

Abstract
Emerging research has provided support for the use of the Kessler Psychological Distress Scales in developing countries; however, this research has yet to be extended to southern Africa. This study sought to evaluate the performance of the Kessler scales in screening for depression and anxiety disorders in the South African population. The scales along with the Composite International Diagnostic Interview (CIDI) were included in the South African Stress and Health study, a nationally representative household survey. The K10/K6 demonstrated moderate discriminating ability in detecting depression and anxiety disorders in the general population; evidenced by area under the receiver operating curves of 0.73 and 0.72 respectively. However, both scales failed to meet our acceptability criteria of high sensitivity and high positive predictive value. Examinations of differences in responding by race/ethnicity revealed that the K10/K6 [Kessler Psychological Distress Scale 10‐item (K10) and the abbreviated six‐item (K6)] had significantly lower discriminating ability with respect to depression and anxiety disorders among the Black group (0.71) than among the combined minority race/ethnic groups of White, Colored, and Indian/Asian (0.78; p = 0.016). The difference in time period assessed on the K10/K6 (past 30 days) versus the CIDI (past 12 months) was a notable limitation of this study. Additional validation studies using clinician diagnostic instruments are recommended. Copyright © 2011 John Wiley & Sons, Ltd.
Keywords: psychometrics, epidemiology, affective disorders, screening, South Africa
Introduction
The monitoring of prevalence rates of mental disorders in any country is a necessary and productive step in the development of effective public health care policies and services. Conducting extensive, nationwide psychiatric epidemiological studies, however, requires large sums of money and high levels of expertise, both rare commodities in developing countries such as South Africa (cited in Gureje et al., 2006). A scarcity of resources and trained mental health care personnel add to the challenge of conducting a study of this scale (Seedat et al., 2004). The availability of lay‐administered structured diagnostic interviews coupled with screening questionnaires, which are easy and quick to administer, make the undertaking of nationwide epidemiological studies more feasible (Cairney et al., 2007).
A screening scale that in recent years has received growing attention and use in epidemiological studies is the Kessler Psychological Distress Scale. The 10‐item (K10) and the abbreviated six‐item (K6) version of the scale were specifically developed for use in epidemiological studies to identify people in the general population who are experiencing non‐specific psychological distress (Kessler et al., 2002). Taking questions from 18 commonly used screening scales, Kessler et al. (2002) used modern item response theory methods to identify the questions that were best able to screen for current (within one‐month) psychological distress. Only questions that consistently measured severities across socio‐demographic groups were included (Baillie, 2005).
The K10 and K6 have been validated against highly recognized diagnostic interviews, such as the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI) and the Structured Clinical Interview for DSM‐IV (SCID), in psychiatric epidemiological studies conducted in North America and Australia (Kessler et al., 2002; Kessler et al., 2007). The scales have been found to have strong psychometric properties and good power in discriminating DSM‐IV disorder cases from non‐cases (Furukawa et al., 2003; Kessler et al., 2002; Kessler et al., 2007). Moreover, the K10 and K6 have been found to surpass the performance of other highly utilized screening scales such as the General Health Questionnaire (GHQ; Furukawa et al., 2003).
Translated versions of the Kessler scales have been found to have strong psychometric properties. Translated versions of the K10 and K6 were included in the WHO's world mental health survey in Japan. The area under the curve (AUC) of the K10 and K6 was 0.94 for both scales, indicating excellent screening ability (Furukawa et al., 2008). In the Netherlands, the K10 was included in a study forming part of the Amsterdam Health Monitor (AHM) survey. The K10 was translated and provided to the participants in the language of their choice (Dutch, Turkish, or Dutch/Arabic for the Moroccan sample). The validity of the K10 in screening for depression and anxiety across ethnic groups was explored. AUCs of 0.85, 0.88, and 0.80 were found for the Dutch, Moroccan, and Turkish samples respectively. This suggests the K10 has strong screening abilities among these ethnic groups in the Netherlands (Fassaert et al., 2009).
