 10 repetitions of vertical squats and jumps; Block 2 involved 15 minutes of a circuit composed of exercises that stimulated agility, coordination, speed and muscle power (OMNI-GSE: 6-7); Block 3 included 20 minutes of circuit training with multi-articular exercises that simulated the functional actions of crouching, pulling, pushing and transporting and specific exercises for the core (example: frontal board), (OMNI-GSE: 7-8); and 5 minutes of intermittent cardiometabolic activities (Table 1).
Table 1.
Detailed description of functional (FT) and traditional (TT) training sessions.
| FT | 1° block | 2° block | 3° block | 4° block | ||
| Preparation for movement with mobility exercises for the shoulder, lumbar, thoracic spine, hip, and ankle joints | Sessions 1-18 | Sessions 18-36 | Sessions 1-18 | Sessions 18-36 | High intensity activities. For example, interval race, fun games. and tug of war |
|
| Ascending and descending steps | Step jump | Deadlift with Kettlebell | Deadlift with sandbag | |||
| Alternating waves (rope) | Alternating waves (rope) | Rowing with suspension tape | Rowing with suspension tape | |||
| Sit and lift the bench 40cm | Squat with kettlebell | |||||
| Medicine ball throws on the ground | Medicine ball throws on the wall | Adduction of upper limbs with elastic | Push-ups on the bench 60cm | |||
| Farme’rs walk (kettlebells) | Farmer’s walk (kettlebells) | |||||
| Movement between cones | Run and jump between cones | Rowing with elastic bands | Rowing with elastic bands and knee elevation | |||
| Bilateral pelvic elevation | One-sided pelvic elevation | |||||
| Linear agility ladder | Lateral agility ladder | Front plank on the bench 40cm | Front plank on the step 15cm | |||
| Total time: 5 min., 3-5 exercises per joint, 1 set of 8 seconds |
Total time: 15 min, 5exercises, 3 sets of 30 s, 1 min by exercise, density 1/1. OMINI-GSE: 6-7 |
Total time: 15 min, 5exercises, 3 sets of 30 s, 1 min by exercise, density 2/1. OMINI-GSE: 6-7 |
Total time: 20 min., 8 exercises, 2 sets of 8-12 repetitions, 1 min per station, density 1/1. OMINI-GSE: 7-9 |
Total time: 20 min., 8 exercises, 2 sets of 8-12 repetitions, 1 min per station, density 1/1. OMINI-GSE: 7-9 |
Total time: 5 min., 5-8 efforts, density of 1/1. OMINI-GSE: 8-9 |
|
| TT | Preparation for movement with mobility exercises for the shoulder, lumbar, thoracic spine, hip, and ankle joints | Continuous walking on a 100 meter course | Continuous walking on a 100 meter course | Smith Squat | Free Squat | High intensity activities. For example, interval race, fun games. and tug of war |
| Seated row | Seated row | |||||
| Leg press 45° | Knee extension | |||||
| Chest press | Bench press | |||||
| Knee flexion with the leg curl device | Unilateral knee flexion | |||||
| Lat pull down (supine grip) | Lat pull down (neutral grip) | |||||
| Standing calf rise | Seated calf rise | |||||
| Stiff leg deadlift | Sit up | |||||
| Total time: 5 min., 3-5 exercises per joint, 1 set of 8 seconds |
Total time: 15 min. OMINI-GSE: 6-7 |
Total time: 15 min. OMINI-GSE: 6-7 |
Total time: 20 min., 8 exercises, 2 sets of 8-12 repetitions, 1 min per station, density 1/1. OMINI-GSE: 7-9 |
Total time: 20 min., 8 exercises, 2 sets of 8-12 repetitions, 1 min per station, density 1/1. OMINI-GSE: 7-9 |
Total time: 5 min., 5-8 efforts, density of 1/1. OMINI-GSE: 8-9 |
|
Traditional training: The participants performed mostly machine-based exercises with traditional devices (i.e. resistance machines) and with segmented neuromuscular work. Each session was also divided into four blocks: Block 1 involved 5 minutes of mobility and exercises for general warming of the body; Block 2 included 15 minutes of continuous walking that required mainly muscular and cardiorespiratory endurance (OMNI-GSE: 6-7); Block 3 involved 20 minutes of resisted exercises for lower and upper limbs - OMNI-GSE: 7-8); and 5 minutes of intermittent activities (Table 1).