Clinical studies examining the validity of the K10 and K6 in developing countries such as India, Burkina Faso, and South Africa have been promising (Baggaley et al., 2007; Cairney et al., 2007; Furukawa et al., 2003; Patel et al., 2008; Spies et al., 2009a; Spies et al., 2009b). In a study conducted in India on the ability of the K10 and K6 in detecting common mental disorders in primary care settings, the AUCs for the K10 and K6 were at levels similar to those found in Australia and North America (0.88 and 0.85 respectively; Patel et al., 2008). In Burkina Faso and South Africa, the results of the receiver operating characteristic (ROC) analyses were not as strong for detecting depression among women after pregnancy (AUC values ranging from 0.75 in Burkina Faso to 0.66 in South Africa), (Baggaley et al., 2007; Spies, et al., 2009b). Similar results were found in a clinical study conducted in South Africa on the validity of the K10 in identifying depression and anxiety disorders in HIV‐positive individuals. The ROC analyses conducted in the study revealed AUCs of 0.77 for depression, 0.78 for generalized anxiety disorder (GAD), and 0.77 for post‐traumatic stress disorder (PTSD) (Spies et al., 2009a). Although these AUC values are not as high as those found in epidemiological studies conducted in Australia and the United States, they were considered significant enough to be deemed reasonably valid screeners of depression (Spies et al., 2009a). It has been suggested that AUC values of 0.70 and higher indicate a useful screening scale (Swets, 1988).
Although research on the validity of the K10 in screening for psychological distress in various clinical populations is promising, the applicability of the K10 and the K6 for use in epidemiological studies in developing countries is still under investigation. The South African Stress and Health (SASH) survey, which formed part of the WHO's Mental Health Survey initiative, presented a unique opportunity to evaluate the ability of translated versions of the K10 and K6 in screening for depression and anxiety disorders in the general population. The findings that have been published to date seem promising. Kessler et al. (2010) recently published data on the performance of the K6 in screening for serious mental illness in countries participating in the WHO World Mental Health (WMH) survey initiative, including in South Africa. They reported eigenvalues of 4.1 for the first factor, factor loadings of 0.76 to 0.87 for the first factor, significant model parameters of best‐fitting regression models, and an AUC of 0.76. In addition, a preliminary finding of the K10's ability to screen in the SASH study, published by Myer et al. (2008), indicated highly significant associations between K10 scores and CIDI‐defined diagnoses.
The purpose of the present study was to evaluate the validity of the K10 and the K6 in screening for depression and anxiety disorders in the multi‐cultural population of South Africa. To the authors' knowledge, no studies on the validity of translated versions of both the K10 and K6 in screening for depression and anxiety disorders in the general populations of southern African countries have been published. Data were obtained from the SASH study; the first psychiatric epidemiological study to take place in South Africa. By validating translated measures such as the K10 and K6 in various regions in the world including southern Africa, future attempts to obtain standardized cross‐national data on prevalence of mental disorders will become more manageable.
Methods
Sample
The SASH study, a nationally representative household survey of psychiatric illness, formed part of the WHO's WMH program. The sample in the study consisted of adult (18 years or older) men and women from various racial and ethnic backgrounds living in households or hostel residences between January 2002 and June 2004. Racial constructs developed during apartheid were used in the study, not to reify them, but to allow exploration of persistent differences across groups of individuals in the post‐apartheid era.
The SASH study obtained a nationally representative sample of 4351 adult participants. A three‐stage clustered area probability sample design was employed to select the sample. In stage one; sampled residences were stratified into 10 diverse housing categories based on the 2001 South African Census Enumeration Areas (EAs). In stage two, 600 households were identified within each stratified housing category. Finally in the third stage one adult participant was randomly selected from each household using the Kish method. See Williams et al. (2004) for complete details on study design.
Measures
The WHO Composite International Diagnostic Interview Version 3.0 (CIDI 3.0) was employed in this study to identify participants who met criteria for a psychiatric disorder (Kessler and Ustun, 2004). The CIDI is a fully structured interview designed for face‐to‐face administration by lay‐interviewers. It generates diagnoses based on the International Classification of Diseases, 10th Revision (ICD‐10) and DSM‐IV criteria.
The K10 and the abbreviated K6 scales were included in the study. The K6 is a subset of the K10, containing six of the 10 questions from the K10. These brief scales were developed for use in epidemiological studies to screen for psychological distress in the general population. The scales ask about symptoms experienced in the previous month. The K10 consists of 10 questions such as “During the last 30 days, how often did you feel depressed”, “During the last 30 days, how often did you feel anxious”, and “During the last 30 days, how often did you feel hopeless”. The responses range from one (never) to five (all of the time) and the total score is a summation of the responses.
The English versions of the CIDI, K10, and K6 were translated and back‐translated into Afrikaans, Zulu, Xhosa, Northern Sotho, and Tswana by bilingual and multilingual experts. Discrepancies that emerged from the back‐translation were decided on by consensus of a team of experts.
Statistical analyses
The person‐level SASH data were weighted to adjust for differential probabilities of selection within households, differential non‐response, and residual discrepancies between the sample and the population on a profile of census demographic and geographic variables. These weights were used when calculating proportions.
Data analysis was conducted using STATA version 10.0. Cases were defined as any 12‐month major depressive disorder or anxiety disorder. Anxiety disorders included in these analyses were panic disorder, agoraphobia, GAD, PTSD, and social phobia. Dysthymia had a very low prevalence rate (N = 1) and was therefore excluded from the analyses.
The psychometric properties of the K10 and K6 were tested against the CIDI. ROC analyses were conducted to evaluate the abilities of the K10 and K6 to screen for depression and anxiety disorders, both as a group (any 12‐month major depressive disorder or anxiety disorder) and individually (each disorder on its own). Individual disorders were examined to determine the extent to which the AUCs of the overall categories were driven by certain conditions.
The area under the ROC curve provides an estimated probability of a scale's ability to discriminate between true cases of depression and anxiety versus true non‐cases, i.e. individuals without depression and anxiety, when the cases have been randomly sampled from the population. AUC values range from 0.5 to 1.0; a value of 0.5 means the result is due to chance, while a value of 1.0 indicates perfect discrimination. Given that STATA does not produce weighted AUCs, the lowest and highest quartiles of the weighting variable distribution were examined. No appreciable difference was found from the overall non‐adjusted ROCs. ROC curves were also generated stratifying by sex and by race/ethnicity (Black versus non‐Black) and the equality of these stratified curves was assessed. As previously mentioned racial constructs developed during apartheid were used in this study, not to reify them, but to allow exploration of across‐group differences in the post‐apartheid era. ROC curves were compared using a non‐parametric test (DeLong et al., 1988). The non‐Black grouping was created because the largest race/ethnic group in South Africa is Black (approximately 79%), resulting in the representative sample sizes of the remaining race/ethnic groups (White, Colored, Indian/Asian) in this study being too insufficient in power to be able to detect differences when calculated separately.
Likelihood ratios (LRs) were calculated to determine the likelihood of the result (positive, LR+, or negative, LR–) being observed in a person with the psychiatric disorder in comparison to the likelihood of the same result happening in a person without the psychiatric disorder. Cronbach alphas were calculated to determine the internal consistency of the K10 and the K6.
Due to the limited staff and resources within the public health care system in South Africa, cut‐offs that reduced the misallocation of resources to patients who do not suffer from mental disorders were chosen. Consistent with the approach by Patel et al. (2008) the recommended cut‐offs were therefore based on the optimal balance between sensitivity and positive predictive value (PPV), with both sensitivity and PPV needing to be above 50% to be deemed acceptable.
Results
The total sample size was 4077. Females constituted 53.7% of the sample. The age of participants ranged from 18 to 92; with an interquartile range of 25 to 46, and a median age of 34. Consistent with the racial and ethnic demographics of South Africa, 75.6% of the sample was Black, 10.9% was mixed race (Colored), 10.2% was White, and 3.4% was Indian/Asian. The percentage of participants who had either experienced major depressive disorder or an anxiety disorder within the previous 12 months of the interview was 11.8% (see Table 1).
Table 1.
Weighted prevalence of participants who met CIDI‐defined criteria for 12‐month DSM‐IV depression and anxiety disorders (n = 4351)
| CIDI disorder | Percentage |
|---|---|
| Any depression or anxiety disorder | 11.9 |
| Any anxiety disorder | 8.3 |
| Major depression | 4.9 |
| Post‐traumatic stress disorder | 0.6 |
| Agoraphobia | 5.1 |
| Social phobia | 1.9 |
| Panic disorder | 0.8 |
| Generalized anxiety disorder | 1.4 |
As seen in Figures 1a and 1b the AUC for the K10 was 0.73 and the AUC for the K6 was 0.72 for any 12‐month depression or anxiety disorder. Results were similar for specific 12‐month depression and anxiety disorders for the K10 (see Figure 2) and the K6 (see Figure 3). The AUC of the K10 ranged from 0.76 for panic disorder to 0.69 for PTSD, while the AUC of the K6 ranged from 0.75 for panic disorder to 0.67 for PTSD (see Tables 2 and 3).