Exercise progression was achieved by adding the external load in the TT based on the perception of effort in the OMNI-GSE scale and the maintenance of 8-12 repetitions in each exercise. For the FT group, the same criterion was used for adding external load in the exercises. In the exercises performed with the body mass, biomechanical modifications were applied according to the level of comfort and ability of the individual, also aiming at the maintenance of 8-12 repetitions.
Control group: The participants performed static stretching with two sets of 20 seconds per exercise, which were directed to a full body work (neck, shoulders, back, trunk, arms, wrists, hands, lower torso, hips, knees, thighs, feet and calves) with submaximal joint amplitude levels and relaxation practices without physical exertion, with a frequency of three weekly sessions and duration of 40 minutes per session.
Statistical analysis
The sample size calculation used the Granmo 5.2 program (IMIM, Barcelona, Spain) based on the results obtained by Lohne-Seiler et al. (2013) in the tests of maximum dynamic strength. Thus, 15 subjects per group were required to achieve an alpha of 0.05 and a statistical power of 80%. With five women dropping out of the CG, the pre-test measures between groups were less balanced. It was recommended that an ANCOVA be utilized with the pre-test values as covariates. For the inferential analyses, the data were tabulated in the Statistical Package for Social Sciences (SPSS) version 22, adopting a significance level of 5% (p ≤ 0.05). The normality of the data was verified from the Kolmogorov-Smirnov test, and the homogeneity of the variances were verified by the Levene test. Descriptive statistics were used with mean and standard deviation to characterize the observed variables. The data were analyzed with a two factors ANCOVA (3-groups x 2 times) with contrast of adjusted mean values, inserting the baseline result of each variable as a covariate. Effect size (ES) was calculated according to the Cohen d test (2013), based on the difference between the final and initial mean divided by the standard deviation of the initial mean, where ES varies between trivial < 0.2; small 0.2-0.49; moderate 0.5-0.79; and large > 0.8 magnitudes of change.
Results
There were no statistical differences between groups for anthropometric parameters at baseline (Table 2).
Table 2.
Characteristics of the participants with Functional Training (FT), Traditional Training (TT) and Control groups (CG). Values presented are means and standard deviations (SD).
| FT (n = 16) | TT (n = 14) | CG (n = 15) | |
|---|---|---|---|
| Age (yrs) | 65.6 ± 3.2 | 63.0 ± 1.8 | 66.8 ± 6.1 |
| Height (m) | 1.55 ± 5.2 | 1.54 ± 4.1 | 1.53 ± 3.6 |
| Body mass (kg) | 68.2 ± 9.6 | 67.2 ± 11.8 | 69.3 ± 9.4 |
No significant differences were found between groups (1-way ANOVA).
All means, standard deviations, statistical significance (main effects and interactions), percentage changes and effect size values are provided in Table 3. Within-group interactions revealed that FT had a significant increase between the pre- and post-tests for the six variables analyzed. Additionally, the ES for the maximum trunk flexors (ES = 0.87) and extensors (ES = 0.61) strength was large, and moderate respectively. The ES for the trunk flexor and extensors rate of force development was large (ES = 1.81), and small (ES = 0.41) respectively. The trunk flexors (ES = 0.21) and trunk extensors (ES = 0.27) endurance effect sizes were also small.
Table 3.
Alterations after 12 weeks of Functional Training (FT, n=16), Traditional Training (TT, n=14) and Control Group (CG, n=15) in the maximum isometric strength, rate of force development and endurance of trunk muscles. Values presented as means and standard deviations.
| Pre-test | Post-test | Δ (%) | ES | Main Effect (group) |
Main Effect (time) |
Interactions (time x group) |
Contrast of adjusted mean values |
|
|---|---|---|---|---|---|---|---|---|
| Trunk Flexors Force (N) | ||||||||
| FT | 229.85 ± 58.9 | 281.14 ± 65.0 | 22% | 0.87 | p=0.855 | p=0.045 | p=0.566 | p=0.002 * |
| TT | 235.15 ± 84.4 | 261.36 ± 93.8 | 11% | 0.31 | p=0.108 | |||
| CG | 239.19 ± 59.01 | 252.15 ± 68.18 | 5% | 0.22 | p=0.361 | |||
| Flexors’ RFD (N/s) | ||||||||
| FT | 16.0 ± 7.4 | 29.45 ± 17.21 | 84% | 1.81 | p=0.994 | p=0.001 | p=0.415 | p=0.001 * |
| TT | 18.65 ± 11.55 | 26.39 ±15.0 | 42% | 0.67 | p=0.033 * | |||
| CG | 20.22 ± 8.77 | 25.51 ± 12.7 | 26% | 0.60 | p=0.09 | |||
| Flexors’ Endurance (s) | ||||||||
| FT | 72.37 ± 66.94 | 86.18 ± 69.5 | 19% | 0.21 | p=0.294 | p=0.621 | p=0.221 | p=0.001 * |
| TT | 90.28 ± 81.61 | 100.07 ± 83.67 | 11% | 0.12 | p=0.008 * | |||
| CG | 53.3 ± 46.4 | 57.73 ± 50.65 | 9% | 0.10 | p=0.127 | |||
| Trunk Extensors Force (N) | ||||||||
| FT | 262.8 ± 72.0 | 306.55 ± 78.56 | 17% | 0.61 | p=0.401 | p=0.135 | p=0.426 | p=0.003 * |
| TT | 258.32 ± 97.1 | 288.10 ± 76.4 | 12% | 0.31 | p=0.059 | |||
| CG | 261.28 ± 61.46 | 257.1 ± 58.8 | -1% | -0.06 | p=0.788 | |||
| Extensors’ RFD (N/s) | ||||||||
| FT | 24.58 ±10.4 | 28.59 ± 9.6 | 16% | 0.40 | p=0.023 | p=0.169 | p=0.665 | p=0.050 * |
| TT | 25.96 ± 9.0 | 30.44 ± 14.7 | 17% | 0.49 | p=0.003 * | |||
| CG | 21.18 ± 6.65 | 21.42 ± 9.6 | 1% | 0.04 | p=0.927 | |||
| Extensors’ Endurance (s) | ||||||||
| FT | 106.62 ± 52,.9 | 121.00 ± 65.1 | 13% | 0.27 | p=0.010 | p=0.509 | p=0.918 | p=0.017 * |
| TT | 120.85 ± 73.3 | 128.7 ± 70.1 | 6% | 0.10 | p=0.226 | |||
| CG | 79.26 ± 46.5 | 81.3 ± 44.7 | 3% | 0.04 | p=0.819 | |||
Data analyzed from a two way ANCOVA (3-group x 2 times), ES; (Effect size); N (Newtons); RFD (Rate of force development); s (seconds);
* p ≤ 0.05 (statistical significance pre- to post-test).
The TT group showed training-related increases in only four variables: maximal trunk extensor strength (ES = 0.31: small magnitude), flexor (ES = 0.61: moderate) and extensor rate of force development (ES = 0.49: small), and trunk flexors endurance (ES = 0.12: trivial).
Main effects for time were evident with trunk flexors force and RFD, whereas main effects for group were found with trunk extensors RFD and endurance (see Table 3 for details).