Figure 1.
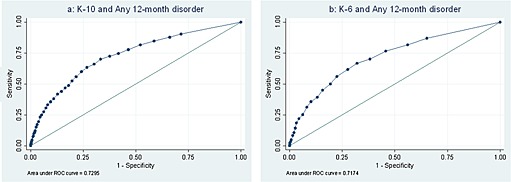
ROC curves for the K10 and K6 scores predicting any cases of 12‐month DSM‐IV depression and anxiety disorders.
Figure 2.
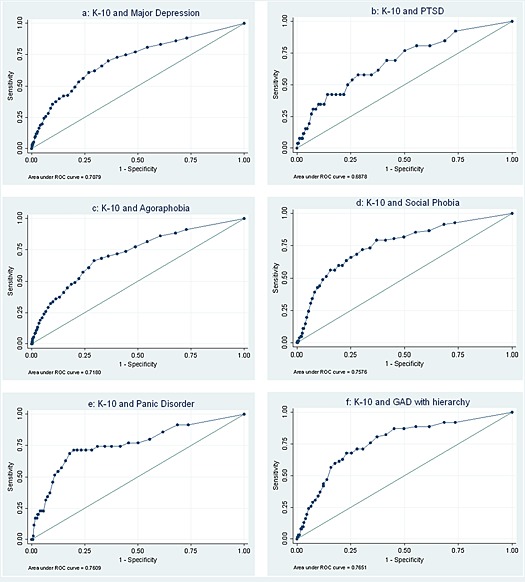
ROC curves for the K10 scores predicting cases of 12‐month DSM‐IV depression and anxiety disorders.
Figure 3.
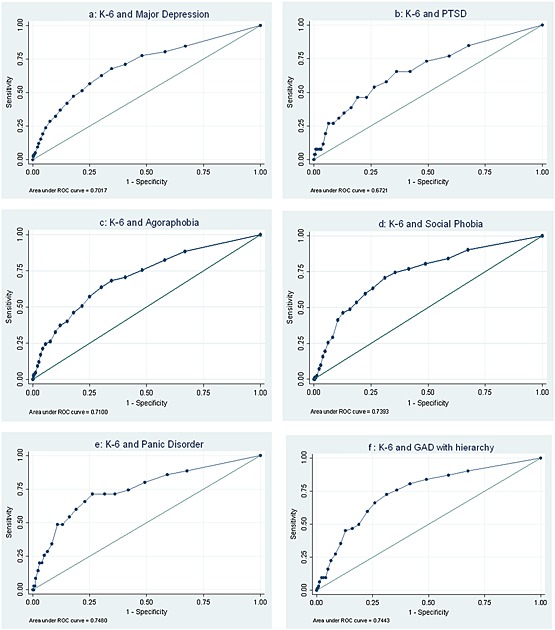
ROC curves for the K6 scores predicting cases of 12‐month DSM‐IV depression and anxiety disorders.
Table 2.
Results of ROC curve analysis for the Kessler scales and any 12‐month depression or anxiety disorder
| Any depression or anxiety disorder | Cut‐off | AUC | Sensitivity | Specificity | Correctly classified | PPV | LR+ | LR– |
|---|---|---|---|---|---|---|---|---|
| K10 | 16 | 73 | 70 | 66.7 | 67.1 | 23 | 2.1 | 0.45 |
| K6 | 10 | 71.7 | 70.2 | 67.9 | 62.8 | 20.7 | 1.84 | 0.48 |
Table 3.
Results of ROC curve analysis for the Kessler scales and individual 12‐month DSM‐IV disorders
| Cut‐off | AUC | Sensitivity | Specificity | Correct classification | PPV | LR+ | LR‐ | |
|---|---|---|---|---|---|---|---|---|
| K10 | ||||||||
| Any anxiety disorder | 16 | 73.5 | 71.4 | 65.3 | 65.8 | 16.3 | 2.06 | 0.44 |
| Major depressive disorder | 16 | 70.8 | 70.1 | 63.9 | 64.2 | 9.7 | 1.94 | 0.47 |
| PTSD | 16 | 68.8 | 61.5 | 62.3 | 62.3 | 1 | 1.63 | 0.62 |
| Agoraphobia | 17 | 71.8 | 68.2 | 67.2 | 67.2 | 10.5 | 2.08 | 0.47 |
| Social phobia | 18 | 75.8 | 72 | 69.5 | 69.5 | 4.6 | 2.3 | 0.4 |
| Panic disorder | 19 | 76.1 | 71.4 | 71.8 | 71.7 | 2.1 | 2.53 | 0.4 |
| GAD | 18 | 76.5 | 71 | 69.3 | 69.3 | 3.5 | 2.31 | 0.42 |
| K6 | ||||||||
| Any anxiety disorder | 11 | 72.2 | 68.3 | 66.7 | 66.8 | 16.3 | 2.05 | 0.48 |
| Major depressive disorder | 11 | 70.2 | 67.8 | 65.4 | 65.5 | 9.8 | 1.96 | 0.49 |
| PTSD | 11 | 67.2 | 65.4 | 63.8 | 63.8 | 1.2 | 1.81 | 0.54 |
| Agoraphobia | 11 | 71 | 68.2 | 65.4 | 65.6 | 10 | 1.97 | 0.49 |
| Social phobia | 12 | 73.9 | 70.7 | 68.9 | 69 | 4.5 | 2.3 | 0.42 |
| Panic disorder | 13 | 74.8 | 71.4 | 73.8 | 73.7 | 2.3 | 2.72 | 0.39 |
| GAD | 12 | 74.4 | 72.6 | 68.7 | 68.8 | 3.5 | 2.32 | 0.4 |
It was not possible to identify a single cut‐off point that optimally balanced sensitivity and PPV in this study. In order to yield a PPV of above 50%, a cut‐off of 42 was necessary, which in turn yielded only 4% sensitivity. Alternatively, when balancing sensitivity and specificity, an approach taken in previous research (Baggaley et al., 2007) the optimum cut‐offs for detecting any cases of CIDI‐defined depression and anxiety disorders on the K10 was ≥ 16, yielding sensitivity 70% and specificity 67% (Table 2). For the K6, the chosen optimum cut‐off for detecting any cases of CIDI‐defined depression and anxiety disorders on the K6 was ≥ 10, yielding sensitivity 70% and specificity 62% (Table 3). However, as mentioned earlier, these cut‐offs (16 for the K10 and 10 for the K6) yielded extremely low PPVs, with PPVs of 23% for the K10 and 21% for the K6.
There was a significant difference when ROC curves were looked at by race/ethnicity, but not when stratified by gender (results not shown). Examinations of differences in responding by race/ethnic groups revealed that the K10 had significantly lower discriminating ability with respect to depression and anxiety disorders among the Black group (0.71) than among the combined minority race/ethnic groups of White, Colored, and Indian/Asian (0.78; p = 0.016). Likewise the K6 had significantly lower discriminating ability with respect to depression and anxiety disorders among the Black group (0.70) than among the combined minority race/ethnic groups of White, Colored, and Indian/Asian (0.77; p = 0.018).
The ROC curves for any 12‐month disorder did not significantly differ among males and females on the K10 or the K6 (p‐values of 0.916 and 0.943). The AUC on the K10 was 0.72 for females and 0.73 for males. The ROC curves on the K6 were comparable to those on the K10, with 0.71 for females and 0.71 for males.
The K10 was also found to have strong internal consistency, with a Cronbach's alpha coefficient of 0.84 for any 12‐month disorder. In contrast, the Cronbach's alpha coefficient for the K6 of any 12‐month disorder was 0.48.
Discussion
The results of this study indicate that the K10 and K6 demonstrate moderate discriminating ability in detecting depression and anxiety disorders in the general population, with AUCs of 0.73 and 0.72 respectively. It appears the Kessler scales are not as useful in screening for depression and/or anxiety disorders among the general population of South Africa as they are in Canada, Australia, and Japan (Furukawa et al., 2003; Kessler et al., 2002; Kessler et al., 2007). Indeed Kessler et al. (2010) recently reported that the K6 had lower AUCs in South Africa than in the other countries reported.