Discussion
This study compared the effects of 12 weeks of FT and TT on maximal isometric strength, rate of force development and endurance of the trunk muscles in an elderly female population. Although there were no statistically significant training group differences, FT showed improvements in all six variables, even with absence of additional exercises specific for the trunk muscles. On the other hand, the TT only showed increased performance with half of the measures (trunk flexors and extensors RFD, and trunk flexors endurance). Furthermore, FT effect sizes were higher than TT or control group with all measures except for trunk extensors RFD. Hence, improvements in training adaptations were more widespread and generally of a greater magnitude with FT.
The more consistent and greater magnitude improvements with FT (FT: 2 large, 1 moderate and 2 small magnitudes of change vs. TT with no large magnitude changes, 1 moderate, 3 small, and 2 trivial magnitude changes: Table 3) can be explained by the greater degrees of freedom, spectrum of movement velocities, and instability of the FT exercises, which allow adjustments in the postural control and the activation of the stabilizing muscles in the spine (Byrne et al., 2016; Sutarno and McGill, 1995). Confirming the findings of this study, Liu and Latham (2009) in a systematic review observed that functional training induces the activation of multiple muscles to perform the exercises in a manner more similar to their daily activities. Thus functional training can provide a greater training specificity transfer (Behm and Sale, 1993), which is a hallmark of an optimal training strategy. A position stand by the Canadian Society for Exercise Physiology suggests that training with greater instability such as typically espoused with FT, can play an important role within rehabilitation programs and for non-athletic individuals to achieve musculoskeletal health benefits (Behm et al., 2010b). These benefits can be attributed to the higher muscle activation achieved with the use of lower loads associated with FT (Behm et al., 2010a).
In addition, in FT, specifically in blocks 2 and 3, multi-articular and multi-planar exercises were used that more closely mimicked the functional actions present in daily life, such as crouching, pulling, pushing and squatting. The inclusion of multi-articular and multi-planar exercises with FT (La Scala Teixeira et al., 2017) can generate a high magnitude of core activation leading to positive training adaptations of the core (trunk), which is in accordance with our results (Comfort et al., 2011; Garcia-Masso et al., 2011; Stastny et al., 2015).
Although there were no significant differences between training groups, within group interactions showed that the FT demonstrated a significant, large magnitude increase in trunk flexors strength compared to a non-significant, trivial change with TT. Moreover, FT displayed significant, small magnitude improvements in trunk flexors and extensors endurance compared to non-significant, trivial changes with TT. This greater magnitude training adaptation may be attributed to the plank exercise performed by the FT group that selectively activate the trunk flexor muscles, especially the rectus abdominis, external and internal oblique muscles to stabilize the spine (Bland and Altman, 1986; Weber et al., 2018). Abdominal bracing is reported to be more effective than abdominal hollowing and other similar exercises for optimizing spinal stability (Behm et al., 2010a; Vera-Garcia et al. 2007). Furthermore, when using the pushing pattern, the recruitment of multiple muscles of the trunk, shoulder, and arms occurs simultaneously with the goal of controlling movement. Marcolin et al. (2015) found high rectus abdominis activation to stabilize the spine during the execution of push-ups. In addition, trunk muscles are essential for core stability when performing agility, power and coordination exercises (Behm et al., 2010a; Byrne et al., 2016; Kasukawa et al., 2010), which were prevalent in the second block of FT.
Both training groups demonstrated significant trunk extensor strength increases with FT exhibiting moderate versus small magnitude training adaptation with TT. This modest advantage with FT may have occurred because there is a greater requirement of the paravertebral muscles for the execution of the deadlift and free squat, for core stability and to prevent the trunk from leaning excessively forward. Highlighting the importance of our findings, Kasukawa et al. (2010) in a cross-sectional study demonstrated that excessive trunk inclination with ageing is related to decreased trunk extensor muscle strength, which is related to greater risks of falling.
Similarly, both training groups experienced significant (p = 0.003) and near significant (p = 0.059) improvements in trunk extensor rate of force development, with moderate versus small magnitude training adaptations for the FT versus TT respectively. Again, the FT showed a modest training advantage, which may be attributed to the stiff-leg deadlift exercise that necessitates high erector spinae muscle activation to perform the trunk extension, and these movements were performed at maximum concentric velocity in training block 2 (Kienbacher et al., 2014).
Regarding trunk extensor muscle endurance, only the FT group presented a significant increase. The mean increase of trunk extension endurance with training was 15 seconds, which may correspond to an important clinical improvement. As mentioned previously the greater degrees of freedom, spectrum of movement velocities, and instability of the FT would be providing great paravertebral muscles activation to generate postural adjustment during the execution of the pull exercises (Byrne et al., 2016). Suri et al. (2011) pointed out that a one-second increase in trunk extension endurance was associated with a significant 4% increase in the Berg balance scale. This could impact the incidence of falls and slips in the elderly.
Although there was a controlled randomization to ensure an equal distribution of participants with greater muscle strength between the groups, one of the limitations of the study was the sample loss during the intervention that made it difficult to analyze the endurance measures during the training. However, the pre-test covariate was used to minimize these limitations. The data was collected from trained elderly women, and thus future research should examine untrained elderly women as well as a spectrum of differentially trained men.
Conclusion
Both FT and TT can promote the improvement of trunk flexor and extensor muscle strength and endurance with trained elderly women. However, the FT was able to generate greater magnitude changes and positively affect more variables in relation to TT. This training advantage is probably due to the greater spectrum of movements, velocities and stability requirements of FT exercises. These changes, regardless of the proposed training, would have a positive impact on the individual’s fitness as well as possibly impacting society's health costs.
Acknowledgements
The study comply with the current laws of the country in which were performed. The authors report no conflict of interest. The authors thank the staff and participants at the Federal University of Sergipe for their participation in this project.
Biographies

Marzo Edir Da SILVA-GRIGOLETTO
Employment
University Research Professor
Degree
PhD
Research interest
Neuromuscular physiology and sport Functional training
E-mail: dasilvame@gmail.com

Marceli Matos Andrade MESQUITA
Employment
Physical therapist
Degree
Msc
Research interest
Exercise and rehabilitative sciences
E-mail: marcelimesquita@hotmail.com
José Carlos ARAGÃO-SANTOS
Employment
Physical therapist
Degree
Bachelor of Physical Education
Research interest
Exercise physiology and exercise immunology
E-mail: carlosaragao.18@gmail.com

Marta Silva SANTOS
Employment
Physical therapist
Degree
Msc
Research interest
Exercise and rehabilitative sciences
E-mail: martasilvaedf@gmail.com

Antônio Gomes de Resende NETO
Employment
Physical therapist
Degree
Msc
Research interest
Exercise and rehabilitative sciences
E-mail: neto.resende-edf@hotmail.com

Josimari Melo de SANTANA
Employment
University Research Professor
Degree
PhD
Research interest
Pain physiology and rehabilitative sciences
E-mail: desantanajm@gmail.com
David G. BEHM
Employment
University Research Professor
Degree
PhD
Research interest
Neuromuscular physiology and sport
E-mail: dbehm@mun.can
References