With respect to clinical use of these measures, neither the K10 nor the K6 met our acceptability criteria. In order to reduce the misallocation of resources to patients who are not in need of services within an overburdened and underfunded health care system, the intention was to identify cut‐offs that optimally balanced sensitivity and PPV, with both needing to be higher than 50% to be deemed acceptable. Neither scale met these criteria. Any cut‐off score that yielded a high PPV concurrently yielded extremely low sensitivity.
Alternatively, when attempting to balance sensitivity and specificity to identify an optimal cut‐off for use in epidemiological research, consistent with the approach taken in similar studies on the Kessler scales, a higher cut‐off was required. For example, in Burkina Faso a cut‐off of 12 was chosen as it yielded 74% sensitivity and 76% specificity (Baggaley et al., 2007). In the current study the optimum cut‐off of 16 yielded 70% sensitivity and 67% specificity.
A particularly interesting and relevant finding in this study is that the Kessler scales had significantly lower discriminating ability with respect to depression and anxiety disorders among the Black group than among the combined non‐Black group. As previously discussed, it was necessary to group White, Colored, and Indian/Asian into one group (non‐Black) due to small sample sizes. This discrepancy in discriminating ability may reflect differential item functioning or biased measurement. It is notable that the Black population in South Africa is historically the most disenfranchised race group with the lowest socio‐economic status; often lacking in basic necessities such as running water and electricity. The Black population may be more likely to endorse items such as “How often do you feel that everything is an effort?” and “How often do you feel worthless?” regardless of the existence of a mental disorder. Alternatively, differences across countries may result from variations in interpretation or expression of symptoms (Mosotho et al., 2008; Smit et al., 2006; Tomlinson et al., 2007). Tomlinson et al. (2007), for example, suggest that although there are universal somatic, cognitive, and emotional symptoms of depression, the expression of these symptoms is culturally defined. Consequently, in order to ascertain cross‐cultural equivalence, follow‐up studies are needed to fully investigate the existence of differential item functioning on the Kessler scales.
It would be interesting to compare item response differences by ethnicity and culture within each nation previously studied, particularly given the findings discussed above. Unfortunately, the majority of studies conducted on the K10 and K6 in North America, Australia, India, and Burkina Faso were either conducted on a homogenous sample, such as the sample in India, which was 88% Konkani speakers (Patel et al., 2008), or they did not report on similarities or differences between various linguistic and cultural groups. Whether this was because no differences were found or the existence of item bias was not considered or was not expected is not known.
The relatively poorer performance of the K10 and K6 in South Africa may be influenced by the discrepancy in time periods assessed by the K10/K6 (past 30 days) versus the CIDI (past 12 months). This time difference may contribute to diluting the specificity of these screeners. Further research, standardizing the time period assessed or asking about worst 30‐day period in the past year is recommended.
While the Kessler scales seem very valuable in most countries (Kessler et al., 2010), they appear less so in South Africa. The use of these measures in clinical settings or epidemiological research is not recommended until further research has lent statistical support to the strength of the scales for use in South Africa. Further work, e.g. additional studies examining the K10 and the K6 against clinician‐rated diagnostic instruments such as the SCID, is needed. Rather than employing local residents trained in the administration of the survey instruments, as was done in the current study, it is recommended that clinician assessments be included in the establishment of diagnoses in future validation research.
The Kessler scales have the potential to play an important role in raising the awareness of the mental health needs of people living in countries with limited funds and services by helping to identify and monitor the prevalence of mental disorders in these populations. Moreover by employing a screening scale, which has been validated for global use, in epidemiological studies conducted throughout the world, valuable cross‐regional and cross‐national comparisons can be made.
Declaration of interest statement
D.J.S. has received research grants and/or consultancy honoraria from AstraZeneca, Eli‐Lilly, GlaxoSmithKline, Jazz Pharmaceuticals, Johnson & Johnson, Lundbeck, Orion, Pfizer, Pharmacia, Roche, Servier, Solvay, Sumitomo, Takeda, Tikvah, and Wyeth. These funders had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication. All of the other authors declare that they have no competing interests.