- Aagaard P., Suetta C., Caserotti P., Magnusson S.P., Kjaer M. (2010) Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scandinavian Journal of Medicine and Science in Sports 20, 49-64. [DOI] [PubMed] [Google Scholar]
- Afilalo J., Karunananthan S., Eisenberg M.J., Alexander K.P., Bergman H. (2009) Role of frailty in patients with cardiovascular disease. American Journal of Cardiology 103, 1616-1621. [DOI] [PubMed] [Google Scholar]
- M. American College of Sports Chodzko-Zajko W.J., Proctor D.N., Fiatarone Singh M.A., Minson C.T., Nigg C.R., Salem G.J., Skinner J.S. (2009) American College of Sports Medicine position stand. Exercise and physical activity for older adults. Medicine & Science in Sports & Exercise 41, 1510-1530. [DOI] [PubMed] [Google Scholar]
- Barbado D., Lopez-Valenciano A., Juan-Recio C., Montero-Carretero C., van Dieen J.H., Vera-Garcia F.J. (2016) Trunk Stability, Trunk Strength and Sport Performance Level in Judo. PLoS One 11, e0156267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behm D.G., Sale D.G. (1993) Velocity specificity of resistance training. Sports Medicine 15, 374-388. [DOI] [PubMed] [Google Scholar]
- Behm D.G., Cappa D., Power G.A. (2009) Trunk muscle activation during moderate- and high-intensity running. Applied Physiology, Nutrition, and Metabolism 34, 1008-1016. [DOI] [PubMed] [Google Scholar]
- Behm D.G., Drinkwater E.J., Willardson J.M., Cowley P.M. (2010a) The use of instability to train the core musculature. Applied Physiology, Nutrition, and Metabolism 35, 91-108. [DOI] [PubMed] [Google Scholar]
- Behm D.G., Drinkwater E.J., Willardson J.M., Cowley P.M.Canadian Society for Exercise, P. (2010b) Canadian Society for Exercise Physiology position stand: The use of instability to train the core in athletic and nonathletic conditioning. Applied Physiology, Nutrition, and Metabolism 35, 109-112 [DOI] [PubMed] [Google Scholar]
- Bland J.M., Altman D.G. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307-310. [PubMed] [Google Scholar]
- Byrne C., Faure C., Keene D.J., Lamb S.E. (2016) Ageing, Muscle Power and Physical Function: A Systematic Review and Implications for Pragmatic Training Interventions. Sports Medicine 46, 1311-1332. [DOI] [PubMed] [Google Scholar]
- Cadore E.L., Rodriguez-Manas L., Sinclair A., Izquierdo M. (2013) Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Research 16, 105-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J. (2013) Statistical power analysis for the behavioral sciences. Routledge. [Google Scholar]
- Comfort P., Pearson S.J., Mather D. (2011) An electromyographical comparison of trunk muscle activity during isometric trunk and dynamic strengthening exercises. Journal of Strength & Conditioning Research 25, 149-154. [DOI] [PubMed] [Google Scholar]
- Ebenbichler G.R., Oddsson L.I., Kollmitzer J., Erim Z. (2001) Sensory-motor control of the lower back: implications for rehabilitation. Medicine & Science in Sports & Exercise 33, 1889-1898. [DOI] [PubMed] [Google Scholar]
- Fielding R.A., Vellas B., Evans W.J., Bhasin S., Morley J.E., Newman A.B., Abellan van Kan G., Andrieu S., Bauer J., Breuille D., Cederholm T., Chandler J., De Meynard C., Donini L., Harris T., Kannt A., Keime Guibert F., Onder G., Papanicolaou D., Rolland Y., Rooks D., Sieber C., Souhami E., Verlaan S., Zamboni M. (2011) Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. Journal of the American Medical Directors Association 12, 249-256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Figueiredo V.C., de Salles B.F., Trajano G.S. (2018) Volume for Muscle Hypertrophy and Health Outcomes: The Most Effective Variable in Resistance Training. Sports Medicine 48, 499-505. [DOI] [PubMed] [Google Scholar]
- Fried L.P., Tangen C.M., Walston J., Newman A.B., Hirsch C., Gottdiener J., Seeman T., Tracy R., Kop W.J., Burke G., McBurnie M.A., Cardiovascular Health. Study Collaborative Research, G. (2001) Frailty in older adults: evidence for a phenotype. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences 56, M146-156. [DOI] [PubMed] [Google Scholar]
- Garcia-Hermoso A., Cavero-Redondo I., Ramirez-Velez R., Ruiz J.R., Ortega F.B., Lee D.C., Martinez-Vizcaino V. (2018) Muscular Strength as a Predictor of All-Cause Mortality in an Apparently Healthy Population: A Systematic Review and Meta-Analysis of Data From Approximately 2 Million Men and Women. Archives of Physical Medicine and Rehabilitation 99, 2100-2113. [DOI] [PubMed] [Google Scholar]
- Garcia-Masso X., Colado J.C., Gonzalez L.M., Salva P., Alves J., Tella V., Triplett N.T. (2011) Myoelectric activation and kinetics of different plyometric push-up exercises. Journal of Strength & Conditioning Research 25, 2040-2047. [DOI] [PubMed] [Google Scholar]
- Granacher U., Gollhofer A., Hortobágyi T., Kressig R. W., Muehlbauer T. (2013) The importance of trunk muscle strength for balance, functional performance, and fall prevention in seniors: a systematic review. Sports Medicine 43, 627-641. [DOI] [PubMed] [Google Scholar]
- Hicks G.E., Shardell M., Alley D.E., Miller R.R., Bandinelli S., Guralnik J., Lauretani F., Simonsick E.M., Ferrucci L. (2012) Absolute strength and loss of strength as predictors of mobility decline in older adults: the InCHIANTI study. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences 67, 66-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hicks G.E., Simonsick E.M., Harris T.B., Newman A.B., Weiner D.K., Nevitt M.A., Tylavsky F.A. (2005) Trunk muscle composition as a predictor of reduced functional capacity in the health, aging and body composition study: the moderating role of back pain. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences 60, 1420-1424. [DOI] [PubMed] [Google Scholar]
- Hunter S.K., Pereira H.M., Keenan K.G. (2016) The aging neuromuscular system and motor performance. Journal of Applied Physiology (1985) 121, 982-995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahle N., Tevald M. A. (2014) Core muscle strengthening’s improvement of balance performance in community-dwelling older adults: A pilot study. Journal of Aging and Physical Activity 22, 65-73. [DOI] [PubMed] [Google Scholar]
- Kasukawa Y., Miyakoshi N., Hongo M., Ishikawa Y., Noguchi H., Kamo K., Sasaki H., Murata K., Shimada Y. (2010) Relationships between falls, spinal curvature, spinal mobility and back extensor strength in elderly people. Journal of Bone and Mineral Metabolism 28, 82-87. [DOI] [PubMed] [Google Scholar]
- Kibler W.B., Press J., Sciascia A. (2006) The role of core stability in athletic function. Sports Medicine 36, 189-198. [DOI] [PubMed] [Google Scholar]
- Kienbacher T., Paul B., Habenicht R., Starek C., Wolf M., Kollmitzer J., Ebenbichler G. (2014) Reliability of isometric trunk moment measurements in healthy persons over 50 years of age. Journal of Rehabilitation Medicine 46, 241-249. [DOI] [PubMed] [Google Scholar]
- La Scala Teixeira C.V., Evangelista A.L., Novaes J.S., Da Silva Grigoletto M.E., Behm D.G. (2017) "You're Only as Strong as Your Weakest Link": A Current Opinion about the Concepts and Characteristics of Functional Training. Frontiers in Physiology 8, 643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehman G., Drinkwater E.J., Behm D.G. (2013) Correlation of throwing velocity to the results of lower-body field tests in male college baseball players. Journal of Strength & Conditioning Research 27, 902-908. [DOI] [PubMed] [Google Scholar]
- Liu C.J., Latham N.K. (2009) Progressive resistance strength training for improving physical function in older adults. The Cochrane Database of Systematic Reviews CD002759, Jul 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lohne-Seiler H., Torstveit M.K., Anderssen S.A. (2013) Traditional versus functional strength training: effects on muscle strength and power in the elderly. Journal of Aging and Physical Activity 21, 51-70. [DOI] [PubMed] [Google Scholar]