Acknowledgements
These activities were supported by the US National Institute of Mental Health (R01MH070884), the John D. and Catherine T. MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13‐MH066849, R01‐MH069864, and R01‐DA016558), the Fogarty International Center (FIRCA R01‐TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho‐McNeil Pharmaceutical, GlaxoSmithKline and Bristol‐Myers Squibb. The South Africa Stress and Health study was funded by grant R01‐MH059575 from the National Institute of Mental Health and the National Institute of Drug Abuse, with supplemental funding from the South African Department of Health and the University of Michigan. S.S. and L.S.A. are supported by the South African Research Chairs Initiative of the Department of Science and Technology and the National Research Foundation. D.J.S. is supported by the Medical Research Council of South Africa. The South African Stress and Health study was carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork, and data analysis. We thank Martin Kidd for his advice on the interpretation of results.
References
- Baggaley R.F., Ganaba R., Filippi V., Kere M., Marshall T., Sombie I., Storeng K.T., Patel V. (2007) Detecting depression after pregnancy: The validity of the 10 and K6 in Burkina Faso. Tropical Medicine & International Health, 12(10), 1225–1229, DOI: 10.1111/j.1365-3156.2007.01906.x [DOI] [PubMed] [Google Scholar]
- Baillie A.J. (2005) Predictive gender and education bias in Kessler's psychological distress scale (K10). Social Psychiatry and Psychiatric Epidemiology, 40(9), 743–748, DOI: 10.1007/s00127-005-0935-9 [DOI] [PubMed] [Google Scholar]
- Cairney J., Veldhuizen S., Wade T.J., Kurdyak P., Streiner D.L. (2007) Evaluation of 2 measures of psychological distress as screeners for depression in the general population. Canadian Journal of Psychiatry, 52(2), 111–120. [DOI] [PubMed] [Google Scholar]
- DeLong E.R., DeLong M., Clarke‐Pearson D.L. (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics, 44(3), 837–845. [PubMed] [Google Scholar]
- Fassaert T., De Wit M.A.S., Tuinebreijer W.C., Wouters H., Verhoeff A.P., Beekman A.T.F., Dekker J. (2009) Psychometric properties of an interviewer‐administered version of the Kessler Psychological Distress scale (K10) among Dutch, Moroccan, and Turkish respondents. International Journal of Methods in Psychiatric Research, 18(3), 159–168, DOI: 10.1002/mpr.288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furukawa T.A., Kawakami N., Saitoh M., Ono Y., Nakane Y., Nakamura Y., Tachimori H., Iwata N., Uda H., Nakane H., Watanabe M., Naganuma Y., Hata Y., Kobayashi M., Miyake Y., Takeshima T., Kikkawa T. (2008) The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. International Journal of Methods in Psychiatric Research, 17(3), 152–158, DOI: 10.1002/mpr.257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furukawa T.A., Kessler R.C., Slade T., Andrews G. (2003) The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well‐Being. Psychological Medicine, 33(2), 357–362, DOI: 10.1017/s0033291702006700 [DOI] [PubMed] [Google Scholar]
- Gureje O., Lasebikan V.O., Kola L., Makanjuola V.A. (2006) Lifetime and 12‐month prevalence of mental disorders in the Nigerian Survey of Mental Health and Well‐Being. The British Journal of Psychiatry, 188(5), 465–471, DOI: 10.1192/bjp.188.5.465 [DOI] [PubMed] [Google Scholar]
- Kessler R.C., Ustun T.B. (2004) The World Mental Health (WMH) survey initiative version of the WHO‐CIDI. International Journal of Methods in Psychiatric Research, 13(2), 93–121, DOI: 10.1002/mpr.168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler R.C., Andrews G., Colpe L.J., Hiripi E., Mroczek D.K., Normand S.L.T., Walters E.E., Zaslavsky A.M. (2002) Short screening scales to monitor population prevalences and trends in non‐specific psychological distress. Psychological Medicine, 32(6), 959–976, DOI: 10.1017/s0033291702006074 [DOI] [PubMed] [Google Scholar]
- Kessler R.C., Barker P.R., Colpe L.J., Epstein J.F., Gfroerer J.C., Hiripi E., Howes M.J., Normand S.T., Manderscheid R.W., Walters E.E., Zaslavsky A.M. (2007) Screening for serious mental illness in the general population. Archives of General Psychiatry, 60(2), 184–189, DOI: 10.1001/archpsyc.60.2.184 [DOI] [PubMed] [Google Scholar]
- Kessler R.C., Green J.G., Gruber M.J., Sampson N.A., Bromet E., Cuitan M., Furukawa T.A., Gureje O., Hinkov H., Hu C., Lee S., Mneimneh Z., Myer L., Oakley‐Browne M., Posada‐Villa J., Sagar R., Viana M.C., Zaslavsky A.M. (2010) Screening for serious mental illness in the general population with the K6 screening scale: results from the WHO World Mental Health (WMH) survey initiative. International Journal of Methods in Psychiatric Research, 19(Suppl. 1), 4–22, DOI: 10.1002/mpr.310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mosotho N.L., Louw D.A., Calitz F.J.W., Esterhuyse K.G.F. (2008) Depression among Sesotho speakers in Mangaung, South Africa. African Journal of Psychiatry, 11(1), 35–43. [DOI] [PubMed] [Google Scholar]
- Myer L., Stein D.J., Grimsrud A., Seedat S., Williams D.R. (2008) Social determinants of psychological distress in a nationally‐representative sample of South African adults. Social Science & Medicine, 66(8), 1828–1840, DOI: 10.1016/j.socscimed.2008.01.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel V., Araya R., Chowdhary N., King M., Kirkwood S., Nayak S., Simon G., Weiss H.A. (2008) Detecting common mental disorders in primary care in India: A comparison of five screening questionnaires. Psychological Medicine, 38(2), 221–228, DOI: 10.1017/s0033291707002334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seedat S., Emsley R.A., Stein D.J. (2004) Land of promise: Challenges and opportunities for research in South Africa. Molecular Psychiatry, 9(10), 891–892, DOI: 10.1038/sj.mp.4001572 [DOI] [PubMed] [Google Scholar]
- Smit J., van den Berg C.E., Bekker L.‐G., Seedat S., Stein D. (2006) Translation and cross‐cultural adaptation of a mental health battery in an African setting. African Health Sciences, 6(4), 215–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spies G., Kader K., Kidd M., Smit J., Myer L., Stein D.J., Seedat S. (2009a) Validity of the K10 in detecting DSM‐IV‐defined depression and anxiety among HIV‐infected individuals. AIDS Care, 21(9), 1163–1168. [DOI] [PubMed] [Google Scholar]
- Spies G., Stein D.J., Roos A., Faure S.C., Mostert J., Seedat S., Vythilingum B. (2009b) Validity of the Kessler 10 (K10) in detecting DSM‐IV defined mood and anxiety disorders among pregnant women. Archives of Women's Mental Health, 12(2), 69–74, DOI: 10.1007/s00737-009-0050-0 [DOI] [PubMed] [Google Scholar]
- Swets J.A. (1988) Measuring the accuracy of diagnostic systems. Science, 240(4857), 1285–1293, DOI: 10.1126/science.3287615 [DOI] [PubMed] [Google Scholar]
- Tomlinson M., Swartz L., Kruger L.M., Gureje O. (2007) Manifestations of affective disturbances in sub‐Saharan Africa: Key themes. Journal of Affective Disorder, 102(1/2), 191–198, DOI: 10.1016/j.jad.2006.09.029 [DOI] [PubMed] [Google Scholar]
- Williams D.R., Herman A., Kessler R.C., Sonnega J., Seedat S., Stein D.J., Moomal H., Wilson C.M. (2004) The South African Stress and Health study: Rationale and design. Metabolic Brain Disease, 19(1/2), 135–147, DOI: 10.1023/B:MEBR.0000027424.86587.74 [DOI] [PubMed] [Google Scholar]
- Williams D.R., Herman A., Stein D.J., Heeringa S.G., Jackson P.B., Moomal H., Kessler R.C. (2007) Twelve‐month mental disorders in South Africa: Prevalence, service use, and demographic correlates in the population‐based South African Stress and Health study. Psychological Medicine, 38(2), 1–10, DOI: 10.1017/s0033291707001420 [DOI] [PMC free article] [PubMed] [Google Scholar]