- Maddigan M.E., Button D.C., Behm D.G. (2014) Lower-limb and trunk muscle activation with back squats and weighted sled apparatus. Journal of Strength & Conditioning Research 28, 3346-3353. [DOI] [PubMed] [Google Scholar]
- Marcolin G., Petrone N., Moro T., Battaglia G., Bianco A., Paoli A. (2015) Selective Activation of Shoulder, Trunk, and Arm Muscles: A Comparative Analysis of Different Push-Up Variants. Journal of Athletic Training 50, 1126-1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGill S.M., Childs A., Liebenson C. (1999) Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Archives of Physical Medicine and Rehabilitation 80, 941-944. [DOI] [PubMed] [Google Scholar]
- Mesquita M.M.A., Santos M.S., Vasconcelos A.B.S., de S’a C.A., Pereira L.C.D., da Silva-Santos I.B.M., da Silva Junior W.M., de Matos D.G., Fontes A.S., Oliveira P.M.P., Aidar F.J., DeSantana J.M., Fernandes I.G.S., Da Silva-Grigoletto M.E. (2019) Reliability of a Test for Assessment of Isometric Trunk Muscle Strength in Elderly Women. Journal of Aging Research Jul 1;2019:9061839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shahtahmassebi B., Hebert J.J., Hecimovich M.D., Fairchild T.J. (2017) Associations between trunk muscle morphology, strength and function in older adults. Scientific Reports 7, 10907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silfies S. P., Ebaugh D., Pontillo M., Butowicz C. M. (2015) Critical review of the impact of core stability on upper extremity athletic injury and performance. Brazilian Journal of Physical Therapy 19, 360–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sions J.M., Elliott J.M., Pohlig R.T., Hicks G.E. (2017) Trunk Muscle Characteristics of the Multifidi, Erector Spinae, Psoas, and Quadratus Lumborum in Older Adults With and Without Chronic Low Back Pain. Journal of Orthopaedic & Sports Physical Therapy 47, 173-179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stastny P., Lehnert M., Zaatar A.M., Svoboda Z., Xaverova Z. (2015) Does the Dumbbell-Carrying Position Change the Muscle Activity in Split Squats and Walking Lunges? Journal of Strength & Conditioning Research 29, 3177-3187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suri P., Kiely D.K., Leveille S.G., Frontera W.R., Bean J.F. (2011) Increased trunk extension endurance is associated with meaningful improvement in balance among older adults with mobility problems. Archives of Physical Medicine & Rehabilitation 92, 1038-1043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutarno C.G., McGill S.M. (1995) Isovelocity investigation of the lengthening behaviour of the erector spinae muscles. European Journal of Applied Physiology and Occupational Physiology 70, 146-153. [DOI] [PubMed] [Google Scholar]
- Vera-Garcia F.J., Elvira J.L.L., Brown S.H.M., McGill S.M. (2007) Effects of abdominal stabilization maneuvers on the control of spine motion and stability against sudden trunk perturbations. Journal of Electromyography and Kinesiology 17, 556-567. [DOI] [PubMed] [Google Scholar]
- Visser M., Goodpaster B.H., Kritchevsky S.B., Newman A.B., Nevitt M., Rubin S.M., Simonsick E.M., Harris T.B. (2005) Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences 60, 324-333. [DOI] [PubMed] [Google Scholar]
- Weber M., Belala N., Clemson L., Boulton E., Hawley-Hague H., Becker C., Schwenk M. (2018) Feasibility and Effectiveness of Intervention Programmes Integrating Functional Exercise into Daily Life of Older Adults: A Systematic Review. Gerontology 64, 172-187. [DOI] [PubMed] [Google Scholar]
- Willardson J.M., Tudor-Locke C. (2005) Survival of the strongest: A brief review examining the association between muscular fitness and mortality. Strength and Conditioning Journal 27, 80-85. [Google Scholar]